
Abstract
Background:
Healthcare workers were at the forefront of the COVID-19 pandemic. The acceptability and uptake of COVID-19 vaccines among healthcare workers was an important strategy in halting the spread of the virus as well as the antecedent implications on global health and the world economy.
Objectives:
This study aims to determine the acceptability rate and barriers to COVID-19 vaccination of frontline healthcare workers in Awka, Nigeria.
Design:
This is an analytical cross-sectional study.
Methods:
An online cross-sectional survey was conducted from February 2022 to April 2022 to obtain the data for this study. One hundred healthcare workers were studied. Acceptability rate and barriers to uptake of COVID-19 vaccination were outcome measures.
Results:
The COVID-19 vaccination rate was 45.0% among healthcare workers in study area of Awka metropolis. Ages 30–39 years had the highest acceptance rate of COVID-19 vaccination, 19 (47.5%; p = 0.262) with a more female preponderance of COVID-19 vaccine acceptance compared to males [26 (41.3%) vs 16 (42.2%), p = 0.721]. The place of residence of respondents (urban vs rural) and their marital status (married vs single) appeared not to influence the acceptance of COVID-19 vaccination [(38 (42.2%) vs 3 (33.3%); p = 0.667; 25 (36.8% vs 17 (54.8%); p = 0.433)]. Years of work experience (<10 years vs >10 years) significantly affected COVID-19 vaccine acceptance [27 (45.8%) vs 12 (52.2%); p = 0.029]. Educational status and monthly income appeared not to influence vaccine uptake (p > 0.05, for both). A significant number of respondents were not sure why they should or should not take the COVID-19 vaccine [49 (92.5%) vs 35 (83.3%); p = 0.001].
Conclusion:
The COVID-19 vaccination rate is still poor among healthcare workers in Awka metropolis. The majority of respondents do not know why they should or should not take COVID-19 vaccine. We therefore recommend robust awareness campaigns that will explain in clear terms the essence and efficacy of COVID-19 vaccination in order to improve vaccine acceptance.
Introduction
Coronavirus is caused by a novel coronavirus [severe acute respiratory syndrome corona virus 2 (SARS-CoV-2)] which has the same veiled RNA structure resembling SARS-CoV-1 that caused the severe acute respiratory syndrome (SARS) outbreak. 1 This virus was first identified in the respiratory tract of patients with pneumonia in Wuhan, Hubei China, at the end of December 2019, which was then indicated as a newly identified β-coronavirus (nCoV).2,3 As of March 11, 2020, coronavirus (COVID-19) was declared a pandemic by the World Health Organization (WHO), as it had spread to other parts of the globe and the fatality of the cases continued to rise. 4
The first case of COVID-19 was reported in Nigeria on February 27, 2020, and this led to researchers’ forecast that Nigeria would likely be the focal point of Africa’s pandemic.5,6 In the face of the many deaths from the COVID-19 virus, many countries around the globe put up cogent and strict measures to curb the pandemic, which included social distancing and compulsory use of face masks among others.7,8
It was however noted that the preventive measures on the ground were not adequate to stop the spread of COVID-19, and this led to the development and use of vaccines as one of the preventive strategies deployed to halt the spread of the virus.9,10 Due to the inadequacy of the measures on the ground to flatten the epidemic curve, the COVID-19 vaccine was developed and approved for use within a short period of time. This raised concerns and anxieties about the unknown side effects that could result from such a vaccine.11,12
COVID-19 vaccines have become available in many countries including Nigeria. On 2 March 2021, the country received the long-awaited vaccine, its first shipment of 4 million Oxford-AstraZeneca COVID-19 vaccine doses. 13 Subsequently, the vaccination was rolled out in phases following the approval of the vaccine in Nigeria. Health workers, support staff in health institutions, frontline workers, and first responders were the first group of people on the priority list.14,15 Vaccination has been opined to be the most effective way of controlling infectious diseases, though its success is often challenged by people who choose either to delay the uptake or refuse to get vaccinated. 16
Immunization coverage could be negatively affected by a wide range of side effects, which are often associated with vaccinations. These side effects may be scientifically based, in some cases, may be coincidental or mere speculations, and are often not substantiated. 17 In most viral outbreaks, COVID-19-inclusive healthcare workers (HCWs) are proactive agents of change whose skills and experience have been proven to contribute significantly to the protection of the populace. 18 HCWs were considered as a group at high risk of SARS-CoV-2 infection, and as such, candidates for early vaccination. This has become so important, such that in Italy, data showed an early decrease of the SARS-CoV-2 circulation among HCWs in the first 50 days of vaccination campaign, during which most HCWs had not yet achieved the state of full protection, since immunized persons are not considered protected against COVID-19 until at least 7 days after receiving the second dose. 19 Similarly, a study examining HCWs working in publicly funded hospitals in the United Kingdom revealed that the COVID-19 vaccine can prevent both symptomatic and asymptomatic infection in among adult HCWs. 20
It is noteworthy, that the success of any vaccination programme is highly dependent on the vaccine acceptance and uptake,20,21 while the main setback lies on getting the population to trust the emergent–release vaccine. Vaccine hesitancy is imminent in the presence of mistrust and lack of confidence in the vaccine.22,23 In the light of this, it is pertinent to look at the real-time acceptability rate and barriers to COVID-19 vaccination, as their acceptability would help address the barriers to wide acceptability among the populace.
Methods
Study design
A cross-sectional analytical study was employed to determine the acceptability and effects of the COVID-19 vaccine among HCWs at Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH).
Study population
The study was conducted among HCWs in COOUTH, Amaku, Nigeria.
Study site
COOUTH, Amaku-Awka, Anambra State Nigeria was the study site. The hospital is a tertiary healthcare institution responsible for postgraduate medical training and boasts of numerous consultant obstetricians and resident doctors (registrars and senior registrars). It is the only state teaching hospital in Anambra State and sub-serves the state and parts of Delta, Imo, and Enugu states of the country.
Eligibility criteria
Inclusion criteria
The participants include all HCWs aged between 18 and 60 years who received the COVID-19 vaccine between 18 April 2021 and 25 July 2021 at COOUTH, Amaku, Awka, Anambra State, Nigeria. They signed an informed consent form, and only HCWs such as medical doctors, nurses, physiotherapists, laboratory scientists, cleaners, and administrative personnel in any department of the Hospital were sampled.
Exclusion criteria
Non-HCWs were excluded.
Sample size determination
The minimum sample size was calculated using the formula

where N = sample size;
Z = standard normal deviation at 95% confidence interval which is 1.96;
d = degree of precision set at 0.05;
P = proportion of the target population;
*In this case, corona vaccine acceptance rate in a Congo study
Q = alternate proportion (1 – P)
Therefore


To account for attrition:
New sample size N1 was then
N1 = calculated sample ×
where



Hence, a total of 105 subjects were used as the minimum sample size for the study.
Sample technique
A non-random sampling approach was used and all available case files or data from all the personnel vaccinated were also considered in the study.
Data collection and management
A structured questionnaire was used to collect socio-demographic and clinical data of the participants.
The participants were duly informed about the study protocol using an information sheet, which was written in a plain language. They also signed informed consent forms prior to the commencement of the study. They were later interviewed in private by the researcher in the vaccination clinic, and information on socio-demographic characteristics as well as relevant history was obtained using a questionnaire which was number-coded to ensure confidentiality. Data collected were analysed using SPSS 26.0 IBM Corporation. Fisher’s exact test was performed for categorical data, Student’s t-test, or Mann–Whitney U-test was applied to continuous variables depending on their distribution, and a p value < 0.05 was considered statistically significant.
Result
From February to April 2022, the COVID-19 vaccine questionnaires were completed for 100 HCWs in Awka, Nigeria. Table 1 presents the participants’ socio-demographic characteristics. Most of the participants were in the age group 30–39 years and were educated, with 65.66% of the participants having obtained a bachelor’s degree. None of the participants was illiterate. The majority (63.0%) of the participants were females.
Showing the socio-demographics of the study participants (N = 100).

FSLC, First School Leaving Certificate; SD, standard deviation; SSCE, senior school certificate.
18 participants did not specify their age.
Only 86 reported their ethnicity.
82 participants specified their years of working experience.
Nigeria students are awarded this certificate on taking the FSLC examination after completing the grade six elementary class.
Table 2 describes the specific occupations of the study participants. Overall, majority (19.19%) of the participants were nurses, followed by medical doctors (16.16%) and pharmacists (13.13%).
Showing the occupation of the study participants.

Table 3 presents data about the sources of information on COVID-19 of the study participants. Overall, 97.98 % of participants stated that they had heard of the novel COVID-19 virus.
Showing sources of information on COVID-19 of the study participants.
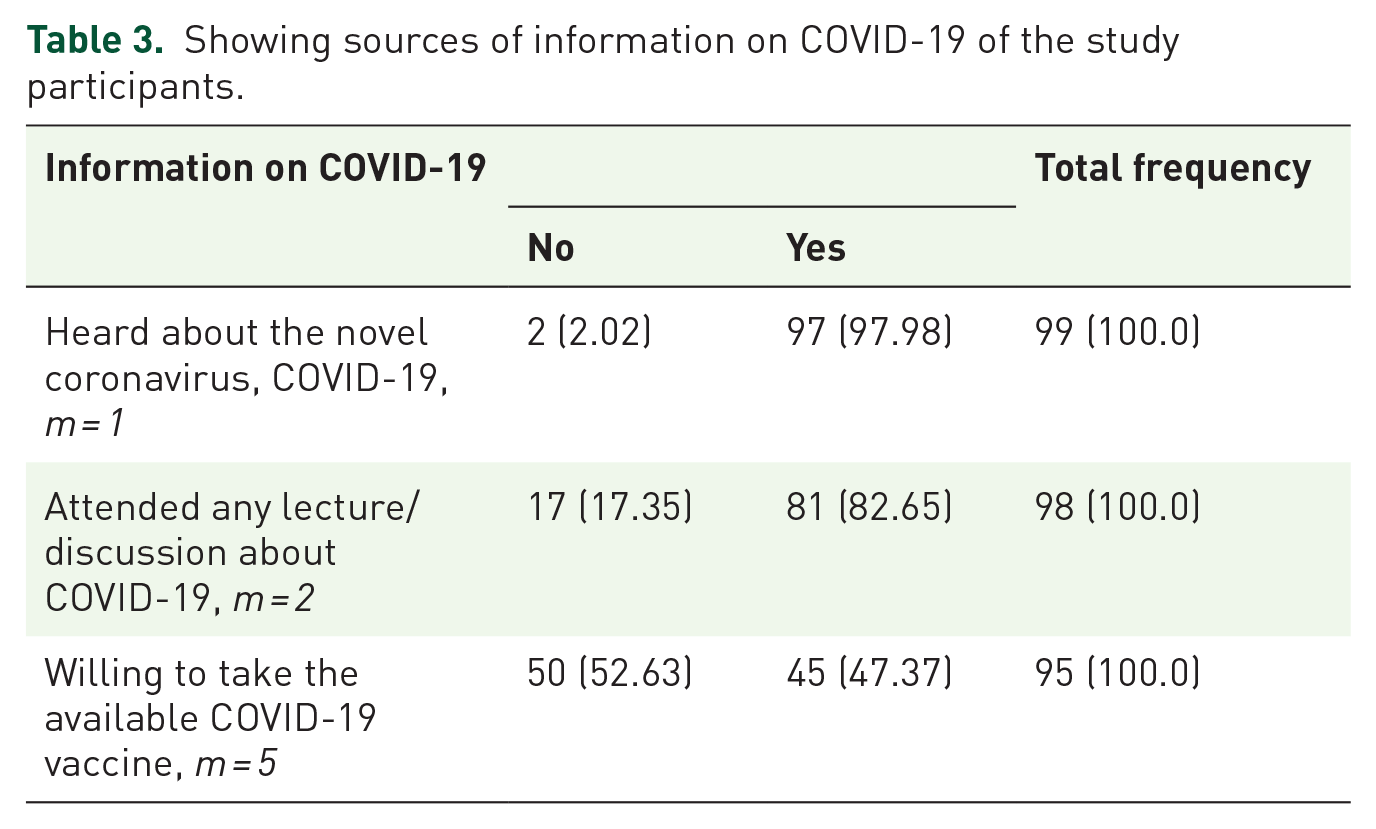
Table 4 shows the HCWs status in relation to COVID-19 among the study participants. Nearly 80% of the participants were frontline health workers. Table 5 describes the gender barriers preventing the study participants from receiving/accepting the COVID-19 vaccine. Pregnancy (2.00%) and breastfeeding (2.00%) were identified as gender-specific barriers, but the majority (87.0%) of participants did not report being affected by any gender-specific barriers.
Showing the healthcare workers status in relation to COVID-19 among the study participants. m = 8.

Barriers against COVID-19 vaccination among the study participants.

Table 6 presents the level of risk posed by the study participants to others. Up to 24.74% of the participants were greatly concerned about infecting others with COVID-19 and getting infected with COVID-19 (42.27%).
Showing the level of risk posed by the study participants to others.

Table 7 describes the COVID-19 status of the family members of the study participants. Up to 75.76% of participants revealed that none of their family members had COVID-19, and none of their family members were currently infected with COVID-19 (89.00%).
Showing the COVID-19 status of the family members of the study participants.

M, missing values.
Table 8 described the test of association between socio-demographics and acceptability of COVID-19 vaccine among the study participants. Ages 30–39 years had the highest acceptance rate of COVID-19 vaccination 19 (47.5%; p value = 0.262) with a more female preponderance of COVID-19 vaccine acceptance compared to males [26 (41.3%) vs 16 (42.2%), p = 0.721]. However, the p value for both these confrontations are >0.05, thus rendering them statistically non-significant. The place of residence of respondents (urban vs rural) and their marital status (married vs single) appeared not to influence the acceptance of COVID-19 vaccination [(38 (42.2%) vs 3 (33.3%); p = 0.667; 25 (36.8% vs 17 (54.8%); p = 0.433)]. Years of work experience (<10 years vs >10 years) significantly affected COVID-19 vaccine acceptance [27 (45.8%) vs 12 (52.2%); p = 0.029].
Test of association between socio-demographics and acceptability of COVID-19 vaccine among the study participants.

FSLC, First School Leaving Certificate; SSCE, senior school certificate.
18 participants did not specify their age.
56 participants don’t know.
Discussion
At the time of this study, 45.0% of the studied HCWs had received the COVID-19 vaccine, while the barriers to vaccination of frontline health workers in Awka, Nigeria was relatively unknown. This acceptability rate is less than the 67% quoted by Di Gennaro et al. 25 in their Italian HCW correspondents and even lesser than the 80.9% reported by Dzieciolowska et al. 26 in their Canadian study among health workers. Similarly, in a recent systematic review and meta-analysis aimed at estimating the proportion of HCWs in Italy who expressed COVID-19 vaccine hesitancy, it was revealed that the vaccine hesitancy rate among HCWs was 13.1%. 27 The systematic review further revealed that the vaccine hesitancy rate among HCWs investigated before and during the vaccination campaign was 18.2% and 8.9%, respectively. 27
The mean age of participants was 35.5 ± 7.971 and was higher than figures obtained by Germann et al. 28 which was 29.5 ± 5.10 years. Germann believed that older, parous employed and individuals with higher educational attainment were more likely to be vaccinated, but this was not so in our findings. The age of the individual, sex, and educational status appeared to influence uptake of vaccination. Dzieciolowska et al. 26 reported that male gender and age above 50 years were independently associated with vaccine acceptance, while Zammit et al. 29 reported that female gender, working in the capital, and having concerns about the vaccine components predicted more hesitancy among participants. However, what was obvious in our study was the effect of years of work experience on uptake of vaccination. It appeared as if the lesser the years of work, the better the uptake of vaccination. The explanation may be due to the enforcement of vaccination as a measure of employment by different parastatals. Alyu et al. 30 showed that there was higher vaccine uptake in higher monthly income earners and in HCWs working in the non-governmental sector. Nevertheless, participants aged 30–39 years reported the highest acceptance rate of COVID-19 vaccination, and the increase in female preponderance of COVID-19 vaccine acceptance compared to males did not reach a significant level in this study.
Income, place of residence, marital status, and educational status appear not to influence the uptake of COVID-19 vaccination. For better coverage of vaccination, the distribution of vaccination was per local government while observing strict vaccine cold chain. A high-quality cold chain allows health workers to deliver life-saving vaccines to every patient who needs it. The cold chain acts to preserve biological product quality from the time of manufacture until the point of administration by ensuring that the vaccines are stored and transported within the recommended temperature ranges. 31 Establishing a secure cold chain management of global vaccine chain supply is critical. As a result, innovative technologies and techniques are needed to simplify vaccine distribution, by minimizing the need for a cold chain. 31 Improvements in the stringent cold chain storage requirements can be made by improving vaccine formulation. One approach is to eliminate the cold chain altogether by making vaccines that can withstand more natural temperatures. 31 Another method would be to stabilize vaccines through improved formulation, such as excipient innovation, protein engineering, and lyophilization if suitable. 31
There was no premium placed on different local government areas or income of individuals per say during COVID-19 vaccination. The higher the educational attainment, the more likely the individual is to be vaccinated according to Germann et al, in their study done in Ohio, USA. It may be possible that the varied ethno-cultural and religious plurality of Nigeria may have had an affect on the decision making process in individuals with an average education. The reason for acceptability and non-acceptability of COVID-19 vaccine intake was spread across the following reasons/statuses: breast feeding, previous COVID-19 vaccination, illness, infertility among men, life barriers, pregnancy, and lactation. There were different conspiracy theories on COVID-19 vaccination that possibly delayed the uptake world wide. 31 Dzieciolowska et al. 26 identified factors that led to vaccine hesitancy as vaccine novelty, wanting others to receive it first, and insufficient time for decision making. Germann et al., found 93% COVID-19 vaccine hesitancy in the pregnant population. 28 This may follow the initial restrictive recommendation of COVID-19 vaccination in pregnancy.
The findings of our study are generally consistent with another study conducted in a non-health worker population in Awka, Nigeria, a city with similar incidence of COVID-19 cases. This study found that the COVID-19 hesitancy rate was 65.04%, and the strongest predictors related to vaccine acceptance were marital status, age, and Christian denominational affiliation. 32 Conversely, in this previous study in the non-health worker population, gender, occupation, previous vaccination experience, awareness of COVID-19, and previous symptoms of COVID-19 did not significantly (p = 0.05) influence respondents’ willingness to be vaccinated. 33
Based on the findings of this study, there is a need to strengthen the importance of information, communication, and organizational and educational strategies to reduce vaccine hesitancy. For example, in a recent cross-sectional descriptive study, Tomietto et al. 34 aimed at determining COVID-19 vaccination hesitancy in healthcare professionals and healthcare students in Italy across four generations. The results showed that worries about unforeseen future effects accounted for the higher vaccination hesitancy factor across generations. The results suggest that public health campaigns should consider the generational differences in COVID-19 vaccination hesitancy to achieve higher levels of vaccine acceptance, including among healthcare professionals and students. 34 Vaccination remains the utmost operational strategy to tackle the COVID-19 pandemic. The advice of health professionals strongly influences vaccination willingness in the general population. A consideration of the generational patterns in the COVID-19 vaccination hesitancy of HCWs and students may increase vaccination uptake in these populations, which in turn may lead to greater public acceptance of the vaccine. In addition, Toth-Manikowski et al. 35 adapted a survey using the Health Belief Model framework to evaluate HCWs vaccine hesitancy and reasons for choosing for or against COVID-19 vaccination. The results showed that HCWs were less likely to receive COVID-19 vaccination if they were Black, Republican, or allergic to any vaccine component and more likely to receive if they believed people close to them thought it was important for them to receive the vaccine. The study concluded that a sizable number of HCWs remain vaccine hesitant 1 year into the COVID-19 pandemic. 35 As HCWs are positively influenced by colleagues who believe in COVID-19 vaccination, development of improved communication across HCW departments and roles may improve vaccination rates. 35
Our study has some limitations and some strengths. Among the strengths are the hospital population-based data from the study site as well as the standard data collection protocol used in the study site. One of the weaknesses is the single site nature of the study, which may have affected the observed findings of the barriers and acceptability of COVID-19 vaccination. Another limitation is the lack of available data about the status of the pandemic in the study site, the ongoing educational efforts at the each site, and our limited knowledge of how each of these factors influences the participants’ acceptability of COVID-19 vaccination. In addition, the presence of missing data affects the quality of the data set, which impacts on the analysis and interpretation of the data. Therefore, our findings should be taken with caution due to the missing data. In addition, in this study, technical and economic limitations occurred, which drastically affected the sample size of participants included in the study. Therefore, the sample size was built keeping into consideration the feasibility of the study itself in a difficult researching context.
Conclusion
At the time of this study, the uptake of COVID-19 vaccination was suboptimal among HCWs working in Awka metropolis in Nigeria. The majority of HCWs were unsure about the efficacy of this vaccine. There is a need for more scientific research and further public health education among healthcare workers to encourage larger vaccine uptake.