
Abstract
Background:
Ischemic stroke is one of the main causes of mortality and long-term disability worldwide. Although it contributes substantially to the worldwide burden of disease, there is still a great scarcity of research on the in-hospital mortality and its predictors in Eastern Ethiopia. Therefore, this study aimed to assess in-hospital mortality and its predictors among adult ischemic stroke patients in public hospitals in the Harari region, Eastern Ethiopia.
Methodology:
A retrospective cohort study was conducted among 292 ischemic stroke patients in the Harari region’s public hospitals from July 1, 2019, to June 30, 2024. The incidence of mortality was calculated with a 95% confidence interval, and predictors of mortality were identified through Cox regression analyses.
Results:
Of the 292 patients included, 190 (65.07%) improved, 13 (4.45%) were discharged with complications, 32 (10.96%) died, and 57 (19.52%) were discharged against medical advice. The 60-month follow-up revealed a mortality rate of 7.42 (95% CI: 5.25–10.49) per 1000 person-months. The mortality risk was greater among stroke patients with diabetes (AHR: 3.31, 95% CI: 1.35, 8.14), kidney disease (AHR: 4.29, 95% CI: 1.59, 11.59), aspiration pneumonia (AHR: 4.16, 95% CI: 1.76, 9.86), and poor Glasgow Coma Scale (GCS) scores (AHR: 3.74, 95% CI: 1.14, 12.33).
Conclusion:
In this study, in-hospital mortality occurred in one out of nine ischemic stroke patients treated at public medical facilities. Factors such as diabetes, kidney disease, poor GCS score, and aspiration pneumonia associated with increased mortality risk. Hence, special emphasis should be given to early screening and follow-up of at-risk patients.
Introduction
Ischemic stroke is a leading cause of mortality and long-term disability globally, contributing substantially to the worldwide burden of disease.1,2 It occurs when an interruption in cerebral blood flow causes damage to brain tissue, resulting in severe neurological impairments and often fatal outcomes. 3 Low- and middle-income countries, including Ethiopia, have experienced a rising incidence of stroke in recent decades due to demographic transitions, an increased prevalence of vascular risk factors, and limited access to timely and effective stroke care.4,5
A study conducted in Spain revealed that the cumulative incidence of cerebrovascular disease per 100,000 population was 218 in men and 127 in women. 6 Studies have reported in-hospital mortality rates ranging from 6% to over 37% and case fatality rates reaching 40% within 5 years of stroke onset in some sub-Saharan African countries. 7 Moreover, long-term case fatality rates remain high, with stroke-related mortality reaching 40% within 5 years in some sub-Saharan populations. 8 In Ethiopia, stroke accounted for 6.23% of total deaths in 2017, with an age-adjusted death rate of approximately 90 per 100,000 people. 5 The pooled prevalence of poor treatment outcomes, including death and significant disability, among stroke patients is approximately 30%, with mortality alone at approximately 22.6%. 5
A significant healthcare gap exists in low-income and lower-middle-income countries, characterized by delays in stroke diagnosis and higher rates of unfavorable clinical outcomes for affected patients. 9 Interventions like intravenous thrombolysis and mechanical thrombectomy are available for only a small fraction of patients due to cost, infrastructure, and trained staff constraints. 10 Despite this growing challenge, data on the survival outcomes and determinants of mortality among ischemic stroke patients in Ethiopian healthcare settings remain scarce. Few studies in Ethiopia have examined the mortality and its predictors among adult ischemic stroke patients,5,11,12 and the findings of these studies cannot be generalized to other settings because of differences in lifestyle and environmental factors across various regions of the country, which can significantly influence stroke outcomes.
Studies have revealed that advanced age, delayed hospital presentation, and a low Glasgow Coma Scale (GCS) score at admission are among the strongest independent predictors of poor outcomes and high in-hospital mortality in ischemic stroke patients.5,11,12 These clinical factors are often compounded by a patient’s medical history, which includes having a prior stroke, as well as preexisting conditions such as diabetes, hypertension, structural heart disease, and atrial fibrillation. Furthermore, a prolonged hospital stay is associated with poor prognosis, and an elevation in the critical serum creatinine biochemical marker is strongly associated with an increased risk of in-hospital mortality. 5 In a clinical study early recurrent embolization was a predictive clinical factor for in-hospital mortality in cardioembolic ischemic stroke. 13 However, context-specific studies are essential to guide evidence-based interventions tailored to local healthcare infrastructure and population needs.
Many studies in Ethiopia focus on stroke as a general topic. Nevertheless, there is a paucity of evidence concerning ischemic stroke because ischemic and hemorrhagic strokes have different causes, risk factors, clinical presentations, and outcomes.14,15 Studying ischemic stroke predictors allows for a more precise understanding of its unique risk factors and clinical course, enabling targeted interventions to improve outcomes for this specific stroke type. This study aims to fill this gap by investigating the survival patterns and predictors of mortality among adult ischemic stroke patients admitted to public hospitals in the Harari region in Eastern Ethiopia. By employing a retrospective cohort design over 5 years, this study provides insight into clinical outcomes and highlights key predictors that can inform stroke care strategies in similar resource-limited settings.
Methods
Study design and setting
A retrospective cohort study was conducted among patients diagnosed with ischemic stroke at public hospitals in the Harari region, eastern Ethiopia, from July 15 to August 1, 2024. The Harari region is situated 526 km east of Addis Ababa, the capital city of Ethiopia. The region is currently served by two public hospitals, two private hospitals, one police hospital, and one non-governmental hospital. Additionally, healthcare services are provided through 9 health centers, 29 private clinics, 26 health posts, and a regional laboratory. The two public hospitals in the area—Jugal General Hospital (JGH) and Hiwot Fana Comprehensive Specialized University Hospital (HFCSUH)—provide the local population with medical services.
Populations and sampling
The source population for this study included all patients aged 15 years and older who were treated for Ischemic stroke at public hospitals in the Harari Regional State. The study population specifically consisted of Ischemic stroke patients aged 15 years or older who were admitted and registered in the adult medical wards of these hospitals between July 1, 2019, and June 30, 2024. Patients with incomplete medical records (who lacked information on treatment outcomes or if the date of diagnosis was unknown) were excluded.
A total of 313 ischemic stroke patients were treated at the medical ward of HFCSUH and Jugal General Hospital between July 1, 2019, and June 30, 2024. There were 282 and 31 patients from each hospital, respectively. Of these, 21 patients’ medical records were incomplete. The final analysis included 292 ischemic strokes.
Variables
The main outcome of this study was in-hospital mortality among ischemic stroke.
Operational definitions
Data collection and quality control
The data were collected via a data extraction format adapted from the WHO STEPSwise approach to stroke surveillance. 18 This form included key patient information such as demographic details, treatment outcomes, comorbidities, medications used, laboratory investigations, and clinical data. Four public health professionals from Haramaya University carried out the data collection under the supervision of two trained supervisors. Data were extracted from patients’ paper-based medical records.
Before the actual data collection, a pretest was conducted using 5% (16) of the medical records of stroke patients from both hospitals to assess the reliability and consistency of the data collection tools. Based on the pretest findings, necessary revisions were made to the instruments. Data collectors received training for 2 days on the procedures and tools of data collection. Data collection was closely supervised by the principal investigators, and any inconsistencies identified were promptly addressed. Data was collected using the Kobo toolbox were reviewed for consistency and completeness before being uploaded to the server.
Data analysis
The dataset was then imported into STATA version 17.0 for analysis. The outcome variable was categorized into two groups: death (event) and censored. The cumulative incidence of mortality was calculated by dividing the number of deaths by the total initial population at risk during follow-up. Incidence density was calculated as the number of deaths per patient-months at risk. Kaplan‒Meier failure curves were used to estimate mortality probabilities, and the log-rank test was employed to compare survival functions across explanatory variables. To address missing data, a complete case analysis was applied under the assumption that data were missing completely at random (MCAR). Cox PH was fitted to determine the predictors of mortality. The variance inflation factor was used to determine the presence of multicollinearity. To control for the possible effect of confounders, variables with a p-value of ≤0.2 were entered by stepwise regression into a multivariable Cox regression model. The multivariable model’s statistical significance was declared by a p value < 0.05, and the strength of the association was indicated by the hazard ratio (HR) with its 95% confidence interval. The goodness of fit of the model was assessed via the Cox–Snell residual technique. The cumulative hazard plot follows a straight line through the origin with slope, indicating that the model fits the data well. (Figure 1). The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement. 19 The completed STROBE checklist is available as Supplemental File 1.
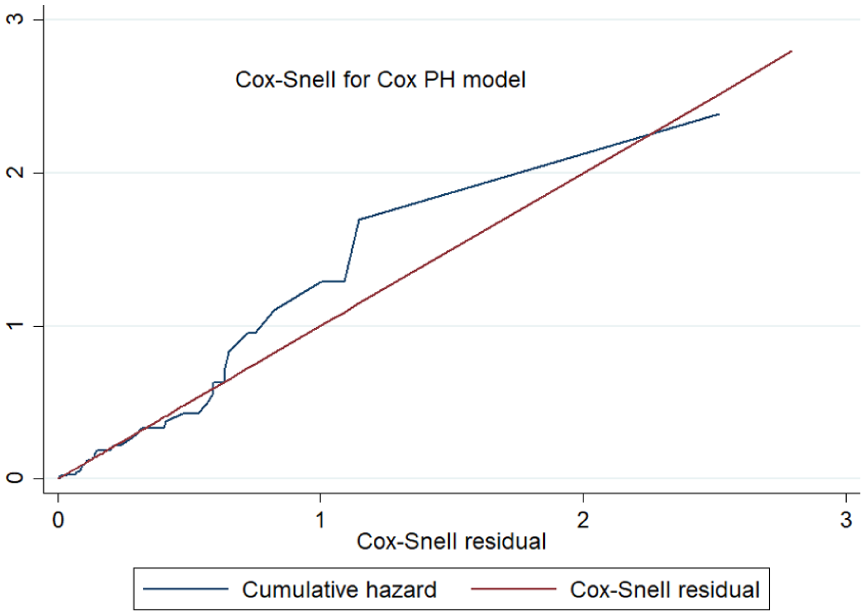
Cox–Snell residuals for Cox PH models of ischemic stroke patients in Harari, eastern Ethiopia, 2024.
Results
Sociodemographic characteristics
A total of 313 medical records of patients with ischemic stroke were identified. Of these, 21 patients’ medical records were incomplete. The final analysis included 292 ischemic strokes. Among the 292 adult ischemic stroke patients, 190 (65.07%) were males, and the mean age (±SD) was 56 years (±16.11). With respect to residence, approximately 67.12% of the patients were from rural areas (Table 1).
Sociodemographic characteristics of ischemic stroke patients at public hospitals in the Harari region, East Ethiopia, from 2019 to 2024 (N = 292).

Clinical characteristics
Hemiparesis was the most frequent clinical manifestation (76.71%), followed by unconsciousness (27.74%). The median time from symptom onset to symptom onset was 45 (IQR: 64.50) h, and approximately 54.45% of the time from symptom onset to admission was >24 h. The majority of them, 211 (72.26%), had comorbidities. The most prevalent comorbid condition was hypertension (47.26%), which was followed by heart failure (15.07%), diabetes (10.27%), and kidney disease (8.22%). The mean (SD) systolic blood pressure and diastolic blood pressure at hospitalization were 133.28 ± 26.82 and 78.63 ± 17.19 mmHg, respectively. About 9.47% of the patients had elevated total cholesterol levels with a mean total cholesterol of 140.60 ± 47.31 mg/dl. The median length of hospital stay was 5 ± 5.50 days (Table 2).
Clinical characteristics of ischemic stroke patients at public hospitals in the Harari region, East Ethiopia, from 2019 to 2024 (N = 292).

Treatment characteristics
Among the 292 patients, 190 (65.07%) 95% CI (59.39%–70.35%) had improved outcomes, 13 (4.45%) 95% CI (2.59%–7.54%) were discharged with complications, approximately 32 (10.96%) 95% CI (7.84%–15.12%) died, and approximately 57 (19.52%) 95% CI (15.34%–24.50%) were discharged against medical advice on self- and family requests. Among the 32 patients who died, hypertension 20, 62.5%), aspiration pneumonia 19 (59.38%), and increased intracranial pressure 14 (43.75%) were the most frequently documented causes of death secondary to ischemic stroke. Of 292 ischemic stroke patients, 130 (44.52%) experienced complications. Aspiration pneumonia (55 patients; 18.84%) and ICP/brain edema (44 patients; 15.07%) were the most common complications during hospitalization. The most frequently utilized antiplatelet and lipid-lowering medications throughout the patients’ hospital stay were aspirin and atorvastatin, which were given to approximately 68.49% and 70.21% of the patients, respectively. Enalapril, which was administered in approximately 26.03% of cases, was the antihypertensive drug that ischemic stroke patients used the most frequently. In 27.74% of hospitalized ischemic stroke patients, antibiotics (ceftriaxone and metronidazole) were also given for the management of stroke and comorbid diseases, primarily for the treatment of aspiration pneumonia and sepsis (Table 3).
Treatment outcomes for ischemic stroke patients at public hospitals in the Harari region, East Ethiopia, from 2019 to −2024. (N = 292).

Incidence mortality rate of ischemic stroke patients
The study samples were followed for a maximum of 60 months, with no median survival time. Among the total number of stroke patients followed for approximately 60 months, 32 (10.96%, 95% CI (7.84%–15.12%) died. The incidence of death was 7.42 cases per 1000 person‒months of observation, with a 95% CI of 5.25–10.49. The survival probability was highest in the first month of follow-up after ischemic stroke was diagnosed and then decreased as the follow-up time increased (Figure 2).
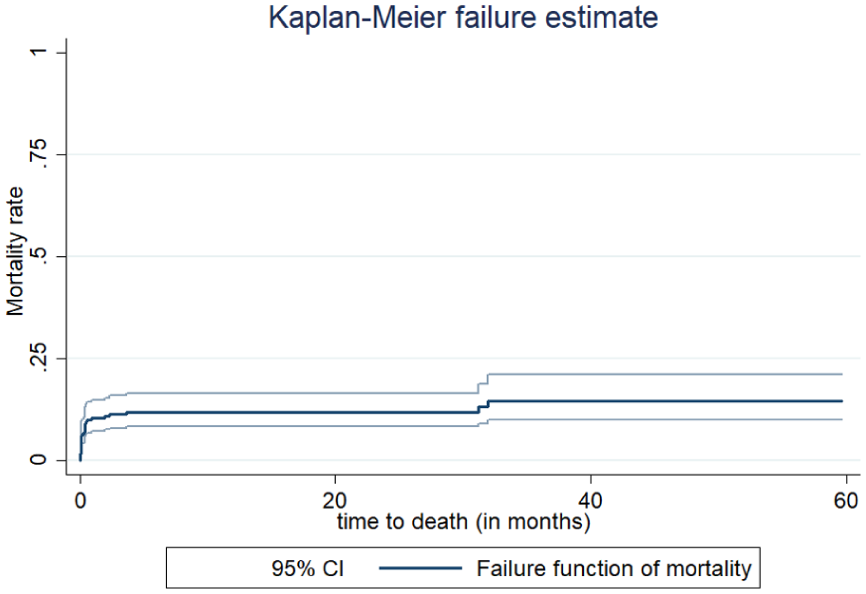
Kaplan‒Meier curve for the cumulative probability of mortality of ischemic stroke in Harari, Ethiopia, 2024.
Predictors of Mortality
In the bivariable Cox regression analysis, 12 variables (sex, residence, hypertension, DM, kidney diseases, myocardial infarction, seizure, HAI, aspirin pneumonia, GCS, statin, and antiplatelet) were identified as factors associated with mortality at p ≤ 0.25. In the multivariable Cox regression analysis, four variables were identified as predictors of mortality. These were DM, kidney diseases, aspirin pneumonia, and poor GCS.
Accordingly, diabetic patients had a threefold greater probability of death because of ischemic stroke than nondiabetic patients did (AHR: 3.31, 95% CI: 1.35, 8.14). The risk of mortality from ischemic stroke was 4.29 times greater among patients with kidney diseases than among those without kidney diseases (AHR: 4.29, 95% CI: 1.59, 11.59). Ischemic stroke patients with aspiration pneumonia were 4.16 times more likely to die than those without aspiration pneumonia (AHR: 4.16, 95% CI: 1.76, 9.86). The hazard of mortality from ischemic stroke was 3.74 times greater among patients with a GCS score < 8 than among those with a GCS score of 13–15 (AHR: 3.74, 95% CI: 1.14, 12.33; Table 4).
Bivariate and multivariate Cox regression analyses of predictors of mortality among ischemic stroke patients at public hospitals in the Harari region, East Ethiopia, 2024.

Bold- Significant at p<0.05
Discussion
This study was performed to assess in-hospital mortality and its predictors among adult ischemic stroke patients in public hospitals in Harar, Eastern Ethiopia. In this study, approximately 32 (10.96%) 95% CI (7.84%–15.12%) of ischemic stroke patients died, with an incidence density of 7.42 cases per 1000 person‒months of observation and a 95% CI of 5.25–10.49. The findings of this study identified poor GCS score, aspiration pneumonia, DM, and kidney disease as independent predictors of ischemic stroke mortality.
The cumulative mortality incidence in this study was in line with that reported in a survey at Gondar University Hospital, Ethiopia (12.5%), 12 and in Spain (7.13%). 20 The in-hospital mortality rate reported in the present study was relatively higher than the 3.1% reported in Taiwan. 21 Furthermore, the cumulative incidence in this study was lower than that reported at the Felege-Hiwot Federal Hospital (29.74%) 21 and in Addis Ababa (20.55%). 22 This could be due to differences in sample size, follow-up period, treatment, complications, and comorbidities. In Taiwan, 2556 patients were followed, and thrombolytic therapy was available. In a study at Felege Hiwot Referral Hospital, Ethiopia, 34.85% of ischemic stroke patients had a previous history of ischemic stroke, and in Addis Ababa, 61.19% of patients were aged 60 years or older. Hypertension (61.19%), dyslipidemia (49%), and diabetes mellitus (46.12%) were the most common comorbidities. In contrast, in this study, hypertension (47.26%) was the most common comorbid disease, followed by heart failure (15.07%) and diabetes (10.27%). The greater number of comorbidities and complications reported in other studies is associated with increased mortality.
In this study, patients with ischemic stroke who presented with a Glasgow Coma Scale (GCS) score of less than 8 had a significantly greater hazard of mortality than did those with a GCS score of 13–15. This finding is consistent with evidence from a previous study conducted in Bahir Dar city, northwestern Ethiopia, 23 which demonstrated that low GCS scores at admission strongly predict poor clinical outcomes and higher case fatality rates among ischemic stroke patients. A possible explanation is that a GCS score < 8 reflects severe neurological injury and impaired consciousness, which are often associated with extensive brain damage, large infarct size, or secondary complications such as aspiration pneumonia, respiratory failure, and increased intracranial pressure. Such conditions reduce the likelihood of recovery and increase the risk of early death.24,25
The risk of mortality was greater among ischemic stroke patients who developed aspiration pneumonia than among those without aspiration pneumonia. This finding is supported by studies conducted in Australia, 26 Germany, 27 and Ethiopia, 23 which reported that poststroke pneumonia is among the most frequent and serious medical complications and substantially contributes to mortality. The increased risk may be explained by an impaired swallowing reflex and reduced consciousness after stroke, which predispose patients to aspiration and subsequent infection. This, in turn, worsens the overall clinical condition, prolongs hospitalization, and leads to systemic complications such as sepsis and respiratory failure, ultimately resulting in increased mortality. 28
Diabetes was positively associated with mortality in this study. Patients with DM were more likely to die from a stroke than those without DM. This finding is congruent with several other studies, 29 including those conducted in Iran.30,31 DM can damage blood vessels over time, making them harder and more prone to blockage and causing microvascular and macrovascular changes, which can worsen ischemic stroke outcomes.29,32
Similarly, the risk of mortality from ischemic stroke was greater among patients with preexisting kidney disease than among those without kidney disease. This finding is consistent with previous studies showing that kidney disease is an independent predictor of poor outcomes and mortality after stroke.23,33,34 The possible explanation for this might be attributed to the combined effects of multiple mechanisms, as patients with kidney disease often carry a greater burden of vascular risk factors such as hypertension, diabetes, and atherosclerosis, which can worsen stroke severity and prognosis, whereas impaired renal function is also closely linked with endothelial dysfunction, systemic inflammation, and a prothrombotic state that together further increase the risk of mortality.35,36 Furthermore, kidney disease may limit treatment options such as anticoagulation and complicate poststroke management due to electrolyte disturbances, anemia, and fluid overload, and these factors together increase vulnerability to mortality after ischemic stroke.36,37
A potential line for future research on ischemic stroke could be a comparative study between lacunar versus non-lacunar infarctions. This is important because the pathophysiology, prognosis, and clinical features of ischemic lacunar strokes are different from other acute ischemic cerebrovascular diseases, which often have a notable favorable short-term prognosis. 38 The study was conducted at two sites, which supported the possibility of generalizations and allowed for a reflection of the regional burden of ischemic stroke since there were two public hospitals in the region.
Limitations of the study
Since the study was based on secondary data, information on several important factors (occupation, public awareness, physical exercise, substance use, and educational status) could not be found on the medical cards and were not assessed. Therefore, we have not used such variables in our models. This could lead to an underestimation of the results and a decrease in the study’s statistical power. In this study, 19.52% were discharged against medical advice, and treating these cases as non-informative censoring may bias mortality estimates.
Conclusion
In this study, in-hospital mortality occurred in one out of nine ischemic stroke patients treated at public hospitals. With respect to aspiration pneumonia, DM, and kidney diseases, a poor GCS score is associated with increased mortality among ischemic stroke patients. Based on the findings of this study, we recommend that health professionals prioritize the care of ischemic stroke patients with aspiration pneumonia, DM, and kidney diseases, and a poor GCS. Administrators at HFCSH and JGH should ensure treatments for managing risk factors such as DM and kidney diseases, as well as secondary prevention measures, including the use of thrombolytic therapy. Additionally, researchers are encouraged to undertake further prospective follow-up studies to investigate the incidence and potential predictors of mortality among ischemic stroke patients.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261433150 – Supplemental material for In-hospital mortality and its predictors among adult ischemic stroke patients in public hospitals in the Harari region, Eastern Ethiopia: A retrospective cohort study
Supplemental material, sj-docx-1-phj-10.1177_22799036261433150 for In-hospital mortality and its predictors among adult ischemic stroke patients in public hospitals in the Harari region, Eastern Ethiopia: A retrospective cohort study by Alemayehu Tesfaye, Abdi Gari Negasa, Birhanu Shegene, Mentesenot Seid, Obsan Kassa and Dawit Firdisa in Journal of Public Health Research
Footnotes
Acknowledgements
We acknowledge the Haramaya University Colleges of Health and Medical Sciences Institutional Health Research Ethical Review Committee for providing ethical clearance. We would like to thank the data collectors and supervisors for their commitment during data collection. We would also like to thank Hiwot Fana Comprehensive Specialized University Hospital and Jugal General Hospital administrative bodies and card room workers for their cooperation and permission to conduct the study.
Abbreviations and Acronyms
AHR: adjusted hazard ratio; CT: computed tomography; DALYs: disability adjusted life years; GCS: Glasgow Coma Scale; HICs: high-income countries; HFCSUH: Hiwot Fana Comprehensive Specialized University Hospital; ICU: intensive care unit; ICP: intracranial pressure; IV-tPA: intravenous tissue plasminogen activator; JGH: Jugal General Hospital; LMICs: low- and middle-income countries; mRS: modified Rankin score; SSA: sub-Saharan Africa; TIA: transient ischemic attack; WHO: World Health Organization.
Ethical considerations
The study was carried out under consideration of the Helsinki Declaration of Medical Research Ethics.39 This work was approved by the Institutional Health Research Ethical Review Committee of Haramaya University College of Health and Medical Sciences (Ref. No. IHRERC/175/2024). The administration of Haramaya University College of Health and Medical Science granted permission. Patients’ MRN numbers were locked for confidentiality, and their names were not registered in the checklist.
Consent to Participate
Because the study was retrospective, the need for written informed consent to participate was waived by the Institutional Health Research Ethical Review Committee of the Haramaya University College of Health and Medical Sciences. Data were accessed from July 15 to August 1, 2024
Author contributions
AT*, BS, AG, and MS were involved in the conception and design, acquisition of data, or analysis and interpretation of data. OK contributed to data analysis, writing, and editing the document. DF gave valuable ideas for the manuscript and revised it critically for important intellectual content. Finally, all authors read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Most of the data generated or analyzed during this study are included in this article. The full datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.