
Abstract
Background:
Venous thromboembolism is the third most common cause of cardiovascular death and is responsible for more than 3 million deaths annually worldwide. Despite high rates of morbidity and mortality associated with venous thromboembolism, limited studies have been conducted on in-hospital mortality and its associated factors in Ethiopia, particularly in study settings.
Objective:
To assess in-hospital mortality and associated factors among patients admitted with venous thromboembolism at selected public hospitals of Harar town, Eastern Ethiopia, from 10 March 2018 to 8 March 2022.
Methods:
A retrospective cohort study design was conducted among 502 patients admitted with venous thromboembolism at Hiwot Fana Comprehensive Specialized Hospital and Jugal General Hospital using a simple random sampling technique. Data extraction formats were used to collect data from patient medical record cards. Then data were coded and entered into EpiData version 3.1 computer programs and exported to SPSS version 26 for analysis. Bivariate and multivariate backward Cox regression analysis was used to verify the associated factors of in-hospital mortality among venous thromboembolism patients. A p-value of less than 0.05 at a 95% confidence interval was used to establish a statistically significant association.
Results:
A total of 502 patient medical record cards with outcome variables were included in the study. More than half of the patients 350 (69.7%) were females. Among the 502 patients who were admitted with venous thromboembolism, 8.2% (95% CI: 5.6–10.6) of patients had in-hospital mortality. DM (AHR = 4.28, 95% CI: 1.80–10.15, p = 0.001) and unfractionated heparin duration (AHR = 10.26, 95% CI: 2.45–43.01, p = 0.001) were statistically significant association with venous thromboembolism mortality.
Conclusion:
Approximately 8.2% of venous thromboembolism patients died in the hospital. Diabetes and heparin were independently associated with higher mortality. Therefore, it is better to give more attention to the patients co-morbid with diabetes mellitus and for unfractionated heparin treatment duration to reduce venous thromboembolism mortality.
Introduction
Venous thromboembolism (VTE) is the term used to describe the formation of a blood clot in a deep vein. It can manifest as post-thrombotic syndrome, pulmonary embolism (PE), or deep vein thrombus (DVT). 1 DVT typically begins in the calf veins and may progress to the proximal veins before breaking free to cause PE. 2 In addition to determining how quickly and how severe the patient’s symptoms show, the degree or severity of the thrombosis or embolism also determines the size and extent of the ensuing occlusion, the presence and patency of any collateral veins, and the presence of inflammation. 3 A typical and potentially fatal venous thromboembolic condition is PE, 4 and in this case, a thrombus from a deep leg or pelvic vein obstructs one or more pulmonary arteries, reducing blood flow and increasing pressure in the right ventricle. 5 PE may be asymptomatic or manifest with recognizable symptoms including tachycardia, dyspnea, chest discomfort, hypoxemia, and shock that are nonspecific and occur in several other illnesses, such as acute myocardial infarction (MI), congestive heart failure, or pneumonia. 6 Three broad categories, known as “Virchow’s triad,” can be used to categorize risk factors for VTE: those that increase venous stasis, those that promote blood hypercoagulability, and those that promote endothelial injury or inflammation. 7 Increasing age, prolonged immobility, malignancy, major surgery, multiple trauma, prior VTE, and chronic heart failure have all been shown to be risk factors for VTE. 8
The cornerstone of treating VTE is anticoagulant therapy. Two stages comprise such a treatment: Rapid initial anticoagulation is used to reduce the risk of thrombus extension and fatal PE, while extended anticoagulation is used to prevent recurrent VTE and lower the risk of postphlebitis syndrome. 9 Due to its convenience of administration (once daily vs 2–3 times daily) and lower risk of DVT, LMWH is recommended for unfractionated heparin (UFH). UFH is utilized in patients with low glomerular filtration rate; the prophylactic dosage is typically 5000 units administered subcutaneously twice or three times per day. 1 Unfractionated heparin is given as an initial bolus dose followed by a continuous infusion starting after thrombolysis has been examined in combination with the currently approved thrombolytic regimens for the treatment of acute PE. 10 Acute DVT is treated for 5–7 days as an inpatient in an Ethiopian hospital. 11 A weight-based parenteral anticoagulant is started at first. Due to cost and availability, UFH is typically preferred to low-molecular-weight heparin–like enoxaparin (except in specified cases). The only regularly obtainable oral anticoagulant, warfarin, will be added to the parenteral regimen after 24–48 hours. When the international normalization ratio (INR) falls within the advised limits of 2–3, the parenteral regimen will be stopped for the remaining 5–7 days. 12
VTE is the third most common cause of cardiovascular death, following acute coronary artery disease and stroke, and is responsible for more than 3 million deaths per year worldwide. 13 VTE represents a major public health problem that affects 350,000–600,000 Americans annually. Estimates vary widely, but the overall annual prevalence was increasing. 14 A modeling study estimated 370,000 deaths annually in Europe, with 7% diagnosed ante mortem, 34% sudden fatal PE not diagnosed ante mortem, and 59% following undiagnosed PE. 15 The prevalence of DVT varied between 2.4% and 9.6% in postoperative patients and the prevalence of VTE and associated mortality were high following surgery and in pregnant and postpartum women in Africa. 16 Symptomatic VTE is associated with extended duration of inpatient stays and high (10%–15%) fatality rates. 17 It is a serious condition with an incidence of 10%–30% of people dying within 1 month of diagnosis and one-half of them have long-term complications. The mortality rate is high, hospitalizations are frequent and associated with worse outcomes with high use healthcare costs. 18 Around the world, thrombosis-related disorders account for one in four fatalities. 19 The United States of America and Europe account for the majority of global and regional statistics on VT-related deaths and impairments. Every year, more than 2 million people in the USA alone suffer from DVT. 20
According to a study done in Addis Ababa, 95% of patients had lower limb DVT and 5% had upper limb DVT, indicating that VTE, particularly DVT is common in Ethiopia. 21 Therefore, given the increasing prevalence of several of the known risk factors, such as old age, immobility, surgery, and obesity, VTE is a serious and growing public health concern. Yet, until recently, this condition has received little attention from the public health community. Despite, the high rate of poor treatment outcomes of VTE, limited studies have been conducted regarding the assessment of treatment outcomes and associated factors with VTE in our country, particularly in the eastern part of Ethiopia. So the current study aimed to assess in-hospital mortality and its associated factors among patients admitted with VTE at public hospitals of Harar town, Eastern Ethiopia from 10 March 2018 to 8 March 2022.
Materials and methods
Study design, area, and period
A retrospective cohort study was conducted at Hiwot Fana Comprehensive Specialized Hospital (HFCSH) and Jugal General Hospital (JGH), Harar town, Eastern Ethiopia, which is located 526 km from Addis Ababa the capital city of Ethiopia. Harari regional state is one of the 10 states in Ethiopia, and it has a total population of 226,000 of those 114,000 are males, and the remaining are females. 22 This region is bounded by east, west, north, and south by the Oromia regional state. 23 There are 1 federal police, 2 public, and 2 private hospitals, 8 health centers (4 urban and 4 rural), 24 health posts, and 10 nonprofit clinics in this region. 24 One of the public hospitals is HFCSH, which is a teaching hospital of Haramaya University and serves as a referral hospital for the entire Eastern part of Ethiopia including Eastern Oromia, Dire Dawa City Administration, Somali Regional State, and Harari Regional State. In both hospitals, there are different wards and clinics, including an internal medicine (medical) ward, surgery ward, pediatric ward, gynecology and obstetrics ward, antenatal clinic, dental clinic, tuberculosis clinic, anti-retroviral therapy clinic, dermatology clinic, and an ophthalmologic clinic. This study was conducted from 10 March 2022 to 8 April 2022.
Study population
All patient medical records at HFCSH and JGH who were diagnosed with VTE represented the source population. Patients with a diagnosis of VTE were admitted to HFCSH and JGH who fulfilled the inclusion criteria of the study during the study period from 10 March 2018 to 8 March 2022, were the study population.
Eligibility criteria
Inclusion criteria
•All medical record cards of patients aged ⩾18 years old admitted with proven VTE, treated with an anticoagulant, and admitted to medical wards of HFCSH and JGH during the study period from 10 March 2018 to 8 March 2022, were included. An established DVT diagnosis confirmed by leg veins Doppler Ultrasound and PE diagnosis confirmed by CT scan of the chest, or echocardiography result in the patient chart were included.
Exclusion criteria
• Those medical record cards with incomplete information on treatment and patients with unknown treatment outcomes (referred and self-discharged) were excluded.
• Patient’s medical record cards that started anticoagulants for the prophylaxis purpose were excluded from the study.
Sample size determination and sampling procedures
To determine the sample size for this study, the outcome variable and factors that were significantly associated with the outcome variable were considered. The sample size for specific objectives was calculated separately by adding 10% contingency and the one with the largest number was considered for this study.1,4,25–27 Among the calculated sample, 502 was the largest, and considered as the final sample size.
Medical record cards of patients admitted with VTE at the medical wards of HFCSH and JGH between 10 March 2018 and 8 March 2022 were reviewed and identified from the patient registration book. Then patient’s medical record card numbers were registered and entered into a computer program (Microsoft Excel). Finally, the study unit was selected using the proportionally allocated simple random sampling technique (lottery method) (Figure 1).

Sampling procedure of patients with VTE at the medical ward of HFCSH and JGH, Harar, eastern Ethiopia, 2022 (n = 502).
Data collection tool, collectors, and procedure
The data abstraction sheet was prepared by reviewing previous studies in consideration of the objective of this study.25,28–32 The data collection tool contains two subsections; the first section contains the sociodemographic (age, sex, and residence) of the patients while, the second section contains clinical characteristics, laboratory findings, medications given to the patient, and outcomes of treatment. Data were collected from the medical record cards of the patients using a data abstraction sheet by six pharmacists.
Variables of the study
Dependent variable
• In-hospital mortality.
Independent variable
• Sociodemographic characteristics of the patients (age, sex, and residence)
• Comorbidity: TB, MI, CHF, CKD, DM, PVD, stroke, anemia, liver disease, cancer
• Clinical characteristics: Lower limb amputation, BMI, surgery, pregnancy
• Laboratory findings (CBC and D-dimer)
• Medication prescribed (name of the drug, dose, route, frequency of administration, and duration).
Operational definitions
Hospital death was defined as patients who died during a hospitalization episode, independent of the death cause. 33
Bleeding is defined as clinical status, laboratory, and/or imaging evidence of bleeding from internal or external body as a result of anticoagulant therapy. 34
Comorbidity the presence of one or more additional concomitant diseases or disorders co-occurring with DVT. 13
Improved VTE adequate progress is being made toward achieving the prevention of the extension and recurrence of thrombosis at this point.
Data quality control
To maintain the quality of data the following strategies were applied: data collection tool was developed by reviewing related studies. Then pretest was done on 5% of the calculated sample size at Dil Chora Referral Hospital (other than the study cite) to ensure clarity, avoidance of ambiguity, comprehensiveness, and content uniformity of the data collection tool. Before beginning the data collection process, data collectors were given half-day training on the importance, objectives, and method of data collection by the principal investigator.
Data processing and analysis
Data were coded and entered into EpiData version 3.1 computer programs (a global privately-owned company specialized in innovation outsourcing, dedicated to providing software development and software design services, application modernization, robotic process automation, machine learning and big data). Then exported to Stastical Package for Soscial Science (SPSS) version 26 for analysis which is manufactured by International Business Machines Corporation a an American multinational technology company headquartered in Armonk, New York. Descriptive statistics were conducted by using frequencies and cross-tabulation. For the purpose of analysis, the outcome variable was classified as improved and died. Then, Kaplan–Meier survival analysis method was used to predict the probability of death over follow-up time. Cox regression was used to identify factors associated with in-hospital mortality. Variables with p ⩽ 0.25 were considered as cut-off points to select candidate variables in binary Cox regression. Multivariable Cox regression with a backward stepwise approach was used to identify factors associated with VTE mortality. Variables with a p-value of less than or equal to 0.05 were declared significantly associated with in-hospital mortality in multivariable Cox regression analysis. The adjusted hazards ratio (HR) with a 95% confidence interval (CI) was used to express the association between the in-hospital mortality and the independent variables.
Results
Sociodemographic characteristics of patients
This study included 502 patients. Of these, 350 (69.7%) were females. The patients’ ages ranged from 18 to 85 years, with a mean ± SD of 39.72 ± 19.48 years. Less than half of the patients 227 (45.2%) were between the ages of 18 and 34 years. Among the total study participants, three-fourths (75.9%) were urban residents (Table 1).
Baseline sociodemographic characteristics of patients with VTE at the medical wards of HFCSH and JGH, Harar, eastern Ethiopia, 2022.

HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital.
Clinical characteristics and laboratory results of VTE patients
As shown in Table 2, of 502 patients, 496 (98.8%) were admitted with DVT, while the others were admitted with PE (1.2%) as a result of DVT complication, which was confirmed by CT-scan. About 461 (91.8%) patients were found to have unilateral thrombosis, and only 41 (8.2%) patients had combined involvement of bilateral VTE. This study also showed that 496 (98.8%) patients had lower extremity involvement. The majority of Doppler ultrasonography examinations proved DVT cases 271 (54.7%) were proximal. Out of the 502 patients with VTE, 284 (57.3%) had involvement of the left lower-limb extremities. Regarding clinical presentation, about 98.4% of patients presented with pain, and 98.0% of them had swelling with the affected limbs on admission. Regarding the coagulation profile, the Mean ± SD result of activated partial thromboplastin time (aPTT) was 38.93 ± 20.120 s at baseline and INR was 1.834 ± 0.617 at baseline (Table 3).
Baseline clinical characteristics of patients with VTE at the medical wards of HFCSH and JGH, Harar, eastern Ethiopia, 2022.

HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital; DVT: deep venous thrombosis; VTE: venous thromboembolism.
Baseline laboratory tests and other data during hospital stay of patients with VTE at the medical wards of HFCSH and JGH, Harar, eastern Ethiopia, 2022.

HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital; DVT: deep venous thrombosis; VTE: venous thromboembolism.
VTE risk assessment and comorbidity among VTE patients
The majority of study participants (92%) presented with known risk factors. Prolonged immobilization accounted for 227 (45.2%) of the VTE risk assessment in the study population. Combined major medical conditions such as metabolic diseases, endocrine diseases, respiratory diseases, acute infectious disease, and inflammatory conditions (arthritis), were presented in 115 (22.9%) of the patients. In terms of the burden of risk factors among study participants, the majority of patients 286 (61.9%) had only one risk factor for VTE (Table 4). In addition, more than half study participants 336 (66.9%) had comorbidities. Anemia accounted for 124 (24.7%) of the VTE comorbidity in the study population (Table 5).
Risk factors of venous thromboembolism among patients admitted at medical wards of HFCSH and JGH, Harar, eastern Ethiopia, 2022 (n = 462).

HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital.
Comorbidity presenting with VTE among patients at the medical ward of HFCSH and JGH, Harar, eastern Ethiopia, 2022 (n = 336).

HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital.
Chronic lung diseases, hypertension, and acute infectious disease.
Medications prescribed for VTE patients and duration of anticoagulant therapy for hospitalized VTE patients
The majority 485 (96.6%) of study participants were administered unfractionated heparin during their admission, warfarin was prescribed for 471 (93.8%) and of which around 17 (3.4%) patients were treated with LWMH (enoxaparin). Co-administered drugs were prescribed for more than half (66.7%) of patients who were taking iron products (Table 6). Besides, the majority of study participants 463 (95.5%) took heparin for 5–10 days, while around 28.2% of study participants took warfarin for more than 30 days (Table 7).
Duration of anticoagulant therapy among patients with VTE at the medical ward of HFCSH and JGH, Harar, eastern Ethiopia, 2022.
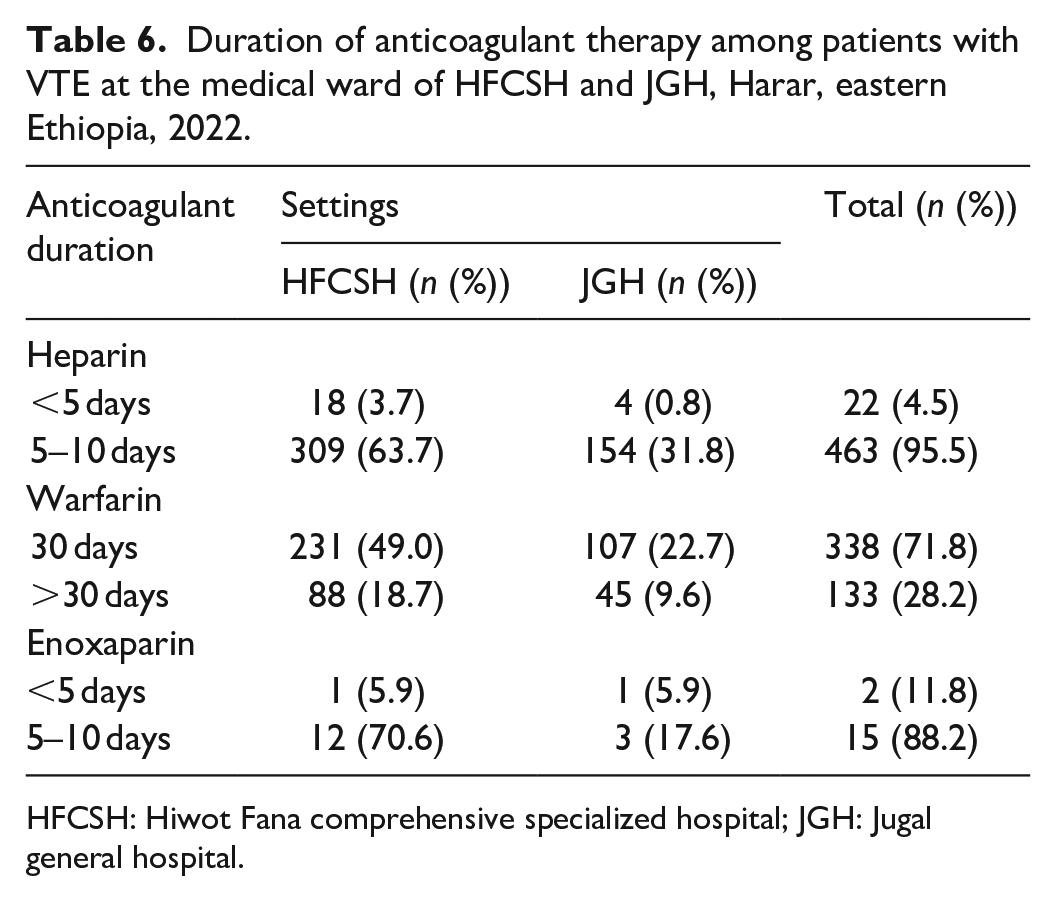
HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital.
In-hospital medications used among patients with VTE at the medical ward of HFCSH and JGH, Harar, eastern Ethiopia, 2022 (n = 502).

HFCSH: Hiwot Fana comprehensive specialized hospital; JGH: Jugal general hospital.
Antibiotics, vitamins and minerals, diuretics, and antidepressants.
In-hospital mortality and overall survival rate of VTE patients
The finding of this study showed that the overall in-hospital mortality was 8.2% (Figure 2). The study samples were followed for a minimum of 1 day and a maximum of 20 days with an estimated mean survival time of 9.415 (95% CI: 7.99–10.83) days and an estimated median survival time was 9.00 (95% CI: 7.74–10.25) days. The survival probability was highest in the first days of follow-up after a VTE was diagnosed, and then it relatively decreased as the follow-up time increased (Figure 3). The cumulative survival time to VTE mortality was lower for patients with diabetes comorbidity (Figure 4) and heparin duration of 5–10 days (Figure 5).
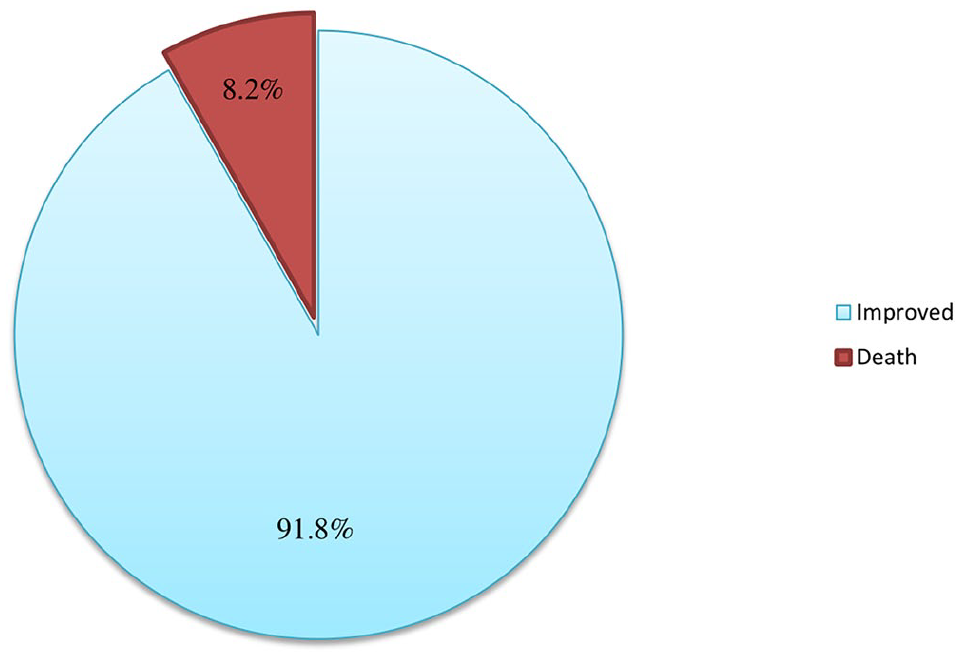
In-hospital mortality among patients with VTE at the medical ward of HFCSH and JGH, Harar, eastern Ethiopia, 2022.

Overall Kaplan–Meier estimation of survival functions of VTE patients in HFCSH and Jugal General Hospital, eastern Ethiopia, 2022.

Survival function estimates of cumulative incidence of VTE mortality event for diabetes comorbidity.

Survival function estimates of cumulative incidence of VTE mortality event for Heparin duration.
Factors associated with in-hospital mortality
In the bi-variable Cox regression analysis, five variables (cancer, DM, Pitting edema, prolonged immobility, and heparin duration) were identified for further analyzing predictors of mortality at p ⩽ 0.25. The multivariate Cox regression analysis showed just two factors as linked with mortality. Diabetes mellitus (AHR = 4.28, 95% CI: 1.80–10.15, p = 0.001) and heparin duration (AHR = 10.26, 95% CI: 2.45–43.01, p = 0.001) (Table 8).
Bivariate and multivariate Cox regression analysis of factors associated with in-hospital mortality among hospitalized VTE patients at HFSUH and Jugal General Hospital, eastern Ethiopia, 2022.

Bold: significant association
Discussion
The finding of this study showed that the overall in-hospital mortality was 8.2%. Diabetes and heparin were independently associated with higher mortality.
The magnitude of in-hospital mortality was 8.2% (95% CI: 5.6–10.6). This finding was lower than studies done in Korea (24.6%) 35 and in Denmark (40%). 36 However, higher than another study conducted at hospitals in China (2.1%), 37 and Saudi Arabia (1.9%). 38 This contradiction might be due to differences in the care given in each setting, the nature of the study design (prospective), comorbidities, complications, and treatment approaches. Besides, mortality after VTE varies with advanced age, cardiovascular disease, underlying cancer, recurrent VTE, or other medical conditions representing important predictors of mortality. 36
The rate of in-hospital mortality in patients comorbid with diabetes mellitus was 4.28 times more than those patients without Diabetes mellitus. This was comparable with the study done in Ethiopia at Jimma and Addis Ababa (8.04%). 13 However, this was higher as compared to studies done in Germany (1.21%) 39 and Sweden (1.49%). 40 The association between vascular complications from diabetes and decreased peripheral circulation results in distal ischemia. Theoretically, hyperglycemia contributes to elevated coagulation factors, impaired fibrinolysis, and increased likelihood of thrombosis. Also, high plasma glucose levels increase oxidative stress, which in turn increases gene transcription of coagulation factors, degrade the glycocalyx layer of the endothelial wall, which releases coagulation factors and stimulates the coagulation cascade, and increase glycation of proteins involved in coagulation and fibrinolysis, shifting their activity toward a procoagulant state. 41 These pathophysiologic conditions might challenge the anticoagulant treatment outcomes implicating appropriate glucose control is important.
The hazards of in-hospital mortality were 10.26 times more likely among patients taking unfractionated heparin for 5–10 days than those <5 days. This was consistent with a study done in the USA (6.7%). 29 However, it was higher than another study done in Michigan (2.1%). 42 The timing of initial heparinization and achieving therapeutic anticoagulation relate to mortality. Rapid initiation of treatment helps to curb fibrin clot formation and augment the body’s fibrinolytic response, thereby reducing symptoms and risk of further thrombus formation or progression to PE. Heparin is not thrombolytic, but rather it prevents clot propagation and recurrent VTE. 29 The short-course regimen has obvious appeal, reducing hospital stay and the risk of heparin-induced thrombocytopenia (HIT). Although a shorter course of treatment can be recommended for most patients with VTE, this may not be appropriate in cases of extensive iliofemoral vein thrombosis or major PE. 43
Conclusion and recommendation
This study found that nearly 8.2% of patients with VTE had in-hospital mortality. Diabetes and heparin were independently associated with higher mortality. Therefore, it is better to give more attention to the comorbid with diabetes mellitus and to unfractionated heparin treatment duration to reduce the mortality of these populations. Moreover, researchers strongly recommended doing further studies on VTE treatment outcomes and associated factors of VTE in Ethiopia because there are only a few published studies in the country.
Strength and limitation of the study
The main strength of this study was being the first research that reported the treatment outcomes and associated factors of VTE in the two large centers in the study area. This study included a relatively large sample size compared with other studies that assessed VTE treatment outcomes. Due to the retrospective nature of the data, we were unable to assess VTE complications (bleeding) and behavioral factors (smoking, alcohol use, and medication adherence) reported directly by the patient that might influence the direction of the treatment outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241266360 – Supplemental material for In-hospital mortality and associated factors among patients admitted with venous thromboembolism at selected public hospitals of Harar Town, Eastern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121241266360 for In-hospital mortality and associated factors among patients admitted with venous thromboembolism at selected public hospitals of Harar Town, Eastern Ethiopia by Dawit Abraham, Kirubel Minsamo Mishore, Shambel Nigussie, Abera Jambo and Tigist Gashaw in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank the management and card room staff at Hiwot Fana Specialized University Hospital and Jugal Hospital for their cooperation during data collection.
Authors’ contribution
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis, and interpretation. All took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, and agreed on the journal to which the article was to be submitted.
Data availability statement
All relevant data that support the findings of this study are included in the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial supportfor the research, authorship, and/or publication of this article.
Ethical consideration
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee with the reference number of IHRERC/3688/22 Haramaya University, College of Health and Medical Sciences (CHMS). Official letters of cooperation to conduct the study were presented to HFSUH and JGH. The purpose of the study and method of data collection was communicated to the concerned body.
Informed consent
Informed, voluntary, written, and signed consent was obtained from each hospital administrator before the data collection. The information obtained from patient medical record cards was kept confidential, and the name of the patient and other information that specifically identified the patient were not recorded.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.