
Abstract
Background:
Cholera remains a persistent public health challenge in low-resource settings, where effective multi-sectoral coordination and meaningful community engagement are often limited. This cross-sectional study examined the socioeconomic and contextual factors influencing community participation during a recent cholera outbreak in Ethiopia’s Sidama Region. The study assessed levels of involvement across preparedness, response, and recovery phases to inform context-specific strategies.
Methods:
A community-based cross-sectional survey was conducted between June and August 2023 among 613 residents in the Sidama Region following a cholera outbreak. A structured checklist assessed sociodemographic characteristics, knowledge, attitudes, practices, and engagement in preparedness, detection/response, and recovery activities. Logistic regression analysis was used to identify factors associated with low engagement.
Results:
Engagement was measured using Likert-scale items across preparedness, surveillance, response, and coordination domains. The overall community engagement index was 48%, indicating that fewer than half of participants were actively involved in outbreak management. Key barriers included poor socioeconomic status (33%), large household size exceeding four members (82%), and low educational attainment, with 27% having no formal education. Low engagement was significantly more likely among participants with poor wealth status (AOR 2.98), households with three or more children under 5 years (AOR 12.6), individuals with poor knowledge of cholera (AOR 2.51), and males compared to females (AOR 1.87).
Conclusion:
Community engagement in the cholera outbreak response was suboptimal. Poverty, large household, and low educational attainment were the principal barriers. Addressing these constraints is essential to strengthen early detection, improve response effectiveness, and sustain cholera control through enhanced community involvement.
Introduction
Cholera remains a major global public health challenge, affecting over one-third of countries worldwide 1 and leading to an estimated 2.9 million cases and 95,000 deaths annually,1,2 with the greatest burden in sub-Saharan Africa. The populations most at risk include those with low socioeconomic status, refugees, and communities lacking access to safe water and proper sanitation infrastructure.3–6 Although cholera’s impact is widespread, it is particularly severe in endemic regions like Ethiopia, where recurrent outbreaks persist due to challenges in coordinating cross-sectoral efforts and a lack of community support for outbreak control. 7 The continued prevalence of the disease is largely due to difficulties in reaching vulnerable populations with proven prevention and containment strategies. Addressing this issue requires multisectoral coordination to improve local water, sanitation, and hygiene conditions, alongside enhanced community engagement in preparedness, early detection, response, and recovery efforts,7–12 These efforts must be tailored to the specific needs and barriers faced by at-risk communities to ensure effective engagement and control of cholera outbreaks.
Research has shown that communities actively involved in emergency preparedness, response, and recovery are more effective in managing crises through locally led initiatives.13–15 For example, a study in the Philippines found that communities with high levels of engagement in disaster preparedness activities such as risk mapping, early warning systems, and evacuation planning had significantly lower mortality rates (0.2%) during typhoons compared to less engaged communities (1.8%). 4 Successful emergency programs integrate preparedness, response, and recovery efforts, with preparedness serving as the cornerstone. 16 However, assessments in Ethiopia, Kenya, and Malawi have highlighted insufficient community engagement in preparedness as a barrier to local resilience.16,17 A joint evaluation by United Nations Children’s Fund (UNICEF) and the World Food Program (WFP) in Ethiopia revealed that only 25% of communities had functional early warning systems, and less than 15% had participated in risk mapping exercises. 5 In Malawi, research indicated that just 30% of households had emergency preparedness plans, and under 20% had received training on emergency response. 6 Additionally, studies emphasize the critical role of community engagement in public health emergency management.8,9 Communities actively participating in recovery efforts, such as debris removal, shelter construction, and livelihood restoration, reported higher resilience and quicker recovery times. 10 Conversely, inadequate community engagement can lead to a lack of awareness, preparedness, and ownership of emergency plans, resulting in greater vulnerability and slower recovery times. 7 According to established cholera management guidelines, individuals with suspected cholera symptoms are advised to seek immediate professional medical treatment at a health facility. 18
While previous research has highlighted the importance of community engagement in emergency preparedness, response, and recovery, there is limited evidence specifically examining engagement levels and influencing factors during cholera outbreaks in high-burden countries like Ethiopia. Most studies have focused broadly on disaster risk reduction rather than the distinct phases of epidemic management. Furthermore, there is a lack of local data identifying the barriers and facilitators that impact community engagement in cholera control efforts within vulnerable populations in endemic regions. This study aims to address these gaps by thoroughly assessing community engagement across preparedness, detection, response, and recovery phases during a recent cholera outbreak in Ethiopia’s Sidama Region. By evaluating engagement levels and exploring the roles of socioeconomic, demographic, and health system factors, the findings provide valuable insights for developing tailored strategies that foster meaningful community involvement and ownership, thereby enhancing outbreak resilience in at-risk areas.
Methods
Study design, area, and periods
A community-based, cross-sectional study was conducted to assess the levels of community engagement in cholera outbreak management in Ethiopia’s Sidama Region. This design enabled the simultaneous collection of engagement indicators through quantitative surveys.
The study was conducted in the Sidama Region, located in southern Ethiopia, which was intentionally selected due to its history of recurrent cholera outbreaks, active surveillance systems involving healthcare facilities and communities, and the need for a thorough assessment of regional outbreak preparedness and response efforts. The research took place between June and August 2023, utilizing field data collection methods, including quantitative questionnaires. This period coincided with the peak of the ongoing cholera outbreak in the region, providing an optimal context to evaluate community engagement in management activities and to gather insights from stakeholders on the factors influencing engagement.
Study population and sampling method
The target population for this study consisted of community members residing in the Sidama Region, Ethiopia, an area prone to recurrent cholera outbreaks. A multistage cluster sampling technique was used to select a representative sample from the population. According to local health records, the Sidama Region comprises 38 districts. From this sampling frame, eight priority districts with a history of repeated outbreaks were chosen. Within each district, three kebeles (villages) were randomly selected, resulting in 24 primary sampling clusters. Subsequently, two sub-clusters were randomly identified within each kebele by listing households and systematically sampling every second residence.
This process resulted in the creation of 48 subclusters across eight districts. Individuals aged 18–60 years residing in the selected households within these subclusters were invited to participate in face-to-face interviews. Data collectors visited the identified households and conducted interviews with the selected individuals. If a selected household was not available after repeated visits, the nearest neighboring household was approached as a direct substitute to maintain the required sample size for that subcluster. Each replacement was one-to-one and did not alter the number of households sampled within any subcluster.
The multi-stage cluster design allowed for intra-kebele comparisons, which are crucial for assessing targeted engagement strategies in areas with repeated outbreaks. The detailed sampling frames, along with the selection process for districts, villages, and subclusters, highlight the study’s rigorous design and enhance the generalizability of the findings to the broader study population.
Eligibility criteria
Individuals were eligible to participate if they were permanent residents of the selected households in the study area, aged 18–60 years, and present at the time of data collection. Individuals who were severely ill, unable to communicate, or unwilling to provide informed consent were excluded from the study.
Sample size determination
To determine an appropriate sample size, a review of similar studies assessing community engagement in public health emergencies was conducted. Prevalence estimates of key engagement indicators from three comparable studies in sub-Saharan Africa ranged between 30% and 60%. Given the differences in scope and setting between the current outbreak response and previous research, a more conservative prevalence estimates of 40% was chosen to calculate the required sample size. 19 This resulted in a minimum sample size of 605 participants. A design effect of 1.5 was applied to account for the multistage cluster sampling approach, which introduces intra-cluster correlation and reduces the statistical independence of observations. After applying this adjustment, the final sample size was 634 participants.
Variables
The primary outcome variable of this study was the level of community engagement in cholera outbreak management, defined as participants’ involvement across preparedness, surveillance, response, and coordination activities. Community engagement was measured using a composite engagement index and categorized as good or poor based on the predefined scoring criteria.
The main independent variables included socio-demographic characteristics (age, sex, educational status, household size, number of children under 5 years, and wealth index), knowledge-related factors (knowledge of cholera transmission, symptoms, risks, and prevention), attitudinal factors (perceived severity of cholera and prevention beliefs), behavioral factors (prevention practices, hygiene behaviors, exposure to media information sources), and health service-related factors (access to clean water, medication availability, healthcare access, exposure to health education, and sources of health information).
All variables were defined a priori based on the study objectives and existing literature on community engagement and public health emergency management and were operationalized through a structured interviewer-administered questionnaire.
Data collection instrument
The survey instrument gathered data on various socio-demographic, sociocultural, and behavioral factors that were hypothesized to influence community engagement in cholera prevention and control efforts. Socio-demographic variables included participants’ age, sex, and education level. 20 Sociocultural factors assessed included beliefs about the severity of cholera 21 as well as knowledge of cholera transmission, symptoms, risks, and prevention methods Behavioral factors measured included exposure to media information sources 22 and self-reported hygiene practices, such as water treatment and handwashing 23 (Supplemental File 1).
To assess community engagement, we utilized a combination of Likert scale and dichotomous response questions. The Likert scale questions measured the frequency of activities on a 5-point agreement scale, while the dichotomous questions used yes/no response options to evaluate specific engagement indicators. These questions were adapted from engagement measurement scales used in previous studies on public health emergency management, focusing on constructs such as participation in preparedness, surveillance, response, and coordination activities. Although the general constructs were based on validated research, the wording of individual questions and response scales was adjusted to ensure cultural and contextual relevance for this population and outbreak setting.
The questions were designed to capture participation in various aspects, such as attending meetings to assess preparedness, inquiring about formal reporting structures to evaluate surveillance, and asking about notifying health workers for response. By building on engagement measurement approaches from other contexts while tailoring the tool for local relevance, we aimed to reliably assess engagement levels specific to this outbreak, all while maintaining connections to established theoretical frameworks for the concept. 24
Furthermore, factors related to health service delivery, such as medication availability, healthcare access, and the source and coverage of health education, were assessed to better understand the current landscape. Questions were included to identify the main channels through which people receive cholera-related information, providing insights to guide outreach efforts. The questionnaire was pretested to ensure clarity, eliminate ambiguity, and confirm cultural appropriateness. Trained data collectors conducted the interviews in the local language to enhance understanding, creating a thorough yet culturally relevant data collection process. Data collection was carried out by eight trained data collectors supported by two supervisors. To minimize interviewer-related bias, data collectors were not restricted to a single kebele; instead, they worked across multiple sites, and supervisors rotated between locations to ensure consistency in procedures.
Data quality control process
To ensure the collection of high-quality data, a pre-test of the questionnaire was conducted on 5% of the sample size to evaluate the clarity, understandability, and comprehensiveness of the questions. Based on the results, necessary revisions were made to the questionnaire. Experienced data collectors and supervisors, each holding at least a BSc in health sciences, were recruited and underwent training. During this training, supervisors provided detailed guidance on each question explaining its meaning, how to ask it naturally in the local language, possible prompts, and proper recording methods. The training also included demonstrations of interviewing techniques and role-playing exercises to prepare the data collectors, allowing trainees to take notes on unfamiliar areas and have their questions addressed.
During the active data collection phase, the project team conducted daily checks of completed questionnaires to ensure completeness and consistency, promptly verifying any issues with the data collectors. This pre-testing of the tool, selection of an experienced data collection team, thorough training, and daily review of completed questionnaires with feedback contributed to the collection of high-quality data, ensuring reliable results and conclusions from the study.
Bias
Several measures were taken to minimize potential sources of bias. Selection bias was reduced through the use of a multistage cluster sampling approach and systematic household selection within clusters. Information and interviewer-related bias were minimized by using a pretested structured questionnaire, employing trained data collectors, conducting interviews in the local language, and rotating data collectors and supervisors across study sites. Daily supervision and review of completed questionnaires were performed to ensure consistency and completeness. To limit social desirability bias, participants were informed about the confidentiality of their responses and encouraged to provide honest answers. The reporting of this study conforms to the STROBE Statement for observational studies. The completed STROBE checklist is provided as Supplemental File S2.
Data Analysis
Data were entered into EpiData software and further analyzed quantitatively using Stata 18. Descriptive statistics, including tables, graphs, and charts, were employed to summarize the characteristics of the study participants. Binary logistic regression was used to identify factors associated with the outcome of interest. Variables with a p-value <0.2 were included in the multivariable logistic regression analysis. The crude odds ratio (COR) and adjusted odds ratio (AOR), along with their corresponding 95% confidence intervals, were calculated to determine the strength of the associations. In the multivariate analysis, variables with a p-value <0.05 were considered statistically significant. The model’s fitness was evaluated using the Hosmer-Lemeshow goodness-of-fit test.
Ethical clearance
The Institutional Review Board of St. Paulo’s Millenium Medical College approved this study (reference number PM 23/71, dated 26/7/2022). Participants provided written informed consent after being fully informed about the study procedures, potential risks, benefits, confidentiality, and their right to voluntarily participate or withdraw at any time. Data were anonymized by replacing personal identifiers with codes. Hardcopy data were securely stored in locked cabinets, while electronic files were encrypted and password-protected. Data were reported in aggregate form to ensure anonymity. There were no risks associated with participation, and participants had the option to refuse to answer any questions or withdraw from the study at any point. The potential benefits of contributing to improved programs and policies outweighed any minimal risks. The study adhered to ethical standards to protect the privacy, dignity, and welfare of participants, in accordance with relevant guidelines. The reporting of this study conforms to the STROBE Statement (Strengthening the Reporting of Observational Studies in Epidemiology) and the completed STROBE checklist is provided as Supplemental File 2.
Results
Sociodemographic characteristics
The study achieved a high response rate of 97%, with a total of 613 community members participating. The majority of participants were of working age, with over a third falling within the 31–40-year-old range. Slightly more than half of the sample were male. Education levels varied, but the majority had completed at least elementary school. The most common occupations among participants were housewife, farmer, student, and merchant (Table 1).
The sociodemographic characteristics of study participants status of community engagement in PHEM activities of cholera outbreak, 2023, Ethiopia.

Health and cholera related experiences
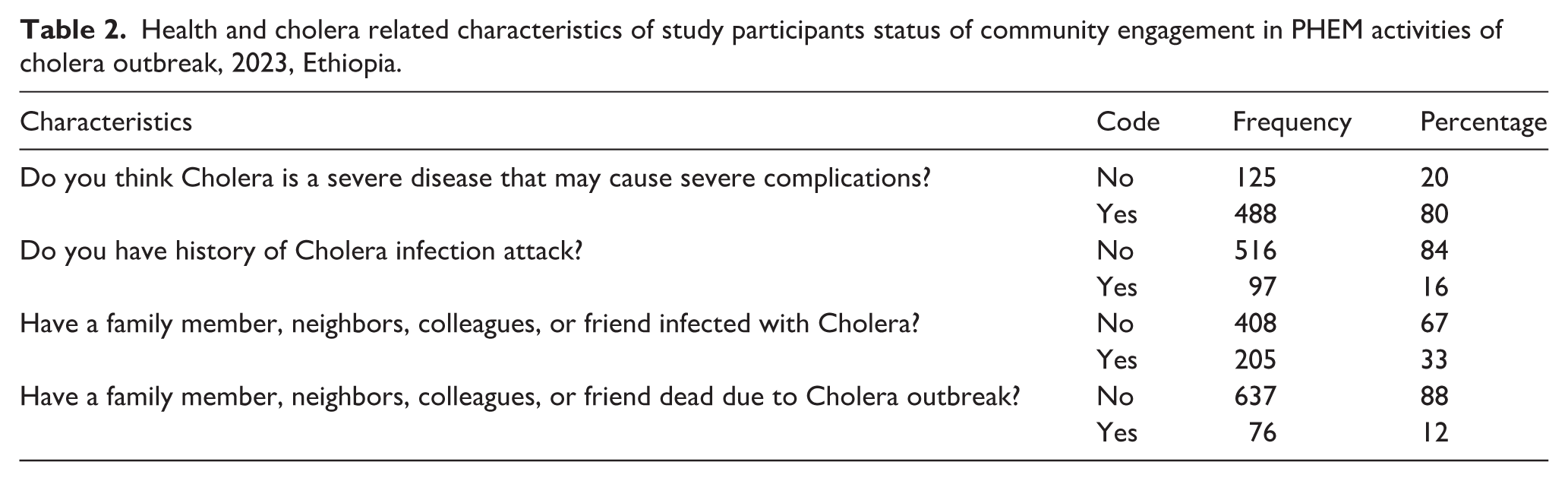
Among the participants, 80% believed that cholera is a severe disease capable of leading to serious complications. Additionally, 16% reported having a history of cholera infection themselves, while 33% indicated that a family member, neighbor, colleague, or friend had been infected with cholera (Table 2).
Health and cholera related characteristics of study participants status of community engagement in PHEM activities of cholera outbreak, 2023, Ethiopia.
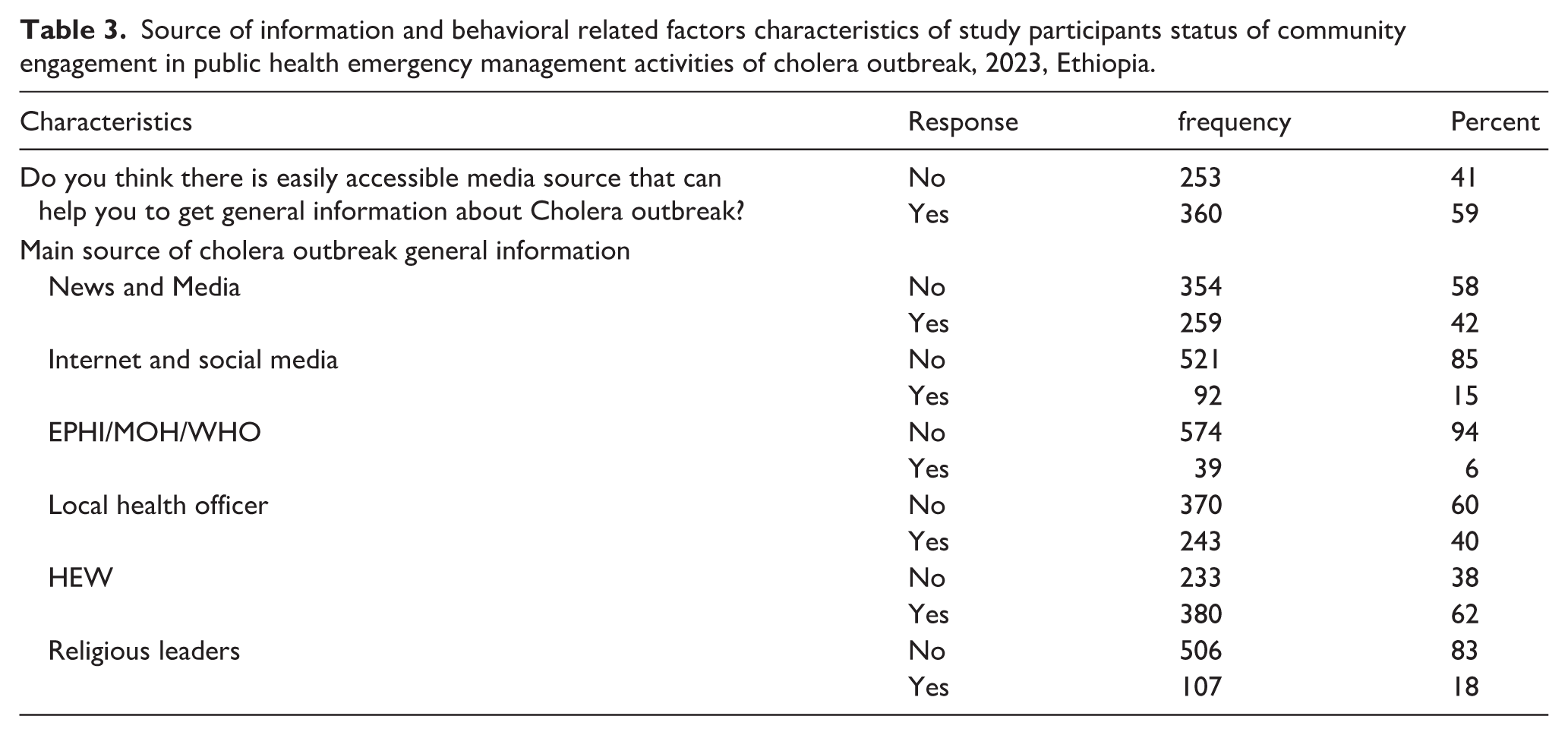
Among the study participants, 59% believed that there is an easily accessible media source to obtain information about the cholera outbreak. The main sources of information about cholera outbreak were news and media (42%), internet and social media (15%), EPHI/MOH (6%), local health officers (40%), health extension workers (62%), and religious leaders (18%; Table 3).
Source of information and behavioral related factors characteristics of study participants status of community engagement in public health emergency management activities of cholera outbreak, 2023, Ethiopia.
Community engagement in PHEM activities
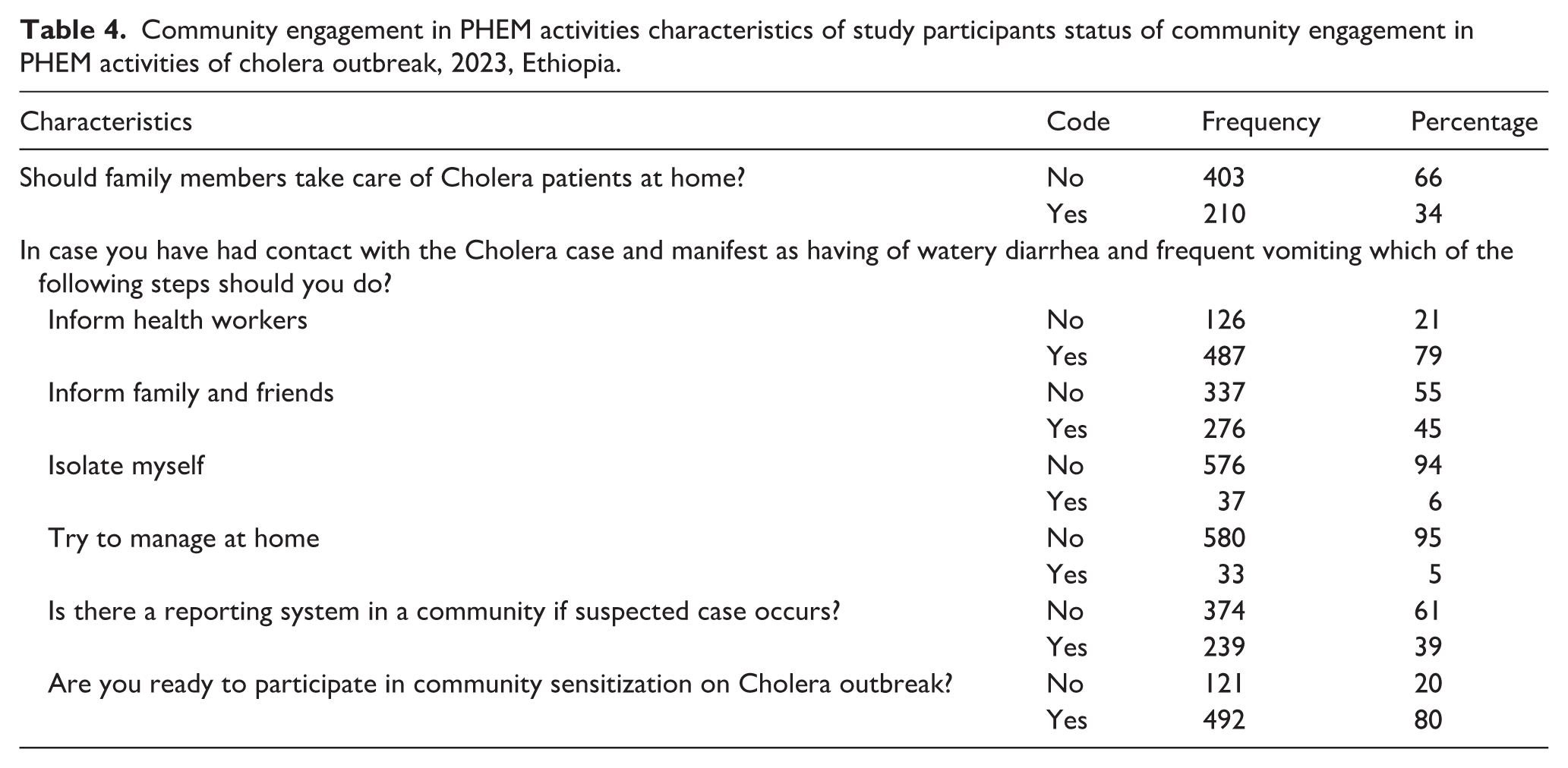
The study findings highlight concerning attitudes and potential poor behaviors related to community engagement in public health emergency management (PHEM) activities during cholera outbreaks. Notably, 34% of participants believe that cholera patients should be cared for at home by family members, rather than seeking professional medical care at health facilities. When asked about their intended actions if they came into contact with a cholera case and began experiencing symptoms like watery diarrhea and frequent vomiting, responses varied. While the majority (79%) said they would notify medical personnel, a significant portion (45%) indicated they would inform family and friends. Some participants expressed intentions to isolate themselves (6%) or attempt home treatment (5%) without seeking proper medical care (Table 4).
Community engagement in PHEM activities characteristics of study participants status of community engagement in PHEM activities of cholera outbreak, 2023, Ethiopia.
Cholera outbreak prevention instrument and health service-related factors
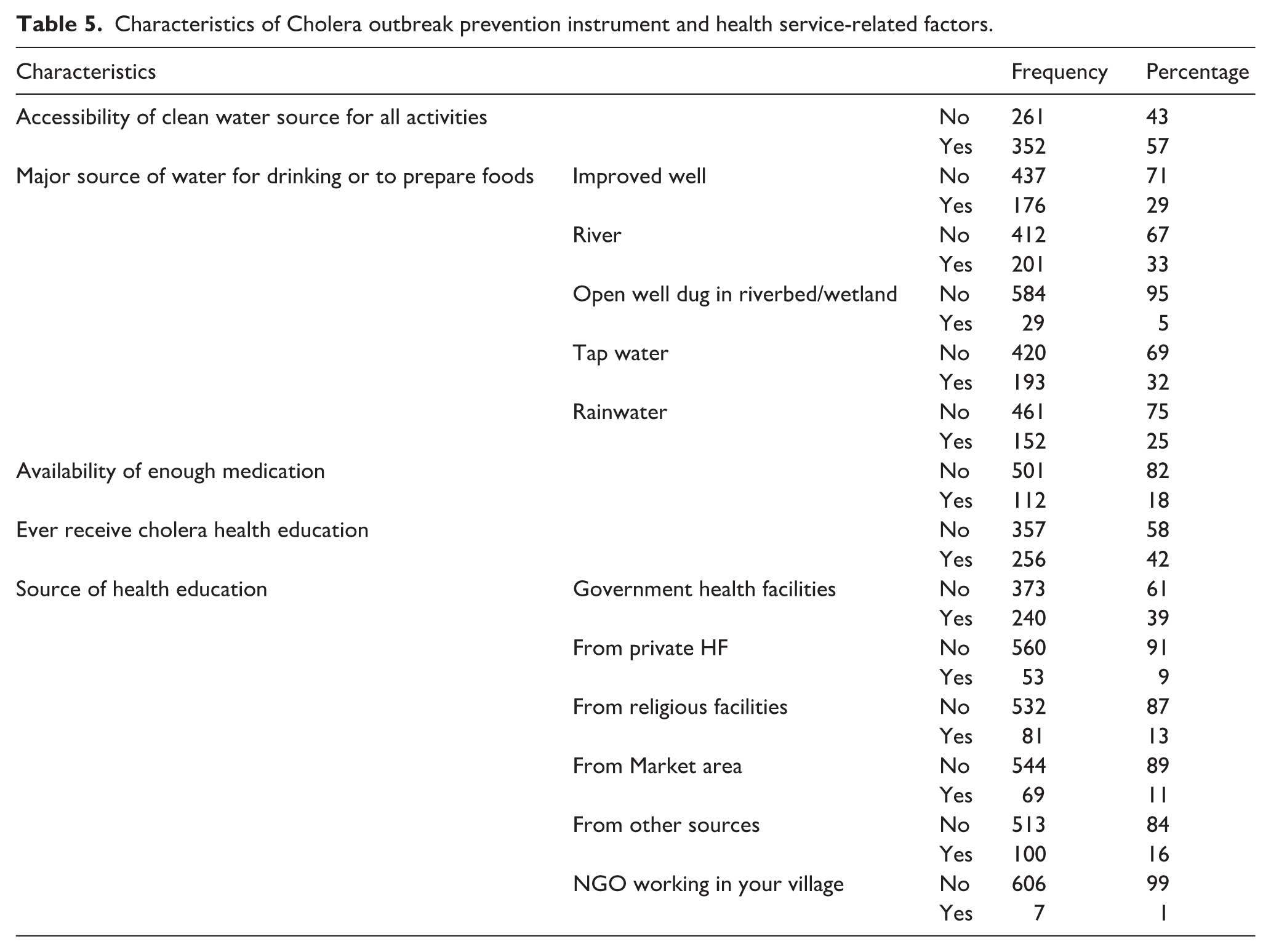
The findings indicate significant gaps in access to clean water and health services among the participants. A large proportion (43%) lacked access to clean drinking water, instead relying on sources such as rivers (34%), open wells (5%), and rainwater (25%). Medication availability was also limited, with only 18% reporting sufficient access to necessary medications. Health education efforts appeared insufficient, as only 42% had ever received cholera-related information. However, there was a substantial demand for knowledge, particularly regarding treatment (79%), transmission (67%), symptoms (49%), high-risk groups (45%), and available treatments (36%). In this study, ‘treatment’ refers to participants’ interest in information about cholera care, whereas ‘available treatments’ denotes the availability of essential cholera medications at nearby health facilities (Table 5).
Characteristics of Cholera outbreak prevention instrument and health service-related factors.
Level of community engagement
In this study, community engagement in managing cholera outbreaks was measured, revealing that 52% of participants were considered effective. This means slightly more than half of the community was effectively involved in preventing, preparing for, responding to, and recovering from cholera outbreaks. The confidence interval (95% CI: 48, 56) shows that the true level of effective engagement likely falls between 48% and 56%. On the other hand, 48% of community engagement was assumed inadequate, meaning almost half of the community’s engagement in cholera-related interventions was insufficient.
Bivariable and multivariable logistic regression toward level of community engagement
The bivariate logistic regression model identified several factors as candidates for the multivariable analysis, including wealth index, number of children under five in the household, prevention practices, level of knowledge, age, gender, and education level (p ≤ 0.20). In the multivariable model, poor and medium wealth status, having three or more under-five children, poor prevention practices, low knowledge levels, being male, and lower educational attainment were significantly associated with higher odds of poor community engagement.
The crude engagement proportions presented in Table 6 reflect unadjusted distributions and do not account for differences in knowledge, prevention practices, education, or household characteristics. These descriptive values should not be interpreted as determinants of engagement. The adjusted associations from the multivariable model provide the appropriate estimates after controlling for potential confounders.
Bivariable and multivariable logistic regression model to identify factors associated with level of community engagement toward cholera and COVID 19 disease preventions, preparedness, response, and recovery interventions.
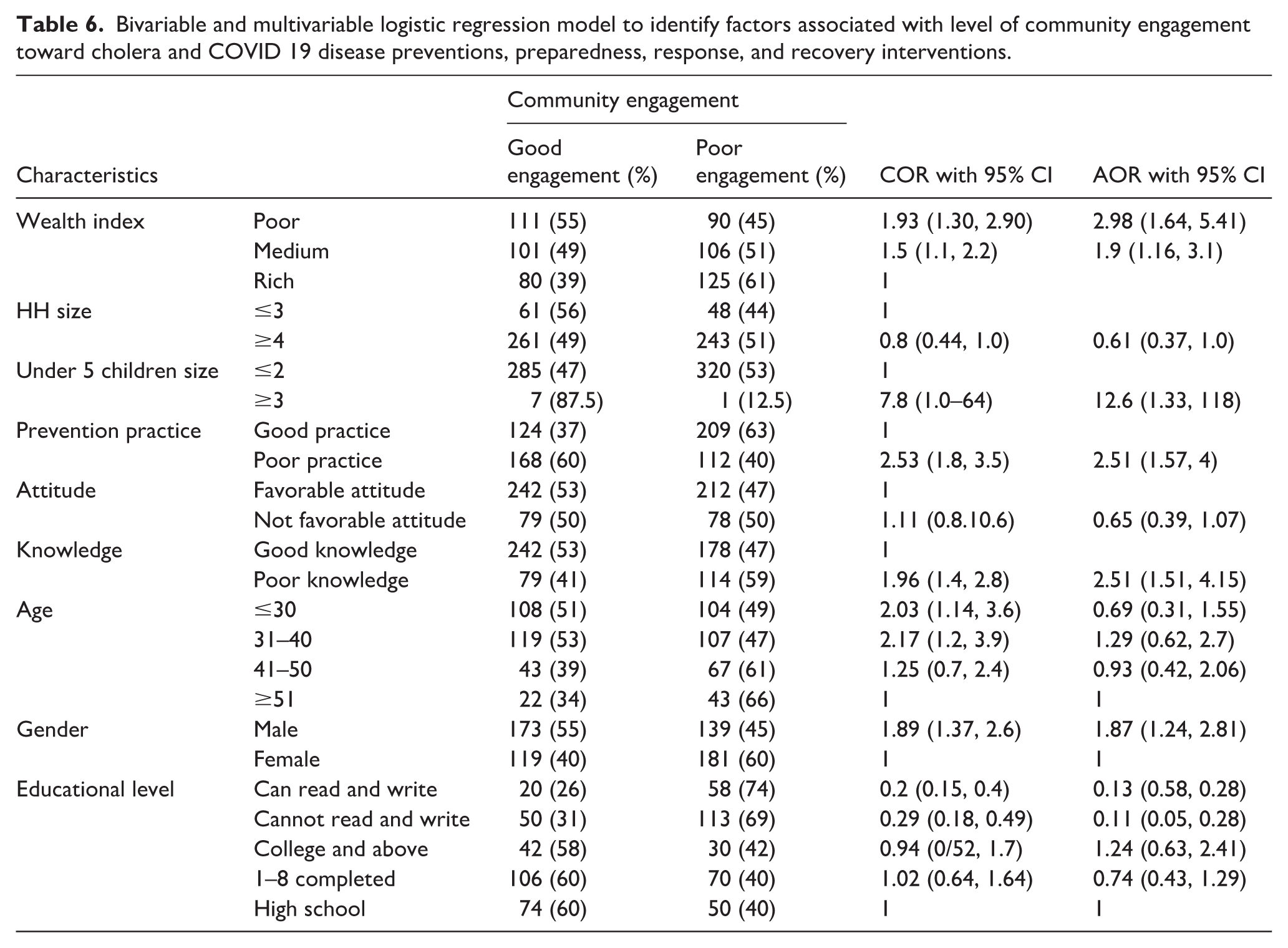
Although the crude proportions suggest higher engagement among males and individuals in the poor or medium wealth categories, these patterns did not persist after adjustment. In the multivariable analysis, male participants had higher odds of poor engagement (AOR 1.87; 95% CI 1.24–2.81). Similarly, participants in the poor and medium wealth categories had significantly higher odds of poor engagement compared with those in the rich category (AOR 2.98; 95% CI 1.64–5.41 and AOR 1.90; 95% CI 1.16–3.10, respectively). The subgroup with three or more under-five children was small (n = 8), but the model showed increased odds of poor engagement in these households as well (AOR 12.60; 95% CI 1.33–118.0), reflected by the wide confidence interval (Table 6).
Discussion
This study found that community engagement in cholera prevention and response was generally low, with only about half of participants demonstrating good engagement. The multivariable analysis identified several factors independently associated with poor engagement. Lower socioeconomic status, reflected in poor and medium wealth categories, was strongly linked to higher odds of poor engagement. Households with three or more young children also showed substantially higher odds of poor engagement, although the number of such households was small. Individuals with poor prevention practices and lower levels of knowledge were similarly more likely to exhibit poor engagement. Male participants also had higher odds of poor engagement compared with females. Together, these findings indicate the social, economic, and behavioral constraints that shape community participation and point to specific population groups requiring targeted support in public health emergency preparedness and response.
Given that data collection occurred during the peak of the cholera outbreak, the timing may have influenced participants’ perceptions, risk awareness, and reported engagement levels. Heightened transmission periods are often accompanied by intensified community mobilization, increased exposure to health messages, and greater perceived urgency, all of which can elevate engagement compared with periods of lower incidence A recent assessment in Ethiopia similarly noted low engagement early in an outbreak, with participation increasing as response activities expanded. 25 These dynamics suggest that the findings may reflect outbreak-specific behaviors, and generalizability to non-outbreak settings may be limited.
Having a low income or a larger family size significantly increased the likelihood of poor engagement. These findings are consistent with other research exploring the link between socioeconomic status and health-related engagement. Studies from Nigeria and Bangladesh similarly found that populations with limited economic resources often prioritize daily work over community engagement due to financial constraints.26,27 The current results reinforce this, indicating that households facing greater economic hardship struggle to dedicate time and resources to communal health activities.
Additional factors contributing to decreased engagement included weaker prevention practices and limited knowledge about cholera. The study’s implication that insufficient information sharing undermines awareness and engagement aligns with findings from WHO and Nigeria.28,29 Without effective community education on disease risks and control strategies, preventive behaviors and engagement are likely to be compromised. However, other research from Malawi indicated that radio messaging and community meetings significantly improved knowledge and self-reported prevention measures.2,8,9,30–32 Targeted health promotion through culturally appropriate channels could help address the information gaps identified in this population.
The study also uncovered some unique factors. For instance, men showed poorer engagement compared to women, who had more frequent contact with health services. This contrasts with findings from a Ugandan study, which reported no gender differences in engagement levels.33,34 These disparities may be more related to program-specific interactions than to inherent attitudes. Additionally, lower educational attainment was a significant predictor of reduced engagement in this study, while a Tanzanian analysis found that literacy had no impact on engagement.2,31 These nuanced differences likely arise from varying cultural and health system contexts.
Strengths
This study had several strengths. The multistage cluster sampling approach provided a representative sample, improving the generalizability of the findings. The sample size was adequately powered, and the inclusion of socioeconomic, knowledge, and practice variables offered a comprehensive view of factors influencing engagement. Identifying vulnerable groups also provides practical insights for designing targeted interventions. The study contributes meaningful evidence to the limited research on community engagement in cholera outbreak settings.
Limitations
This study also had several limitations. Its cross-sectional design prevents causal inference, and self-reported data may be affected by recall or social desirability bias. The cluster sampling approach may have overlooked some communities. Because data collection occurred during the outbreak response phase, engagement levels may differ from those in preparedness or recovery periods. The study did not include qualitative methods to explore community perspectives in depth, and the standardized questionnaire may not fully capture the complexity of engagement. Finally, measuring engagement at a single time point offers only a snapshot, and unmeasured contextual factors may have influenced the associations observed.
Implications
Despite these limitations, the study offers important implications for policy and practice. The gaps identified in community engagement underscore the need for strengthened, targeted strategies. Integrating community-driven initiatives in water, sanitation, and hygiene (WASH), education, and primary care could help mitigate the socioeconomic barriers that hinder engagement. Enhancing coordination between health authorities, community leaders, and civil society organizations is likely to promote more inclusive and effective engagement. Collaborative approaches aimed at building sustained stewardship capacities will be crucial for long-term preparedness against outbreaks. Multi-sectoral ‘health in all policies’ solutions have the potential to create more resilient communities better equipped to manage public health threats. By addressing engagement barriers through empowering systems-level solutions guided by the communities themselves, cholera outbreak control could be significantly improved.
Conclusion
The study revealed inadequate levels of knowledge, positive attitudes, and preventive practices related to community engagement in cholera outbreak management within the study area. Only about half of the participants exhibited sufficient levels of engagement. Factors such as lower socioeconomic status, larger household size, weaker community connections, and limited knowledge and practices were independently associated with poorer engagement outcomes. Although the cross-sectional design limits the ability to draw causal conclusions, the findings highlight critical gaps that need to be addressed to enhance community engagement in outbreak preparedness, control, and prevention. Targeted interventions, particularly for marginalized groups, are necessary to improve engagement.
Supplemental Material
sj-docx-1-phj-10.1177_22799036261423664 – Supplemental material for Empowering communities in cholera outbreak response: Local perspectives from Sidama, Ethiopia
Supplemental material, sj-docx-1-phj-10.1177_22799036261423664 for Empowering communities in cholera outbreak response: Local perspectives from Sidama, Ethiopia by Aschalew Abayneh, Sileshi Demelash. Sasie, Selamawit Mengesha and Mark Spigt in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036261423664 – Supplemental material for Empowering communities in cholera outbreak response: Local perspectives from Sidama, Ethiopia
Supplemental material, sj-docx-2-phj-10.1177_22799036261423664 for Empowering communities in cholera outbreak response: Local perspectives from Sidama, Ethiopia by Aschalew Abayneh, Sileshi Demelash. Sasie, Selamawit Mengesha and Mark Spigt in Journal of Public Health Research
Footnotes
Consent to participate
Informed consent was obtained.
Consent for publication
Not applicable.
Author contributions
AA & SDS originated the research idea. AA, SDS, SM, & MS contributed to the data synthesis and writing the manuscript. All authors have read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data analyzed during this study are included in its supplementary information files.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.