
Abstract
Background
A complex interplay of social and political influences, cultural and religious beliefs, the availability and interpretation of health and scientific information, individual and population experiences with health systems, and government policies contributes to the anxiety about vaccines and their programs that results in vaccine hesitancy. Vaccine hesitancy is becoming a serious threat to vaccination programs; in 2019, the World Health Organization (WHO) listed it as one of the top ten global health threats. The negative impacts of antivaccination movements are blamed for the major portion of the global resistance to vaccination.
Objective
To evaluate and compare parental attitudes and reluctance regarding routine childhood vaccinations versus COVID-19 vaccines among children in the United Arab Emirates (UAE).
Methods
A study of 102 parents with children admitted to SAQR Hospital in Ras Al Khaimah, UAE, was conducted using a convenience sample approach in a descriptive cross-sectional study. One-on-one interviews were conducted to gather data using the standardized Vaccine Hesitancy Scale (VHS) questionnaire developed by the WHO. Statistical Package for Social Sciences version 25 was used for data analysis.
Results
Vaccine-hesitant respondents are also highly resistant to the required proof of vaccination. A statistically significant difference (P = .000) was observed between parental reluctance to receive the COVID-19 vaccination and routine childhood vaccination. Parental knowledge of the COVID-19 vaccine hesitancy (P = .001) and confidence (P = .000) showed a statistically significant correlation. No significant correlation was observed with sociodemographic factors.
Conclusion
The impact of vaccine hesitancy on herd immunity, social, psychological, and public health strategies to combat vaccine hesitancy was observed in this study with various challenges to overcome in COVID-19 vaccination campaigns. Expanding access to and acceptance of vaccines among parents in low- and middle-income nations, as well as raising vaccination rates among those who express a lack of confidence in vaccines.
Keywords
Background
One of the top ten global health threats in 2019 was vaccine hesitancy, which was defined by the World Health Organization Strategic Advisory Group for Emergencies (WHO SAGE) Working Group on Vaccine Hesitancy as the “delay in acceptance or refusal of vaccination despite the availability of vaccination services”. The authors of this study found that in June 2020, less than 13,000 respondents in 19 of the world's hardest-hit countries had accepted the COVID-19 vaccine even though there was still no approved vaccine and that most countries were still going through the initial surge of SARS-CoV-2 transmission (Lazarus et al., 2021). Nearly one billion people had received a partial vaccination against COVID-19 as of December 14, 2021, while 3.64 billion people had received the full vaccination. Nevertheless, over 44% of the world's population, primarily those living in low- and middle-income countries (LMICs), remained unvaccinated, and the global case, hospitalization, and mortality rates remained high.
This persistent problem has continuously presented a serious threat to public health, with dire outcomes like the return of illnesses that were previously contained by immunization and the difficulty in developing herd immunity (Jacobson et al., 2015). Fisher et al. (2020) state that among the many factors influencing vaccine hesitancy, worries about vaccine safety and the possibility of adverse events (AEs) have drawn a lot of attention from the general public. Vaccine hesitancy has become an increasingly pressing concern within the field of public health in recent times.
Acute respiratory distress of severe magnitude SARS-CoV-2, a newly discovered severe acute respiratory syndrome, is a virus. It was initially isolated from three pneumonia sufferers who were linked to the Wuhan, China cluster of cases of acute respiratory illnesses. Virus infections and respiratory illnesses are very different from COVID-19 infections because they can be very harmful to young children (e.g., infants with respiratory syncytial virus). The outbreak was deemed a pandemic by the World Health Organization (WHO) in March 2020 after it was classified as a Public Health Emergency of International Concern on January 30, 2020. When someone is infected with SARS-CoV-2, they can spread the virus to two or three other people. Higher numbers, however, can be explained when this occurs in groups (clusters), such as nosocomial infections. It was estimated that a person with COVID-19 infection can infect up to 22 individuals (Kamps & Hoffmann, 2020). As a result, the study assessed and compared parental attitudes and levels of hesitancy toward COVID-19 compared to routine vaccinations. Parents’ attitudes are influenced by many factors, which this study identified and examined. These factors include sociodemographic traits, individual beliefs, ethnicity, and educational attainment.
Literature Review
According to a cohort study conducted in 629 acutely infected children with COVID-19 in Italy, “Long COVID-19 syndrome” is a real condition among pediatric patients. Long COVID Syndrome was occurring in children who had no underlying medical conditions. Gianfranco et al.'s study from 2022 indicated that children ages birth to five were more likely to experience acute respiratory symptoms. Conversely, adolescents between the ages of 11 and 16 were exhibiting neurological and psychological signs of infection. To prevent complications and long-term effects of COVID-19 infection in the pediatric population, the study demonstrated the significance of early monitoring, acute primary care, and immunization against the virus (Trapani et al., 2022).
September 2020 saw the development of the National Policy on COVID-19 vaccination in the United Arab Emirates (UAE). Under the direction of the Ministry of Health and Prevention (MOHAP), the COVID-19 vaccination program was implemented for residents and citizens over the age of 18, starting in December 2020, and for children between the ages of 5 and 11 in February 2022. To determine parents’ attitudes toward the COVID-19 vaccine for their children between the ages of 5 and 11, Alhazza et al. (2022) conducted a cross-sectional questionnaire-based national survey in Najran, Saudi Arabia. The results showed that roughly 72.2% of parents showed vaccine hesitancy, and approximately 27.8% were ready to vaccinate their children against COVID-19 as early as possible, compared to 15.51% of parents who were not at all willing to vaccinate their offspring (Alhazza et al., 2022).
A review of earlier research revealed that, in contrast to routine childhood vaccinations administered in the United Arab Emirates, there was no clear study on parents’ attitudes and reluctance regarding the COVID-19 vaccine. This study was carried out to ascertain parental acceptance and hesitancy toward vaccinating their children against COVID-19 as compared to routine vaccination because parents are the ones who ultimately decide whether or not to vaccinate their children.
An important factor in determining vaccination coverage and, eventually, public health outcomes is parents’ knowledge and attitude toward routine vaccination. Several regional studies have emphasized important conclusions. While there was a moderate level of hesitancy in AL Qassim, parents’ decisions were influenced by safety concerns, a lack of perceived need, and negative media (Al-Feraidi & Alghasham, 2023); in India, parents were still doubtful about the safety of vaccines and worried about long-term effects despite good immunization coverage (Jayaraj et al., 2023).
In contrast, mothers visiting Ugbiyokho Primary Healthcare Center to vaccinate their children showed a strong correlation between educational level and favorable attitudes toward immunization, highlighting the influence of knowledge on vaccination decisions. Numerous studies have shown that Muslims have generally positive attitudes and good knowledge regarding routine immunization; however, some misconceptions and concerns have been noted regarding the efficacy and safety of vaccines. Ansari et al. (2021) found that approximately 17.6% of participants thought vaccinations could cause autism, and 13.2% were worried about vaccination side effects. These studies highlight how crucial it is to address parental attitudes and knowledge gaps to improve vaccination uptake and acceptance.
Material and Methods
Study Design
A cross-sectional descriptive survey design was used to assess and compare parental attitudes and hesitancy toward COVID-19 versus routine childhood vaccines among children in the UAE.
Study Population
One hundred and two parents of children between 3 and 15 years of age visiting the pediatrics outpatient unit and admitted to Pediatric Units I and II in SAQR Hospital, UAE, were selected for this study. They used a nonprobability convenience sampling method to recruit the participants in this study from January to June 2023.
Study Size
In this study, approximately 138 admissions visited the pediatrics units at SAQR hospital. The sample size was calculated using the Rao soft online sample size calculation, with a 5% margin of error and 95% confidence level; the estimated sample size was 102 (http://www.raosoft.com/samplesize.html).
Inclusion Criteria
Parents who meet the following criteria: Children aged 3 to 15; only children between the ages of 3 and 15 who were admitted to the pediatric inpatient units (Unit I and Unit II) and expressed a desire to participate were included in the study.
Exclusion Criteria
Parents who have children who are unwell and unwilling to participate, parents with children admitted to Intensive Care Units, and parents with children younger than 3 years or older than 15 years of age.
Study Instrument
In 2012, the WHO Strategic Advisory Group of Experts (SAGE) on Immunization recognized this global challenge and established the Working Group (WG) on Vaccine Hesitancy Scale a tool used to assess and measure an individual's level of vaccine hesitancy. The vaccine Hesitancy Scale (VHS) was adopted and used for data collection, without any modification. This standard self-administered questionnaire has 15 items that evaluate different factors contributing to vaccine hesitancy, including fear of safety, lack of trust in healthcare professionals or the government, and personal beliefs about the efficacy of the vaccines. Arabic version of the tool was used for non-English speakers. The cutting point of the VHS shows that the Arabic-validated version of the scale has a good discriminatory power to predict the COVID-19 vaccine antecedent. Cronbach's alpha was .936. to confirm the validity and reliability of the tool. Various studies (Grossman-Giron et al., 2023) have reported that the VHS is a reliable and valid tool for assessing vaccine hesitancy in different populations, including parents, healthcare workers, and the general public. Many studies have reported that VHS has good internal consistency and test–retest reliability (Larson et al., 2015). There are 15 questions on the Likert scale of hesitant; (2) not sure (1), and nonhesitant (0). These findings demonstrate that VHS is a reliable data collection instrument for measuring hesitancy.
Scoring and Interpretations
The survey comprised distinct categories of assessment, each represented by a set of scale items. The first set, encompassing scale items 1 to 4, aimed to measure the “attitude” toward vaccines. Items 5 to 7 were grouped to assess the individual's “knowledge and awareness” about vaccines, while scale items 8 to 12 measured the “fear of potential adverse effects and hesitancy” toward vaccination. Lastly, items 13 to 15 were grouped to measure “trust and confidence” in information sources and healthcare professionals.
Data Collection Procedure and Ethical Consideration
Parents who met the criteria and were willing to participate were selected for the study, and the study's scope, objectives, and implications were explained to the parents.
Approval was obtained from the REC-019-2022/23-PG-N and the Ministry of Health and Prevention in March 2023. Written informed consent was obtained from the participants before the study. Strict adherence to the hospital policy and procedure about patient privacy and confidentiality was ensured.
Data Analysis
A Chi-squared test was done to determine the correlation between selected demographic data and parents’ level of knowledge about the role of the COVID-19 vaccine. The demographic factors taken in this study include age, gender, education, occupation, and ethnicity. t-Tests compared the mean and hesitancy scores for COVID-19 and routine vaccination. Multiple regression analyses identified the critical factors, such as parental knowledge, attitude, and confidence that contributed to their children's hesitancy toward COVID-19 vaccination.
Results
Table 1 displays the socio-demographic variables, which are listed below; 31–40 years old constituted the largest proportion, accounting for 41.2% of the sample. Out of the total number of participants, 74 individuals (72.5%) were females, while the remaining 28 participants represented males, accounting for 27.5%. The majority of participants, comprising 71 individuals (69.6% of the sample), were of Arabic ethnicity, while the remaining participants belonged to other nationalities. Of the parents 34.1% possessed a diploma-level education, while 66.6% of their parents, specifically 68 individuals, were unemployed.
Distribution of Participants Based on Demographic Variables (N = 102).

Table 2 displays the participants’ responses to different scale items. The data analysis and survey results revealed a spectrum of confidence, hesitancy, ambiguity, and skepticism among parents regarding the COVID-19 vaccine. Several scale items identified noteworthy responses from the parents. Of parents, 20.7% expressed a desire to postpone receiving the COVID-19 vaccine for reasons unrelated to illness or allergy, whereas 12.7% indicated a favorable attitude toward COVID vaccination. Likewise, 13.7% of individuals chose not to receive the vaccine due to reasons unrelated to illness or allergies, indicating a high level of hesitancy. Additionally, 24.5% displayed a moderate level of hesitancy. The average self-perceived vaccine hesitancy level of parents was approximately 3.15 on a scale ranging from 1 to 5. The data reveals a substantial degree of vaccine hesitancy among parents, characterized by notable apprehensions regarding vaccine safety and potential side effects.
Distribution Based on Responses of Parents Regarding COVID-19 Vaccination (N = 102).

Table 3 displays the demographic characteristics of parents and their level of knowledge regarding the COVID-19 vaccine. There is no significant correlation between parental knowledge and various demographic factors such as age, gender, ethnicity, and educational attainment. Based on the P-values, the null hypothesis (H0) was accepted, indicating that there was no significant association between parental knowledge about the vaccine and the demographic variables.
Association Between Parental Knowledge of COVID Vaccination with Selected Demographic Variables (N = 102).

P < .05 level.
Additionally, a statistically significant relationship was found between parental confidence, trust in the information regarding the vaccine and healthcare team, and hesitancy (β = .574, P = .000). The coefficient has a 95% confidence interval of 0.345 to 0.738. However, there was no significant relationship found between parental attitude and hesitancy (β = .151, P = .066). The coefficient has a 95% confidence interval ranging from 0.004 to 0.327. The P-value is greater than the significance level (P < .05), indicating that the relationship does not have statistical significance. Consequently, the alternative hypothesis was refuted, and the null hypothesis was supported.
Table 4 presents a distribution analysis that compares routine vaccination and COVID-19 vaccination based on the difference in mean scores. The t-value of 20.349 was highly statistically significant (P < .05), indicating that the disparity in willingness between the two vaccination types was not attributable to random chance. The P-value is .000, signifying that the observed difference was statistically significant. Thus, H1 was validated as the study findings exhibit substantial disparities in parental reluctance toward routine and COVID-19 vaccination.
Distribution Based on a Difference Between Routine Vaccination and COVID Vaccination (N = 102).

Significant difference at P < .05 levels.
Figure 1 illustrates the proportion of children who have received the COVID-19 vaccine as reported by their parents. Approximately 80.39% of parents have refrained from administering the recently developed vaccine for the novel coronavirus to their children. Just 19.6% of parents have opted to immunize their children against this potentially lethal virus.

Distribution based on the COVID-19 vaccination status.
Figure 2 illustrates the parental stance regarding the COVID-19 vaccine. According to the data, only 19.61% of parents exhibited a positive attitude toward COVID-19 vaccination. This was determined by their highly confident and confident responses. Approximately 38.24% of parents were uncertain, grappling with a predicament regarding whether or not to receive the vaccine. In addition, 26.47% and 15.69% of parents expressed hesitancy and high levels of hesitancy, respectively, which suggests a negative disposition toward the COVID-19 vaccine.

Distribution based on the parental attitude regarding COVID-19 vaccine.
Figure 3 depicts the parental knowledge level, which indirectly influences the vaccination rate of children against COVID-19 infection. Approximately 48.04% of parents exhibited a substantial level of understanding regarding the vaccine. In contrast, approximately 42% of parents exhibited a deficient or extremely deficient comprehension of different facets of the vaccine. In addition, a mere 17.65% of participants were determined to possess comprehensive knowledge regarding the specifics of the COVID-19 vaccine.
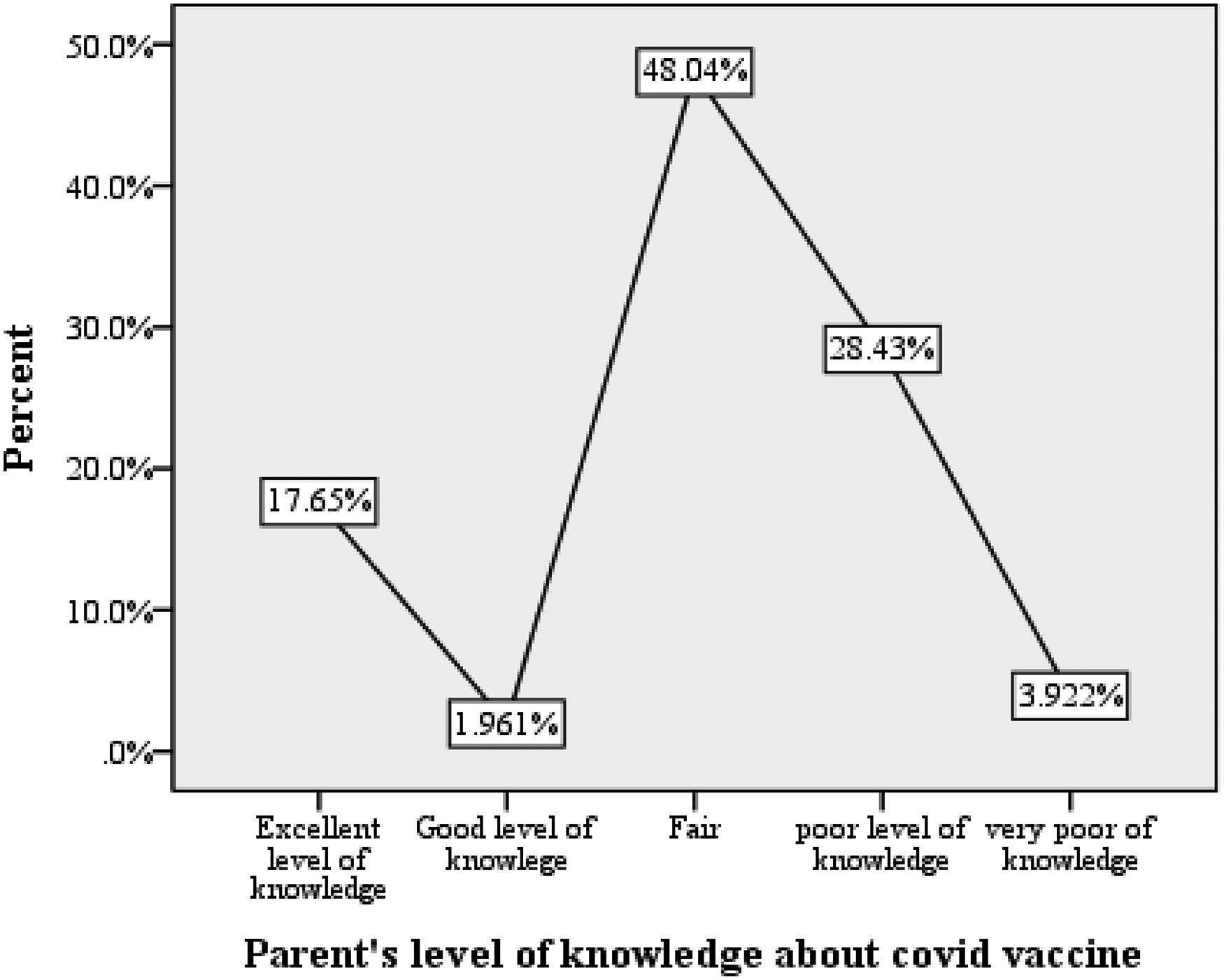
Distribution based on the level of knowledge of parents regarding COVID-19 Vaccine.
Figure 4 depicts the varying degrees of reluctance exhibited by parents toward the COVID-19 vaccine. Of parents 50% exhibit hesitancy and are disinclined to immunize their children against COVID-19 infection. In addition, a total of 3.92% of the participants expressed complete disapproval regarding the necessity of receiving the COVID-19 vaccination. Approximately 26.47% of participants exhibited uncertainty and ambiguity regarding the necessity of vaccination. However, only a minority of parents (17.65%) are both confident and willing to vaccinate their children.

Distribution based on parent's level of hesitancy toward COVID vaccine.
Discussion
Socio-Demographic Characteristics
The demographic data analysis revealed that most parents, comprising 41.2% of the total sample, are in the age group of 31–40 years; the gender distribution revealed that a significant portion of the participants was female, representing 72.5% of the sample. The current findings align with a study conducted by Alsuwaidi et al. (2020), which assessed the reliability of the Parent Attitudes about Childhood Vaccines (PACV) survey and determined the prevalence of vaccine hesitancy among parents in the UAE. The research study revealed that most participants (n = 300) were mothers, accounting for 77% of the sample, and most were within the age range of 30–49 years.
However, a contrasting trend was observed in a study conducted by Khatatbeh et al. (2022) across multiple countries within the Eastern Mediterranean Region, which compared parents of different age groups to the likelihood of vaccinating their children against COVID-19. Surprisingly, parents in the older age groups (≥50 years and 40–50 years) displayed a higher willingness to vaccinate their children compared to parents in the younger age group (18–29 years (Khatatbeh et al., 2022). These variations in the different study findings could be attributed to various factors, including differences in personal and cultural beliefs, access to information, and perceptions of vaccine safety and efficacy across the studied populations.
The study findings revealed that approximately 27.5% of parents possessed university degrees, while 25.5% had attained a high school level of education. According to UAE Government (n.d.), the literacy rates for both genders were recorded at approximately 95% in the UAE. Understanding the relationship between education and public awareness of health-related issues, including the importance of vaccinations, is crucial. The study suggests a significant correlation between parents’ education level and vaccination willingness.
This is supported by a survey conducted in 2022 that investigated COVID-19 vaccine acceptance across 23 countries and found that COVID-19 vaccine hesitancy increased in eight countries, with the highest hesitancy rate recorded in Brazil at 56.3% and the lowest in Poland at 2.4%. The research also pinpointed distinct demographic aspects contributing to childhood vaccine hesitancy, specifically in Ecuador, India, and South Africa; older parents demonstrated higher hesitancy rates, whereas gender played a role, with male respondents in Ecuador, Mexico, and Peru showing greater hesitancy. Furthermore, economic disparities emerged as parents with lower incomes in Canada, France, Germany, and the United States showed increased reluctance to vaccinate their children against COVID-19 (Lazarus et al., 2023). Based on the studies above and the results of the present study, a holistic approach will be necessary to address vaccine hesitancy and promote vaccination acceptance among parents.
Participants’ employment status reveals that the majority were unemployed (66.6%), with only 33.3% employed. This imbalance could be attributed to the sample size being predominantly females, accounting for 72.5%, while male participants were just 28 individuals.
A different scenario to the current study findings was observed in Najran, Saudi Arabia, where in a survey conducted by Aedh (2022), the majority of participants were male 56.9%) and aged between 26 and 40 (56.7%). The majority of participants (39.5%) who had postgraduate or higher degrees and were employed displayed a higher willingness to vaccinate their children against COVID-19; the difference could be attributed to regional differences (Aedh, 2022)
Parental Hesitancy
In the parental responses to the Vaccine Hesitancy Scale item on hesitancy toward the COVID-19 vaccine (item 12), the findings were approximately 44.1% (combination of both highly hesitant and hesitant responses) of parents were hesitant, around 20% (for combination of both strongly agree and agree responses) of parents were willing to vaccinate their children. The remaining 37% needed to be more specific about vaccination. Interestingly, nearly half of the sample (53 individuals) expressed high hesitancy in vaccinating their children, while only 19.6% showed a positive outlook regarding COVID-19 vaccination for their children.
Similarly, the study conducted by Gjini et al. (2023) in Albania and, Padhi et al. (2022) and Choi et al. (2021) also observed a high level of hesitancy toward COVID-19 vaccination among parents, with 75% of the participants showing hesitancy in different regions. On the contrary, the study by Kharaba et al. (2022) across the Emirates presented a positive response toward COVID-19 vaccination for children, in which 74% of parents confirmed that their children aged 16 years and above had already received the vaccine, and 71% expressed willingness to vaccinate their children aged above 5 years. The results of this study demonstrated a significantly higher acceptance of COVID-19 vaccination among parents in the surveyed emirates (Kharaba et al., 2022).
The current study findings indicated a low vaccination rate among children against COVID-19 (19.6%), which was quite concerning and highlighted the presence of vaccine hesitancy among parents. The prominent safety concerns (53%) and worries about adverse effects (52.9%) reported by a parent could contribute to their hesitancy. Understanding and addressing these parental concerns are crucial steps toward improving vaccination rates among children and effectively combatting the pandemic.
The variations in acceptance/hesitancy toward COVID-19 vaccination among parents in different parts of the world emphasize the importance of targeted interventions. Tailored communication strategies that are culturally sensitive and community-specific factors play a pivotal role in addressing vaccine hesitancy. Engaging with parents, understanding their concerns, and providing accurate and transparent information about vaccine safety and efficacy are essential steps in building trust and promoting vaccination acceptance.
To assess parents' knowledge and willingness toward Covid-19 vaccination and determine the association between selected demographic variables and parents' knowledge in UAE.
This research study's first objective showed no significant association between age and parental knowledge of COVID-19 vaccination (χ2 = 10.385, P = .582). Similarly, gender (χ2 = 8.415, P = .078), ethnicity (χ2 = 7.454, P = .489), and educational level (χ2 = 21.144, P = .173) of parents were found to have no statistically significant association with their knowledge on COVID-19 vaccine. The highest level of knowledge was observed in the undergraduate category, and the lowest level was found in the postgraduate category. The findings inferred that regardless of participants’ age, gender, or ethnicity, their knowledge about COVID-19 vaccines was similar. Notably, this lack of significant association could be due to the relatively small sample size and potential homogeneity within the sample. Although the results are not statistically significant, they still indicate some variation in knowledge among parents with different educational backgrounds. Parents with higher educational levels may have better access to information and resources, allowing them to stay informed about COVID-19 vaccines.
In a study by Padhi et al. (2022) in India, a positive association was found between parents’ educational level and their knowledge and willingness to vaccinate their children against COVID-19. Parents with a bachelor's degree or higher education exhibited a higher level of knowledge. They were more willing to vaccinate their children when compared to parents with lower educational levels (adjusted odds ratio [AOR]: 1.98, 95% confidence interval [CI]: 1.15–3.51).
A Saudi Arabian study by Altulaihi et al. (2021) identified a significant link between age and vaccine acceptance (parental age 31–40 years > covid vaccine acceptance), while the Taiwanese study by Deng et al. (2023) highlighted the gender-based differences (67.5% mothers vs. 50% others) in vaccine hesitancy among parents. In contrast to the current study, both the studies conducted by Altulaihi et al. in Saudi Arabia and Deng et al. in Taiwan align with the current study, indicating that education and occupational status were not significant factors influencing vaccine acceptance.
Half of the parents (48.04%) displayed satisfactory knowledge concerning the vaccine. Of parents 42% exhibited an inadequate understanding of the vaccine. Only 17.65% of the participants were identified to possess a comprehensive understanding of the details regarding the COVID-19 vaccine: Ashour et al.’s (2023) study in Saudi Arabia found that 45% of mothers (n = 293) had excellent knowledge of the COVID-19 vaccine, and the majority had either average or poor knowledge.
Bourguiba et al. (2022) reported that 93.1% of parents in the UAE had good knowledge and awareness about the COVID-19 vaccine, which does not support the current study's findings. Differences in the findings of these studies done in India, UAE, and Saudi Arabia can be attributed to the potential influence of ethnic variations on parents’ knowledge and awareness of the COVID-19 vaccine. The variation in knowledge levels observed among parents from different nations with different educational backgrounds emphasizes the importance of designing educational strategies specific to each ethnic group by addressing misconceptions and providing accurate information in various regional languages.
To compare parents’ hesitancy between routine childhood vaccine versus COVID-19 vaccine to their children in UAE. There was a significant difference in the willingness to vaccination among parents in a national survey conducted by Temsah et al. (2021) in Saudi Arabia; the majority of parents showed a positive attitude and agreement toward the effectiveness of routine childhood vaccines in comparison to the COVID-19 vaccine (Cohen's d: 0.946 and 0.826, respect very, with P-values < .001 using t-test). These findings align with the present study results, which also showed an extremely high significance (t-value of 20.349, P < .000), suggesting that the difference in willingness to vaccinate between the two types of vaccines was not due to random chance.
Moreover, the survey in Saudi clearly showed significant anxiety among parents regarding the severe side effects of the COVID-19 vaccine compared to routine vaccines (medium difference Cohen's d = 0.706, with P-value < .001), and the main reasons for refusal were inadequate safety information (69%) and concerns about side effects (60.6%), which was consistent with the current study where nearly 49% of parents were worried about the side-effects and 48 about the safety of the COVID-19 vaccine. Further, the report demonstrated that Saudi parents exhibited significantly more positive attitudes toward routine childhood vaccines compared to the COVID-19 vaccine, as reflected in a higher mean VHS score for routine vaccines (2.98 ± 0.58) than for the COVID-19 vaccine (2.63 ± 0.73) (P-value < .001), which strongly supports the present study findings.
Similar results were seen in a descriptive cross-sectional survey that aimed to analyze changes in parental attitudes toward routine childhood vaccines and COVID-19 vaccinations at different periods in Wuxi City, Jiangsu Province, China. Three waves of cross-sectional surveys were conducted from February 2020 to June 2021 and reported that the percentage of parents showing hesitancy varied across the three waves, with 7.8%, 15.1%, and 5.5% (P < .001). Throughout all three surveys, the most common reason for vaccine refusal was “concerns about vaccine safety and side effects” (Wang et al., 2022).
In contrast to the current findings indicating nearly 100% of children had routine childhood vaccinations, in a qualitative study conducted at the Children's Hospital of Philadelphia (CHOP), 61.0% of families demonstrated a nonhesitant attitude toward vaccines. In comparison, 39.0% expressed vaccine hesitancy; their children were not up to date on childhood vaccinations, and 63.4% of their first children were not vaccinated against influenza (Shen et al., 2022).
The factors influencing vaccine acceptance can be multifaceted, and understanding the reasons behind such discrepancies is crucial to ensure vaccine coverage and protection against preventable diseases.
Parental hesitancy toward the COVID-19 vaccine is an area of concern, as it impacted overall vaccination rates among children and hindered efforts to achieve herd immunity. Addressing parental concerns and misconceptions about COVID-19 vaccine safety and effectiveness is crucial, as many factors were associated with vaccine hesitancy among parents in Ras Al Khaimah, UAE, in the current year. Understanding the specific reasons behind the discrepancy (COVID-19 vaccine vs. routine vaccine) can aid in tailoring targeted communication strategies and educational campaigns to address parents’ concerns effectively. Interventions should focus on providing accurate and accessible information to increase parents’ confidence in both routine and COVID-19 vaccinations.
Limitations
Firstly, the small sample size of 102 participants prevents generalizing the findings to a larger population. With a limited number of participants, the study needed to fully represent the diverse perspectives and attitudes that may be present among a broader population of parents in the UAE.
Secondly, the use of nonprobability sampling, specifically convenience sampling, to select participants might have introduced bias into the study, leading to an overrepresentation or underrepresentation of certain groups of ethnicities, leading to a lack of representativeness for the broader population. Lastly, the study was limited to a specific unit within the hospital (pediatric units I & II).
Implications for Practice
1. Tailored Communication Strategies: According to the study, healthcare professionals should use customized communication techniques to address parents’ particular worries and reluctance about conventional immunizations as well as the COVID-19 vaccine. By identifying the underlying causes of parental reluctance, messaging can be more effectively tailored to each parent, leading to a rise in vaccine acceptance rates.
2. Thorough Vaccine Education: Educating patients about the significance, safety, and effectiveness of routine immunizations as well as COVID-19 should be a top priority for medical personnel. By addressing common misconceptions and worries, this information should enable parents to make knowledgeable decisions regarding vaccinating their children.
3. Rebuilding Faith and Confidence: The study highlights the significance of helping parents who are afraid to get vaccinations to regain faith and confidence in them. Healthcare personnel must cultivate a trustworthy rapport with parents by highlighting the advantages of immunization for both individual children and the larger society. This could entail open communication, compassion, and nonjudgmental handling of concerns. Positive attitudes toward vaccinations can also be strengthened by utilizing community influencers and reliable information sources.
Conclusion and Recommendation
This study aimed to assess parental attitudes and hesitancy regarding COVID-19 vaccination compared to routine childhood vaccination in a selected hospital in the UAE. One hundred and two participants who met the inclusion criteria were recruited using convenience sampling. The primary researcher conducted a one-on-one conversation with the parents and collected data using the WHO questionnaire (VHS).
The study found that only a few percent of parents displayed a positive attitude toward COVID-19 vaccination, while almost half were undecided, facing a dilemma about getting the vaccine. A quarter of parents were hesitant and highly hesitant, respectively, showing a negative attitude toward the COVID-19 vaccine compared to routine vaccination. However, most children had been vaccinated against routine childhood vaccines.
The current study concludes that parental knowledge and confidence are the primary determinant factors in COVID-19 vaccination for their children and highlights the diverse range of attitudes and hesitancy among parents regarding COVID-19 versus routine vaccination in the selected hospital setting. The findings stress the importance of targeted education and communication strategies to address concerns and misconceptions about COVID-19 vaccination, ultimately promoting vaccine acceptance and ensuring the well-being of children and the community.
A similar study can be conducted across multiple healthcare facilities across different emirates, which will provide a more comprehensive and inclusive perspective of parental attitudes toward vaccination. This study can be used as a reference point for addressing future pandemics.
Supplemental Material
sj-docx-1-son-10.1177_23779608241271660 - Supplemental material for Parental Attitudes and Hesitancy About COVID-19 Vaccination Versus Routine Childhood Vaccination in a Selected Hospital in the United Arab Emirates: A Cross-Sectional Study
Supplemental material, sj-docx-1-son-10.1177_23779608241271660 for Parental Attitudes and Hesitancy About COVID-19 Vaccination Versus Routine Childhood Vaccination in a Selected Hospital in the United Arab Emirates: A Cross-Sectional Study by Vijayalakshmi Selvam, Victoria Funmilayo Hanson and Sneha Pitre in SAGE Open Nursing
Supplemental Material
sj-docx-2-son-10.1177_23779608241271660 - Supplemental material for Parental Attitudes and Hesitancy About COVID-19 Vaccination Versus Routine Childhood Vaccination in a Selected Hospital in the United Arab Emirates: A Cross-Sectional Study
Supplemental material, sj-docx-2-son-10.1177_23779608241271660 for Parental Attitudes and Hesitancy About COVID-19 Vaccination Versus Routine Childhood Vaccination in a Selected Hospital in the United Arab Emirates: A Cross-Sectional Study by Vijayalakshmi Selvam, Victoria Funmilayo Hanson and Sneha Pitre in SAGE Open Nursing
Footnotes
Acknowledgments
The authors would like to express their sincere thanks to all the parents who actively participated in the study.
Author Contributions
VS did conceptualization, investigation, and writing and preparing the original draft.
VFH did methodology, investigation, and writing the review and editing.
SP did formal analysis, investigation, and writing the review and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Ethical approval was obtained from the RAK MHSU (RAKMHSU-REC-019-2022/23-PG-N) and the Ministry of Health and Prevention (MOHAP/REC/022/53-22PG-N). This was followed by approval from the hospital where the study was conducted. Informed consent was obtained from the parents who met the inclusion criteria after an explanation of the purpose of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.