
Abstract
Background:
Vaccine hesitancy is a problematic phenomenon for vaccination campaigns. It played a significant role during the recent COVID-19 pandemic, where the role of HealthCare Workers (HCW) was particularly relevant. Understanding the motivation of HCW regarding vaccines is, therefore, paramount.
Design and methods:
We presented an online questionnaire to 5283 Italian HCW to investigate the role played by personal reasons and the potential perception of risk, the social environment, and the vaccine efficacy and safety perception in affecting HCW willingness to adhere to the vaccination campaign.
Results:
First, we discovered that those who took the vaccine to minimize health risk tended to vaccinate earlier, whereas those who did it due to social pressure received it later. Second, that those who indicated acquaintances as more important than the workplace in their vaccination choice showed more altruistic-related reasons to vaccinate, and the reverse held true. Third, that regarding two salient features of the vaccine, namely safety and efficacy, only the former was playing a role in the willingness to vaccinate, whereas the latter did not show an impact.
Conclusions:
The lessons that can be taken from these results are that future communication campaigns that push toward a timely vaccination should focus less on the social pressure, especially the one related to work environments, and more on the internal motivations of workers. Moreover, we can conclude that emphasizing the safety features of vaccines tend to play a more significant role in shaping vaccine behaviors than emphasizing efficacy.
Introduction
The outbreak of Sars-CoV-2 pandemic has been a severe social and public health problem. In addition to the suffering directly caused by the disease, it prompted the enactment of restrictive measures such as lockdowns, reduced mobility, and social distancing, in order to decrease the spread of the virus and to reduce hospitalization in intensive care units. The development of several vaccines was decisive for the containment of the virus and the achievement of herd immunity. 1 However, reaching such an immunity threshold requires compliance from the population as a whole: barring that, the entire process becomes complex, time-consuming, and potentially ineffective. 2 Therefore, immunization efforts are hampered by vaccine hesitancy.
The phenomenon of vaccine hesitancy was not new at the onset of the Covid-19 pandemic.3,4 However, the pandemic underlined how compliance with vaccination policies, or lack of it, has become more relevant for society as a whole. 5 It also emphasized to the general public some finer points on the nature of vaccination and its intrinsic dilemmas. One regards the comparison or risks: the uptake carries a certain, albeit tiny, risk of developing adverse reactions, compared to a much greater risk if one catches the disease, which however is not a certain fact. 6 Another regards the social dimension: vaccination is a personal choice, which nonetheless carries social repercussions, and one could be caught in the dilemma of having to incur a personal cost to achieve a collective gain. 7 A third point is the progressive nature of general immunization, which has to reach threshold limits in the form of rates needed to achieve herd immunity: this interrelated nature of immunization could prompt some people to disregard the effectiveness and the need for vaccination. 8 It also has to be remembered that the decision to vaccinate or not is the result of a complex decision-making process, which can be affected by numerous cognitive biases. 9
As it is, the decision on whether to vaccinate against COVID-19 involved several internal and external factors. On the one hand, the personal perception of salient features of vaccines, specifically safety and efficacy, strongly impacted on this decision. 10 On the other hand, the social dimension of the decision should not be underestimated. External constraints such as specific requirements from superiors, peer pressure, judgment or fear of judgment by family, friends, co-workers, and acquaintances were all powerful drives, which could even trump inner beliefs.11,12 This study aims to clarify and quantify these two separate, but interconnected, dimensions, focusing on a population consisting of HealthCare Workers (from now on, HCW). Crucially, this work fills a gap that, to the best of our knowledge, has not been addressed by previous literature on the subject: an estimation of the relative weight of two different features of vaccines and vaccine communications, namely safety and effectiveness.
Motivations
Healthcare workers during the pandemic
HCW were selected as the first targets of the immunization campaign due to both their constant exposure to the pathogen agent and to their role as trusted health information sources for the general public. 13 HCW beliefs and behaviors regarding vaccination tend to influence compliance in the general population, 14 so they represent a crucial population to investigate to get an overview of a population compliance factor. In Europe and in the USA, the planning of the vaccination campaign against COVID-19 started as soon as the EMA and FDA allowed the large-scale distribution of doses. 15 In Italy, vaccination was made mandatory for HCW in April 2021 (D.L. n°44, 01/04/2021, see Ref. 16 ). However, the obligatoriness of vaccination did not make the investigation of HCW perception of vaccines a moot point. Studying the timing of vaccine uptake before the introduction of mandatory vaccines reveals crucial points about HCW intrinsic beliefs and actions, which in turn shape those of their patients and the people who epistemically rely on them as experts and sources of information. 17 Even if a minority of HCW harbor suspicion toward vaccines, those inclinations tend to reverberate and be amplified in the general public. 18 For these reasons, studying the motivations that prompt HCW in the decision to vaccinate or not is extremely important.
To achieve this result, our research developed in a twofold direction. First, we enquired into vaccine-related beliefs and the actual perception of risk when self-regarding, other-regarding, and social factors were involved in the context of vaccination against COVID-19. Second, we investigated those elements’ importance in shaping decisions regarding vaccination. In other words, we aimed to assess the influence of various individual motivations on vaccination intentions. Moreover, we sought to determine the perceived significance of risk reduction in terms of both personal infection and transmission to others, as well as the avoidance of negative social judgment. Lastly, we aimed to ascertain the relative weight of these factors in the decision-making process regarding vaccination.
It is important to notice that the data collection of this study, carried out between January and April 2021, represents a once-off treasure trove, casting new light on the opinions of HCW, because it was the last opportunity to collect data unadulterated by the promulgation of the laws introducing vaccine compulsiveness, in April 2021. But what are these opinions among this segment of the population?
Personal subjective reasons
According to previous literature, one of the main reasons behind vaccination among HCW is the protection of oneself and the community. Conversely, fear, low estimation of contagion risk, and high estimation of personal immune system capacity are strongly related to vaccination hesitancy.19,20 The general models of measuring psychological antecedents of vaccination in the general population21,22 seems to hold even for HCW.23,24 However, there are crucial differences between HCW and the general population. During the Covid-19 pandemic, as in every sanitary emergency, HCW were the first and the most affected fraction of the population in dealing with the virus. The result were higher workloads, job stress, and time pressure, compounding with an organizational support necessarily limited. These aspects led to a higher burnout rate. 25 In that case, the situation led to an increase in vaccination intention among Italian HCW, 26 which was shadowed but not superseded by the introduction of mandatory vaccination. Since the influence of healthcare providers’ recommendations to vaccinate proved to be a highly significant factor in shaping citizens’ decisions regarding vaccination,27,28 this study aimed to explore their beliefs regarding vaccination prior to its mandatory implementation.
The role of social contexts
In that regard, it has to be reminded that the legal and practical responsibility to enforce compliance with mandatory vaccination laws was given to hospitals and local sanitary structures. That created a further layer of complexity, given how much influence the social context has on both what people (and, specifically, HCW) believe, and how they behave. This social context influenced several aspects. First, it fixed a salient reference point for a certain behavior within a specific community, highlighting relevant information. Second, it underlined one specific behavior as more socially accepted. Third, it created social incentives to conform to the norm, and disincentives to deviate from it. These reasons contributed to the fact that we observed a convergence of personal behavior toward what’s perceived as the socially accepted one, 29 especially when the reference community was relatively narrow, well-defined, and considered to share values and professional practices 30 : such is the case of HCW. In that regard, vaccination does not differ. 31 Regarding vaccination, there is strong evidence that people’s beliefs and motivation are shaped by information gathered from social reference communities.32,33 However, the role of social context most not be overestimated as the main culprit. Rather, it blends with personal preferences and values. If it is true that one’s beliefs are shaped by their context, it is also true that personal beliefs influence the kind of social context one feels to belong to, and decides to spend cognitive effort to fit in. Lower or higher importance given to self- or other-regarding protection, priority of values, presence or lack of safety concerns, and ideological affiliation have an impact as strong as perception of vaccine as a social norm regarding the acceptance or refusal of the vaccine among HCW. 34 It is also important to clarify why we focused on the social context as broadly defined, instead of considering the impact of mere conformity. Social pressure can generate conformity in the vast majority of people, but it can also generate non-conformity, dissidence, or rebellion. Even if the recognition of conformity tendencies has been firmly established for a long time, 35 cultural factors heavily modulate conformity.36,37 Disentangling “Social Pressure” from “Conformity” allowed us not to be mired in complex analyses on whether social pressure was driving vaccination up or down, given how we were focusing on gauging the comparative impact between “internal” and “external” drivers for vaccination. For these reasons, this study investigated the role played by different social contexts in shaping HCW’ beliefs and their vaccination attitude.
Potential perception of risk
In this study, we also consider how different beliefs on the perceived probabilities, namely the probabilities of (1) being infected, (2) infecting others, and (3) having your own opinion judged, interact with the perception of safety and efficacy. This last point is important to remember, considering how beliefs of inadequate efficacy can push in the direction of delayed uptake, even if self- and other-regarding considerations are deemed high. Here, we focused our research on safety and efficacy perception, given their role as modulators of confidence and trust in vaccination.38,39 The term vaccine safety refers to the probability of not having any adverse reactions after administration. 40 The various vaccines against COVID-19 are considered very safe, with an almost total absence of severe side effect. 41 However, people still harbored doubts about them, due to the quick development of the vaccines themselves, 42 side effects both real and circulated due to fake news, 43 and concerns over impact on fertility rates. 44 Conversely, the term vaccine efficacy refers to the degree of protection against severe disease, hospitalization or death as a result of the infection. The beliefs on these two aspects played a pivotal role in the decision to vaccinate. 45 Indeed, those two are considered the main mediators between the source of information and the vaccination uptake. 46 However, to the best of our knowledge, no study has investigated their relative weight in shaping vaccine uptake. On that ground, this study investigates the role that HCW perception of vaccine efficacy, on one hand, and safety, on the other, has in shaping vaccine-related behaviors.
The present study
In the present study, our aim was to investigate the role played by the personal reasons and the potential perception of risk, the social environment, and the vaccine efficacy and safety perception in affecting the willingness of HealthCare Workers to adhere to the vaccination campaign. More specifically, we addressed three main research questions:
We investigated how different personal subjective reasons affect the decision to adhere to the vaccination campaign. More specifically, we explored the difference between egoistic and altruistic reasons in predicting the vaccination date and the direct effect of the perceived social pressure on the healthcare’s choice to postpone the vaccination (
Taking into account the collective environment and its social influence, we investigated how different contexts (i.e. acquaintances and work) and job responsibility contributed to building and strengthening the individual reasons behind vaccination and how different and opposite social reasons (i.e. altruistic vs social pressure) mediated this relationship (
We examined how the potential perception of risk of not being vaccinated modulated the perception of the efficacy and safety of the vaccine. Lastly, we evaluated the differential direct predictive power of safety and efficacy regarding vaccination campaign subscription (
Answering these questions will help us better understand how social reasons and perception of risk modulated the response to the pandemic. These questions remain relevant for three reasons. First, despite the end of the pandemic, its social and health consequences are far from over, and unraveling their mechanism could help in better correcting for their effects. Secondly, while the hope is contrary, a new pandemic in the future cannot be ruled out, and it would be wise to come to such a predicament with a better understanding of our past mistakes. Third, vaccine hesitancy among HCW is still a problem, even with regard to other vaccines (such as the flu shot), which is another facet of the question that ought to be addressed.
Design and methods
Participants
An initial sample of 6037 healthcare workers was recruited for this study. 754 participants did not consent to participate in the survey and were excluded. All our participants were healthcare providers and worked in Tuscany. All major local health units (USLs; USL Toscana NO, USL Toscana Centro, USL Toscana SE) have been involved in this project. The survey was disseminated by USLs using their private networks through different forms of communication (i.e. emails, private messages, word-of-mouth). This sampling technique allowed us to reach the largest number of healthcare providers in Tuscany. Importantly, because dissemination was managed directly by the public health system, we had no direct control over the final sample size. Moreover, it would have been neither fair nor ethically appropriate to restrict participation to a subset of healthcare workers in order to meet a predetermined sample size, as this would have arbitrarily excluded eligible professionals. All participants were informed about the purpose of data collection, assured that their responses would remain anonymous, and consented to the anonymization of their data for research purposes. The questionnaire was open to be filled from 1/04/2021 to 30/04/2021. No monetary compensation or other forms of reward were provided to participants for their involvement in this study and no follow-up or reminders were conducted. After data collection, 373 participants were excluded since they did not complete the questionnaire. The present study received ethical approval from the ethical commission of the University of Siena (16/2021), and it followed the ethical guidelines for behavioral research of the American Psychological Association. All our participants were adult Italian native speakers; Table 1 summarized the main socio-demographic characteristics of the HCW sample and vaccination rates.
Sample characteristics.

Survey structure and procedure
This is a cross-sectional, observational study based on a web survey administered in April 2021 to a large sample of Italian healthcare workers. The questionnaire was developed on Qualtrics.com, a website designed for online surveys. The questionnaire lasted 5 min on average (M = 4.15; SD = 126.80). Participants could access the survey via an un-reusable link, and complete the questionnaire directly from their own laptop or smartphone. The survey was designed in a within-subject fashion and consisted of a total of 24 items measured by means of a 5-point Likert scale (from “strongly disagree” to “strongly agree”). Before proceeding to the questionnaire, participants provided informed consent by clicking a “Consent” button, which indicated their agreement to the following statement: “I have read and understand the above consent form. I certify that I am 18 years old or older. By clicking the ‘Consent’ button to enter the survey, I indicate my willingness to voluntarily take part in this study.” This action was treated as an electronic signature. After consenting, participants read the instructions and was informed about the main objective and purposes of the present survey. After that, participants answered questions related to their vaccination status (e.g. “Did you receive the vaccine?”; “In which month did you adhere to the vaccination campaign?”). Subsequently, according to the previous responses, participants completed two sections that investigated the personal reasons behind their vaccination choice and the (potential) perception of risk of not being vaccinated in a randomized order.
The following sections investigated the importance of different social contexts when choosing about vaccination. Participants evaluated the importance (and the influence) of their acquaintances (family and friends) and the work environment (heads and colleagues). The next items assessed the quality of the vaccination campaign (3 items) and previous flu vaccination. Then, HCW expressed their perceived efficacy and safety of the vaccine administered in the early stages of the pandemic (from very low to very high). Lastly, participants provided basic socio-demographic information. All the items of the present questionnaire were developed by consulting experts in vaccine hesitancy from local healthcare units (USLs), including healthcare professionals and researchers in public health.
All constructs were assessed using single-item questions designed to capture salient motivational drivers (e.g. altruistic motives, perceived safety, perceived efficacy). These items were developed in consultation with domain experts and are reported in full in the Supplemental Material. The single-item format was chosen to ensure brevity and feasibility given participants’ time constraints, and was informed by prior research highlighting the salience of such constructs in vaccine decision-making.47,48
Statistical analyses
IBM SPSS 26 49 was used for the main statistical analysis. The path analysis models were built and run on Jamovi 2.3. 50 In each analysis, the effect size is provided by using the η value (eta squared for ANOVA statistics). ANOVA post-hoc observed power is provided in terms of (1-β). As regards saturated path analysis, the models were estimated using maximum likelihood (ML) estimation. We reported the standardized path coefficient (β), the relative Standard Error (S.E.), the level of statistical significance (p value), and the 95% bias-corrected bootstrap confidence interval (95% CI) for each measured path. Indirect effects and their standard errors were computed through a bootstrap procedure (N = 5000). Given the saturated nature of the employed models, fit indices are not informative. The significance level was set to α = 0.05. All variables were checked for normality by the Shapiro–Wilk test and for homoscedasticity by Levene test. When violating the above assumptions, we computed the Z score for large samples using skewness and kurtosis measures to determine substantial normality. 51 All the post-hoc comparisons have been corrected using the Bonferroni correction and were investigated upon a significant main effect or interaction.
Results
Although there was no mandatory vaccination at the moment of data collection (nor any vaccination certificate, April 2021), of the 4910 healthcare workers included in the analyses, 4737 (96.5%) reported having been vaccinated, while 173 (3.5%) had not. Descriptive statistics for all variables are presented in Table 2. On average, participants reported high endorsement of both egoistic reasons (M = 4.49, SD = 0.95) and altruistic reasons (M = 4.68, SD = 0.77) for vaccination, whereas social pressure was less frequently endorsed (M = 3.42, SD = 1.50). Risk perceptions were generally moderate to high for egoistic (M = 3.93, SD = 0.93) and altruistic motives (M = 3.92, SD = 0.98), but lower for social pressure (M = 2.77, SD = 1.39). Social influence from acquaintances (M = 3.52, SD = 1.30) and the work environment (M = 3.25, SD = 1.25) were reported at intermediate levels. Perceived efficacy (M = 3.93, SD = 0.80) and perceived safety (M = 3.91, SD = 0.82) were also rated above the midpoint of the scale.
Descriptive statistics of study variables.

As for exploring our main research questions, we performed three path analyses testing partial mediation models 52 through a transmittal approach. 53 The three models aimed to investigate what factors can lead to a timely vaccination. In this context, we restricted the sample to HCW who adhered to the vaccination campaign (N = 4865). The common dependent variable of the three models was the month of vaccination (from December 2020, the date of issue of the vaccine’s first dose to the end of April 2021).
How did different personal subjective reasons affect the decision to adhere to the vaccination campaign? (Q1)
The first model investigated the relationship between the personal reasons behind the vaccination choice (egoistic reasons; altruistic reasons; social expectation – exogenous variables) and the vaccination date (endogenous variable). Exogenous variables were measured through a 5-point Likert scale. Both the effect of the egoistic reasons (“I got vaccinated to reduce the risk of contagion”) and altruistic ones (“[. . .] to reduce the risk of infecting other people”) proved to be negatively associated with the month of vaccination (Ego: β = −0.14, 95% CI [−0.19, −0.11], p < 0.001; Altruistic: β = −0.13, 95% CI [−0.22, −0.13], p < 0.001). Conversely, social blame reasons (“[. . .] to avoid being judged”) positively predicted the month of vaccination (SB: β = 0.05, 95% CI [0.03, 0.07], p < 0.001 (Figure 1) In a nutshell, those who cited egoistic reasons, expressing their desire to reduce the risk of contagion, tended to get vaccinated earlier. Similarly, individuals driven by altruistic motives, seeking to minimize the risk of infecting others, also chose to get vaccinated sooner. On the other hand, those who felt social pressure tended to vaccinate at a later time.
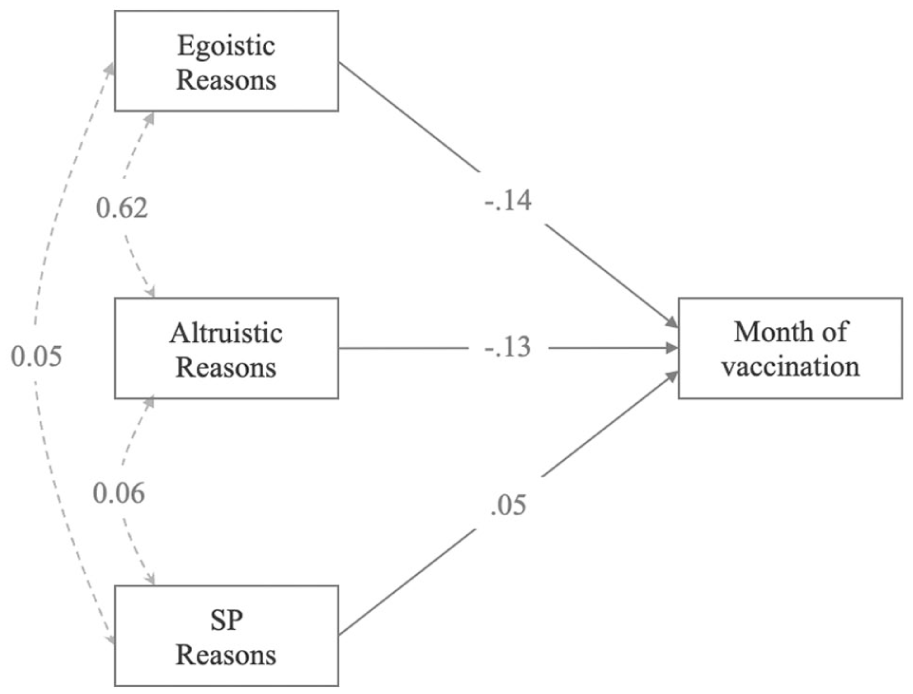
Path analysis: Parameters estimates are standardized. Dotted lines represent insignificant paths. Continuous lines represent significant paths.
Moreover, to deepen our understanding of the main drivers behind vaccination choice, we investigated the relationship between the personal reasons behind vaccination and our participants’ potential perception of risk. A two-way repeated measure ANOVA Motivation (Egoistic, Altruistic, Social pressure) * 2 Type (Personal reasons, perception of risk) was conducted to understand the main drivers behind the vaccination choice. The ANOVA revealed a main effect of the motivation, F (2, 9472) = 3453.73, p < 0.001, η p 2 = 0.42, (1−β) > 0.99, and a significant main effect of the type, F (1, 4736) = 2896.31, p < 0.001, η p 2 = 0.28, (1−β) > 0.99 as well as a small significant interaction between them (p < 0.001, η p 2 = 0.008). Interaction post hoc analysis confirmed that all the personal reasons (Egoistic: M = 4.52, SD = 0.89; Altruistic: M = 4.71, SD = 0.71; Social Reasons: M = 3.43, SD = 1.50) represented a stronger motivation toward the vaccination as compared to perception of risk (Egoistic: M = 3.95, SD = 0.91; Altruistic: M = 3.94, SD = 0.97; Social Blame: M = 2.77, SD = 1.38; all ps < 0.001). Secondly, both as regards personal reasons and perception of risk, social blame was found to be a weaker driver of vaccination (ps < 0.001). Lastly, among the personal reasons, post-hoc comparisons revealed a greater role of altruistic reasons as compared to egoistic ones (p < 0.001). It suggested that while the perception of risk certainly played a role, the desire to protect oneself and loved ones from harm was found to be the stronger drive toward vaccination.
How did different social contexts and job responsibility contribute to building and strengthening the individual reasons behind vaccination? (Q2)
The second path analysis studied how the environmental categories affect vaccination date as mediated by personal reasons. The two endogenous variables (acquaintances and work environment) were calculated by averaging 4 different items (family and friends; heads and colleagues) measured using a 5-point Likert scale that measured the impact of the social context on the vaccination choice. The social reasons (altruistic and social blame), codified as mentioned above, were the mediators, whereas the vaccination date was the dependent variable. Our model highlighted an opposite influence of the social context in building vaccines’ motivation. In particular, the importance of the acquaintances was positively related with altruistic reasons (β = 0.28, 95% CI [0.15, 0.18], p < 0.001) and negatively associated with social blame (β = −0.12, 95% CI [−0.18, −0.09], p < 0.001). On the contrary, the work environment was positively associated with the fear of social blame (β = 0.33, 95% CI [0.36, 0.44], p < 0.001) and negatively predicted altruistic reason (β = −0.12, 95% CI [−0.10, −0.07], p < 0.001). Moreover, the direct effects of the acquaintances and the work environment on the vaccination date were significant and opposite (β = −0.17, 95% CI [−0.16, −0.10], p < 0.001; β = 0.14, 95% CI [0.08, 0.14], p < 0.001). Lastly, the effect of altruistic and social pressure reasons was symmetrical to the model presented in the previous paragraph. As for indirect effects, the model highlighted a significant partial mediation of the acquaintances – vaccination month through the altruistic reasons (β = −0.05, p < 0.001) and the social blame (β = −0.006, p = 0.002) and, symmetrically, a partial mediation of the work environment – vaccination month via altruistic reasons (β = 0.03, p < 0.001) and the social blame (β = 0.02, p < 0.001). In other words, acquaintances had a strong influence on altruistic reasons and were negatively associated with social blame as motivations for vaccination. On the other hand, the work environment had a different impact, with a higher tendency toward social blame and a negative effect on altruistic reasons. Furthermore, individuals who prioritized their acquaintances tended to get vaccinated earlier, while those who gave importance to the work environment tended to delay their vaccination.
A second two-way mixed ANOVA was also run to investigate the influence of the perceptions of the vaccine’s efficacy (between factor: low efficacy, high efficacy) and the social contexts (within factor: acquaintances, work environment;

Left panel: Path analysis: Parameters estimates are standardized. Dotted lines represent insignificant paths. Continuous lines represent significant paths. Right panel: Differences in the environmental influences depending on efficacy perception. HCPs who judged the vaccine as low effective were mainly influenced by the work environment. Conversely, those who perceived a high efficacy of the vaccine attributed a higher importance to their acquaintances.
How did the potential perception of risk of not being vaccinated modulate the perception of the efficacy and safety of the vaccine? (Q3)
A path analysis was conducted to explore the relationship between different perceptions of risks (egoistic, altruistic, and social blame) and the vaccination date as mediated by the efficacy and safety perception. Interestingly, the model reported that egoistic and altruistic perceptions of risk (the possibility of being infected/infecting other people in the absence of vaccination) positively predicted efficacy and safety scores (Ego-Efficacy: β = 0.17, p < 0.001; Ego-Safety β = 0.16, p < 0.001; Altruistic-Efficacy: β = 0.11, p < 0.001; Altruistic-Safety β = 0.11, p < 0.001). Conversely, the risk of potential social blame did not reveal any association with vaccine’s perception [p = 0.27; p = 0.35]. Moreover, if the egoistic and altruistic perception of risk negatively predicted the vaccination date (Egoistic: β = −0.11, p < 0.001; Altruistic: β = −0.13, p < 0.001) driving people to a timely vaccination, the risk of any potential social blame was positively associated with the month of the vaccine uptake (Ego-Efficacy: β = 0.05, p < 0.001) leading to procrastination in the vaccination decision. Secondly, and crucially, we found that, considering the safety and efficacy as main drivers of vaccination compliance, only the former resulted to be a significant negative predictor of the vaccination date (β = −0.11, p < 0.001). Coherently, we found a partial significant mediation (indirect effects) of the egoistic and altruistic perception of risk and the month of vaccination only for the safety mediator (ps < 0.001; β [−0.018; −0.013]), whereas the efficacy evaluation never affected the relationship between the perception of risk and the month of vaccination (Figure 3). In short, both egoistic and altruistic perceptions of risk, regarding the possibility of being infected or infecting others without vaccination, had positive effects on efficacy and safety scores. Conversely, the risk of potential social blame did not show any association with vaccine perception. When it came to the timing of vaccination, only the perception of vaccine safety emerged as a significant negative predictor of the timing of vaccination. A mixed ANOVA also investigated the difference in the efficacy and safety (within factors) subjective perception across different job titles (between factors: HC assistants, nurses, and physicians;

Left panel: Path analysis: Parameters estimates are standardized. Dotted lines represent insignificant paths. Continuous lines represent significant paths. Right panel: Differences in efficacy and safety vaccine evaluation on the basis of the job title: efficacy and safety perception grew in proportion to the responsibility within the hospital of the HCP.
Discussion
Our research aimed to achieve a finer level of granularity in the analysis of how the social context and the perception of risk, safety and efficacy of vaccines would translate into a timely vaccination in healthcare workers. These components are, without a doubt, important. However, the analysis over vaccine hesitancy often bundles these elements together, falling short of achieving a detailed account.
Indeed, in what can be considered the earliest attempt at seriously categorizing the antecedents of vaccine hesitancy, the 3C model developed by the World Health Organization in the mid-2010s, considerations over vaccines’ safety and efficacy are presented conjoined in the first C, confidence, whereas the social elements shaping vaccination choices are left aside. 38 It must be kept in mind that the past decade has seen an enormous amount of effort at refining and further developing explanations for attitudes toward vaccines. The 3C model evolved into the 5C model 21 : the already present Confidence, Convenience and Complacency were replaced by Confidence, Complacency, Constraints, Calculation, Collective Responsibility. A recognition for the social context was partially included within the Collective Responsibility antecedent, but it has to be underlined how that element focuses more on the evaluation of how vaccination impacts one’s own social environment, rather than how much the choice to vaccinate is shaped by the social environment. More recently, a further evolution into a 7C model has been proposed, 22 and its validity as a model appears to hold for HCW as well. 54 These developments are giving an increasingly fine-grained picture. Several authors suggested55,56 that the Confidence element should be split to distinguish between confidence in the inherent features of the vaccine (safety and efficacy) and confidence in the systems that push for vaccination. At the same time, Social Conformism was explicitly proposed and analyzed as a psychological antecedent of vaccination. 24 The present study wanted to fit into this collective endeavor. Appreciating the importance of social conformism, on the one hand, and of the role of considerations over safety and efficacy, on the other, still leaves ample space for analyses. Not every element of the social environment plays the same role in the choice to vaccinate, and not every feature of the vaccine is equally salient. Personal acquaintances have a more positive influence on the time of vaccination than the work environment, and safety of a vaccine appears to be more important than its efficacy. But specifically, how?
Mapping of personal subjective reasons into adherence (Q1)
Concerning our first research question, the main result we found was that those who mainly wished to minimize the risk of infection for themselves and for others tended to get vaccinated earlier. On the contrary, those who took the shot due to a sense of social pressure tended to vaccinate at a later time. Intuitively, this may not come as a shocking result. Those who comply with a public measure out of personal conviction would adopt the suggested behavior even in the absence of the measure in itself, and therefore would actively seek out the inoculation. Conversely, one could expect from those who would take the vaccine due to the pressure of colleagues, superiors, and social expectations, rather than their own reasons, that they would not be as proactive as the former category in their pursuit.
This result is interesting for two reasons. The first lies in the judgment of the communication campaign that surrounded and supported the vaccination efforts. The narration revolving around the virus was rich in metaphorical images, such as the one that depicted the pandemic as a sort of war. HCW were prominently featured in the public discourse over vaccination, being at the same time receivers and providers, object, and subject. Due to this, the language evoked in the HCW role narration was conforming to this framework of conflict. HCW were “at the frontline,” and their “service” was turning them into “heroes.” The consequences of this rhetoric have been widely criticized: blurring the divide between work and service, between duty and heroism, stifled a meaningful discussion over HCW responsibilities, placing an unwarranted burden on the entire category. 57 This move could have been justified if the creation of social expectations over HCW would push them toward a more timely compliance with public policies. At least for what pertains to vaccination, our result suggests this was not the case. Hence, we conclude that in that regard, this narrative lacked beneficial consequences: a lesson that ought to be remembered when dealing with such cases in the future.
The second interesting implication of our result is on how it fits into a debate that is currently underway regarding the role and the weight of prosociality in the decision on whether to vaccinate or not. As we mentioned, the decision to vaccinate or not carries an interesting conundrum: it is a personal decision that affects one’s health, but it achieves a collective impact because it means contributing to herd immunity. As in every decision with a social component, a greater or lower tendency to prosociality might affect the decision itself. Evidence in that regard, however, is mixed. While some data points out how emphasizing the social benefits of vaccination is a viable communication strategy to improve vaccine uptake, 48 other data suggests that this is not the case and that insisting on social expectations and repercussions of one’s behavior regarding vaccination does not change attitudes toward vaccination. 58 Our results may be of help to disentangle this apparent conundrum. Prosocial behavior is a broad class of behavior defined as involving costs for the self and resulting in benefits for others. 59 Both the decisions to vaccinate to protect others (what we call “altruistic reasons”) and to conform to social expectations in order to be of example to the general population might be considered forms of prosocial behavior. However, our results show that the former is much more relevant than the latter. This element emphasizes the need for a much finer granularity in the analysis and the description of the impact of prosociality over vaccination, taking into account personal networks of kin, colleagues, and acquaintances in order to design effective campaigns.
Social contexts and job responsibility (Q2)
To disentangle the actual effect of social pressure, we analyzed the collective environment, distinguishing between personal relationships and social ties developed in the work setting. Our results in that regard were three. First, those who indicated the workplace as more important in their choice to vaccinate showed less altruistic-related reasons and more social pressure-related reasons. Conversely, those who indicated acquaintances as more important show the inverse pattern. Lastly, those who indicated the workplace as more important got the shot later than those who were prompted by close acquaintances.
These results are relevant because while it is important to point out how the social environment modulates the decision to vaccinate, it has to be kept in mind that the degree and the direction of that influence depend on what kind of social environment we are considering.
The impact of the work environment seems to be mixed: it might deplete altruistic motivation, rather than increase it. Organizational expectations may elicit a sense of constriction, which must be followed only when other alternatives are exhausted. Through the lens of individual job requests, vaccination scheduling acquires a mandatory meaning, more than a communitarian benevolent choice. While the working environment creates a complex matrix of judgment from peers and supervisors, 60 which could discourage a clear choice toward vaccination, the relevance of the personal relationship encourages a proactive decision to protect loved ones. This decision may be explained by a different interpretation of the concept of “relevance,” which we were inquiring about. Acquaintances are relevant in the sense that they are people who need to be taken care of, in this case in terms of indirect protection from contagion through vaccination, prompting prosocial motivations. 61 The work environment, on the contrary, is relevant because there is a structure of monetary, bureaucratic and social incentives/disincentives. It follows, perhaps unsurprisingly, that systems toward which HCW show greater intrinsic motivations, such as acquaintances and families, carry a greater weight than the work environment, and prompt an earlier vaccination.
Another result we observed was a higher efficacy and safety perception with a higher responsibility level role in the hospital hierarchy, a result in line with previous literature. 62 We acknowledge that our data are in line with other studies showing how higher levels of responsibility correspond with a higher adherence to institutional policy toward vaccination and trust in claims from the authority.63,64 It is worthy considering whether this result stems from a higher educational level of the upper echelons of the hierarchy. Data on the relationship between education levels and vaccine attitudes are conflicting.3,14,65,66 However, this lack of clarity stems from taking into account only educational milestones, and not considering rates of domain-specific education. Numerous studies from multiple countries67 –70 showed that for HCW, increased rates of referring to scientific journals as a source of information correlate with more accurate information on vaccines, higher levels of uptake, and higher intentions to receive and recommend vaccines.
Perception of risk, safety, and efficacy (Q3)
Regarding our third research question, we found two main results. The first one is that the greater the possibility of being infected or infecting other people without a vaccination, the greater the vaccine’s perception as safe and effective; social blame did not play any role in shaping this perception. The second one is that disentangling the perception of safety and efficacy of vaccines, two elements commonly taken together in this research, shows that only the former shapes and translates into vaccination intentions.
The first result is coherent with what we have seen so far. Deeming the vaccine as something valuable to get in order to protect the important people in one’s life (including oneself) means estimating not vaccinating oneself as way worse. In this regard, the effect (or, better, the lack of it) of the social blame is striking, and it underlines again how the impact of the social environment depends crucially on what kind of social environment we are considering.
The second result, however, is most interesting. In the analyses of the determinants of vaccination attitudes, safety and efficacy of vaccines are often considered conjoined, as the intrinsic characteristics of the vaccine itself. However, even if they can be considered two sides of the same coin, they elicit different cognitive reactions. To explain these results we can follow a framework based on prospect theory. 71 Such a framework states that humans, in evaluating risk, show a loss-gain asymmetry, that is, a cognitive tendency to express a preference in avoiding losses over acquiring equivalent gains; medical risk does not deviate from this tendency. 72 Efficacy of a medical procedure, in this case the vaccine, can be described as performing the part of acquiring gains, while safety can be seen as preventing losses.
Using this framework underlines the utility of disentangling the notion of safety and efficacy, as it allows a differential analysis of their impact and it makes easier to translate it into useful policy indications. If safety is the only feature of the vaccine that shapes vaccination intentions, or the one with the most impact, 73 there is little practical point in pouring resources into communication campaigns that praise both safety and efficacy. However, there is an important caveat. Framing efficacy as the “gain” part and safety as the “loss” part might be debatable. Taking the COVID-19 pandemic as an example, we can acknowledge that at the beginning of it, when the fear from the pernicious effects of the disease was widespread, the notion of efficacy could be seen as pertaining to the “loss” framework (loss of health and life, which can be prevented with an effective vaccine). However, the more the pandemic unfolded, the more the notion of efficacy was tied to a “gain” framework: gaining further protection, in addition to the one already provided by social measures of containment, previous inoculations, etc. On the contrary, the “safety” element is inextricably tied to a “loss” framework. With this interpretation, we canvass a profoundly complex cognitive landscape, one in which the perceptions are in evolution while events unfold. Indeed, studies that explicitly focused on tracking the diachronic evolution of the perception of safety and efficacy confirm this complexity, with an inversion of the relative weight between efficacy and safety perception during the course of the pandemic. 74 The only clear thing, in that regard, is that the human cognitive architecture should be taken into account in explaining vaccination attitudes, as it is vastly relevant to future public communication campaigns, as well as in the design, evaluation and reports of clinical trials and guidelines.
Limitations
This study presents some limitations, which must be kept in mind when interpreting its results. First and foremost, it has to be noticed that the peculiar pandemic moment in which the questionnaire was developed and disseminated, as well as the multiplicity of academic and institutional actors involved in the study and the sheer number of participants, made impossible to record some characteristics of the sample population. Specifically, it should be noted that we were unable to determine the response rate. However, this shortcoming is assuaged, for what pertains to statistical power, by the sheer number of participants. Secondly, it has to be underlined how the overwhelming majority of the respondents did get the vaccine, and this might have influenced their answers. In any case, our sample can be considered representative of the situation within the HCW population at the time: at January 2022 the rate of doctors sanctioned for avoiding vaccination was 0.4%. 75 Third, it should be stressed how the present study was conducted in the context of a pandemic, a globally disruptive event which heavily influenced virtually every person on the planet: generalization of behavioral results obtained during such an event should be made with utmost care. Fourth, some potential biases in our sample should be acknowledged. We were asking participants to recall and self-report their beliefs and preferences regarding vaccination at the time it was performed, which happened 1–4 months before the dissemination: this might have triggered a recall bias. The survey answers were given online and on a voluntary basis, and that entails the possibility of a self-selection bias among participants: people harboring strong distrust toward the vaccines might have refused to participate in the study. This bias might be responsible for the extremely high vaccination rates of our sample (96.5%), which may limit insights into vaccine hesitancy. However, it has to be noted that we dealt with an unavoidable methodological tension. On the one hand, we contemplated the possibility that participants’ voluntary participation could limit data gathering. On the other hand, we acknowledged that a more top-down approach to participation, which could have resulted in a more representative sample, could have compromised the voluntary nature of participation and skewed answers toward compliance with established guidelines, rather than genuine personal beliefs. This trade-off is often unavoidable. 76 Another limitation of this study is the absence of a pilot phase, which was not conducted due to the urgent need to capture HCW’s attitudes before vaccine mandates took effect. Moreover, the questions provided were single-item questions regarding salient topics, and as such, they were not subject to validation. Although our path models were specified directionally, the cross-sectional design does not allow strong causal claims. Still, directionality was theory-driven, consistent with established frameworks on vaccine decision-making, 21 and our outcome, the month of vaccination, offered a temporal anchor that strengthens plausibility. Nevertheless, longitudinal or experimental studies are needed to establish causality more firmly. Lastly, the fact that the survey was disseminated via an institutional source might have tilted some answers in a direction that might have been deemed in line with the position considered socially desirable by the institution. Consequently, no a priori power analysis was conducted to determine sample size. Instead, the number of participants was entirely driven by feasibility and ethical considerations, as the survey was disseminated through the public health system to all healthcare workers and we could not selectively restrict access.
Conclusion
The results of this study should be kept in mind in designing future vaccination and healthcare campaigns targeted at HCW, especially those in which time constraints are present. In a nutshell, the indications to improve in that regard are two. First, the emphasis given to the social pressure, especially the one related to work environments, should be downplayed to the benefit on the internal motivations of workers. As a result, vaccination campaigns should refrain from employing social pressure to promote vaccination. Second, it should be kept in mind that the safety features of vaccines tend to play a bigger role in shaping vaccine behaviors than those involving efficacy: therefore, the safety should have a predominant role while promoting vaccines. Even if we all hope that another pandemic is as far as possible in time, we must nonetheless consider the possibility that healthcare emergencies of global reach will be more and more present in a world that is increasingly more interconnected. Hopefully, next time we will be better prepared.
Supplemental Material
sj-odt-1-phj-10.1177_22799036251401950 – Supplemental material for What leads to vaccine compliance? Evidence from healthcare workers
Supplemental material, sj-odt-1-phj-10.1177_22799036251401950 for What leads to vaccine compliance? Evidence from healthcare workers by Alessandro Demichelis, Marco Marini, Dario Menicagli, Giovanna Mancini, Ennio Bilancini, Folco Panizza, Tommaso Bellandi, Leonardo Boncinelli, Paolo Pin, Giacomo Galletti, Roberta Caldesi and Gustavo Cevolani in Journal of Public Health Research
Footnotes
ORCID iDs
Author contributions
EB, LB, PP, and GC conceptualized the survey and designed the questionnaire. TB, RC, and GG cooperated at the study design and provided institutional access to the sample. EB collected the data. MM and EB analyzed the data. AD and GM reviewed the relevant literature. AD, MM, GM, and DM interpreted the data and wrote the manuscript. All authors approved the current version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Spin.Ge.Vac.S. research project D69J21006470002 and the 2023-2025 PRIN project 2022389MRW.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.