
Abstract
Background:
Ethiopia has launched a community-based health insurance (CBHI) since 2011, which is an innovative financing mechanism to enhance domestic resource mobilization and sustainable health financing. This study assessed determinants of CBHI enrollment among HHs (households) of East Wollega, Ethiopia, 2022.
Method and materials:
Community based unmatched 1:2 case-control study design was conducted between Jan 7and Feb 5/2022 among 428 HHs (144 cases and 284 controls). Cases were selected from HHs who registered for CBHI and currently using CBHI. Controls were from those who do not registered for CBHI membership. Data collected using a semi-structured, interview administered questionnaire. Multivariable logistic regression with SPSS version 25 was employed for analysis and variables were declared statistical significant association at p-value < 0.05, 95% CI.
Result:
Data from 428 (144 cases and 284 controls to CBHI) were collected; a response rate of 98.8%. Statistically lower odds of CBHI enrollment was observed among HHs who have poor knowledge [AOR = 0.48 (95% CI:0.27, 0.85)], perceived not respectful care [AOR = 0.44 (95% CI :0.24, 0.81)], unavailability of laboratory services [AOR = 0.37(95% CI:0.21, 0.66)], inappropriate time of premium payment [AOR = 0.31(95% CI:0.18, 0.52)]. In addition, medium wealth status category [AOR = 0.11(95% CI: 0.03, 0.45)]. Higher odd of CBHI enrollment observed among who have formal education [AOR = 2.39(95% CI: 1.28, 4.48)].
Conclusion and recommendation:
Educational level, knowledge, time of membership payment, laboratory test availability, perception of respectful care and wealth status were significant determinants of CBHI enrollment status. Hence, the responsible bodies should discuss and decide with community on the appropriate time of premium payment collection, and enhance community education on CBHI benefit package.
Significance for public health
Benefits people through available prompt medical care, improving their health status, providing better health outcomes, reducing the physical burden for the insured and the demand for free-cost care from the provider by encourage them to be insured. The study will improve household enrollment in CBHI program after factors identified. Regardless of the promising government’s health financing strategy in that the scheme can be expanded and that CBHI can provide an important basis for reducing out-of-pocket payments, researches on the households enrollment in CBHI program and the associated factors are still very limited in Ethiopia in general and Oromia region, East Wollega districts of west Ethiopia in particular. The aim of this study is to assess the determinant of CBHI enrollment at household level in East Wollega Zone. Policy makers and stakeholders will use the finding of the study to modify strategy for implementation of CBHI. Serve as a baseline for further researchers for the study area
Introduction
The out-of-pocket (OOP) spending is the most inequitable way of financing the healthcare that affects the poor worst, lack of risk pooling and insurance could be argued as the main reasons for health-related impoverishment in developing nations. 1 In the majority of Sub-Saharan countries, healthcare cost is mainly paid at the time of sickness and out-of-pocket (OOP) at the point of service delivery, which potentially could inhibit access to universal health coverage (UHC). 2 To achieve UHC, service and population coverage of health services has to be expanded along with financial protection for marginalized communities. 3 Therefore, community-based health insurance (CBHI) was evolved as an alternative health financing mechanism to OOPs in low- and middle-income countries (LMICs), particularly in areas where government or employer-based health insurance is minimal. 1 CBHI is a scheme that requires community members to prepay for health services and a pledge agreement requiring the health insurer to cover basic health service costs in exchange for premium payments into a collective fund which is designed, owned, and administered by members. 4 Community financing for health is a mechanism whereby households in a community finance or co-finance the current and/or capital costs associated with a given set of health services. At the same time, they are expected to gain participation in the management of the community financing scheme and the organization of the health services. 5
Over 800 million people spend at least 10% of their household budget to pay for health care and 100 million people pushed to extreme poverty due to excessive or “catastrophic” healthcare expenditure on their livelihood and suffer from financial shocks each year globally. The total economic cost of illness for households (HHs) estimated to be frequently above 10% of household income. This is potentially catastrophic: as such expenditure levels are likely to force households to cut their consumption of other minimum needs, trigger productive asset sales or high levels of debt, and lead to impoverishment. 6 Over 90% of healthcare financial hardship and their outcome have been occurring in Sub-Saharan African countries, where resources are limited. In fact, however, CBHI frequently unable to achieve its aim, mostly because of inadequate level of household enrollment. 7
No country in the world is able to full providing health cover to citizens effectively due to a lack of spending money for health care services. UHC monitoring report in 2017 showed that many people lack essential health service and people pushed into poverty spending too much budget. It showed that in the entire worlds, more than 7.3 billion people do not receive all the essential health service they need. 2
In Africa, enrollment in the community based health insurance is low; having more than 90% of the targeted population uninsured except Rwanda with an enrollment of over 80% of the population, but their scheme no longer meets the definition of CBHI, as it has been compulsory. 8
Access to health care services in most of developing countries were affected since healthcare cost is mainly paid at the time of sickness and OOP at the point of service delivery. 1 UHC is becoming a priority, there is a need to increase the financial accessibility of health care services, protecting the population from catastrophic expenditure and decreasing the risk of extreme poverty. The way a country finances its health care system is a critical determinant for reaching UHC. This is so because it determines whether the health services that are available are affordable to those that need them. 9
In Ethiopia, CBHI was accepted as one of the strategies to attain UHC, since it recognized to ease resource mobilization to promote health service uptake and provide financial threat protection to insured members like that of most Sub-Saharan countries. 10
Ethiopian Ministry of Health has a vision for sustainable development goal, equitable, sustainable, adaptive and efficient health services. To provide equitable service, the financial issue should be considered; CBHI is one of the strategies set as a policy to solve this problem and one of governmental concern in health care financing systems. 11
The Ethiopian health care system is characterized by high OOP expenditure, increased health care needs, inability to mobilize more resources for health among rural dwellers, and inability to fully recover costs of care incurred by beneficiaries. 12
Thus, strong commitment is required to shift from an OOP model to CBHI to achieve UHC, and increase access to essential health care while spreading the financial consequence of sickness among the residents. 13
CBHI piloted 4 years ago in four regions in Ethiopia, accounting for 85% of the total population. Under the CBHI system, each district or Woreda will have a collective health fund to which participants will contribute. The poor are eligible for membership in community health funds sponsored by the woredas and regions. The infancy stage of CBHI studies in piloted areas revealed that the scheme benefited members by reducing the need to borrow money for medical care, improving outpatient care, seeking ever-increasing enrollment, and a better willingness to pay than other East African countries. Rural households in most developing countries excluded from the formal insurance system. Thus, CBHI is being promoted for its potential to pool risks and resources to reduce HHs OOP expenditure and improve access to health care. 14
In Oromia, regional state, the CBHI coverage is 43.5% in 2020/2021less than the national coverage, which was 50%. Indeed, the CBHI scheme’s members are able to access health care benefits without financial hardship when they actually seek health care services, although in Oromia still majority of vulnerable groups are not yet included in the scheme. 15
Though measures like awareness creation, community mobilization by health sectors have taken to increase the enrollment of HHs, the Zonal report shows that the CBHI coverage of East Wollega Zone is currently very low (18.69%). There was limited study that documented on factors determining CBHI enrollment in Oromia Regional State in general, East Wollega zone in particular. Hence, the aim of this study is to assess determinants of CBHI in East Wollega zone, Oromia Regional State, Ethiopia.
Methods and materials
Study area and period
This study was conducted in East Wollega zone from Jan-07 to Feb 05/2022. It is one of the 21 zones of Oromia regional state west of Ethiopia. The zone currently has 17 woredas’, and has 340 Kebeles” with 338,599 HHs. The zone has currently 327 health posts, 65 public health centers, five public hospitals, and one regional laboratory facility, as reported by the zonal Health Office in the 2021-second quarter report.
Study design
● Community based unmatched 1:2 case-control study conducted.
Population
All HHs reside in East Wollega zone during study period were a source population. Cases were HHs who enrolled to CBHI and currently using the program. Controls were HHs those who didn’t enrolled to CBHI membership. Study unit was all selected HHs who resides in the selected kebeles. HH heads older than 18 years who reside at least for 6 months were included in the study, and HH heads that are unable to communicate during data collection were excluded from the study.
Sample size determination
The sample size was calculated by using Epi info version 7.2.2.6 Stat Calc. The known independent factors from the previous study considered to get maximum sample size for this study. Numerous factors considered to determine sample size for this study. Thus, sex of household head from the study conducted in North Gondar gave the maximum sample size required to conduct this study. Based on the following assumption; by 80% power at 95% CI, ratio of control to cases (r) =2, Odds ratio = 2.79%, P2 = 17.2%. 16 Considering design effect of two and possible non-response rate 10%; sample size of 433 (144 cases and 289 Controls) HHs was included in the study.
Sampling procedure
The study participants were drawn by using multistage sampling. In the first stage, seven districts were selected randomly from 14 districts launched to implement the CBHI before 2021. Then, 60 kebeles selected randomly from seven districts (143 kebeles). The final stage involved selection of HHs from 60 kebeles. List of cases and controls identified from each kebele administrations and utilized for sampling frame. Sample size proportionally allocated for selected kebeles based on each kebeles HHs. Simple random sampling applied to select cases and controls by taking their lists as frame [Figure 1].
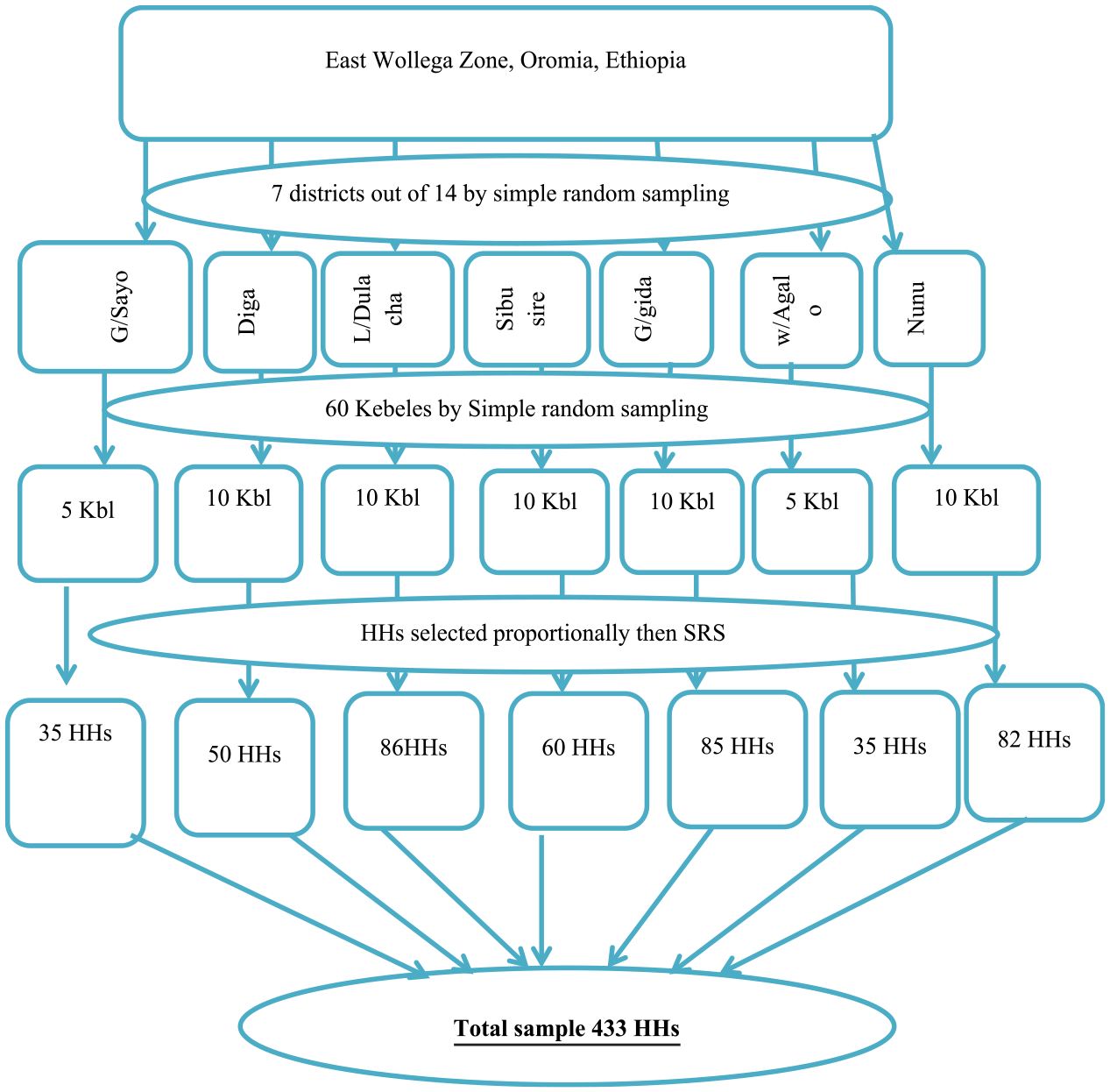
Pictorial presentation of sampling procedure.
Data quality assurance
Data were collected using a semi-structured, interview administered questionnaire, which initially prepared in English and translated into Afaan Oromo, by those proficient in the language, and checked for consistency. Data collectors and supervisors trained intensively for 3 days, focusing for data collectors mainly on how to interview respondents and how to fill the questionnaires on a given instruction. Similarly, for supervisors, how to check reliability and validity of information daily collected. Besides, training which emphasized on the importance of respondents’ verbal consent and right, privacy and confidentiality.
Two nurses per Woreda assigned for data collection. Similarly, three primary health care unit (PHCU) directors were assigned to all woredas as supervisors.
All the data were checked for completeness, accuracy, and consistency by the principal investigator and the supervisors immediately after the data collection. In addition, the principal investigator and supervisors closely monitored the data collection. To check consistence of the questionnaire, a pre-test conducted on 5% of the total sample size outside study area. The purpose of the pre-test was to ensure that the data collectors are familiar to the tools; the respondents are able to understand the questions, wording, and logic and skip order of the questions in a sensible way to the respondents. An amendment was done accordingly after the pre-test.
The validity of questionnaire was kept by using World Health Organization guideline for health insurance implementation, Ethiopian federal ministry of health standard tools for assessment of CRC (compassionate, respectful and caring) implementation, and adopted from published study done in Northern Ethiopia.
Description of variables
Outcome variable
● CBHI enrollment
Independent/explanatory variables
•
•
•
•
Operational definition
Data processing and analysis
For completeness and consistency at the end of data collection period, the principal investigators checked questionnaires completed by respondents. Then coded and entered to SPSS for analysis. Before running statistical analysis, the categorical variables recoded and categorized to fit for analysis using SPSS. Odds ratio at 95% CI used to describe the association between the independent and outcome variables. Descriptive statistics presented using narration and table in the form of frequency and percentage to describe the relevant variables correlated study population. Bivariate logistic regression analysis performed to find a crude association of explanatory variables with the outcome variable at p-value ≤ 0.25 and crude odds’ ratio (COR) with 95% CI. Those explanatory variables demonstrate association by bivariate logistic regression models considered candidate for multivariable model. The multivariate logistic regression models will be calculated at 95% confidence level (AOR with 95% CI) and alpha (α) =5% cut off point (at p-value less 0.05). Those variables found significant at p-value 0.05 level & Adjusted Odds ratio (AOR) with 95% CI considered as independent determinant factors associated with community-based health insurance enrollment status. Principal component analysis was done to analysis to classify wealth status of participants.
Ethical considerations
Before conducting any research work, Ethical clearance was obtained from Institutional Review Board of Nekemte health Science College. Besides, the letter of approval was taken from East Wollega Zonal health department, and it was taken to district health office for final approval. Informed verbal consent was taken from each study participant after briefed on their right and autonomy, study objective and what needed from them. All methods of this research work were carried out in accordance with relevant guidelines and regulations.
Results
Among 433 of the study participants, a total of 428 (case 144 and 284 controls) of HHs in east Wollega zone were involved in study at response rate of 98.8%.
Socio demographic characteristics
Demographic status shows that the mean age (standard deviation) for cases and control were 39.5(SD: +10.5) and 38.4 (SD: +12. 6) years, respectively. Concerning sex of respondents, 108(75%) of cases and 193(68%) of controls were male, headed HHs. The marital status of respondents found as about half, 125(86.8%) of cases and majority 246 (86.6%) of controls were in marriage. Regarding ethnicity, 137 (95.1%) cases and 277 (97%) of controls were Oromo. Seven (4.9%) of cases and two (0.7%) of controls belongs Amhara.
Regarding the job status, 93(64.6%) cases and 189 (66.5%) of controls were farmers. According to literacy status, 66 (45.8%) of cases and 76 (26.8%) of controls attended primary education. According to number member, 80(55.4%) of cases and 151(53.2%) of controls have greater than five family members [Table 1].
Sociodemographic characteristics of study participants in east Wollega zone, 2022.

Wealth status of respondents by principal component analysis (PCA)
According to wealth status of respondents, 72 (50%) of cases and 130(45.8%) of controls were found in fourth quantile (rich)[Figure 2].

Wealth status category of study participants of East Wollega Zone 2022.
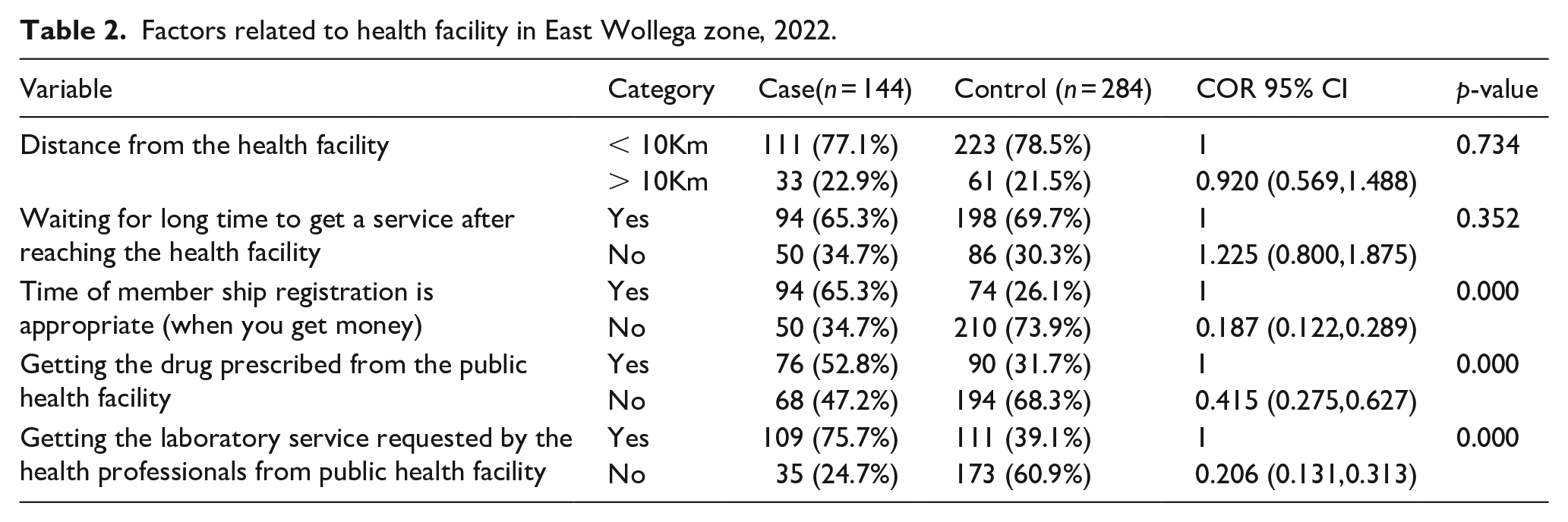
Health facility factors
Ninety-four (65.3%) and 198 (69.7%) of the cases and controls respectively perceive that they wait for a long time to get service from a public health facility. Ninety-four (65.3%) of the cases and 74 (26.1%) controls HHs respectively reported as the time of membership is appropriate [Table 2].
Factors related to health facility in East Wollega zone, 2022.
Knowledge assessing characteristics of respondents
Knowledge of respondents on CBHI assessed based on the following variables. The response of a participant summed up to categorize the participant as having good knowledge or poor knowledge on community-based health insurance [Table 3].
Knowledge assessing items.

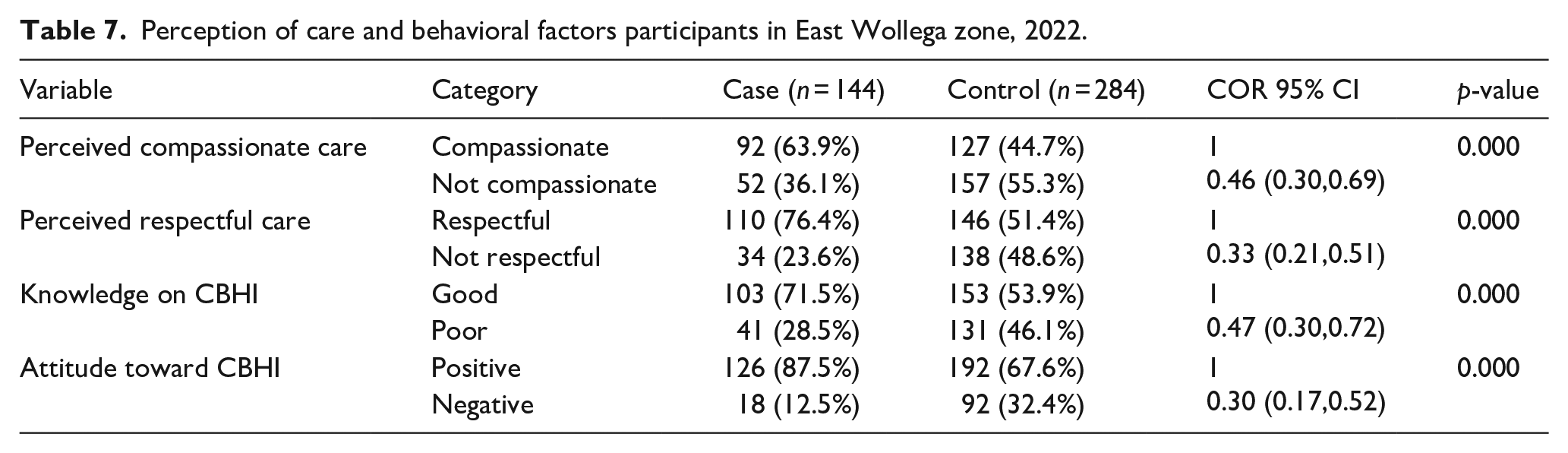
When data computed for assessing knowledge 71.5% of those cases to CBHI and 53.9% of controls have good knowledge on CBHI whereas 28.5% of cases, and 46.1% of controls have poor knowledge on CBHI [Table 7].
Attitude assessing characteristics of respondents
Likert scale of measurement applied to measure the attitude of respondents toward CBHI. Thus, nine item statements regarding CBHI were prepared to measure the attitude of respondents. Strong agreement to express favorable at one extreme of scale and strong disagreement to show unfavorable attitude toward CBHI considered. The score of each respondent was obtained by summing of each item. Accordingly, numerical score indicating the least favorable attitude given one (1) and the most favorable attitude had given five (5) to yield total score that indicate attitude toward the scheme. The scoring system was used with respects to respondents’ responses as follows: strongly agree 5, agree 4, neither agree nor disagree had given 3, disagree 2, and strongly disagree 1. The median score was calculated and those scored above the median and median score categorized as positive attitude and scores below the median meant negative attitude toward CBHI [Table 4].
Attitude assessing items.

Finally, the computed data reveals 126 (87.5%) of cases and 192 (67.6%) of controls have positive (Favorable) attitude toward CBHI. But, 18 (12.5%) of cases and 18 (12.5) have negative attitude on CBHI. Majority of the controls have positive attitude and 92(32.4) of them have negative attitude toward CBHI [Table 7].
Community’s perception toward compassion care
Standard checklist from national compassionate and respectful and care (CRC) training guideline designed to assess how compassion health worker is used. Eight statements were taken to assess how communities feel about the health workforce. Respondents score median and above classified as perceived compassionate and score below the median of compassionate assessment items classified as perceive not compassionate [Table 5].
Service provider’s Compassion assessment items.

According to the data collected on perception, 92 (63.9%) of cases and 127 (44.7%) controls perceive health work force is compassionate. Whereas 52 (36.1%) of cases and 157 (55.3%) of controls perceived health care workforces not compassionate respectively [Table 7].
Items to assess respect of health work force to community
Standard checklist from national CRC training guideline designed to assess how Health worker respect the client used. Ten statements had taken to assess how the communities feel about health workforce. If the respondents score median and above of respectful assessment items/questions categorized as perceived respectful. Not respectful care: If the respondents score below the median of respectful assessment items/questions [Table 6].
Service provider’s Respect assessment items.

The study, indicates110 (76.4%) of cases; and 146(51.4%) controls, perceived work force as respectful. Whereas 34(23.6%) of cases and 138(48.6%) controls perceived health care work forces do not show respect [Table 7].
Perception of care and behavioral factors participants in East Wollega zone, 2022.
Knowledge, attitude, and perception on CRC and quality of health service
On bi-variable analysis; perception of compassion and respect, knowledge and attitude of study participants are selected for multivariable analysis at p-value < 0.25 and 95% CI [Table 7].
Determinants of community based health insurance
Bi-variable analysis
After bi-variable analysis in Binary logistic regression; some variables were selected by being potential candidate for multivariate analysis at 95% CI and p-value < 0.25. High CBHI enrollment status observed in those who asked to enroll in appropriate time for membership registration when they got money than those asked at any time [Table 2]. Educational level and wealth status of the respondents also show association with CBHI enrollment [Table 1]. Among service delivery, related factors, availability of drug prescribed and laboratory service analyzed for being potential candidate for multivariate analysis [Table 2]. From CRC assessment factors, CBHI enrollment status was higher among those who perceive that health care provider were compassionate than not. In addition, those who perceive that health worker shows respect ion to client enrolled in CBHI program than that do not perceive respect ion of health workers [Table 3].
Other factors such as knowledge and attitude of respondents were analyzed for being candidate for CBHI enrollment at 95% CI and p-value < 0.25. In which CBHI enrollment was higher in those who have good knowledge about CBHI than who have poor knowledge. Similarly, those who have good attitude toward CBHI enrolled more when compared with those who have negative attitude about CBHI [Table 3].
Multivariable analysis
After all variables in the study entered to binary logistic regression to identify candidate variable; for multivariate analysis, some variables were selected being potential candidates by p-value < 0.25. These variables are; Wealth status, Level of education, membership registration time, Drug availability, Laboratory service availability, perception of community toward compassion of health care, respect of health service provider, Knowledge on CBHI and attitude of community toward CBHI program.
To control possible confounders all candidate variables were included in multivariate analysis in logistic regression using backward likelihood ratio model (LR); membership registration time, wealth status, level of education, Laboratory service availability, perception of community on respect of health service provider and attitude of community toward CBHI program had statistically significant association with CBHI enrollment (p- value <0.05). p-value and confidence interval were a test used to declare significance association and multicollinearity checked for variance inflation factor [Table 8].
Multivariable analysis of independent factors of CBHI enrollment at East Wollega Zone, Oromia Region, West Ethiopia, 2022.

CI: confidence interval.
Significant.
Discussion
This study revealed that, educational status of HH heads, Wealth index, Knowledge, HH head’s perception of Respectful care, Time of membership premium payment and Unavailability of continuous laboratory service were independent determinant factors for CBHI enrollment in East Wollega Zone.
This study revealed that, having primary education show a positive association with CBHI enrollment. This finding is consistent with the study conducted in Southern Ethiopia, 23 Northwest Ethiopia, 24 Oromia Regional state, 11 and Ghana [32]. The odds of attending primary education are two times more likely in cases than controls. This could be because those who are educated can understand the CBHI scheme principle and benefit.
In this study, knowledge of HH heads is significantly associated with CBHI enrollment. Having poor knowledge on CBHI reduces the probability of enrollment by 52%. This agrees with the studies conducted in North East 21 and North West Ethiopia. 24 This might be for the reason that those individuals with good knowledge could ask details of the package benefit and convinced, and decide enrolled.
Perception of HH heads on respectful care found to be factors significantly associated with enrollment to CBHI scheme. The community members perceive health work force as no respectful care by health work force enroll by 56% less likely than those who perceive as respectful. Similarly, a study conducted in Ghana shows that Perceptions related to providers were among the factors that affect enrollment to health insurance. 16 This could be because the more the community perceives, as health care providers are respectful, the more likely they enroll in CBHI scheme to utilize public health care services.
The study pointed out that CBHI premium collection time was a significant determinant factor of enrollment into CBHI schemes. Household heads who perceived collection time as appropriate were 69% more likely to be enrolled into CBHI compared to those responded as not appropriate. This could be because of the truth that even though they have convinced and have willingness to be enrolled. However, the time and mode of premium collection is not during when the community gets the money. Known that they fill inconvenient, and they could not be the member. This finding is similar with studies conducted in developing countries 7 and southern Ethiopia. 23
Conferring to this study, level of wealth index of household head’s category medium was a significant predictor for CBHI enrollment. It agrees/consistent with studies conducted in North West Ethiopia, 22 South Ethiopia, 23 Kenya 24 and Ghana’s Upper West Region [32]. This is explaining that those who have wealth index (income) medium category might have the potential to pay from out-of-pocket payment for their health care cost and less likely to be enroll to CBHI scheme. On the other hand, the poorest have the worry of covering the health care cost it incurs from their own out of pocket payment when their family member gets sick and, they could be more likely to enroll in CBHI scheme. Those who are unable to pay for the CBHI service showed that the insurer could subsidize in part at least for basic health services for the poor part of the households.
According to this study, unavailability of continuous laboratory tests in health facility was significantly associated with community-based health insurance enrollment status. Availability to laboratory increases CBHI enrollment by 63% more likely. This is similar to the study conducted in South Ethiopia 23 and North West Ethiopia [33]. This linked to; household heads who perceived lack of continuous laboratory tests were hinder from enrollment the community-based health insurance scheme. This is due to the decline in confidence in getting quality health care from the scheme benefit package in the lack of continuous laboratory tests.
Limitation of the study
• This research is not free of limitations: -recall bias, since some of the data were collected through interviewing the respondents.
Conclusion
The study pinpointed determinant factors of CBHI enrollment. Educational level, Knowledge, Time of membership payment, Laboratory test availability, Perception of Respectful care and Wealth status were significant determinants of CBHI enrollment status.
Recommendation
• Amend time of membership premium payment, by involving the community to decide the appropriate time for premium payment (membership time).
• Conduct further study on premium renewal status of the community.
• Conduct further study on the respectful care status of the health care work force to gain further evidence and appreciate the perception of the community on respectful care characteristics.
• Further, work to increase the knowledge of the community on CBHI benefit package in a tailored way using different channels of communication.
• Supervise and monitor laboratory services in the health facilities, since unavailability of continuous laboratory tests was among the determinant factors for CBHI enrollment.
• Pay special attention for those with low educational status to enhance their participation in CBHI enrollment.
• Supervise and monitor laboratory services supply in the health facilities and fill the gaps continuously.
• Decide on premium collection time as conducive to the specific woredas.
• Assess the respectful care provision of health workforces periodically.
• Facilitate means to enhance knowledge of the community on CBHI benefit package
• Involve the community to decide the convenient premium payment collection time based on their specific tangible income variability.
• Improve the level of knowledge of the community on CBHI benefit package, through periodic and planned community conversation.
• Assess the health work force respectful care provision whether it attracts the community toward CBHI enrollment.
• Prepare and provide information on CBHI enrollment, particularly focusing on uneducated household heads based on their level of understanding.
• Work with other stakeholders (agricultural, education, Business sectors and others) collaboratively to increase wealth of the community.
• Assess and avail the basic laboratory services continuously, and request to fill the potential gaps timely.
• Conduct community conversation to fix appropriate time for premium payment collection.
• Provide tailored education for the community on CBHI benefit package.
• Validate the respectful care provision of health care work force and act on it accordingly.
Footnotes
Acknowledgements
Our deep gratitude goes to Nekemte Health Science College for funding this research. We would like to extend our heartfelt appreciation to data collectors and supervisors for their contribution in this research. At last, but not the least, we are delightful to extend our appreciation to East Wollega Health Insurance Agency, East Wollega Zonal and woredas health offices for providing us valuable information throughout the research process.
Authors’ contributions
Authors’ information
Availability of data and materials
The finding of this study was generated from the data collected and analyzed based on stated methods and materials. The original data supporting this finding are available from the corresponding author on reasonable request.
Consent for publication
“Not applicable.”
Ethics approval and consent to participate
Initially, ethical clearance obtained from the Institutional Review Board of Nekemte health science college, and then letter of approval was taken from East Wollega Zonal health department. This approved letter taken to the district health office for final approval. After approval, it handed to the data collectors and used throughout their visit to all selected sites for data collection. Each study participants briefed on their right and autonomy, study objective and what needed from them. To whom show permission, verbal consent granted and included in participants of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Nekemte Health Science College.