
Abstract
Background:
Onchocerciasis is prevalent near riverine environments, where black flies breed in large quantity. The study assessed the knowledge, attitudes, and preventive practices (KAP) towards onchocerciasis among residents of Ogun Waterside Local Government Area (OGWLGA), Nigeria.
Methods:
A cross-sectional study was conducted among 267 respondents aged between 18 and 60 years in OGWLGA using a purposive sampling technique. A semi-structured pre-tested questionnaire comprising information on socio-demographic characteristics, KAP towards onchocerciasis was used. Questions on KAP were scored: 0 for incorrect and 1 for correct answers and computed into overall scores. The mean score of the population studied were used as the cut-off point for each segment. Knowledge Scores ≥21 was good knowledge, Attitude scores ≥6 was positive attitude, and practice scores ≥4 was good practice. Data was analyzed with SPSS version 24 using descriptive statistics and inferential statistics with p set at <0.05.
Results:
The mean age of respondents was 42.1 ± 11.2 years. Over half (56.9%) of the respondents had good knowledge of onchocerciasis, but less than half had a positive attitude 111 (41.6%) and good practice 119 (44.6%) towards onchocerciasis prevention. Participants with good knowledge were more likely to have a positive attitude (aOR = 13.08, 95%CI: 6.47–26.42, p ≤ 0.001) and 14 good prevention practices (aOR = 14.66, 95%CI = 6.49–33.12, p ≤ 0.001) when compared to those with poor knowledge.
Conclusion:
Health education efforts should emphasize the need to translate good knowledge into positive attitudes and prevention practices that can lead to onchocerciasis elimination in the communities
Introduction
One of the neglected tropical diseases (NTDs) of public health concern in Nigeria is onchocerciasis, an infection that affects humans and is brought on by the filarial parasite Onchocerca volvulus. 1 Black flies, which reproduce in swiftly moving streams and rivers, are one of the simulium vector species that repeatedly bite people to spread the disease. 2 Since the blackfly that spreads the virus thrives and breeds in swift-moving streams and rivers, the condition is frequently referred to as ‘river blindness’. 2 Blindness and severe skin manifestations are the commonest symptoms of the disease. 1 The disease also often comes with severe itching, skin diseases, and disfiguration, which frequently leads to stigmatization. 2 According to estimates, onchocerciasis is the second most common infectious cause of blindness, right after trachoma. 3 About 125 million people worldwide are estimated to be at risk of onchocerciasis and Africa has the greatest burden of the disease with about 96% among all the continents of the world. 4 Nigeria alone has about 50 million people in over 40,000 at-risk communities. As with the other NTDs, onchocerciasis is common in places characterized by poverty and inadequate access to improved water, sanitation, and hygiene. In most rural parts of Nigeria, this is an increase in the risk of onchocerciasis transmission where people rely on contaminated rivers and streams for bathing, washing, and drinking, and are devoid of appropriate waste management systems.5,6 Furthermore, poor faecal management in most of these rural areas also creates an ideal breeding ground for blackflies in slow-moving or stagnant water bodies and soil, providing a nutrient-rich environment for the blackfly larvae to develop.7,8 Additionally, heavy metals and other pollutants can indirectly create or modify blackfly breeding sites by altering the flow and quality of water and changing the physicochemical characteristics of soil. 9 Up to 60% of blindness in Africa occurs as a result of onchocerciasis, which also has an impact on socioeconomic development 10 of the people in many significant ways, including abandonment of farmlands, which leads to food insecurity, reduced school attendance because sometimes, children have to stop school to support their blind parents. In Nigeria and parts of sub-Saharan countries, an upsurge in inter-communal conflicts and insurgency in recent years has contributed to the spread of Onchocerciasis through the displacement of people from their homes, leading to the introduction of the disease to new areas. 11
The onchocerciasis control program (OCP) has employed vector control as its primary strategy in West Africa since 1974. Its main objective is to stop the spread of Onchocerca volvulus by regularly spraying all simulium larval breeding sites with aerial herbicides, and to maintain this for at least 14 years until the infection has completely disappeared from human populations. 4 This strategy has been combined with annual mass drug administration of Invermectin. 4 The two strategies together have been very effective in onchocerciasis control and have made it possible to eliminate the disease in seven OCP countries and this justified the closing down of the OCP in 2002. The only chemotherapy drug that is currently advised for the treatment of onchocerciasis is ivermectin. 5 There is some progress with the control of the disease because of the over two decades of intervention majorly through the annual mass administration of Merck-donated Ivermectin (MectizanR) for treatment in onchocerciasis endemic communities. A series of mapping was conducted between 1990 and 1995 and onchocerciasis was found to be prevalent in most states of Nigeria except Rivers, Bayelsa, Katsina and Lagos. 1 The year 2020 was set to achieve interruption of human onchocerciasis and its ultimate elimination by year 2025. 1
Furthermore, the presence of large river bodies in Efire, Ibiade, and Abigi in Ogun waterside LGA of Ogun State provides breeding sites for black flies and thus makes these communities endemic with onchocerciasis. The socio-economic implications of onchocerciasis are enormous for the study communities whose mainstay are farming and fishing. Decreased visual acuity and irreversible blindness arising from onchocerciasis could lead to decreased mobility and eventually, loss of means of livelihood leading to a dearth of farmers which may in turn lead to food insecurity in the communities. 12 Decreased mobility also suggests that the visually impaired have to depend on other people to move around thereby decreasing the labour force and increasing the number of dependants leading to a cycle of poverty in the affected communities. 13 The disease’s effects on vision can also affect the intensity of the lights. Visual impairment, light sensitivity, and discomfort under bright lighting are possible symptoms of severe onchocerciasis. 14 Furthermore, the disfiguring skin conditions also lead to increased stigmatization in schools, workplaces, and in social gatherings. 13
Although, some studies have indicated that the management of onchocerciasis in numerous endemic populations has been impacted by a lack of knowledge regarding the disease’s etiology and route of transmission.2,3 This dearth of knowledge affects people’s attitudes towards the disease and definitely, efforts geared at preventing and controlling the disease. Moreover, for optimum community participation and effective control, all stakeholders, including health workers, researchers, and policymakers, need to be aware of the community’s knowledge, beliefs, and behaviors towards the disease. Despite being prevalent, onchocerciasis has never been the subject of any further research or evidence in the current study areas. This study therefore evaluated the knowledge, attitude, and preventive practices of residents of three communities in Ogun waterside towards onchocerciasis.
Methodology
Study design
A community-based cross-sectional design was conducted from May 2023 to June 2023 in selected communities in Ogun Waterside Local Government Area (LGA) to assess the knowledge, attitude, and practice of the local residents toward onchocerciasis.
Study settings and study population
Out of the 20 LGAs in Ogun State, Ogun Waterside LGA is situated in Ijebu ode. It is the only part of the state that borders Lagos Lagoon and has a shoreline on the Bight of Benin. The Local Government Area has ten political wards, and its administrative center is located at 6°29′N4°24′E in the town of Abigi. 15 Approximately 103,200 people live in the LGA. The aquatic environment of the LGA, which includes marshes, vast bodies of water including creeks, rivers, and lagoons, as well as forests, has shaped it significantly. 16 Three wards: Ward 2-Ibiade, Ward 5-Abigi, and Ward 9-Efire, were specifically selected for the study based on guidance from health officials in Ogun state because they have been previously classified as endemic for onchocerciasis. The bulk of the population is employed in trade, agriculture, and fishing, although a sizeable fraction also works as artisans in industries like carpentry, clothing manufacturing, and hair styling. Males and females between the ages of 18 and 60 who had lived in the study communities for at least a year and provided their consent to participate in the study were the inclusion criteria for the research.
Variables
Outcome: knowledge, attitude, and preventive practice
Exposure: age, gender, education, occupation
Predictors: age, occupation, good knowledge, positive attitude
Potential confounders: age
Sample size determination and sampling technique
The sample size was obtained using the Cochran formula, widely used for cross-sectional studies:
Data collection instrument and data collection
Data were gathered using a pretested semi-structured questionnaire and a checklist designed by the authors after reviewing related studies.2,19,20 The questionnaire covered socio-demographic details; knowledge of onchocerciasis, including causes, symptoms, modes of transmission, prevention, and management, and knowledge of MAMs activities; respondents’ attitudes and preventive practices regarding onchocerciasis; and, self-report on the disease. All tools were translated from English into Yoruba, the indigenous tongue. Three research assistants trained in the use of the Kobo Collect app on Android devices collected the data.
Participants’ responses were scored ‘1’ for correct or ‘0’ for incorrect answers, after which all items were summed into a composite score. The knowledge part contained thirty-five (35) items including causes of onchocerciasis, mode of transmission, prevention, and knowledge of the mass administration of medicines (MAMs) program. The mean knowledge score for the population, ‘21’ was used as the cut-off point.21,22 Respondents with less than 21 were categorized as having poor knowledge of onchocerciasis, whilst those with ≥21 were categorized as having good knowledge of the disease. The attitude section comprised 10 items relating to respondents’ feelings if a family member became sick from onchocerciasis, perception of being at risk of onchocerciasis, the place to seek treatment if ever sick from onchocerciasis. The mean attitude score for the population surveyed ‘6’ was used as the cutoff point. Respondents who scored <6 were classified as having negative attitudes and those with ≥6 were categorized as having positive attitudes towards onchocerciasis.
The practice section comprised six-items relating to actions taken by respondents to prevent onchocerciasis and taking medicine during MAMs. The mean practice score for the population studied ‘4’ was used as the cutoff point. Participants with <4 were classified as having poor onchocerciasis prevention practice while those with ≥4 were classified as having good practice towards onchocerciasis prevention.
Validity and reliability of the instrument
Face validity and content validity served as the foundation for the study’s validity. The study supervisor and subject matter experts thoroughly reviewed the questionnaire’s scope, content, and application to the subject matter.
The methodology of test-retest was utilized to evaluate reliability. Thirty respondents, that is, approximately 10% of the sample size as recommended by other studies23,24 were given the questionnaires in another Onchocerciasis endemic community - Imushin in Ijebu East LGA in Ogun State, Nigeria. Pre-testing was used to assess the questionnaire’s consistency. The following minor changes were made to the questionnaires: three knowledge items, two attitude items, and two preventive practice items were all amended. Semantic changes were the only ones performed. A fresh test was administered using the updated questions. The reliability value of the pre-test was 0.84, indicating the validity of the survey tool.
Data management and statistical analysis
After data collection, data was exported from Kobo collect into Statistical product and service solution version 24 (SPSS, Inc.; USA), cleaned and analyzed. Frequency tables, percentages, charts, and descriptive statistics (mean and standard deviation) were used to report the results. Inferential statistics such as chi-square, bivariate and multivariate regression models were carried out. Bivariate analysis was used to further identify particular subgroups of the independent variables that were associated with the dependent variables. Multivariate analysis was then used to examine the relationship between multiple independent variables and the dependent variables and to also identify and adjust for confounding variables. Statistical significance was placed at one-tailed, with a p-value <0.05 for all inferential analyses
Ethical consideration
The Helsinki Declaration of 1975, as amended in 2000, and the established requirements of the relevant Research Ethics Committee on human research were adhered to in this study. The Ogun State Ministry of Health’s Health Research Ethics Committee provided ethical clearance with the registration number HPRS/381/390. Permission was obtained from the local government authority. Written consent was obtained from all the study participants after the study was explained to them. All information relating to the research and all study materials were kept confidential.
The reporting of this study conforms to the STROBE statement 25 (Supplemental File).
Results
Socio-demographic characteristics of respondents
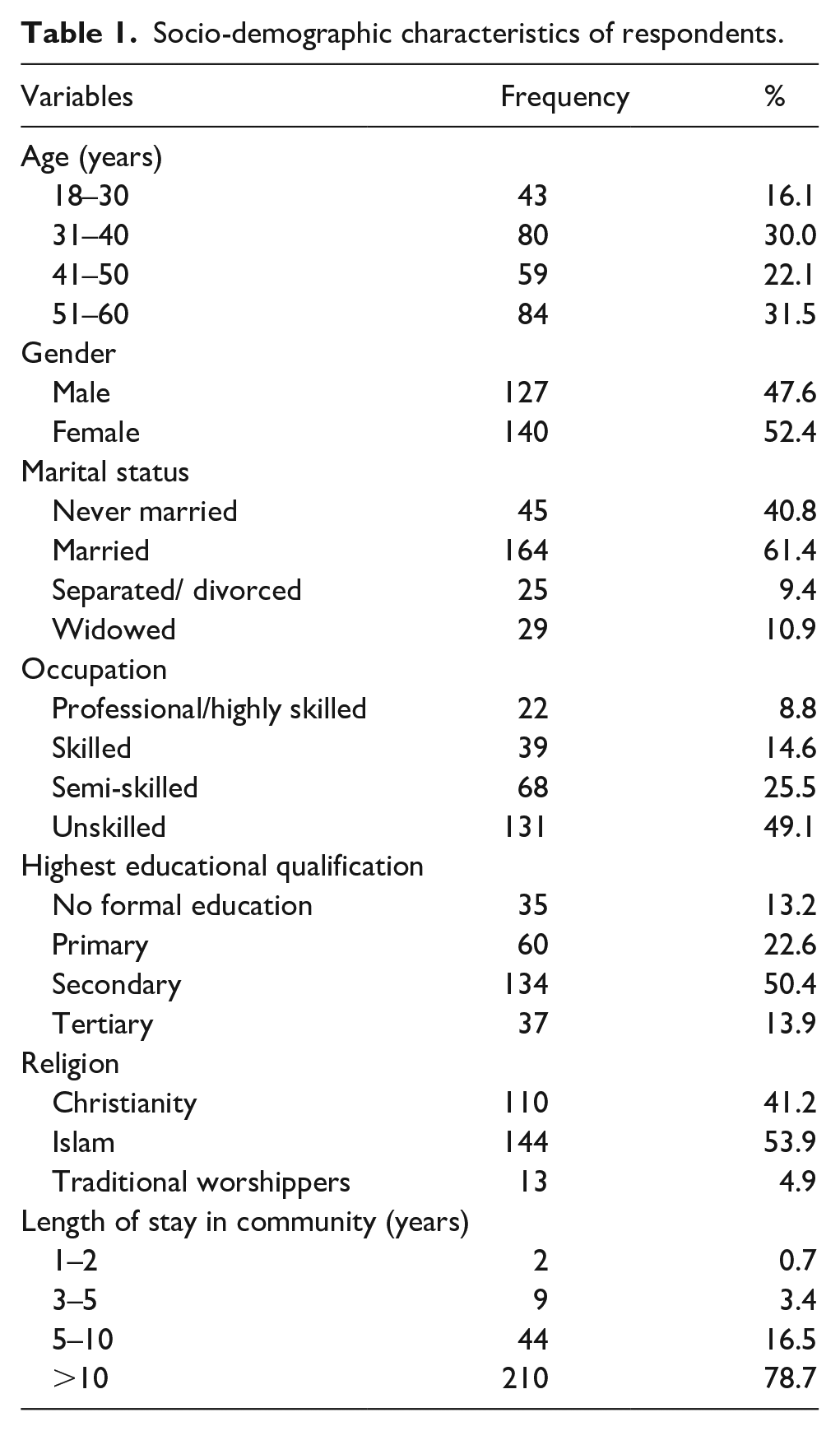
Table 1 shows the socio-demographic characteristics of respondents. Two hundred and eighty
Socio-demographic characteristics of respondents.
Knowledge of onchocerciasis among respondents
A total of 267 respondents participated in the study with the majority 176 (65.9%) respondents reporting that they had heard about the disease. However, knowledge concerning the causes of Onchocerciasis was limited. Only 9 respondents (3.4%) correctly identified filarial worms as the causative agent, while 194 (72.7%) attributed it to black fly bites, which is a near accurate association though. Misconceptions were evident, with 57 (21.3%) attributing the cause to poor personal hygiene and 8 (3.0%) to mosquito bites. In terms of transmission, 172 respondents (64.4%) incorrectly believed that a single bite from a black fly could cause the disease, whereas only 48 (18.0%) correctly indicated that repeated bites are necessary for transmission. Misunderstandings about other modes of transmission were also reported: 82 (30.7%) believed it could be transmitted through contact with infected persons, 15 (5.6%) cited mosquito bites, and 30 (11.2%) mentioned sharing clothes. Very few respondents (7; 2.6%) thought sexual contact could be a route of transmission (Table 2a).
Respondents’ knowledge of onchocerciasis.
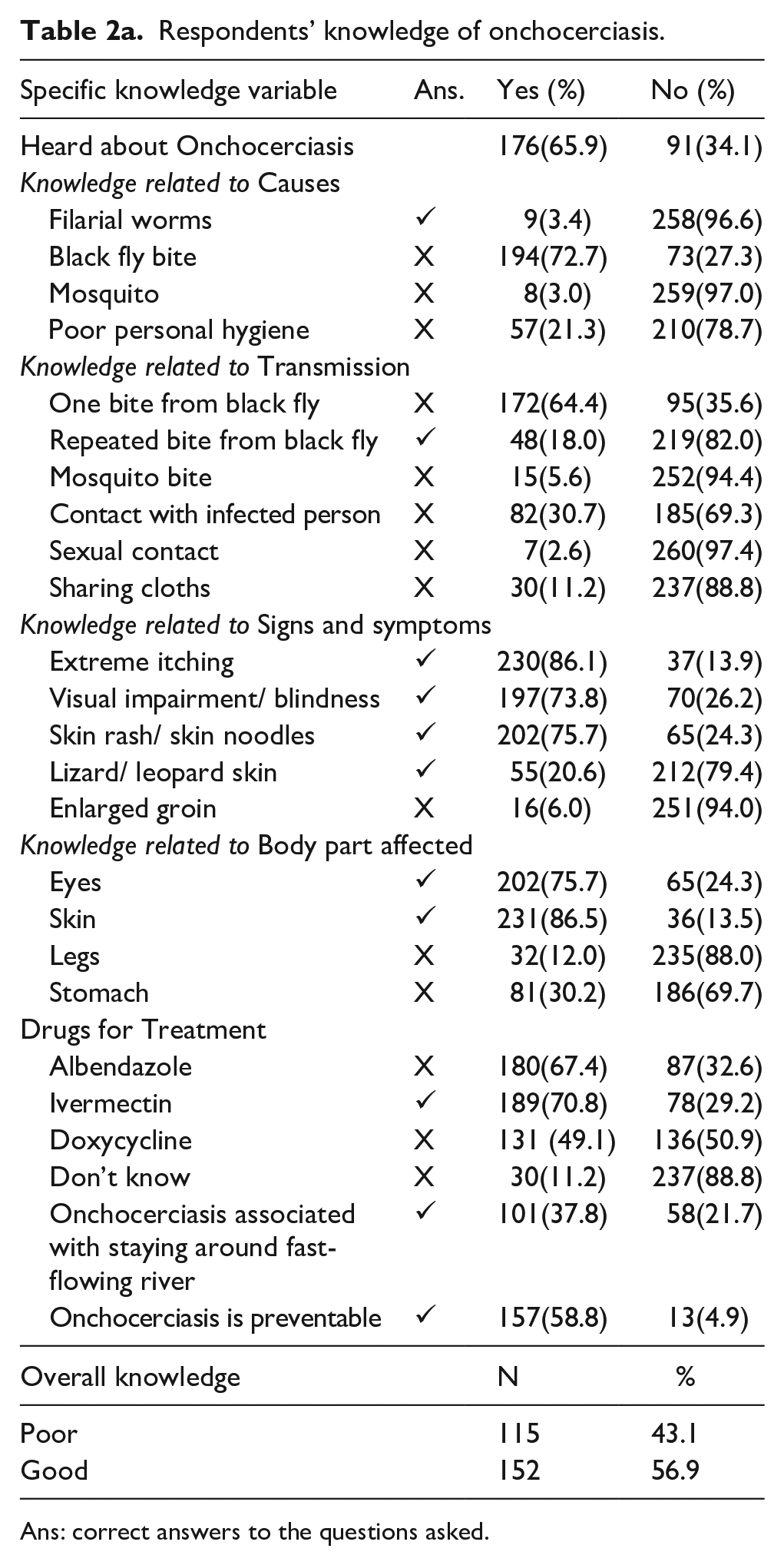
Ans: correct answers to the questions asked.
Knowledge of the clinical manifestations was relatively better. The most commonly recognized symptoms included extreme itching 230 (86.1%), visual impairment or blindness 197 (73.8%), and skin rash or nodules 202 (75.7%). Fewer respondents identified lizard/leopard skin (55; 20.6%) or enlarged groin 16 (6.0%) as signs of the disease. The majority of respondents were aware that the skin 231 (86.5%) and eyes 202 (75.7%) are commonly affected body parts. However, some respondents incorrectly believed that the stomach (81; 30.2%) and legs (32; 12.0%) are affected. In terms of treatment, 189 respondents (70.8%) correctly identified Ivermectin as a drug used for Onchocerciasis management. However, 180 (67.4%) and 131 (49.1%) incorrectly cited Albendazole and Doxycycline, respectively, as treatment options. A total of 30 respondents (11.2%) reported not knowing any drug used in the treatment of the disease. Only 101 respondents (37.8%) associated onchocerciasis with living near fast-flowing rivers, a key environmental risk factor. On a positive note, 157 respondents (58.8%) acknowledged that the disease is preventable (Table 2a). Overall, based on composite knowledge scoring, 152 respondents (56.9%) demonstrated good knowledge of onchocerciasis, while 115 (43.1%) had poor knowledge (Figure 1).

Level of good knowledge, good attitude and good practice of study population about onchocerciasis. Each percentage represented fraction of total respondents who have scored above the mean score within each category of the three outcomes.
Concerning MAMs for onchocerciasis in the study community (Table 2b), the majority of the study respondents 180 (67.4%) did not take medicine in the last round, majority (71.6%) did not know the number of times the medicine is given per year nor when MAMs was last carried out 197 (73.8%), 49 (18.4%) reported MAMs for onchocerciasis occurred more than 10 years prior to the study while less than 10% reported MAM activities occurred within the past 10 years before the survey (Table 2b).
Respondents knowledge of MAMs Activities in their Community.

Respondents’ attitude towards onchocerciasis
Over half, 158 (59.2%) think onchocerciasis is a serious disease in their community, and almost two-thirds, 172 (64.4%), of the respondents think that the disease should be treated. Concerning level of perceived risk, the majority 225 (84.3%) think they had a low or no risk of contracting onchocerciasis, 1 out of every 7 consider their risk of onchocerciasis moderate 37 (13.9%) and only 1 out of every 50 of the study participants consider themselves as having a high risk of the disease 5 (1.9%) (Table 3). Overall, less than half (41.6%) of the respondents had a good attitude towards onchocerciasis prevention, while 58.4% had a poor attitude (Figure 1)
Respondents attitude towards onchocerciasis.

Ans: correct answers to the questions asked.
Respondents’ self-report on onchocerciasis and practice towards onchocerciasis prevention
Almost one-third (31.5%) of the respondents had a household member sick from onchocerciasis in the past year, and one-third (33.7%) had also personally experienced symptoms of onchocerciasis. Symptoms reported were subcutaneous nodules in their face, back, or shoulder 84 (31.5%), itchy skin 92 (34.5%), while 91 (34.1%) had eye problems caused by black fly bites (Figure 2). For treatment, a greater percentage, 60 (71.4%) obtained treatment from health facilities but over one-quarter 24 (28.6%) also visited traditional homes. To prevent onchocerciasis, the majority of the respondents kept a clean environment 226 (84.6%), 182 (68.2%) wore protective clothes, and more than half 156 (58.4%) reported using bed nets. One out of every seven respondents did not do anything to prevent the disease. Only about a third of the study participants 87 (32.9%) received medicine for onchocerciasis in the last MAMs round; 72 (27%) did not know about the MAMs program for onchocerciasis in their community (Table 4). Overall, over half of the population surveyed 148 (55.4%) had poor practice towards the disease (Figure 1).

Respondents’ self-report on onchocerciasis symptoms they had experienced in the past 1 year.
Respondents’ self-report and practice towards preventing onchocerciasis.

Ans: correct answers to the questions asked.
Factors associated with good onchocerciasis knowledge
Knowledge of onchocerciasis appeared to increase with increasing age which remained significant after adjusting for gender, education and occupation. Respondents aged 31–40 years were three times more likely (aOR = 3.02, 95% CI: 1.26–7.22, sig = 0.013) to have good knowledge, those aged 41–50 years were about five times more likely (aOR = 4.47 95% CI: 1.75–11.41, p = 0.001) to have good knowledge and those above 50 years old were about six times more likely (aOR= 6.33, 95% CI: 2.50–16.06, p < 0.001) to have good knowledge of onchocerciasis when compared to those between the ages of 18–30 years old. Similarly, occupation was also found to be significantly associated with good onchocerciasis knowledge even after adjusting for age, gender, and education. Those in semi-skilled occupations (group included farmers) were about twice more likely (aOR: 1.59, 95% CI: 1.91–3.56, sig = 0.042) to have good knowledge than those in unskilled occupations but the respondents working in professional/highly skilled and skilled occupations did not show any significant difference in their knowledge of onchocerciasis when compared to those in unskilled occupations. Respondents’ gender, educational level, and length of stay in the community were not found to be significantly associated with their knowledge of onchocerciasis (Table 5).
Factors associated with good onchocerciasis knowledge.

denotes significance at p < 0.05, 1 represents the reference category, − represents analysis not carried out.
Factors associated with positive attitude towards onchocerciasis
Respondents’ attitude towards onchocerciasis appeared to significantly decrease with age (sig: 0.018, COR: 0.94, 95%CI: 0.32–2.78) but this became insignificant after adjusting for gender, education and occupation (sig: 0.69, aOR: 0.81, 95%CI: 0.29–2.25). Similarly, respondents in semi-skilled occupation showed a higher odds of a positive attitude towards onchocerciasis sig: <0.001, COR: 3.23, 95%CI: 1.80–5.92) but this became insignificant after adjusting for age, gender and occupation (sig: 0.69, aOR: 1.53, 95%CI: 0.19–11.78). However, respondents with good onchocerciasis knowledge had a significantly higher odds of a positive attitude towards onchocerciasis (sig: <0.001, COR: 12.72, 95%CI: 6.64–24.36) and this remained significant after adjusting for age, gender, education and occupation (sig: <0.001, aOR: 13.08, 95%CI: 6.47–26.42) (Table 6).
Factors associated with positive attitude towards onchocerciasis.

denotes significance at p < 0.05, 1 represents the reference category; —represents analysis not carried out.
Factors associated with good onchocerciasis prevention practices
Respondents’ practices towards preventing onchocerciasis appeared to increase with increasing age, but after, adjusting for age, education, and occupation, only respondents between the ages of 41–50 years had a three times higher odds of good onchocerciasis prevention practices (sig: 0.042, aOR: 2.99, 95%CI: 1.19–10.12). Respondents’ education and occupation were also significantly associated with good prevention practices but after adjusting for age, gender, education and occupation, only respondents in semi-skilled occupation were five times more likely to have good onchocerciasis prevention practices (sig: 0.041, aOR: 5.23, 95% CI: 1.14–31.16) compared to those in unskilled occupations. Similarly respondents with good knowledge (sig: 0.001, COR: 23.69, 95% CI: 12.11–46.35) and positive attitude (sig: <0,001, COR: 7.9, 95% CI: 4.41–14.16) had higher odds of good onchocerciasis practice which remained significant after adjusting for age, gender, education and occupation: good knowledge (sig: <0.001, aOR: 14.66, 95% CI: 6.49–33.12) and positive attitude (sig: <0,001, aOR: 8.84, 95% CI: 3.37–23.15) (Table 7)
Factors associated with good onchocerciasis prevention practices.
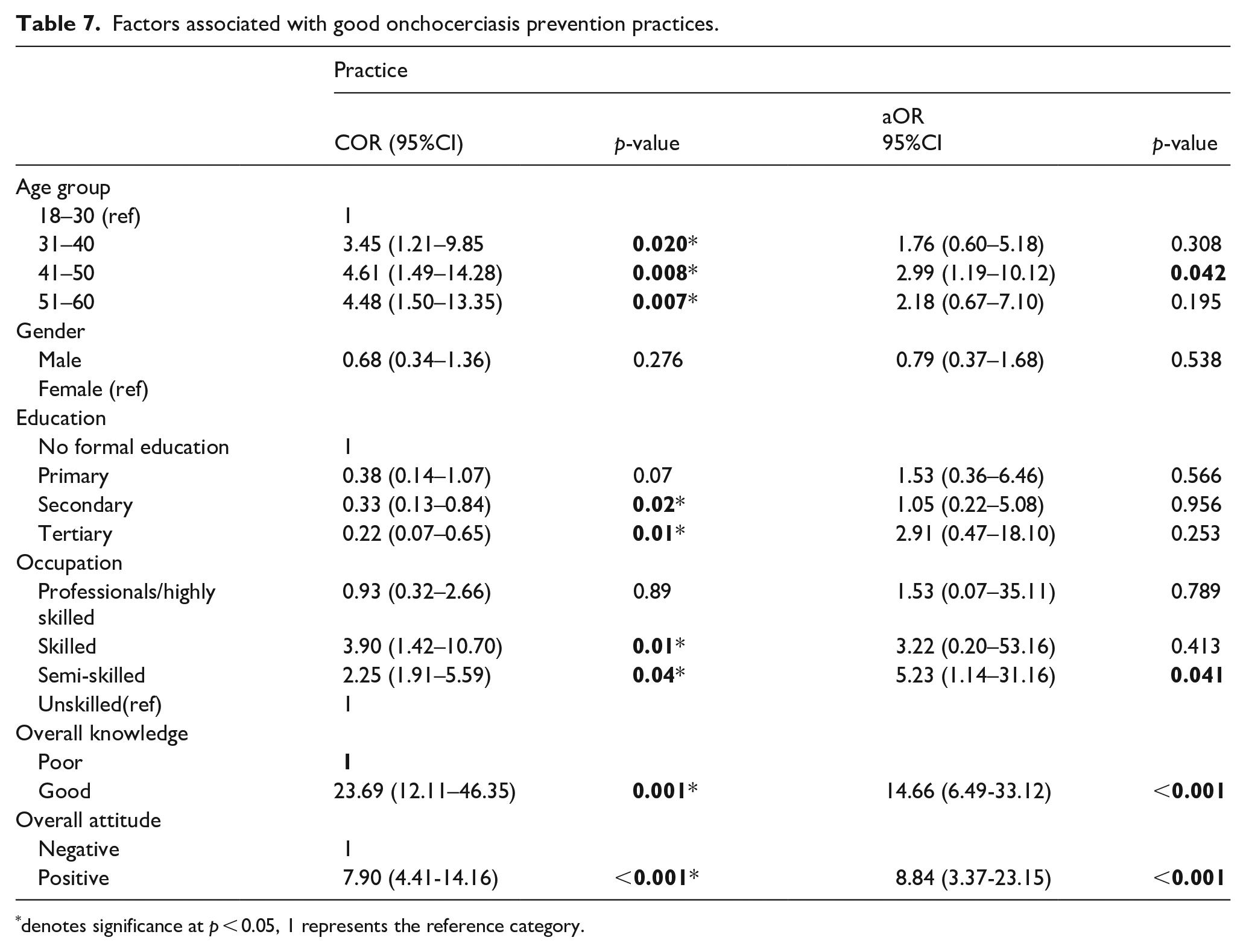
denotes significance at p < 0.05, 1 represents the reference category.
Factors associated with medicine use during MAMs among respondents’
In the bivariate analysis, age group, occupation, knowledge, and attitude were significantly associated with medicine use during MAMs. Respondents aged 31–60 years had significantly higher odds compared to the 18–30-year reference group (COR range: 3.46–5.43; p < 0.05). Similarly, professionals and semi-skilled workers were more likely to exhibit the outcome than unskilled workers (COR = 3.98 and 3.12, respectively; p < 0.01). Those with good knowledge of onchocerciasis were nearly eleven times more likely to use medicine during MAMs (COR = 10.78; 95% CI: 5.24–22.20; p < 0.001), while respondents with a positive attitude were 25 times more likely (COR = 25.00; 95% CI: 12.29–50.87; p < 0.001) (Table 8).
Factors associated with medicine use among respondents.

denotes significance at p < 0.05, 1 represents the reference group in each category.
However, in the multivariate model, after adjusting for potential confounders, only good knowledge and positive attitude remained statistically significant. Respondents with good knowledge had 3.83 times higher odds of the outcome (aOR = 3.83; 95% CI: 1.44–10.12; p = 0.007), while those with a positive attitude had markedly higher odds (aOR = 34.78; 95% CI: 12.45–97.19; p < 0.001). Other variables such as age, gender, education, and occupation lost statistical significance in the adjusted analysis (Table 8).
Discussion of findings
The majority of the study participants had heard about Onchocerciasis and this is similar to the result from studies in south west, 26 and north-west Ethiopia, 27 Osun State, Southwestern, Nigeria 17 and Niger State, in northern Nigeria, 2 where onchocerciasis was widely known in the communities studied. This is mostly because the communities chosen for the study are endemic communities. Concerning the knowledge of causes, only a minimal few knew (9.4%) about filarial worms while the majority (72.7%) erroneously mentioned the disease vector, black flies’ bite. This is also similar to the findings in the Ethiopian studies, where only a few attributed the cause of onchocerciasis to filarial worms (11.2%) and more than half (58.1%) mentioned black fly as the cause of the disease 27 . This result is, however in contrast to a study report in Alabetama, Osun State, Nigeria where the majority of the respondents believed onchocerciasis is caused by mosquito bites. 28 For factors associated with good onchocerciaisis knowledge, age and occupation were significant independent predictors, while gender and educational attainment were not. A consistent and significant association was observed between increasing age and better onchocerciasis knowledge. Participants aged 31–60 years were significantly more likely to have good knowledge compared to those aged 18–30 years, even after adjusting for other factors. Specifically, those aged 51–60 years had over six times higher odds of good knowledge (aOR = 6.33; p < 0.001). This suggests that older individuals may accumulate health knowledge over time due to greater life experience, increased exposure to health information, or heightened awareness of personal health risks. These findings align with prior research indicating that age correlates with improved knowledge and health-seeking behavior, particularly in populations that have lived through health crises or received repeated exposure to health messages. 29 In addition, occupational status also emerged as a significant determinant with semi-skilled workers more likely to have good knowledge compared to unskilled workers (aOR = 1.59; p = 0.042). This may be attributed to continued exposure to the disease and its vector in their work environments. Prior studies have suggested that exposure to such information in the workplace can enhance health awareness and improve knowledge.30–32 Contrary to expectations, education level was not significantly associated with good knowledge after adjusting for confounders. While education is traditionally linked to improved health outcomes, this study suggests that formal education alone may not directly translate into better health knowledge. The results support the growing recognition that functional health literacy—the ability to obtain, understand, and apply health information—may be more critical than educational credentials in influencing health knowledge. 33 This indicates a need for targeted communication strategies that simplify and contextualize health messages for broader reach. Similarly, gender did not significantly influence knowledge levels, a finding consistent with studies that emphasize the role of access, cultural norms, and message framing over biological sex in shaping knowledge and behavior. 34
Concerning respondents’ attitude towards onchocerciasis, more than half (59.2%) think the disease is a serious disease in their community, but this is in contrast to a study in Guatemala 11 where onchocerciasis is not perceived as a serious disease. The majority think the disease needs treatment (64.4%). However, most of the respondents (84.3%) perceived their risk of contracting the disease as low. Overall, more than half of the respondents had poor attitude (58.4%). This result is similar to studies in Ethiopia35,36 where more respondents had poor attitude towards onchocerciasis but in contrast to results from Niger state, 2 Nigeria where the majority had good attitude towards onchocerciasis. The results also showed that good knowledge of onchocerciasis was the most significant independent factor associated with a positive attitude. Participants with good knowledge were more than 13 times more likely to exhibit a positive attitude towards the disease, even after adjusting for potential confounders. This finding aligns with the Knowledge–Attitude–Practice (KAP) model, which emphasizes that improved knowledge is a critical precursor to attitudinal and behavioral change. 34 The initial unadjusted associations between older age groups (41–50 and 51–60 years) and positive attitude suggest that age may influence health perceptions, potentially due to increased health consciousness and risk awareness with age. However, these associations lost statistical significance after adjustment, indicating that age may not independently predict attitude when knowledge and other variables are considered. This supports the notion that the observed age effect is likely mediated by increased exposure to health information and life experiences rather than age itself. 29 Furthermore, occupation, particularly among semi-skilled workers, was associated with a positive attitude in the unadjusted model. However, the effect did not persist after adjustment, suggesting that the occupational influence on attitude may be indirectly mediated through access to information while on the job or experience.
Contrary to expectations, educational attainment did not emerge as an independent predictor of respondents’ attitude towards onchocerciasis. Although a trend toward improved attitude was observed with higher educational levels in the crude analysis, this relationship was no longer significant after adjustment. This finding indicates that education’s influence on attitude may operate primarily through increased health knowledge, rather than acting as a direct driver of attitude formation. This interpretation is consistent with prior studies highlighting the importance of health literacy, rather than formal education alone, in shaping health attitudes and behaviors. 33 Gender was not significantly associated with health attitude in either unadjusted or adjusted models. This suggests that attitudinal differences between males and females may be minimal or more strongly shaped by social and cultural norms than by biological sex. 30 Taken together, these findings underscore the central role of knowledge in shaping positive health attitudes. They highlight the need for public health strategies that focus on knowledge-based interventions, particularly behavior change communication (BCC) strategies that both inform and motivate. 37 Interventions should also be tailored to reach demographic groups with limited access to health information or lower baseline knowledge. By strengthening knowledge, it may be possible to foster more positive attitudes and, in turn, improve health-related behaviors at the community level.
For practice, even though less than one-third of the study population had been sick or had a relation sick from onchocerciasis, the majority of those infected took treatment from a health facility, and more than two-thirds 185, 69%) avoided river bathing to prevent the disease. This is similar to findings from Southwest Ethiopia 26 and other parts of Africa 38 where the majority of those affected by onchocerciasis use modern medicine to treat the disease. This study also investigated the predictors of good onchocerciasis prevention practices, focusing on socio-demographic and other determinants. It found that good knowledge, a positive attitude, being aged 41–50 years, and working in semi-skilled occupations were significantly linked to better preventive practices, even after controlling for confounding factors. The strongest predictors were: Good knowledge (15 times more likely to engage in good practices) and positive attitude (9 times more likely). These results support the Knowledge–Attitude–Practice (KAP) model, emphasizing that improving knowledge and attitudes leads to healthier behaviors. 34 Age was also significant, especially for those aged 41–50, possibly due to increased health awareness. Semi-skilled workers were more likely to adopt good practices than unskilled ones, potentially due to their experience with the disease. Although education and gender were linked to good practices in unadjusted analysis, these associations disappeared after adjustment, indicating that their effects may operate through knowledge and attitude rather than directly influencing behavior.
The limitations of the work were that the prevalence of the disease was not determined in the population studied and qualitative studies including focus group discussions among community members and in-depth interviews among stakeholders such as NTD officials, and community drug distributors were not carried out to support the quantitative results but despite these, the study still provides meaningful insights into the level of knowledge, attitude, and preventive practice of the communities towards onchocerciasis and especially the distribution of the ivermectin medicine in the communities studied.
Public health implications of the study
This study examined inhabitants’ knowledge, attitudes, and preventative practices (KAPP) concerning onchocerciasis in a few endemic regions in southwest Nigeria. The study’s findings are important for public health since they showed that tackling onchocerciasis in Nigeria and sub-Saharan Africa as a whole requires a multifaceted strategy. First, identified deficiencies in attitude and preventive practices highlight the need for community-based behavior change strategies, implying that interventions should be designed to address local beliefs and practices, promote preventive behaviors (such as wearing protective clothing and avoiding blackfly-infested areas), and encourage acceptance of mass drug administration (MDA) programs.
Secondly, identifying the factors associated with good knowledge, positive attitudes, and appropriate preventive practices toward onchocerciasis provides critical insights for strengthening disease control efforts. These findings will enable the development of targeted health education and behavior change strategies tailored to specific population subgroups. By addressing the socio-demographic determinants of KAP, interventions can be made more effective and equitable, leading to improved community participation in mass drug administration (MDA) and preventive measures. Ultimately, this evidence supports data-driven policy formulation and contributes to national and global efforts toward the elimination of onchocerciasis.
Conclusion
The study participants were generally familiar with onchocerciasis, but many lacked correct information on the causative agent and the correct mode of transmission. The study also showed poor attitudes and poor prevention practices by most of the respondents. Overall, the findings reinforce the importance of tailoring public health communication strategies to specific demographic groups. Younger individuals and those in unskilled occupations may benefit from targeted interventions to improve their health knowledge. Mass media, community-based programs, and workplace health education could serve as effective channels for reaching these groups. This assertion is in concordance with the reports of other studies on occupational hazards and the knowledge of respondents on health outcomes.39–42
Supplemental Material
sj-docx-1-phj-10.1177_22799036251376882 – Supplemental material for Knowledge, attitude and preventive practices towards onchocerciasis among residents of Ogun Waterside Local Government, IJEBU South-West, Nigeria: A cross-sectional study
Supplemental material, sj-docx-1-phj-10.1177_22799036251376882 for Knowledge, attitude and preventive practices towards onchocerciasis among residents of Ogun Waterside Local Government, IJEBU South-West, Nigeria: A cross-sectional study by Taiwo Mofadeke Jaiyeola, Adewale Allen Sokan-Adeaga, Tajudeen Tunde Tairu, Samuel Abiodun Kehinde, Esther Oluwabukunola Tella, John Adedayo Olanrewaju, Elizabeth Temitope Adekoya and Ekerette Emmanuel Udoh in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251376882 – Supplemental material for Knowledge, attitude and preventive practices towards onchocerciasis among residents of Ogun Waterside Local Government, IJEBU South-West, Nigeria: A cross-sectional study
Supplemental material, sj-docx-2-phj-10.1177_22799036251376882 for Knowledge, attitude and preventive practices towards onchocerciasis among residents of Ogun Waterside Local Government, IJEBU South-West, Nigeria: A cross-sectional study by Taiwo Mofadeke Jaiyeola, Adewale Allen Sokan-Adeaga, Tajudeen Tunde Tairu, Samuel Abiodun Kehinde, Esther Oluwabukunola Tella, John Adedayo Olanrewaju, Elizabeth Temitope Adekoya and Ekerette Emmanuel Udoh in Journal of Public Health Research
Footnotes
Acknowledgements
The researchers appreciate all the respondents who participated in the study.
ORCID iDs
Author contributions
TMJ and ETA designed the study. TMJ and ETA implemented the research. TMJ, ETA and AAS performed the literature review. TMJ, TTT and EEU analyzed and interpreted the data. TMJ, ETA, and AAS drafted the manuscript. AAS proofread the manuscript. TMJ arranged to journal specifications. TMJ, AASA, TTT, SAK, EOT, JAO, ETA and EEU critically reviewed the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The dataset presented in the study is available on request from the corresponding author during submission or after publication. The data are not publicly available due to confidentiality.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.