
Abstract
This study aims to analyze the global research landscape on Willingness to Pay (WTP) for Community-Based Health Insurance (CBHI) from 2002 to 2024. It seeks to identify key trends, influential contributors, regional disparities, and thematic focus areas, offering insights to guide future research and policy development. A bibliometric analysis was conducted using 354 documents sourced from Dimensions, Scopus, and PubMed. The Bibliometrix package in R Studio, along with the Biblioshiny application, was employed to examine publication trends, citation metrics, collaboration networks, and keyword distributions. Bradford’s and Lotka’s Laws were applied to evaluate journal productivity and author contribution patterns. Data visualizations, including geographical distribution maps and author productivity charts, were used to present findings. The analysis revealed an annual publication growth rate of 10.12%. Ethiopia led in research output (15.8%), while Burkina Faso’s publications were most cited. International collaborations were present in 31.64% of studies, indicating increasing global engagement. Key publishing journals included BMC Health Services Research and PLOS ONE. Influential authors such as Sauerborn R and De Allegri M emerged as central figures in the field. The field of WTP for CBHI is expanding and contributing to the discourse on healthcare financing and equity, especially in LMICs. However, research contributions were regionally skewed, with underrepresentation from South America and Oceania, and a notable reliance on a small group of productive authors. To strengthen CBHI’s potential for achieving universal health coverage, it is crucial to address regional research disparities, foster interdisciplinary collaboration, and explore emerging areas such as behavioral economics and technology integration.
Keywords
Introduction
Community-Based Health Insurance (CBHI) has emerged as a critical mechanism for improving healthcare access and financial protection in low- and middle-income countries (LMICs).1,2 With rising healthcare costs and inequitable access to traditional insurance systems, CBHI offers a potential solution to bridge the gap between affordability and quality care. Willingness to pay (WTP) serves as a vital metric for understanding the feasibility and sustainability of CBHI schemes. By examining how much individuals are willing to contribute, policymakers can design and implement programs that align with community needs and preferences.3–5
Community-Based Health Insurance (CBHI) is a non-profit health insurance model designed to provide financial protection and improve healthcare access for low-income rural households in developing countries.6,7 CBHI schemes rely on members paying small premiums into a collective fund, which is then used to cover health services. 7 The success of CBHI is closely linked to social capital within communities. 6 Community-Based Health Insurance (CBHI) has gained global attention as a pathway toward universal health coverage in low- and middle-income countries.8,9 Ethiopia introduced CBHI in 2011 to reduce out-of-pocket health expenditures and increase service utilization. 9 Factors positively influencing CBHI enrollment include household income, education, age of household head, and understanding of the scheme. 10 However, cost remains a significant barrier to enrollment, particularly for vulnerable households. 8
Access to affordable healthcare remains a pressing global issue, particularly in LMICs where formal insurance coverage is limited. Community-Based Health Insurance (CBHI) models are increasingly being adopted to address these gaps. However, the success and scalability of these models are contingent upon the population’s WTP, which serves as a proxy for perceived value and feasibility. Despite growing academic interest in CBHI, systematic evaluations of research trends, regional disparities, and collaborative networks remain scarce. Moreover, prior studies have not adequately integrated theoretical perspectives to explain variations in WTP across contexts, leaving a conceptual gap that this study aims to address. Given the global push toward Universal Health Coverage (UHC), as highlighted in Sustainable Development Goal (SDG) 3.8, understanding the research landscape of WTP for CBHI is both timely and policy-relevant. Importantly, research on WTP for CBHI also has direct implications for health equity. By identifying the financial thresholds at which low-income and marginalized groups can participate, such evidence informs the design of subsidy mechanisms, cross-subsidization strategies, and progressive premium structures.
Over the past two decades, CBHI has gained significant global attention, reflected in the growing body of academic literature. However, research contributions remain unevenly distributed, with notable gaps in underrepresented regions. This study aims to provide a comprehensive bibliometric analysis of WTP for CBHI, shedding light on identify key trends and growth patterns in the field over the past two decades, highlight major contributors, including authors, countries, and institutions, examine the extent of international collaboration and regional disparities in research contributions and areas for future exploration.
Theoretical framework
The study of WTP for CBHI draws upon several interrelated theoretical perspectives from health economics, behavioral science, and bibliometric theory. These frameworks help explain both the empirical dynamics of WTP in diverse socio-economic contexts and the patterns observed in scholarly research on the topic.
Economic and behavioral foundations of WTP in CBHI
At the microeconomic level, WTP is grounded in the theory of demand for healthcare, which posits that individuals make healthcare purchasing decisions based on perceived utility, income constraints, and expected benefits relative to cost. 11 In the context of CBHI, contingent valuation methods (CVM) are often used to elicit WTP, relying on stated preference theory to measure the monetary value individuals assign to hypothetical health insurance scenarios. 12
The expected utility theory provides a rational-choice framework in which households evaluate the trade-offs between paying regular premiums and the anticipated risk reduction associated with healthcare cost coverage. 13 However, in LMIC settings, decision-making is also influenced by behavioral economics—including bounded rationality, loss aversion, and trust in local institutions—which can lead to deviations from purely rational models.14,15 For instance, social capital theory highlights how collective trust, community participation, and norms of reciprocity influence CBHI uptake and WTP.16,17 Communities with high social cohesion may demonstrate higher WTP due to greater confidence in scheme management and equitable benefit distribution.
Universal health coverage (UHC) and policy frameworks
The conceptual link between CBHI and UHC is anchored in the global health policy discourse, notably the World Health Organization’s health financing framework, which emphasizes financial risk protection, equity in access, and responsiveness to population needs. 18 WTP studies provide critical insights into the affordability and sustainability of CBHI as a mechanism to advance UHC, particularly in regions where formal insurance markets are underdeveloped. 19 In alignment with SDG 3.8, the assessment of WTP informs policy strategies aimed at reducing out-of-pocket expenditures and promoting inclusive health financing models.20,21
Bibliometric laws and the structure of scientific knowledge
In examining the research landscape itself, this study applies established bibliometric theories to understand the distribution and concentration of scholarly activity:
Bradford’s Law of Scattering explains how research on WTP for CBHI is dispersed across a variety of journals, identifying a small core set of high-impact outlets followed by zones of less concentrated publication activity. 22
Lotka’s Law of Scientific Productivity describes the skewed distribution of author contributions, where a small number of highly prolific researchers produce a disproportionate share of publications. 23
These bibliometric principles allow for the systematic mapping of intellectual production and help identify influential contributors, underrepresented regions, and potential gaps in knowledge dissemination.
Integrative perspective
By combining economic theory, behavioral insights, health policy frameworks, and bibliometric analysis, this study situates WTP for CBHI within a multi-dimensional conceptual model. This integrated approach acknowledges that willingness to pay is not solely determined by economic capacity, but is shaped by cultural norms, institutional trust, health system design, and the evolving body of scholarly evidence.16–18 Moreover, by applying bibliometric laws, the study extends beyond economic determinants to critically assess how the research field itself is structured, highlighting opportunities for broader collaboration, diversification of research contexts, and theory-driven inquiry.
Research questions and objectives
Research questions
The research questions of the study include:
What are the global publication trends and growth patterns in research on WTP for CBHI from 2002 to 2024?
Who are the most influential contributors (authors, institutions, and countries) in the WTP for CBHI research, and how productive are they according to bibliometric laws?
Which journals are most prominent in this field, and how is research output distributed across sources and regions?
What is the extent and nature of international and interdisciplinary collaboration in WTP for CBHI research, and where are the key regional disparities or underrepresented areas?
Research objective
Major Research Objective of the study was to map and evaluate the global research landscape on willingness to pay for community-based health insurance (2002–2024), highlighting publication trends, key contributors, leading journals, and patterns of collaboration, while identifying regional disparities and gaps in representation.
The specific objectives include:
To analyze global publication trends and growth patterns in research on willingness to pay for community-based health insurance from 2002 to 2024.
To identify and evaluate the most influential contributors—authors, institutions, and countries—and assess their productivity using bibliometric laws.
To determine the most prominent journals in this field and examine the distribution of research output across sources and regions.
To investigate the extent and nature of international and interdisciplinary collaboration, and to pinpoint regional disparities and underrepresented areas in the literature.
Methods
Study design
This study employed bibliometric analysis to evaluate the scholarly output on WTP for CBHI from 2002 to 2024. Bibliometric analysis was chosen for its ability to provide comprehensive insights into the development and structure of a specific research domain over time.
Data collection
Data for this study was collected from four major bibliographic databases: Dimensions (839), Scopus (33) and PubMed (26). Search from 2002 to 2024 using keywords “Willingness to Pay” and “community based health insurance” and specifying research articles only. The search date was December 2024. These databases were selected for their broad coverage of scholarly literature across disciplines. The final dataset comprised 354 documents published in 158 unique scholarly sources (see Figure 1). Careful data cleaning and preprocessing were performed to ensure consistency and remove duplicates before proceeding with the analysis.
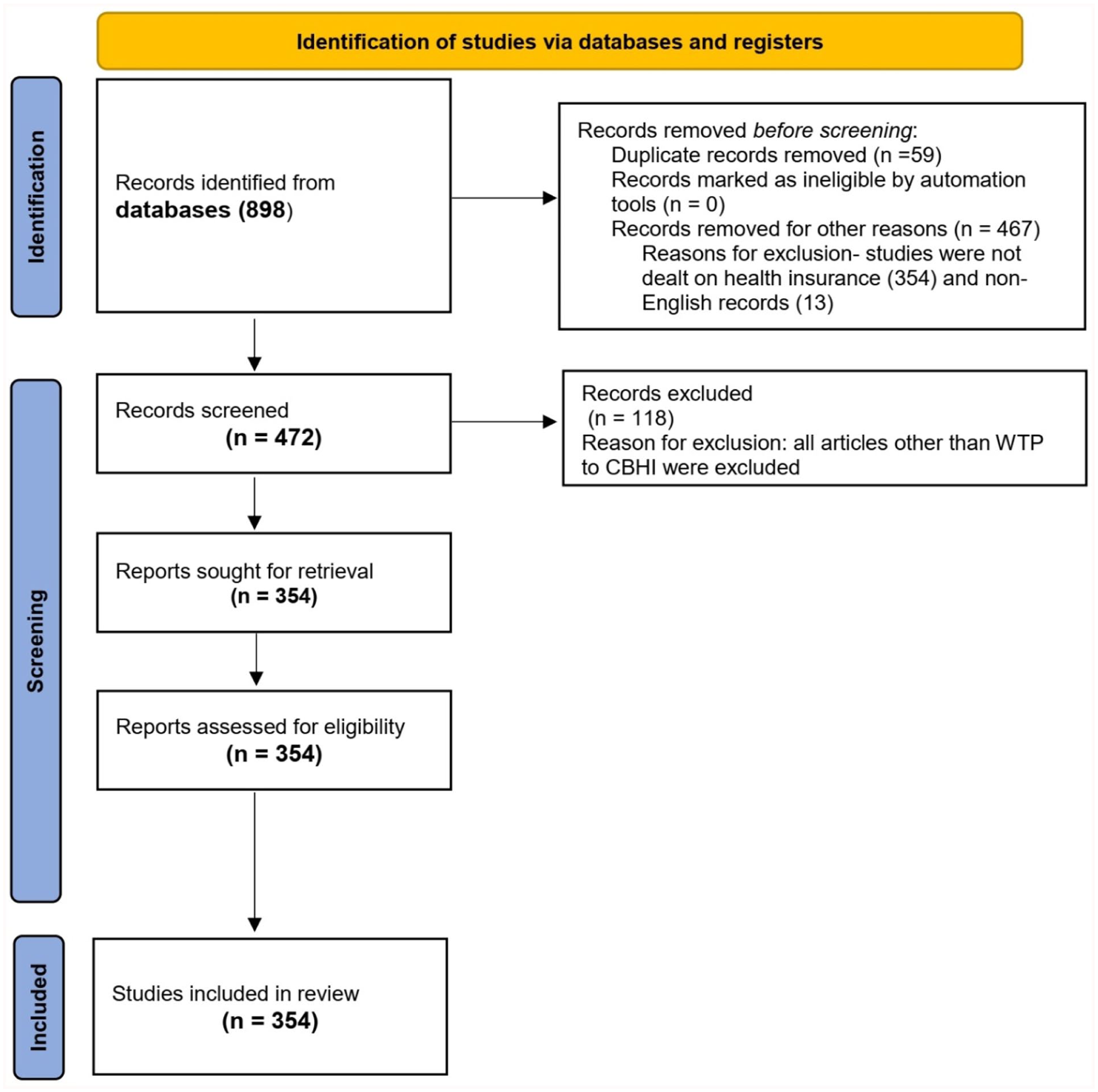
PRISMA flow chart of the study selection process for bibliometric analysis of WTP for CBHI.
The inclusion and exclusion criteria for this systematic review are stated below.
Inclusion Criteria:
Peer-reviewed original research articles.
Published between 2002 and 2024.
Written in English.
Explicit focus on both “WTP” and “CBHI,” as identified through keywords, titles, or abstracts.
Studies involving human populations.
Research centered on CBHI schemes.
Both quantitative and qualitative studies included.
Exclusion Criteria:
Non-peer-reviewed materials (e.g. editorials, commentaries, conference abstracts, book chapters, gray literature).
Systematic review or meta-analysis publications
Articles addressing only one of the two main concepts (WTP or CBHI).
Studies focused solely on national health insurance models not related to CBHI.
Duplicate entries across databases.
Data analysis
The analysis was conducted using R Studio and the Bibliometrix package, along with its Biblioshiny application, which provides an interactive interface for bibliometric analysis and visualization. 24 These tools facilitated the examination of key metrics, including annual growth rates, citation trends, and author productivity. Collaboration indicators, such as the average number of authors per document and international collaboration rates, were calculated to evaluate the extent of interdisciplinary and international partnerships. Additionally, keyword analysis was performed to identify thematic trends and assess the research field’s focus areas. Theoretical frameworks, including Bradford’s Law 25 and Lotka’s Law, 26 were applied to provide further insights into the structure of the field. Bradford’s Law was used to identify core journals based on citation frequency, with journals divided into three Bradford zones. The “core journals” were those in the first zone, which collectively accounted for approximately one-third of all citations—this threshold follows the standard 1: n: n² distribution model recommended in Bibliometrix. Lotka’s Law was employed to examine author productivity, identifying highly prolific contributors by comparing the number of authors to their publication output frequency.
Citation metrics, including total citations and average citations per year, were analyzed to assess the impact and longevity of publications. To visualize the findings, various graphical representations were generated. For all analyses, default settings in Biblioshiny were used unless otherwise specified, including a minimum citation threshold of 5 for inclusion in citation analyses. Geographical distribution maps were created to illustrate the global research activity on WTP for CBHI, highlighting regional contributions. Author productivity charts were also developed to showcase the contributions of individual researchers and institutions over time. These visualizations provided a spatial and temporal perspective on the research landscape.
Results
Collection description
The bibliometric analysis of research on WTP for CBHI spans from 2002 to 2024, reflecting over two decades of scholarly attention. A total of 354 documents from 158 unique sources have been analyzed, indicating a substantial body of literature in this field. The research has grown steadily, with an impressive annual growth rate of 10.12%, demonstrating increasing interest over time. The analysis reveals a high degree of collaboration, as evidenced by the 1169 contributing authors and an average of 4.18 co-authors per document (See Figure 2).

General information and summary of WTP for CBHI bibliometrics analysis. The dataset shows zero references due to incomplete data extraction.
Only 36 documents were authored by single individuals, further emphasizing the collaborative nature of this research. International collaboration is significant, with 31.64% of the documents involving authors from multiple countries, highlighting the global relevance of CBHI studies. Researchers have employed 270 distinct keywords, reflecting the diversity of topics within the field. On average, the documents are 6.41 years old, balancing recent and slightly older studies. With an average of 23.58 citations per document, the research in this area appears to have a strong academic impact. However, the dataset shows zero references, which might indicate incomplete data extraction and warrants further investigation. Overall, the analysis points to a thriving and impactful field that continues to grow and attract global collaboration.
Publication and citation growth trends
Trends in annual publication volume and citations
Figure 3(a) illustrates the annual scientific production of articles related to willingness to pay for CBHI. Over the years, there has been a general upward trend, reflecting growing academic interest and research activity in this area. During the early years (2002–2010), research activity was relatively low, with fewer than 10 articles published annually. Although there were minor fluctuations, the overall production remained limited during this period. From 2010 onward, a significant increase in research is evident, with notable peaks around 2014 and 2018, indicating heightened global interest. This period aligns with an increasing focus on health financing mechanisms aimed at improving equity and financial protection in healthcare. In recent years (2020–2024), scientific production surged, reaching its highest point in 2023 with over 40 articles published. However, a decline is observed in 2024, which might suggest a slowdown in research momentum, data incompleteness for that year, or a potential shift in academic focus. The overall growth in research output likely reflects the increasing global emphasis on achieving universal health coverage and addressing financial barriers to healthcare. The recent dip in 2024 warrants further investigation to understand its cause—whether it indicates saturation in the research field or is a temporary anomaly.

(a) Annual scientific production of WTP for CBHI. (b) Average article citations per year of WTP for CBHI.
Figure 3(b) illustrates the average number of citations received annually by a set of publications between 2002 and 2024. The graph shows a fluctuating trend, with average citations varying between approximately 2 and 5 per year for most of the timeline. There are notable peaks in the mid-2000s and again around 2018–2020, indicating periods when the publications had higher citation impact. However, a significant observation is the sharp and steep decline in average citations starting around 2020, dropping nearly to zero by 2024. This decline may reflect the reduced citation impact of recent publications, though it is more likely a consequence of the natural delay in accumulating citations for newer articles, as they typically take time to be recognized and referenced in subsequent work. The year-to-year fluctuations in average citations may be influenced by various factors, such as changes in the popularity or impact of research topics, the number of publications in each year, or the characteristics of the dataset analyzed. Peaks could represent particularly influential publications or trends, while troughs might indicate years with less impactful research or fewer publications. The recent dramatic decline, while striking, should not necessarily be interpreted as a decrease in research quality; instead, it may simply highlight the need for more time for recent works to gain citations.
Table 1 provides an overview of citation trends for scholarly articles published over several years. The data reveals significant variability in citation impact across years. For example, articles from 2002 show the highest MeanTCperArt (58.33), reflecting a strong long-term impact, although the small number of articles (N = 3) influences this average. These older articles have had the longest time to accumulate citations (23 years), resulting in a moderate MeanTCperYear of 2.54.
Annual total citation per year of WTP for CBHI.

MeanTCperArt: mean total citations per article; MeanTCperYear: mean total citations per year.
Notable variability is observed across years, with 2007 exhibiting a high MeanTCperArt (86.00) despite being based on a single article, making the result less representative. In contrast, years like 2009 show high MeanTCperYear (4.88), indicating significant annual impact even with fewer articles (N = 3) and a shorter time frame (16 years since publication). Articles from 2011, the most recent year in the analysis, have a lower MeanTCperArt (21.11) and the lowest MeanTCperYear (1.51), likely reflecting the shorter time since publication and potentially lower initial impact. Older articles tend to accumulate citations steadily over time, as seen in their high MeanTCperArt, but their annual citation rates (MeanTCperYear) decline as the articles age. Peaks in annual impact, such as those seen in 2007 and 2009, are likely driven by high-impact articles published in smaller numbers. While the metrics provide valuable insights, the variability in article counts and the influence of outliers highlight the need for complementary analyses, such as examining citation distributions or citation half-lives, to gain a more nuanced understanding of the trends.
Geographical distribution map of countries/regions cooperation
Countries’ scientific production
Figure 4(a) highlights the global distribution of scientific production related to “WTP for CBHI.” Countries are shaded in varying intensities of blue, with darker shades representing higher research contributions. Notably, the darkest blue region, likely located in East Africa, suggests that countries such as Ethiopia or Kenya have made significant contributions to research in this area. Other regions across Africa, Asia, Europe, and North America show moderate levels of scientific activity, as indicated by lighter blue shading. In contrast, South America, parts of Central Asia, and Oceania exhibit minimal contributions, shown by gray or very light blue colors. This distribution reflects the relevance of CBHI in regions where traditional health insurance systems are less developed, such as parts of Africa, which have a higher research focus due to practical implementation challenges. Meanwhile, developed countries like the United States and some European nations may be contributing through academic research, funding, or policy evaluation studies. The map underscores global disparities in research productivity, highlighting strong regional interest in CBHI where it is most needed while revealing gaps in contributions from other parts of the world.
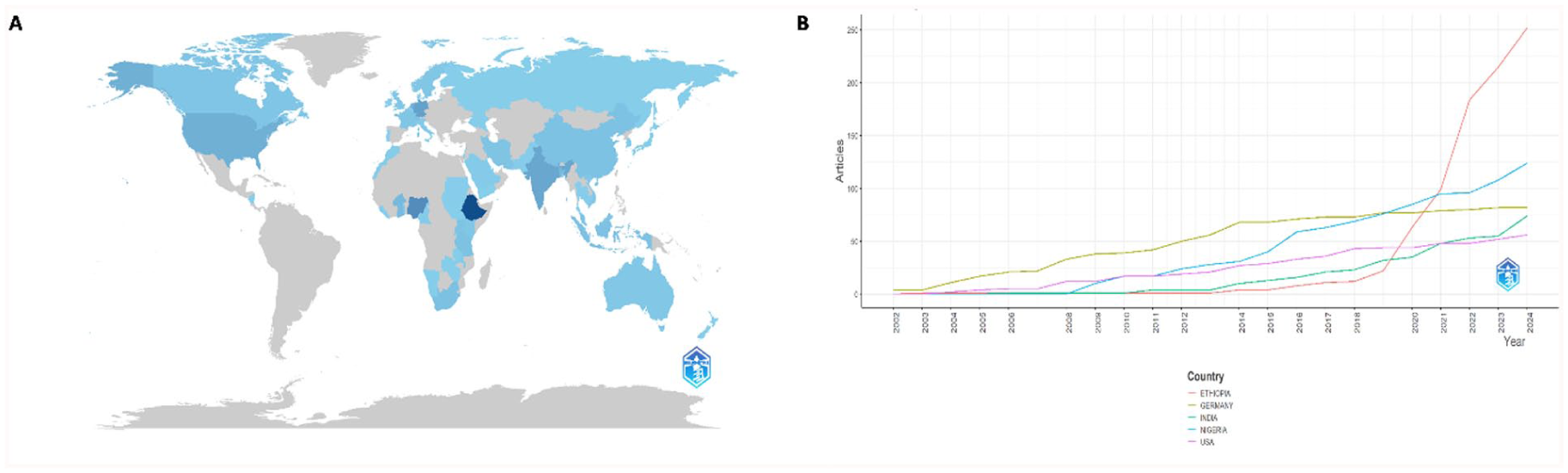
(a) Countries’ scientific production on WTP for CBHI. (b) Countries’ production over time on WTP for CBHI.
Figure 4(b) illustrates the growth in article production on the topic of “WTP for CBHI” across Ethiopia, Germany, India, Nigeria, and the USA over time. Ethiopia stands out with a dramatic surge in research output beginning around 2020, surpassing all other countries by 2023. This rapid growth suggests a significant recent focus on CBHI in Ethiopia, likely driven by the relevance of the topic to local policy or implementation efforts. In contrast, Germany, India, Nigeria, and the USA show steady but moderate growth in article production over the years, reflecting sustained but less intensive engagement compared to Ethiopia.
Between 2002 and 2010, all countries exhibited minimal contributions, indicating that the topic had not yet garnered substantial global research attention. However, post-2010, a gradual increase in article production is evident across all countries, with Germany and the USA maintaining consistent output, while India and Nigeria show slower but steady progress. Ethiopia’s recent surge may highlight emerging research and practical interest in addressing healthcare financing challenges in low- and middle-income countries (LMICs). This trend underscores the growing importance of CBHI globally and suggests opportunities for collaborative research to further explore its implementation and impact, especially in regions like Africa, where the need for such schemes is pronounced.
Most cited countries and country co-authorship network of publications
Figure 5(a) highlights the most cited countries in studies related to WTP for CBHI. Burkina Faso leads with the highest number of citations (989), indicating its significant scholarly impact and the prominent focus of CBHI-related research in this country. Germany follows with 776 citations, reflecting its important role in contributing to CBHI literature, possibly through comparative studies or as a partner in research initiatives targeting low- and middle-income countries. Ethiopia ranks third with 711 citations, demonstrating strong research activity and relevance to the topic. Other notable contributors include Canada (563 citations), Kenya (448 citations), and Bangladesh (348 citations), underscoring their considerable involvement in the discourse on CBHI and WTP. France, Nigeria, South Africa, and China also feature in the analysis but with fewer citations, suggesting either more specialized studies or a secondary interest in the topic. The mix of high-income countries (Germany, Canada, France) and low- and middle-income countries (Burkina Faso, Ethiopia, Kenya, Bangladesh) reflects a global research interest in CBHI. It also emphasizes the critical role of CBHI in addressing health financing challenges, particularly in developing countries where health insurance mechanisms are essential for achieving universal health coverage.

(a) Most cited countries on WTP for CBHI research. (b) Country of collaboration map on WTP for CBH research.
Figure 5(b) visually represents the global network of research collaborations between countries, highlighting their geographical and collaborative dynamics. The map reveals notable hubs of activity, such as the United States and European countries, which appear to have extensive collaborations spanning multiple regions. European countries demonstrate strong regional partnerships, while the United States is a major global hub, linking with numerous countries across Europe, Asia, and Africa. There is also evidence of collaborations between the Global North and Global South, particularly involving African and Asian nations, though these connections appear less intensive than those between Global North countries.
National and institutional analysis
Table 2 provides insights into the most relevant countries contributing to research on WTP for CBHI based on corresponding authors. Ethiopia leads the field with 56 articles, representing 15.8% of the total. Most of these publications (52) are Single Country Publications (SCPs), while only four are Multiple Country Publications (MCPs), with MCPs accounting for 7.1% of Ethiopia’s output. Nigeria follows with 29 articles (8.2%), primarily SCPs (27), and a small fraction (6.9%) as MCPs, indicating limited international collaboration.
The top 10 countries contributing to publication in WTP for CBHI.

SCP: single country publications; MCP: multiple country publication.
Burkina Faso, with 20 articles (5.6%), stands out for its high level of international collaboration, as 85% of its publications are MCPs. India contributes 19 articles (5.4%), with 16 SCPs and 3 MCPs (15.8%). Germany, though contributing only 14 articles (4%), exhibits strong international collaboration, with 71.4% of its publications being MCPs. Similarly, Australia, with 11 articles (3.1%), has an impressive 90.9% of its output as MCPs, showcasing its dominance in collaborative research. Bangladesh and China each contribute nine articles (2.5%), with 66.7% of their publications being MCPs, reflecting significant international partnerships. Canada, contributing eight articles (2.3%), shows an even higher level of collaboration, with 87.5% of its publications as MCPs. Kenya also produces eight articles (2.3%), with 62.5% being MCPs, indicating balanced involvement in both local and collaborative research. These findings highlight Ethiopia and Nigeria as leaders in local research while countries like Burkina Faso, Australia, and Canada excel in fostering international collaboration, enriching the field with diverse perspectives.
Table 3 presents data on the most prolific affiliations contributing to research on Willingness to Pay (WTP) for Community-Based Health Insurance (CBHI). A total of 55 articles were produced by various institutions, with notable contributions from Ethiopia. The Department of Pediatrics and Child Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Ethiopia, leads the affiliations with 19 articles. This is followed by the Department of Statistics, Debre Tabor University, Ethiopia, which contributed 11 articles.
Most relevant institutions contributed to publications in WTP for CBHI.

Two other Ethiopian institutions, the Department of Health Systems and Policy, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar and the Ethiopian Health Insurance Agency in Addis Ababa, both contributed 10 articles each, emphasizing Ethiopia’s dominance in this research field. Internationally, notable contributors include the Department of Global Health/Amsterdam Institute for Global Health and Development, University of Amsterdam, Netherlands, the Department of Tropical Hygiene and Public Health, University of Heidelberg, Germany, and the Nouna Health Research Centre, Burkina Faso, each producing nine articles. Other significant affiliations include the Health Economics and Financing Research Group, Universal Health Coverage, Health Systems and Population Studies Division, ICDDR,B, Bangladesh, and the Institute of Public Health, Medical Faculty, University of Heidelberg, Germany, each with eight articles. This distribution underscores Ethiopia’s leading role in CBHI research, supported by substantial outputs from other global research hubs in Germany, the Netherlands, and Burkina Faso, which contribute through international collaborations and institutional expertise.
Journal analysis
Most relevant sources
Figure 6 shows insights into the research landscape on WTP for CBHI. Leading contributors include BMC Health Services Research (26 articles) and PLOS ONE (23 articles), highlighting their importance as key platforms for studies in health services and public health economics. Other notable journals, such as Health Policy and Planning (17 articles), Social Science & Medicine (15 articles), and International Journal for Equity in Health (14 articles), emphasize interdisciplinary approaches, equity, and policy dimensions critical to understanding WTP for CBHI.
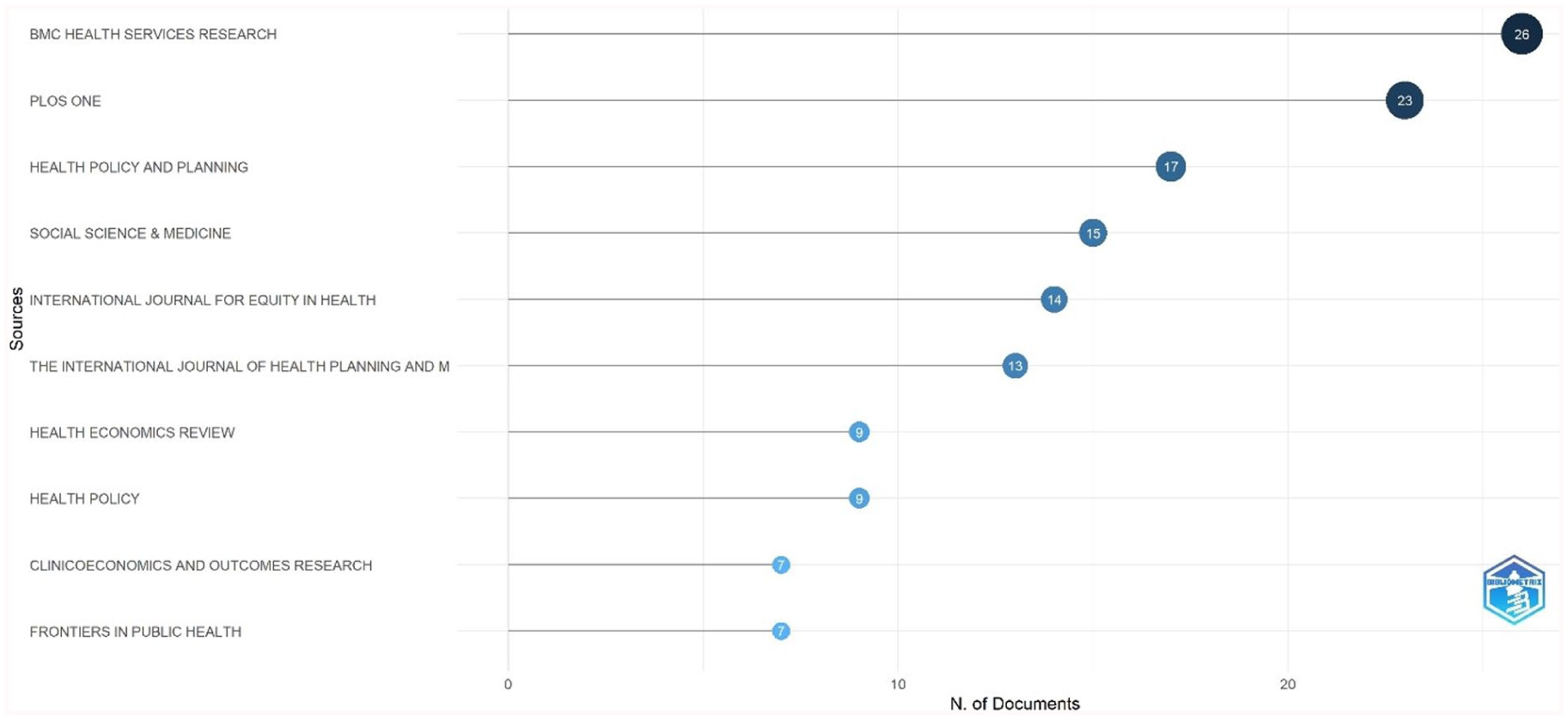
Most relevant sources of WTP for CBHI research.
The concentration of research in these journals reflects a strong focus on both quantitative analyses, such as econometric models, and qualitative studies exploring social acceptability and implementation challenges. Specialized contributions from journals like The International Journal of Health Planning and Management and Health Economics Review underscore the relevance of policy planning and economic evaluations in CBHI schemes. Additionally, the inclusion of ClinicoEconomics and Outcomes Research and Frontiers in Public Health suggests a growing interest in clinical outcomes and broader public health perspectives. This distribution of research underscores the multidisciplinary nature of CBHI, encompassing health economics, social policy, equity, and public health.
Sources’ production over time
Figure 7 depicts the cumulative occurrences of publications over time on the topic of WTP for CBHI, segmented by journal source. There is an overall increasing trend in publications across all sources, reflecting a growing interest and research activity in this field. Among the sources, BMC Health Services Research stands out as the most prolific, particularly after 2012, indicating its central role in disseminating research on this topic. Steady contributions are also observed from Social Science & Medicine and Health Policy and Planning, which show consistent growth over the years, albeit at a slower pace compared to BMC Health Services Research. Notably, PLOS ONE exhibits slower initial activity but shows substantial growth post-2012, highlighting its increasing engagement with WTP for CBHI in recent years. Meanwhile, the International Journal for Equity in Health maintains a steady yet moderate growth, likely due to its focused scope.
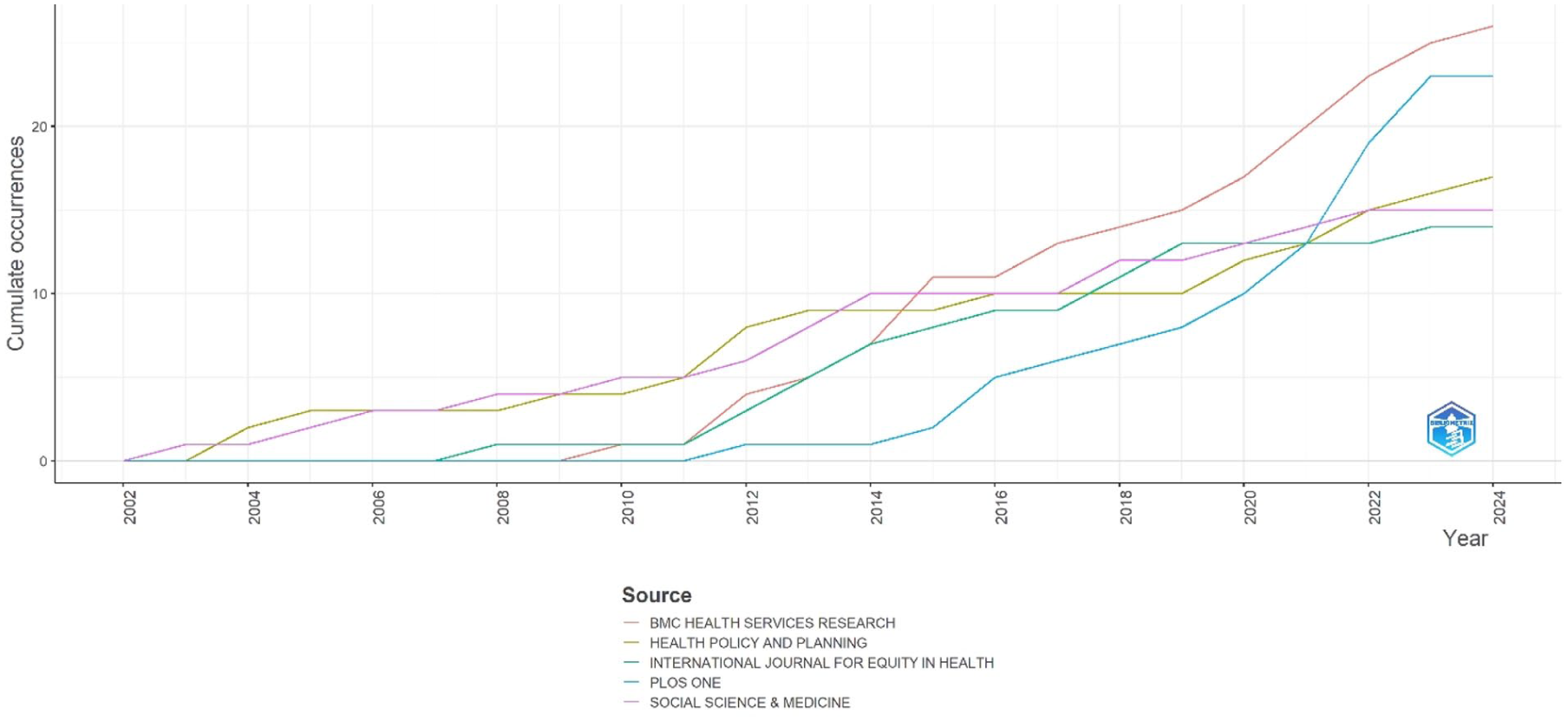
Sources’ production over time on WTP for CBHI research.
In terms of temporal trends, publication activity was relatively sparse across all journals before 2010, indicating that WTP for CBHI was not a major research focus during that period. Between 2010 and 2015, there was a marked increase in publications, with notable contributions from BMC Health Services Research and Social Science & Medicine. After 2015, BMC Health Services Research became the dominant source, while other journals continued to contribute at consistent levels.
Core sources by Bradford’s Law
Bradford’s Law is a bibliometric principle that organizes journals into zones based on their productivity in a specific research field. Table 4 provides categorizes journals on the topic of Willingness to Pay (WTP) for Community-Based Health Insurance (CBHI) into two distinct zones. Zone 1, referred to as the core zone, comprises the most productive journals contributing to the majority of research publications. These include BMC Health Services Research (26 publications), PLOS ONE (23 publications), Health Policy and Planning (17 publications), Social Science & Medicine (15 publications), International Journal for Equity in Health (14 publications), The International Journal of Health Planning and Management (13 publications), and Health Economics Review (9 publications). Together, these journals account for a cumulative total of 117 publications, making them essential sources for foundational and highly relevant research on the topic.
Core sources by Bradford’s law.

In contrast, Zone 2 contains journals that contribute fewer publications but still hold significance in the field. These include Health Policy (nine publications), Clinicoeconomics and Outcomes Research (seven publications), and Frontiers in Public Health (seven publications), collectively adding 19 publications to the total. The distribution reflects Bradford’s observation that a small core group of journals dominates the research output, followed by larger groups with diminishing contributions.
Sources’ local impact
Table 5 highlights the top-performing journals in the field of Community-Based Health Insurance (CBHI) based on various impact metrics. BMC Health Services Research emerges as the leading source with the highest h-index (15), g-index (26), and m-index (1.000), indicating its strong overall impact, productivity, and influence sustained over time. PLOS ONE follows closely, with a notable h-index (12) and g-index (23), and leads in total citations (860), reflecting its widespread recognition and influence in the field. Other key journals include Social Science & Medicine and Health Policy and Planning, both with a strong h-index of 12 and 11, respectively, and significant citation counts. The International Journal for Equity in Health also stands out with a balanced performance across metrics, including an m-index of 0.647 and total citations of 705, emphasizing its role as an impactful journal despite being newer compared to others.
Source impact bibliometrics of WTP for CBHI research.

TC: total citations; NP: number of publications; PY_start: publication year start.
The correlation analysis reveals that citation metrics are closely intertwined, with a strong positive correlation (r = 0.82) between h-index and total citations, suggesting that highly-cited sources are also those with a broader range of impactful publications. Similarly, the g-index correlates strongly with the h-index (r = 0.93), as both metrics measure citation impact but differ in weighting criteria. Interestingly, the m-index, which normalizes h-index by the years since the journal’s inception, highlights newer yet influential sources like Health Economics Review (0.538).
Author and co-cited author analysis
Most relevant authors and authors production over time
Figure 8(a) reports findings on the “Most Relevant Authors” in the field of WTP for CBHI identifies the key contributors based on the number of documents published. The chart highlights Sauerborn R as the most prominent author, with 22 publications, significantly surpassing other contributors. De Allegri M follows with 14 documents, reflecting substantial contributions. A cluster of authors, including Dror DM, Ahmed S, Dong H, Robyn PJ, and Souares A, each have eight publications, demonstrating a shared level of productivity. Additionally, Acharya D, Sanon M, and Sié A each have six publications, showcasing their consistent contributions to the literature on CBHI and WTP. This data underscores Sauerborn R as a leading figure in this research domain, while several other authors contribute notably to expanding knowledge and discussion within the field.

(a) Most relevant authors on WTP for CBHI research. (b) Authors’ production over time on WTP for CBHI research.
Figure 8(b) illustrates the contributions of the Authors’ Production over Time to research on WTP for CBHI over the period from 2002 to 2024. Key contributors include SAUERBORN R and DE ALLEGRI M, who demonstrate consistent and prolific publication records over the years. SAUERBORN R, in particular, appears as a leading figure, maintaining research activity over two decades and producing several highly cited works. DE ALLEGRI M also displays steady contributions, closely mirroring SAUERBORN R in both volume and impact. Other authors, such as DROR DM, show concentrated activity during specific periods, notably between 2008 and 2014, suggesting a significant focus on the topic during that time. Authors such as AHMED S, DONG H, and ROBYN PJ have fewer publications overall, but their works include some impactful studies as evidenced by larger circle sizes in select years. Early contributors like SANON M and SIÉ A show limited activity, primarily concentrated around 2004–2008, while SOUARES A demonstrates consistent but lower-intensity contributions over the years. The chart also reveals trends in publication and citation impact. The most influential years appear to cluster around 2008–2014, with some decline in publication frequency for many authors after 2018, although SAUERBORN R and DE ALLEGRI M remain active. The TC per year data highlights the works that have been widely referenced, emphasizing the influence of specific authors during peak research periods.
Author productivity through Lotka’s Law
Findings on author productivity on WTP for CBHI, highlights significant trends consistent with Lotka’s Law. The data reveals that the majority of authors 1011 (86.5%) contributed only a single document to this research area, indicating a high prevalence of occasional contributors. The number of authors diminishes as their productivity increases, with 98 (8.4%) contributing two documents, 2.7% contributing three documents, and only a handful of authors (less than 1%) producing more than five documents. Notably, just one author each contributed 10, 14, and 22 documents, reflecting the presence of a small core group of highly productive authors driving the field forward. This distribution aligns with the principles of Lotka’s Law, which predicts that the number of authors decreases as their publication count increases, often following an inverse-square relationship. While further statistical analysis would be required to confirm precise adherence to the law, the observed trend supports its general validity.
Authors’ local impact
Table 6 highlights the impact of authors in the field of WTP studies for CBHI through metrics. Among the contributors, SAUERBORN R stands out as a leading figure with the highest h-index (21), TC (1258), and NP (22), reflecting consistent and influential contributions since 2002. Similarly, DE ALLEGRI M demonstrates significant impact, with an h-index of 12, g-index of 14, and TC of 1040, showcasing a balance of productivity and high-citation work since their entry in 2005.
Author impact bibliometric finding on WTP for CBHI research.

TC: total citations; NP: number of publications; PY_start: publication year start.
Emerging contributors like KHAN JAM, who started publishing in 2016, display a high m-index of 0.556, indicating a rapid rise in influence. Authors such as ROBYN PJ, SOUARES A, and DONG H show steady contributions with comparable h-index (8) and g-index (8), reflecting a stable citation impact. Additionally, SANON M demonstrates remarkable citation efficiency, with a high TC-to-NP ratio (419/6), indicating that their fewer publications have had a significant impact. The analysis also highlights the pioneering contributions of early entrants like SAUERBORN R and SANON M, who began their work in 2002.
Authors collaboration network
Figure 9 represents a collaboration network derived from bibliometric analysis of research on “WTP for CBHI.”“ The network highlights distinct clusters of authors, each representing collaborative research groups or geographic regions. A prominent observation is the central role of “Sauerborn R,” whose node is the largest and most connected, indicating significant influence and extensive collaborations in this field. Other key contributors, such as “de Allegri M” and “Robyn PJ,” also feature prominently within the central cluster, suggesting they are pivotal figures in CBHI WTP research.

Authors collaboration network on WTP for CBHI research.
The nodes are color-coded, likely representing different research groups, thematic areas, or geographic focuses. The central blue cluster is dense, reflecting a highly interconnected and dominant research hub. In contrast, smaller, peripheral clusters, such as those associated with “Ahmed S,” “Akazili J,” or “Kagai A,” are relatively isolated, indicating independent or emerging research efforts with limited interaction with the central network. This network demonstrates varying levels of collaboration, with the central cluster acting as a hub of activity and other clusters functioning more independently. The smaller groups may represent niche areas or underexplored topics within CBHI WTP studies. Encouraging greater collaboration between these isolated clusters and the central network could foster knowledge exchange and bridge existing research gaps.
Discussion
The bibliometric analysis of research on WTP for CBHI reveals significant insights into the evolution, focus, and collaboration within this field. Over the span of 22 years, the substantial annual growth rate of 10.12% demonstrates increasing global interest in CBHI as a mechanism for improving healthcare access and equity. This growth is particularly notable post-2010, aligning with heightened global efforts toward achieving universal health coverage (UHC), as outlined in Sustainable Development Goal 3.8. 27 The increasing attention to CBHI reflects its potential to address healthcare affordability challenges, particularly in low- and middle-income countries (LMICs), where out-of-pocket expenses often create significant barriers to accessing care.19,28
In comparing our findings with prior systematic reviews and meta-analyses, important complementarities emerge. Earlier reviews1–3,10,19 have primarily concentrated on identifying determinants of CBHI enrollment, willingness-to-pay thresholds, and sustainability barriers across LMICs. For instance, Dror et al. 10 highlighted socioeconomic and demographic factors such as household income, education, and trust as critical to voluntary uptake, while Fadlallah et al. 2 emphasized challenges of scheme sustainability. Our bibliometric analysis extends these insights by mapping where and how such themes have been studied over the past two decades. Specifically, it reveals that much of the empirical evidence synthesized in prior reviews originates from a small set of countries—most notably Ethiopia and Burkina Faso—reflecting a structural imbalance in the global research landscape. This study complements earlier reviews by moving beyond determinants and outcomes to examine patterns of knowledge production, collaboration, and citation impact.
The collaborative nature of research in this domain is evident, with an average of 4.18 co-authors per document and significant international partnerships in 31.64% of the studies. These collaborations underscore the multidisciplinary and global relevance of CBHI research, particularly in addressing financial barriers to healthcare in LMICs. Collaborative networks facilitate the exchange of diverse perspectives and expertise, enriching the research quality and practical applicability of findings. 29 Regions such as Africa, especially Ethiopia, have emerged as prominent contributors, reflecting the practical application and policy focus of CBHI in these areas. Ethiopia’s prominence can be attributed to its progressive implementation of CBHI schemes, which have provided valuable case studies for scholarly analysis and policy evaluation. 30 Furthermore, the involvement of international organizations and donors in African countries has likely bolstered research efforts and collaborations. 31
The analysis of publication and citation trends highlights periods of increased scholarly impact, such as 2014 and 2018, with notable peaks in citations. The peak in 2014 may correspond to influential studies that shaped the discourse on the sustainability and effectiveness of CBHI models, 32 while the rise in 2018 could reflect heightened global discourse around UHC and innovative financing mechanisms for health. However, the recent decline in 2024 raises questions about either a shift in academic focus or incomplete data for that year. This trend warrants further investigation to determine whether it reflects genuine shifts in scholarly priorities or methodological limitations in data collection. 33 These fluctuations suggest that the field’s dynamic nature is driven by regional healthcare needs, donor priorities, and broader academic trends.
Despite Ethiopia’s dominance in article production, Burkina Faso leads in total citations, showcasing the depth and impact of research originating from this region. This disparity underscores the potential for certain countries to play pivotal roles in advancing CBHI discourse despite fewer contributions in terms of volume. Burkina Faso’s focus on rigorous evaluations of CBHI programs and their long-term impacts has likely contributed to the high citation rates. 34 Similarly, the concentration of research in high-impact journals like BMC Health Services Research and PLOS ONE reflects the field’s interdisciplinary appeal and its anchoring in public health and health economics. Publishing in such journals ensures the dissemination of findings to diverse academic and policy-oriented audiences, amplifying their influence on global health initiatives.
The geographical distribution of research activity highlights significant gaps in contributions from regions such as South America and parts of Asia and Oceania, suggesting untapped potential for expanding the scope of CBHI research. South America’s limited engagement is surprising given the region’s history of community-oriented health initiatives. 35 The regional policy context provides critical explanatory power for the observed geographical disparities. Ethiopia’s prominence in WTP and CBHI research can be traced to its national rollout of CBHI in 2011, subsequent scale-up across districts, and integration with poverty-targeted social protection programs.8,9,30 These efforts generated a fertile policy environment for both domestic universities and international collaborators to engage in empirical research, resulting in Ethiopia producing 15.8% of all publications in this field. By contrast, South America’s underrepresentation reflects the dominance of tax-funded health systems (e.g. Brazil’s Unified Health System) and social insurance reforms (e.g. Colombia), which have reduced the perceived relevance of CBHI as a financing model. 35 Similarly, in Oceania, small and dispersed populations coupled with reliance on donor-driven or publicly funded health systems have limited both implementation and scholarly output on CBHI. 36 These contextual differences suggest that the global distribution of research is shaped not only by academic priorities but also by policy adoption trajectories and financing models, which either create or constrain opportunities for WTP and CBHI-related inquiry. Hence, expanding research into these underrepresented regions could enhance the diversity and applicability of findings, address varied socioeconomic and cultural contexts and promoting more equitable global health outcomes. 37
The productivity and influence of authors like Sauerborn et al. and De Allegri et al. demonstrate the importance of sustained contributions in shaping the field. Their work has not only enriched the academic discourse but has also informed policy frameworks and implementation strategies for CBHI.32,38 However, the high prevalence of occasional contributors (86.5% of authors producing a single document) indicates a need for more consistent engagement to ensure a robust and cumulative knowledge base. This finding reflects broader trends in health systems research, where intermittent contributions can limit the depth and continuity of inquiry. 39
Collaborative networks also reveal central hubs and isolated clusters, suggesting opportunities to integrate peripheral research groups into the broader discourse. Strengthening these networks could involve fostering mentorship programs, cross-regional partnerships, and multi-institutional projects that bridge gaps between established and emerging researchers. Such efforts would not only enhance research quality but also ensure more equitable representation and capacity building across regions. 40 Moreover, promoting open-access publishing and data sharing within CBHI research can further democratize knowledge dissemination and foster global collaboration. 41
Strengths and limitations
This study’s strengths include its comprehensive scope, drawing on multiple databases and applying established bibliometric methods to map over two decades of WTP for CBHI research. It highlights global patterns, key contributors, and policy-relevant insights that can inform strategies toward universal health coverage. However, the analysis is limited by its focus on English-language, peer-reviewed literature, excluding gray sources and regional journals. The underrepresentation of certain regions (e.g. South America, Oceania) and reliance on a small group of prolific authors may also constrain generalizability. In addition, citation metrics for recent years likely reflect time-lag effects rather than actual research influence.
Future research directions
To sustain this research progress, future efforts should focus on diversifying regional contributions, fostering sustained scholarly engagement, and building inclusive collaboration networks. These strategies are essential for leveraging CBHI as a tool to achieve UHC and address global health inequities.
Practical implications
The findings have direct implications for health policy and program design. Policymakers can leverage insights from high-impact studies in Burkina Faso and Ethiopia to replicate successful models. Understanding collaboration networks also enables international funders to channel support toward regions with research gaps. Moreover, health ministries could apply lessons from this study to design communication strategies that increase community trust and perceived value in CBHI schemes, thereby improving enrollment.
Conclusion
In conclusion, this bibliometric analysis underscores the rapid growth, evolving priorities, and collaborative dynamics in research on WTP for CBHI. This study highlights the field’s growing significance in addressing health financing challenges and promoting healthcare equity. Key findings include Ethiopia’s leadership in publication output, Burkina Faso’s citation dominance, and the field’s dependence on contributions from a small group of highly productive authors and journals. The analysis also reveals strong international collaborations and a thriving body of literature with significant academic impact. However, regional and disciplinary gaps present opportunities for more inclusive and diversified research. Furthermore, recent declines in citation impact and publication frequency emphasize the need for renewed focus on emerging themes such as behavioral economics, technology integration, and the long-term sustainability of CBHI models. This bibliometric synthesis offers a valuable foundation for scholars aiming to explore underrepresented regions and integrate behavioral, technological, and economic models into CBHI research. Practically, the findings can inform donor priorities and national health policies by identifying successful case studies and collaboration models. Our study thus serves both as a roadmap for future academic inquiry and a guide for real-world decision-makers.
Footnotes
Author contributions
Conceptualization and methodology: BWA and THM; Data curation, cleaning, analysis and interpretation: BWA, THM and SZK; Writing – original draft: BWA, THM and SZK; Writing – review & editing: SZK. All the author(s) read and approved the final manuscript for submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data related to this manuscript are available upon request and for researchers who meet the criteria for access to confidential data may contact Mr Berhanemeskel Weldegerima Atsbeha (