
Abstract
Background:
Atherosclerotic cardiovascular disease (ASCVD) is a leading cause of morbidity and mortality worldwide, including in the United Arab Emirates (UAE). Public awareness and engagement in preventive practices are critical for reducing ASCVD burden.
Design and methods:
A cross-sectional study was conducted among adults (≥18 years) residing in the UAE to assess their knowledge of ASCVD, engagement in preventive practices, and perceived barriers. A structured questionnaire was distributed online and in person across different emirates. Descriptive statistics and multinomial logistic regression were used for data analysis. A p-value of <0.05 was considered statistically significant.
Results:
Out of the total 401 participants, most were aged between 18 and 39 years (66.3%), females (74.1%), and of Middle Eastern nationality (68.8%). Sedentary work (51.9%), family history of ASCVD (34.7%), and overweight/obesity (41.1%) were the most common risk factors reported. The respondents better recognized classical ASCVD risk factors. Most respondents limited salt intake (67.3%) and screened for diabetes (59.4%). However, only 22.9% take nutritional supplements or consult professionals. Stress and time constraints (66.6%), postponing ASCVD preventive practices (61.3%), and lack of community-based interventions to prevent ASCVD (51.9%) were reported as major barriers. Healthcare-related occupation was significantly associated with better knowledge, while Middle Eastern ethnicity, younger age, and having health insurance were significant predictors of higher engagement in preventive practices.
Conclusions:
This study provides insights into knowledge of ASCVD, preventive practices, and barriers to ASCVD prevention among the surveyed population. Collaborative efforts addressing identified knowledge gaps and barriers are required to optimize ASCVD prevention.
Keywords
Background
Atherosclerotic Cardiovascular Disease (ASCVD) is a condition caused by the accumulation of plaque within arterial walls. 1 ASCVD includes diseases such as coronary artery disease, stroke, and peripheral artery disease. 2 It is associated with significant morbidity and mortality globally which underscores the urgent need for effective prevention strategies. Non-modifiable risk factors for ASCVD include age, gender, and heredity, while modifiable factors include diet, exercise, smoking, and alcohol use.2–4 Ineffective stress management, weight management, and poor sleep quality also heighten ASCVD risk. 5 Therefore, it is important to identify individuals with these risk factors to prioritize preventive measures. Risk estimation tools can help stratify individuals according to their ASCVD risk. 6 Assessing baseline ASCVD risk using global risk scores, based on routine office-based measurements, is endorsed by the American Society for Preventive Cardiology. 1 Healthcare professionals, including pharmacists, play a pivotal role in identifying individuals at risk of ASCVD who can benefit from preventive measures.7,8 The 2019 ACC/AHA Guideline on the Primary Prevention and Secondary Prevention Guidelines of ASCVD advocates for a lifelong commitment to a healthy lifestyle as the cornerstone of ASCVD prevention.9,10 Individuals are advised to optimize their lifestyle through dietary changes, 11 increased physical activity, and abstinence from tobacco use or exposure.3,6,10,12 In addition, controlling blood sugar and blood pressure is imperative, statins can be initiated to control blood cholesterol 13 among selected patients. Medication adherence to preventive drugs is critical.14,15 Although there are clear guidelines on ASCVD prevention, the adoption and engagement of the public are hindered by various personal factors, 16 or other system-based issues. Inadequate ASCVD risk assessment, lack of or limited insurance coverage, and hesitation of clinicians to start preventive medications can undermine preventive efforts. 15 Previous studies have shown that knowledge of cardiovascular disease (CVD) is associated with gender, age, education, smoking status, income, diet, weight, and family history.3,17 Additionally, promoting the adoption of prevention and treatment practices can foster improved knowledge and positive attitudes toward CVD prevention, culminating in enhanced self-reported practices. 17
There is limited research on ASCVD-related knowledge and preventive practices among the public in the UAE. However, cardiovascular disease is a major cause of morbidity and mortality in the UAE. The UAE is a fast-growing, multi-racial country where many people are adopting a modern sedentary lifestyle and poor dietary habits. Therefore, this cross-sectional survey aims to determine the self-reported prevalence of ASCVD risk factors, assess the public knowledge on ASCVD, assess their engagement in preventive measures, and identify perceived barriers. Furthermore, this research aims to determine the factors associated with ASCVD knowledge.
Methods
Study design and setting
This research is a cross-sectional survey designed to assess the UAE public’s knowledge of ASCVD, engagement in preventive practices, and perceived barriers among the target population. The reporting of this study conforms to the STROBE guidelines for observational studies, 18 as shown in Supplemental File 1.
Study population
Participants were eligible if they were adults (≥18 years) residing in the United Arab Emirates (UAE), defined as individuals who have lived in the UAE for at least six consecutive months and consider it their primary place of residence.
Inclusion and exclusion criteria
All adults residing in the UAE, with or without ASCVD, who consented to take part in the study were included. Individuals below 18 years of age, pregnant women, people with cognitive impairment, and those unable to understand Arabic or English are excluded.
Sample size determination and sampling
The sample size for this study was determined using the following formula: n = (1.962 × 0.5 × (1–0.5))/0.052. We assumed a 95% confidence level (Z = 1.96), a margin of error of 5% (E = 0.05), and a conservative estimate of the proportion (p = 0.5), and an infinite population. 19 The study requires a minimum sample size of approximately 385 individuals. The study used a convenient sampling (non-probability) approach to select participants. A convenience sampling method was used due to practical constraints and the exploratory nature of this public health survey. While this limits generalizability, it allowed the inclusion of diverse populations from various Emirates and occupations.
Ethical considerations
Ethical approval was obtained from Dubai Pharmacy College research and ethics committee (reference number: REC/UG/2023/04) to conduct this study. Written informed consent was obtained from all participants before data collection using the informed consent form. All collected data was anonymized, and personal identifiers were removed to ensure participants’ privacy.
Data collection tool development and validation
The data collection took place from December 2023 to March 2024. A structured questionnaire was developed following a structured approach to ensure content validity and clarity. Items were initially generated based on a thorough review of the relevant literature18–20 and aligned with the study objectives. The draft tool was then reviewed by two academicians from the College of Pharmacy, Dubai Medical University, to assess the relevance, clarity, and comprehensiveness of each item. Revisions were made accordingly. To ensure linguistic and conceptual equivalence, the tool was translated from English to Arabic using a forward–backward translation method by independent bilingual translators. Discrepancies were resolved through consensus among the research team and translators.
The questionnaire consisted of five sections (Supplemental File 2). Section 1 included demographic characteristics such as age, gender, ethnicity, education level, marital status, occupation, health insurance coverage, employment status, chronic health conditions, body mass index (BMI), smoking status, alcohol consumption, and medication use status. Section 2 included items that were answered with either a yes or no response to assess the proportion of self-reported ASCVD risk factors. Participants self-reported whether they had been medically diagnosed with conditions such as hypertension, diabetes, and high cholesterol. Thus, the risk factor data are based on participants’ perception of prior physician diagnosis. Section 3 included 26 items that were answered with a yes, no, or not sure response to assess the knowledge level about symptoms, risk factors, preventive practices, and complications of ASCVD. Additionally, sections 4 and 5 included closed-ended questions about engagement in preventive practices and barriers to adopting ASCVD preventive practices. The questionnaire was designed to take approximately 10–15 min to complete. This time frame was stated in the informed consent form and confirmed during the pilot testing phase, and helped ensure participant engagement and response quality.
The questionnaire was created using Google Forms. and was disseminated through multiple platforms, including academic mailing lists, public WhatsApp and Facebook groups, and professional LinkedIn networks, and college outreach programs targeting different emirates. To minimize selection bias, we also included in-person data collection in selected public settings such as parks and malls to ensure diversity in responses. No individual contacts were extracted or used; participation was voluntary via open survey links. This dissemination plan was described in the ethics application. Those who agreed to participate after being informed of the purpose, benefits, and risks were provided with the written consent form and the questionnaire link. The reliability of the scale used in the questionnaire was evaluated using the Cronbach alpha test, based on responses from 21 participants included in the pilot analysis. The Cronbach alpha value for the 26 knowledge items is 0.797, for the 11 practice items is 0.538, and for the 21 barrier questions is 0.881. The participants in the pilot study were not included in the final analysis. Feedback from the pilot phase informed final refinements to the tool, enhancing its reliability and suitability for use in the main study.
For the online component, the response rate could not be calculated due to the open distribution nature. For face-to-face distribution, the response rate was 80% (44/55). Distribution proportions by platform were not tracked due to anonymity in online channels.
Data analysis
The data analysis was conducted using SPSS version 29. Frequencies and percentages were used to summarize categorical variables. The knowledge score was calculated by assigning a value of 2 to a correct answer, 0 to an incorrect answer, and 1 to a “not sure” answer. The “Not sure” response was assigned 1 point to differentiate between incorrect knowledge (score 0) and uncertainty/lack of awareness (score 1). The total score for each respondent was calculated based on 26 knowledge items. A maximum score of 52 is considered 100%. The scores were categorized as good, moderate, or poor according to Bloom’s cutoffs: >80% (score of greater than or equal to 41) for good, 50%–79% (score of 26–40) for moderate, and <50% (less than 26 out of 52) for poor. Pearson correlation was utilized to identify the correlation between different types of barriers. Moreover, multinomial logistic regression was used to examine associations between demographic factors and ASCVD knowledge and engagement in preventive practice. A p-value < 0.05 was considered statistically significant.
Results
Demographic characteristics of participants
The survey was completed by 401 respondents. As shown in Table 1, young adults (18–39 years) make up 66.3% of the surveyed population. Females account for 74.1% of the surveyed population, while 68.8% of respondents have a Middle Eastern origin. The majority (93.2%) of respondents have a college or university education. Over half (57.3%) of the surveyed population resides in Dubai.
Demographic characteristics of the participants.

Proportion of risk factors of ASCVD among the respondents
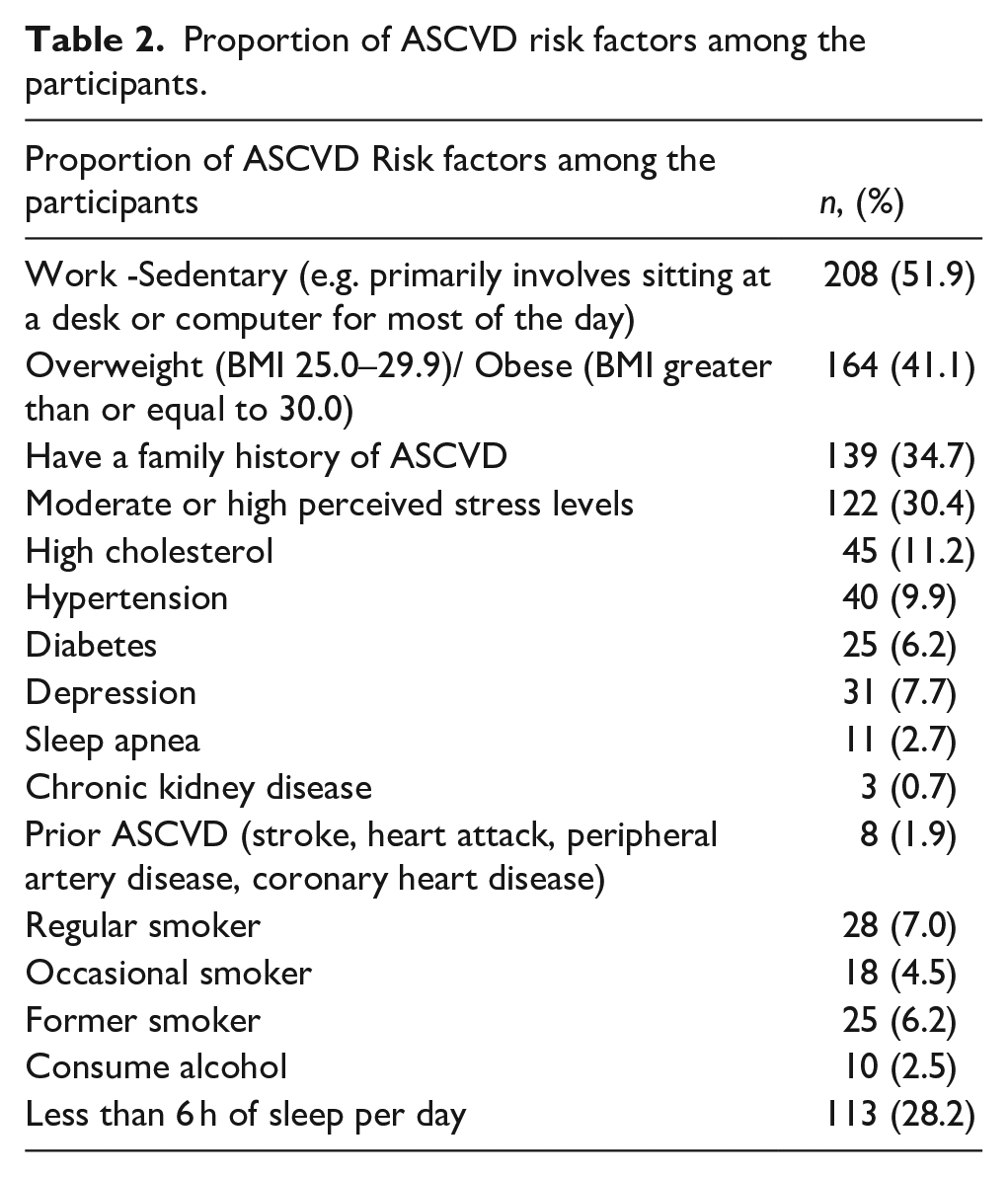
As shown in Table 2, half of the participants had sedentary work (51.9%), a considerable proportion of participants reported a family history of ASCVD (34.7%), and perceived high to moderate stress levels (30.4%). In addition, overweight or obesity (41.1%), high cholesterol (11.2%), hypertension (9.9%), and depression (7.7%) were the most common comorbid conditions reported by the respondents.
Proportion of ASCVD risk factors among the participants.
Knowledge of participants regarding ASCVD
The participants cited social media (51.1%), healthcare providers (34.4%), and friends/relatives (27.2%) as their major sources of information regarding ASCVD (Figure 1).
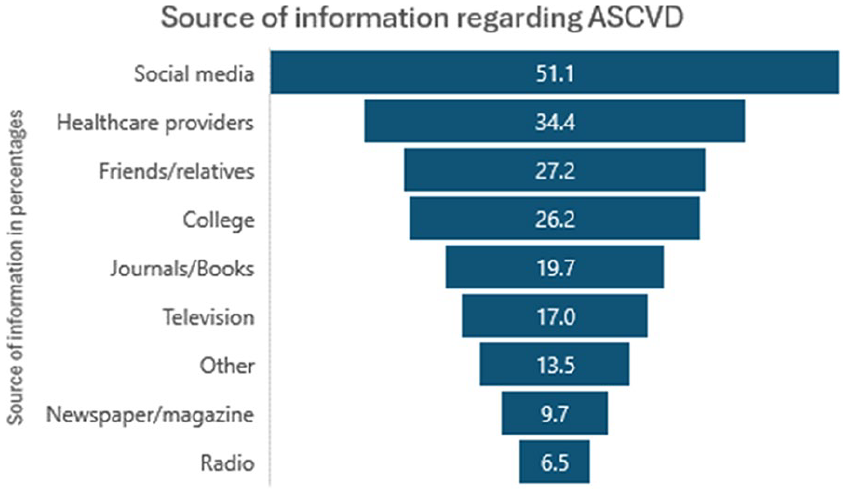
Source of information regarding ASCVD.
Two-thirds of the respondents knew that angina and shortness of breath are symptoms of ASCVD (Table 3). A high percentage of participants were aware of the association between abnormal cholesterol levels, hypertension, smoking, obesity, and increased risk of ASCVD, with percentages ranging from 61.1% to 83.5%. However, the level of awareness regarding other risk factors, including air pollution and sleep apnea, was relatively lower, with reported rates between 40.1% to 50.9%. Only 33.4% of the participants self-reported being aware of the heart disease risk calculator to estimate their risk.
Knowledge of participants on ASCVD.

Engagement of participants in ASCVD preventive practices
Most participants limited the salt intake (67.3%), screened for diabetes (59.4%), and maintained a balanced diet (58.4%). A smaller proportion received professional consultation on ASCVD management (22.9%), used digital devices for maintaining a healthy lifestyle (31.4%), or used nutritional supplements (25.9%) to prevent ASCVD (Figure 2).

Reported engagement in ASCVD Preventive practice.
A total of 92 (23.7%) participants claimed to take antihypertensives, statins, aspirin, or medications to lower blood sugar levels. However, 66 out of the 92 participants reported that they do take their prescribed medications consistently as directed by their healthcare provider.
Barriers to ASCVD preventive practices among the participants
Participants reported personal factors such as stress and time constraints (66.6%), procrastination (61.3%), lack of confidence in maintaining preventive measures (46.4%), and fear of judgment (36.9%). In addition, healthcare-related barriers such as long waiting times for services (41.9%), lack of telehealth services (40.6%), and poor patient-physician communication (48.9%), were reported. High cost of preventive practices (57.4%), limited access to healthy food (39.7%), and easy access to tobacco products (48.1%) were Socioeconomic barriers cited by the respondents (Figure 3).
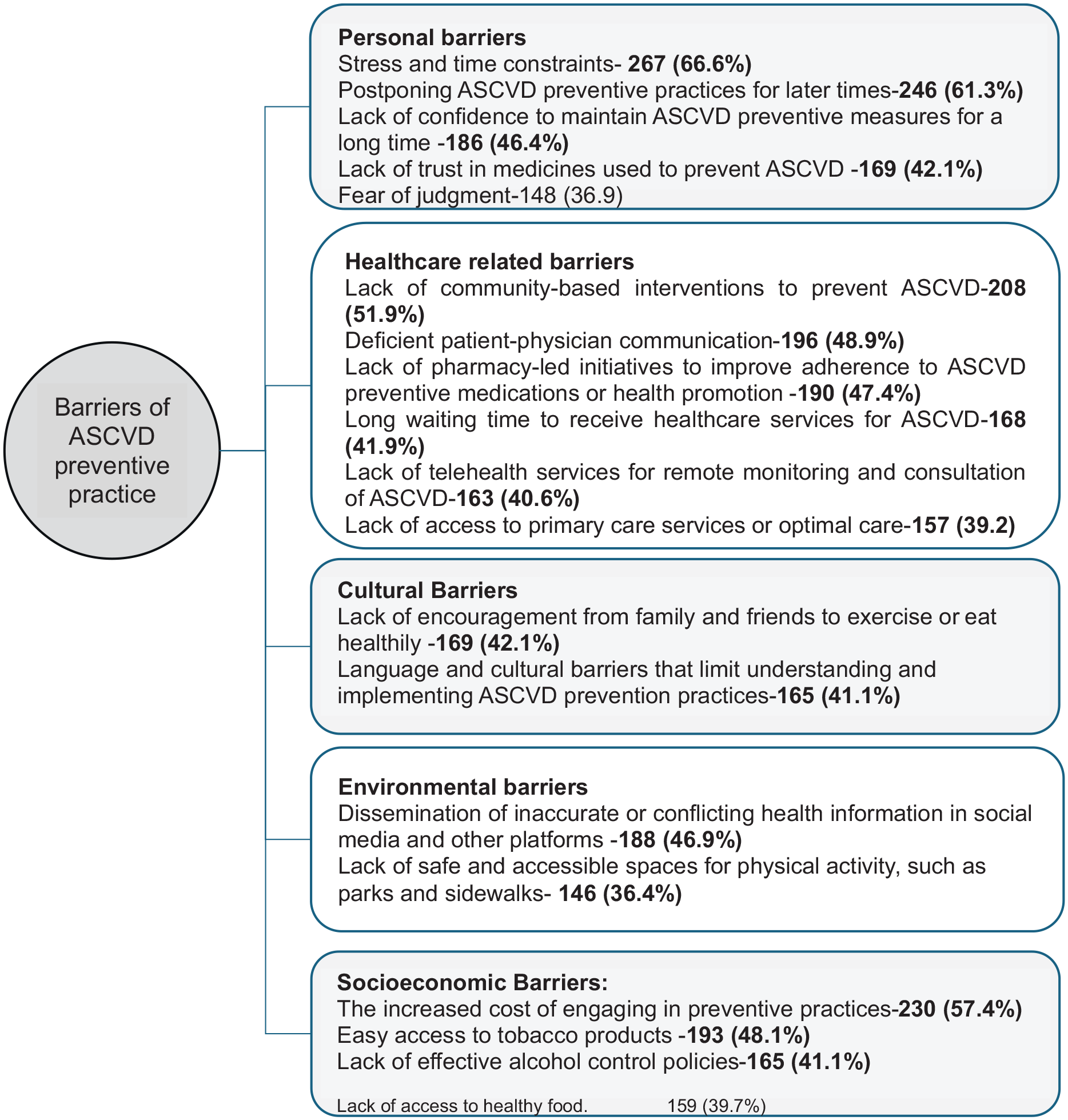
Reported barriers to ASCVD preventive practices.
Pearson correlation analysis among 21 identified barriers to ASCVD preventive practice revealed several statistically significant interrelationships. Notably, 63.8% of all barrier pairs showed moderate to strong positive correlations (r ≥ 0.30, p < 0.01). The strongest correlation was observed between easy access to tobacco products and lack of effective alcohol control policies (r = 0.655, p < 0.01). Similarly, the lack of pharmacy-led initiatives was strongly correlated with the lack of community-based interventions (r = 0.654) and inadequate ASCVD risk assessment by healthcare providers (r = 0.560). In addition, postponing ASCVD preventive actions was significantly correlated with stress and time constraints (r = 0.556), while lack of confidence to maintain preventive behaviors was associated with lack of physical activity infrastructure (r = 0.502). Social-environmental interdependencies were also evident; lack of family/friend encouragement was closely linked to the absence of safe exercise spaces (r = 0.498).
Demographic factors associated with ASCVD knowledge levels
Almost half of the respondents have moderate knowledge levels (Figure 4).

Distribution of knowledge levels among the respondents.
According to the results of multinomial regression analysis, participants with healthcare-related occupations were significantly more likely to report good Knowledge levels compared to poor knowledge levels (AOR = 5.038, p = 0.006). Middle Eastern and younger age showed borderline associations with better knowledge, but did not reach statistical significance (Table 4).
Multinomial logistic regression analysis of factors associated with ASCVD-related knowledge levels (reference category: poor engagement).

Note. AOR: adjusted odds ratio; CI: confidence interval.
Bolded values indicate statistical significance at p < 0.05. Reference categories: Age = older; Ethnicity = non-middle eastern; Education = secondary or less; Occupation = not working; Income = < AED 20,000; Marital status = single; Sex = male; Region = Northern Emirates.
p < 0.05.
As shown in Table 5, Participation in ASCVD preventive practice was significantly linked with younger age, Middle Eastern background, healthcare-related occupation, and lack of health insurance. Participants with Middle Eastern background showed higher odds of good engagement (p = 0.017), while younger participants were more likely to have moderate engagement (p = 0.001). In addition, individuals without health insurance were less likely to report good engagement compared to those insured (p = 0.028).
Multinomial logistic regression analysis of factors associated with engagement in preventive practices (reference category: poor engagement).

Note. AOR: adjusted odds ratio; CI: confidence interval.
Bold indicates statistically significant results (p < 0.05). Reference categories: Age = older; Ethnicity = Non-Middle Eastern; Education = secondary or less; Occupation = not working; Income ≤ AED 20,000; Marital status = single; Sex = male; Barrier = Yes; Health Insurance = Yes.
p < 0.05.
Discussion
The study determined the public’s knowledge of ASCVD, proportions of ASCVD risk factors, engagement in preventive practices, and barriers to ASCVD prevention among a sample of the UAE population. Furthermore, the study examined the demographic characteristics associated with knowledge levels.
Most of the participants were young, female, and highly educated. Many originally came from other Middle Eastern countries and are currently residing in Dubai. This predominance of younger adults is consistent with the overall demographics of the UAE. 21 The predominance of female and younger participants may reflect response bias influenced by social media recruitment patterns. While this group is important for ASCVD prevention efforts, the findings may not fully capture the perspectives of older adults or males, who often carry a higher ASCVD risk burden. The higher number of respondents from Dubai, compared to other emirates, can be attributed to the fact that Dubai is the most populous city in the UAE. Additionally, the researchers’ residence in Dubai made it easier to distribute the survey through their contacts. As shown previously, 22 a study conducted in primary healthcare centers to gauge the awareness of CVD risk factors among a sample of the UAE population included a higher proportion of UAE nationals and married individuals as respondents, in contrast to our study. The difference in demographic profiles underscores the variation in study populations and settings.
A recent study in the UAE revealed a high prevalence of modifiable risk factors for coronary heart disease, with many individuals exhibiting one or more of these risk factors. 22 Our study found that the most common risk factors for ASCVD were sedentary work, being overweight or obese, experiencing high to moderate levels of stress, and having a family history of ASCVD. Similar studies identified a lack of exercise, 23 stress, 23 and obesity23–25as the most frequent CVD risk factors in Arab countries. 23 Similarly, in our study, the top three self-reported comorbid conditions by the study participants are high cholesterol levels, hypertension, and depression. These risk factors, particularly hypertension and hyperlipidemia, have been reported to be the most prevalent CVD risk factors in a similar study. 22 Unhealthy eating habits, sedentary lifestyles, genetic predispositions, as well as the pressures associated with rapid urbanization and economic stresses in the UAE may have contributed to a high proportion of these comorbidities. These conditions frequently occur together and worsen each other’s effects, underscoring the importance of comprehensive healthcare strategies. Various free risk calculators (e.g. ASCVD Risk Estimator, Pooled Cohort Equations (PCE)) are available to assess the risk of developing heart disease. 26 The participants of this study were asked to report if they were aware of any heart disease risk calculators without any demonstration. However, very few respondents self-reported awareness of any heart disease risk calculators, similar to findings from a prior study. 27 Raising awareness through everyday health conversations and community outreach could help more people take early steps toward protecting their heart health.
Many of the participants are aware of established ASCVD risk factors. This may be attributed to the success of public health campaigns about CVD risk factors in the UAE.14,25 As noted previously in a study conducted in Dubai. 22 These risk factors have a detrimental impact on cardiovascular health, and it is important to continue efforts to reinforce awareness and promote healthy lifestyle choices. However, the study also reveals that non-classical risk factors such as sleep apnea, and air or light pollution appear to be less acknowledged as ASCVD risk factors, though research links both factors with increased risk of ASCVD. 28 This could be due to a focus on classical risk factors by healthcare providers and limited exposure of the respondents to literature about ASCVD risk factors. While many recognize the potential impact of ASCVD-related complications on quality of life, they have limited knowledge of available resources in the community for ASCVD prevention, and few respondents are aware of target blood pressure, cholesterol, and blood glucose levels for ASCVD prevention. Comprehensive public health education efforts that focus on raising awareness about preventive measures and available resources for ASCVD management are needed.
In our study, the top three cited sources of ASCVD-related information include social media, healthcare providers, family, and friends. The findings are consistent with a study in Lebanon, which also identified healthcare workers as the second-highest source of information 29 and a study in the UAE that underscores the growing influence of online platforms in disseminating health-related information. 22 Social media is a potent tool for health education and promotion. By involving healthcare providers in the digital domain, credible information can be disseminated to reach a broader audience and raise awareness about ASCVD.
A total of 178 (44.3%) participants in this study exhibited good knowledge, while 47.8% had a moderate knowledge score regarding ASCVD. The awareness level reported in this study was higher than that observed as shown in studies conducted in Lebanon 29 and Saudi 24 but lower that reported in Iran. 20 Direct comparison of the proportions of individuals with good, moderate, and poor knowledge across studies should be interpreted with caution. Although the topics were similar, variations in questionnaire design, item phrasing, and scoring criteria may limit the validity of direct comparisons, as differing methodologies can significantly influence knowledge categorization. However, there is still a knowledge gap to fill. The actual engagement in preventive practices to control modifiable risk factors is inadequate, as noted previously. 22 While many respondents mention reducing salt intake, getting screened for diabetes, and eating a balanced diet, fewer individuals engage in regular physical activity, like a study in Singapore. 30 Lower levels of physical exercise may be attributed to hot weather in the UAE and cultural practices. 31 The use of relaxation techniques, nutritional supplements, and digital tools for lifestyle management to prevent ASCVD is also limited. These findings indicate opportunities for targeted interventions and the need for a more comprehensive recommendation for ASCVD prevention. In the UAE, research on customized algorithms for CVD prevention has been identified as a priority. 32
In this study, healthcare-related occupations were associated with ASCVD knowledge levels. Other factors that showed borderline significance as a predictor of Knowledge levels include age and Middle Eastern background. Prior study in Manglore identified age influences coronary artery disease knowledge. 33 The trend, though not significant calls for further investigation. Individuals working in healthcare-related fields may possess greater familiarity with medical terminology, concepts, and preventive strategies, which could contribute to their enhanced knowledge of ASCVD. 34 In this study higher monthly income was not associated with a higher knowledge level as reported by Hassen et al. 35 Nearly 50% to 66.6% of the study participants reported stress and time constraints, postponing ASCVD preventive practices for later times, increased cost of engaging in preventive practices, lack of community-based interventions, deficient patient-physician communication, and easy access to tobacco products as barriers to ASCVD prevention. A recent study in the UAE highlighted that cultural reasons, boredom, and lack of family support hinder CVD prevention. 36 A previous study found concerns over a future diagnosis and distrust in medicine as significant barriers among individuals with cardiovascular risk factors in the United States. 37 In India, healthcare-related barriers, including long waiting times and deficiencies in patient-physician communication, were also reported. 38 Additionally, a study conducted in Brazil, identified limited access to healthcare services and medication adherence as significant barriers to secondary prevention of cardiovascular disease. 39 Furthermore, increased cost of preventive practices and easy access to tobacco products were identified as barriers in studies from Iran and Canada.40,41
The findings of this study showed that ASCVD preventive barriers do not occur in isolation, but rather form correlated domains of behavioral, systemic, social, and environmental problems. This calls for multi-component public health interventions to effectively mitigate the burden of ASCVD.
The findings suggest that demographic and occupational factors influence ASCVD preventive practices. Younger individuals may be more proactive in preventive practices, possibly due to greater exposure to health information via digital platforms. Studies in the UAE show that younger individuals may have better knowledge regarding heart disease risk factors, which may or may not necessarily translate into better preventive practice.22,42 Higher engagement among Arabs and healthcare workers highlights better awareness of CVD risk, while the lower engagement among uninsured individuals underscores potential barriers to accessing preventive care. Uninsured individuals may have limited access to health education and health prevention opportunities.
Strengths and limitations
This study included a sizable proportion of individuals who are mostly the target group for ASCVD prevention. The result of this study has important implications for practice and policy. However, several limitations exist. The response rate for the online component could not be calculated due to open distribution channels. The study did not incorporate behavioral theory frameworks to assess psychological factors influencing preventive practices. Another key limitation of this survey study is sampling bias. Most participants were young adult females of Middle Eastern nationality, which may restrict the applicability of the findings to the broader UAE population. Moreover, using self-reported data can introduce bias as participants may provide socially desirable responses or inaccurately recall information. In addition, assigning a “Not sure” response to a knowledge question as 1 point to differentiate between incorrect knowledge (score 0) may overestimate knowledge scores in consistently unsure individuals. The cross-sectional design only provides a snapshot of participants’ knowledge, and practice at a specific point in time. Lastly, the study may not have accounted for all confounders that could affect the associations.
Conclusion
The study presents significant findings on ASCVD awareness, knowledge, and preventive practices among a UAE sample. Participants demonstrate awareness of risk factors such as hypertension and smoking, but their knowledge of specific health parameters and prevention programs is limited. Many engage in preventive measures such as dietary changes and regular screenings, but face personal, healthcare-related, and socioeconomic barriers which are interrelated. Notably, healthcare-related occupation was significantly associated with higher knowledge levels, while Middle Eastern ethnicity, younger age, and having health insurance were significant predictors of greater engagement in preventive practices. These findings underscore the need for targeted interventions focusing on at-risk groups to enhance ASCVD prevention in the UAE.
Supplemental Material
sj-doc-1-phj-10.1177_22799036251373011 – Supplemental material for A cross-sectional survey on public awareness of atherosclerotic cardiovascular disease (ASCVD), preventive practices, and perceived barriers in the UAE
Supplemental material, sj-doc-1-phj-10.1177_22799036251373011 for A cross-sectional survey on public awareness of atherosclerotic cardiovascular disease (ASCVD), preventive practices, and perceived barriers in the UAE by Semira Abdi Beshir, Rizah Anwar Assadi, Maimouna Motaz Anis, Farah Mamoon Atout, Kenzy Hosam Hassan, Nujuom Ismael Shakir Alsawad and Daliya Said Abubakar in Journal of Public Health Research
Supplemental Material
sj-docx-2-phj-10.1177_22799036251373011 – Supplemental material for A cross-sectional survey on public awareness of atherosclerotic cardiovascular disease (ASCVD), preventive practices, and perceived barriers in the UAE
Supplemental material, sj-docx-2-phj-10.1177_22799036251373011 for A cross-sectional survey on public awareness of atherosclerotic cardiovascular disease (ASCVD), preventive practices, and perceived barriers in the UAE by Semira Abdi Beshir, Rizah Anwar Assadi, Maimouna Motaz Anis, Farah Mamoon Atout, Kenzy Hosam Hassan, Nujuom Ismael Shakir Alsawad and Daliya Said Abubakar in Journal of Public Health Research
Footnotes
Acknowledgements
The authors would like to thank all participants who took part in this study. Special thanks are also extended to the College of Pharmacy, Dubai Medical University, for approving and supporting the conduct of this research.
Ethical considerations
The research was approved by the Dubai Pharmacy College Research and Ethics Committee (Reference Number: REC/UG/2023/04).
Consent to participate
An informed consent form was provided with the survey questionnaire. Only participants who agreed to participate were granted access to complete the questionnaire.
Author contributions
SAB conceptualized the study, supervised the study, and led manuscript writing. RAA, MMA, FMA, KHH, NISA, and DSA contributed to questionnaire development, data entry, preliminary analysis, and drafting of the manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial supportfor the research, authorship, and/or publication of this article: The article processing Charges (APC) for the publication of this article is covered by Dubai Medical University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.