
Abstract
Background:
Giardiasis represents a significant health problem in Ethiopia, originating from the consumption of contaminated water and poor hygiene practices, such as inadequate hand washing and improper food handling. Despite various regional studies in Ethiopia, this study provides updated insights.
Objective:
To determine the prevalence of Giardia lamblia (G. lamblia) infection and associated risk factors among patients who seek stool examinations at Bule Hora University Teaching Hospital, West Guji Zone, Ethiopia.
Methods:
A facility-based cross-sectional study on 134 patients seeking stool examinations was conducted from February 15 to March 15, 2023. A systematic random sampling method was used to select study participants. Data were collected using a pre-tested structured questionnaire. The stool samples were examined using the wet mount technique. Descriptive and inferential analyses were performed. The chi-square test was performed.
Results:
The results of this study revealed that the prevalence of G. lamblia infection was 18.7% (25/134; 95% CI: 12.1–25.3). This study revealed that factors such as rural residency (χ2 = 2.82, p = 0.027), poorly food hygiene practices (χ2 = 6.6, p = 0.03), lack of hand washing before a meal (χ2 = 4.25, p = 0.003), drinking non-piped water source (χ2 = 12.6, p = 0.0001), and untrimmed patient fingernails (χ2 = 3.47, p = 0.026) were significantly associated with G. lamblia among patients.
Conclusions and recommendations:
G. lamblia was detected in nearly one-fifth of patients. Targeted health education and improved sanitation are recommended to reduce its prevalence. Further research with larger samples is warranted.
Introduction
Giardia lamblia, also known as Giardia intestinalis, is a flagellate protozoan and the most common cause of intestinal infection globally. 1 This group of parasitic protozoans, known as Giardia, infects the small and large intestines of various ourvertebrate hosts. It is particularly prevalent in the tropical regions as a human intestinal protozoan, with G. lamblia ranging from asymptomatic to severely harmful in clinical severity. The severity of giardiasis is believed to be influenced by host factors such as nutrition, immunity, and co-infection with other agents, as well as pathogen factors such as strain and infectious dose. 1 It is the most commonly identified protozoan parasite in humans worldwide, with detection rates between 2% and 5% in developed countries and up to 20%–30% in developing regions. 2
The giardiasis infection with is the result of ingesting resistant environmental cysts through the fecal oral route, contaminated food, or water. 3 Ingestion of as few as 10 cysts can lead to human infection. The parasite can spread rapidly and widely in communities because mature cysts are infectious upon excretion after person-to-person transmission. 4 While G. lamblia primarily infects humans, it can also affect dogs, cats, beavers, and other animals, which carry cysts that can infect humans and contaminate water sources. Giardiasis is transmitted to humans by consuming cysts shed in the feces of infected individuals or animals. Intestinal parasitic infections are highly prevalent among individuals with low socioeconomic status, unfavorable living conditions, overcrowding, poor environmental sanitation, improper waste disposal, unsafe water supplies, and unhygienic personal practices. 5
Gastrointestinal symptoms such as stetorrhea, epigastric discomfort, abdominal cramps, greasy stools, flatulence, and diarrhea are indicative of mal-absorption. However, the infections frequently occur without overt clinical manifestations. Despite being commonly underdiagnosed, epidemiological evidence points to an association with malabsorption-related conditions. 6
In African nations, most Giardia infections occur in children under 5 years of age and school age, highlighting their vulnerability due to immature immune systems and lack of knowledge of personal hygiene. In Ethiopia, giardiasis has been less studied, but a nationwide survey targeting G. lamblia was conducted in 93 villages among students and others. Other parasitic diseases have been extensively investigated in different regions of the country. 7
In Ethiopia, previous studies on G. lamblia infection have reported varying prevalence rates across different regions. For instance, a study at Teda Health Center found a prevalence of 12.4%, 8 while in Borena Yabelo was 15.3%. 9 Other studies from Gambo Rural Hospital in southern Ethiopia reported 15%, 10 Mekanesalem Hospital in the northeast of the country showed 22.3%, 11 and Kochore Health Center reported 23.22%. 12 In contrast, Shahura Health Center in northwest Ethiopia reported a lower prevalence of 7.4%, 13 and the Gamo Gofa area in southern Ethiopia reported 10.6%. 14 Although comprehensive studies on this infection remain limited, existing research highlights significant variation in both prevalence and associated risk factors. This study offers new data on G. lamblia infection among patients at Bule Hora University Teaching Hospital who provided stool samples. This study fills a critical gap by providing new, localized data on the prevalence and risk factors of G. lamblia infection in the West Guji Zone, Ethiopia.
Methods
Study period and setting
The research was carried out between February 15 and March 15, 2023 at Bule Hora University Teaching Hospital, established in the city of Bule Hora (Figure 1). Located in the southern Oromia region, Bule Hora is 467 km away from Addis Ababa and comprises 41 administrative locations. The town has a teaching hospital, 6 health centers, and 27 health posts. The Bule Hora University teaching hospital provides healthcare services for more than 1.3 million people around the Bule Hora town and neighboring districts.

Map of the study area location.
Its laboratory is segmented into various departments, including parasitology, urinalysis, ART, serology, reception, bacteriology, chemistry, and hematology. 15 Last year, Bule Hora University Teaching Hospital conducted stool examinations for a total of 2028 patients.
Study population and design
A facility-based cross-sectional study was carried out to assess the prevalence and associated risks of G. lamblia in patients attending Bule Hora University Teaching Hospital for stool examination via direct microscopy. The study population consisted of all patients randomly selected for stool examination during the data collection period.
Inclusion and exclusion criteria
The study included all randomly selected patients fulfill the inclusion criteria such as willingness to participate, ability to provide a stool sample, and no recent use of anti-parasitic medication (within 2 weeks prior). Children under five were excluded to focus on school-aged children and adults.
Sample size determination
The sample size was calculated using the formula for a single proportion, based on a previously reported prevalence of G. lamblia of 12.4% (0.124) from a study at Teda Health Center. 8 The calculation assumed a 95% confidence level and a 5% margin of error.

therefore, adding 10% (13) of non-response rates, the final sample size required for this study was 137.
Where n represents the number of study subjects, Z is the standard normal distribution value for the 95% confidence interval (1.96), P is the prevalence of G. lamblia (12.4%), which is converted to 0.124. q is 1 − p (0.876), and d is the error margin taken as 5% (0.05).
Sampling procedure
The number of study participants was determined using the average number of patients sent for stool examination over 2 months from the previous year’s reports. The 2-month patient report (N) was divided by the total sample size (n) to obtain the interval (K): K = N/n, which is 338/137, resulting in K = 2.4 ≈ 2. The first participant was chosen through a lottery method. Following this, data collectors used systematic random sampling, selecting every second patient until the necessary sample size was fulfilled.
Data collection procedures
A structured face-to-face interview questionnaire was meticulously designed by drawing on established literature and validated tools from previous studies, ensuring alignment with the study’s objectives and contextual relevance,8,16–21 was utilized to collect data. This included questions on sanitary and environmental factors, socio-demographic characteristics, and health-related issues. The questionnaire comprised 4 segments with 23 items. Patient stool samples were collected using a standardized laboratory method. Then, the trained laboratory technicians analyzed the samples using direct microscopy. 8 The study method was followed STROBE guideline (Supplemental file).
Microscope examination of the stool sample
The wet mounting technique was utilized for stool examination. For solid stool samples, saline was added to the microscope slide, followed by a thorough mixing of the stool sample. A cover slip was used to immobilize the organisms and prevent the preparation from drying. The entire smear area was initially examined using a 10× objective; areas of interest were further magnified to 40× if needed. 21
Data quality assurance
Tools were pre-tested in 5% of study participants (7 individuals) at the Bule Hora Health Center to verify tool quality. These tools were adapted from the related literature. A proficient translator translated the English version into Afan Oromo and then returned to English to maintain the consistency of the survey. Daily reviews ensured the accuracy of the questionnaire. Stool cups were inspected for cleanliness, labeling, secure sealing, and proper ID numbering before sample collection. Regular maintenance checks were conducted on the microscopy equipment. Microscopic examination was conducted in strict adherence to standardized operating procedures (SOPs) established by the health centers, with stringent quality control measures implemented to guarantee the precision and reliability of the microscopy results.
Operational definitions
Food Hygiene practice/maintaining: Refers to behaviors and measures taken to ensure the cleanliness and safety of food includes proper hand washing before food preparation and eating, washing raw fruits and vegetables before consumption, using clean utensils and cooking equipment, safely storing food, and avoiding consumption of leftover or uncovered food. 22
Data analysis and processing
The acquired data were inspected for accuracy and consistency of the information from the study subjects. After entry into Epi-Data Manager version 4.62, the data were exported to SPSS version 25 for analysis. The analysis included descriptive and inferential statistics, using frequency, percentages, means, and standard deviation. Chi-square tests were performed, with statistical significance set at a p-value of 0.05. The findings were presented using text and tables.
Ethical considerations
The study received ethical approval from the Institutional Review Committee of Bule Hora University (reference No. IRC 025/2023). Before starting, informed consent was obtained from participants, ensuring that they understood the objectives of the study and that their well-being and dignity were paramount. Informed consent was taken from a parent or guardian for participants under 18 years of age. The privacy of the participants and the confidentiality of the collected data were rigorously safeguarded.
Results
Socio-demographic of the study participants
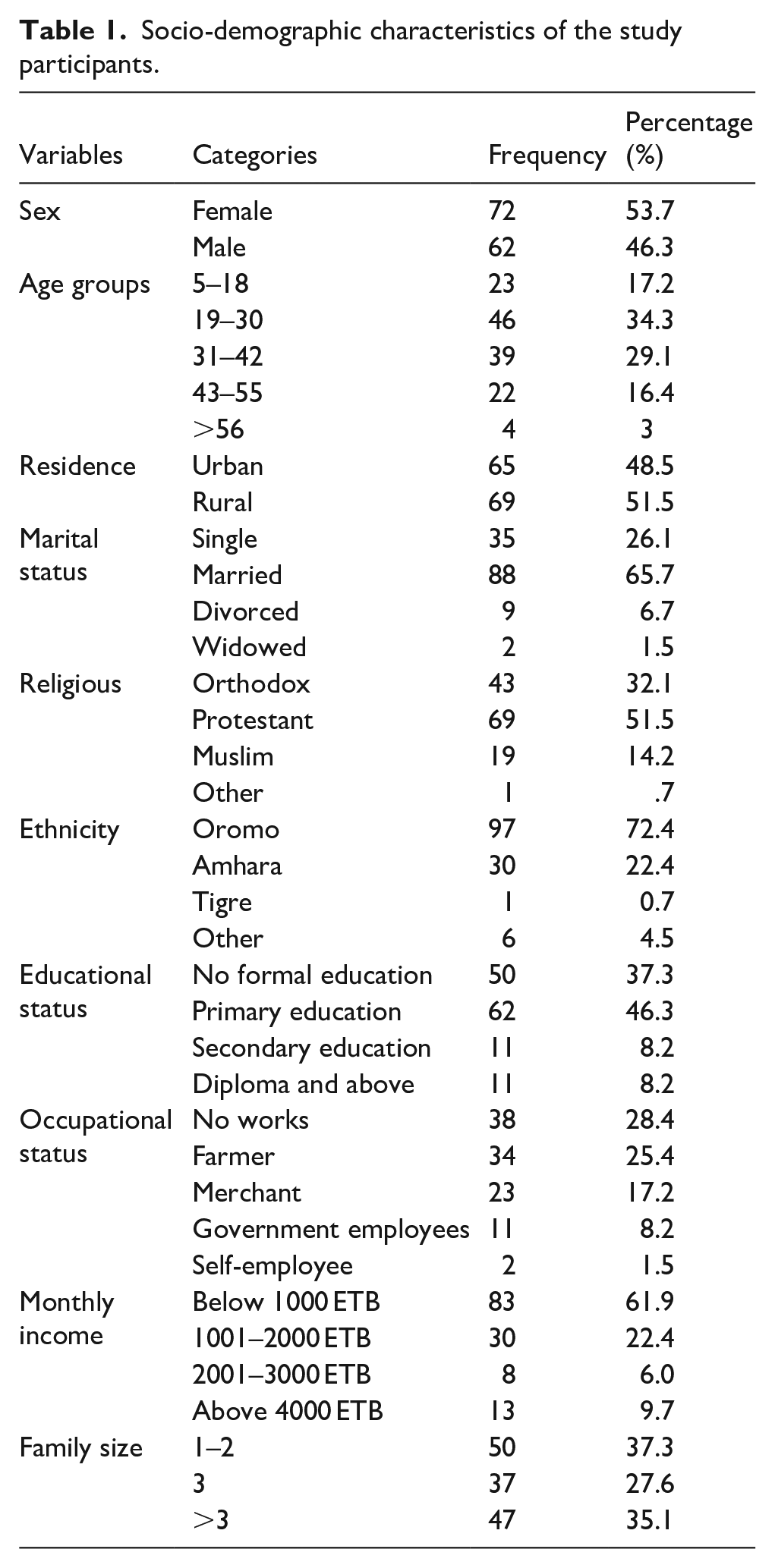
Data were collected from 134 participants, yielding a response rate of 97.81%. The ages of the respondents ranged from 5 to 70 years, with an average age of 29.45 (SD ± 15.63). The majority of the participants were between the ages of 19 and 30 years. Of the participants, 69 (51.5%) were women who grew up in rural areas. Regarding marital status, 65.7%, were married. Approximately 50 (37.3%) participants had not received formal education (refer to Table 1).
Socio-demographic characteristics of the study participants.
Health characteristics of study participants
Of the 134 study participants, 94 (70.1%) reported a history of parasitic infections. Fewer than one-third (29.1%) had previously been admitted to a hospital. Regarding food hygiene practices, 71 (53.3%) of the respondents always practiced it, while 62 (46.3%) did so occasionally (refer to Table 2).
Health conditions of study participants seeking stool examination at the Bule Hora University Teaching Hospital, West Guji Zone, Ethiopia, 2023.

Hygiene and sanitation characteristics of study participants
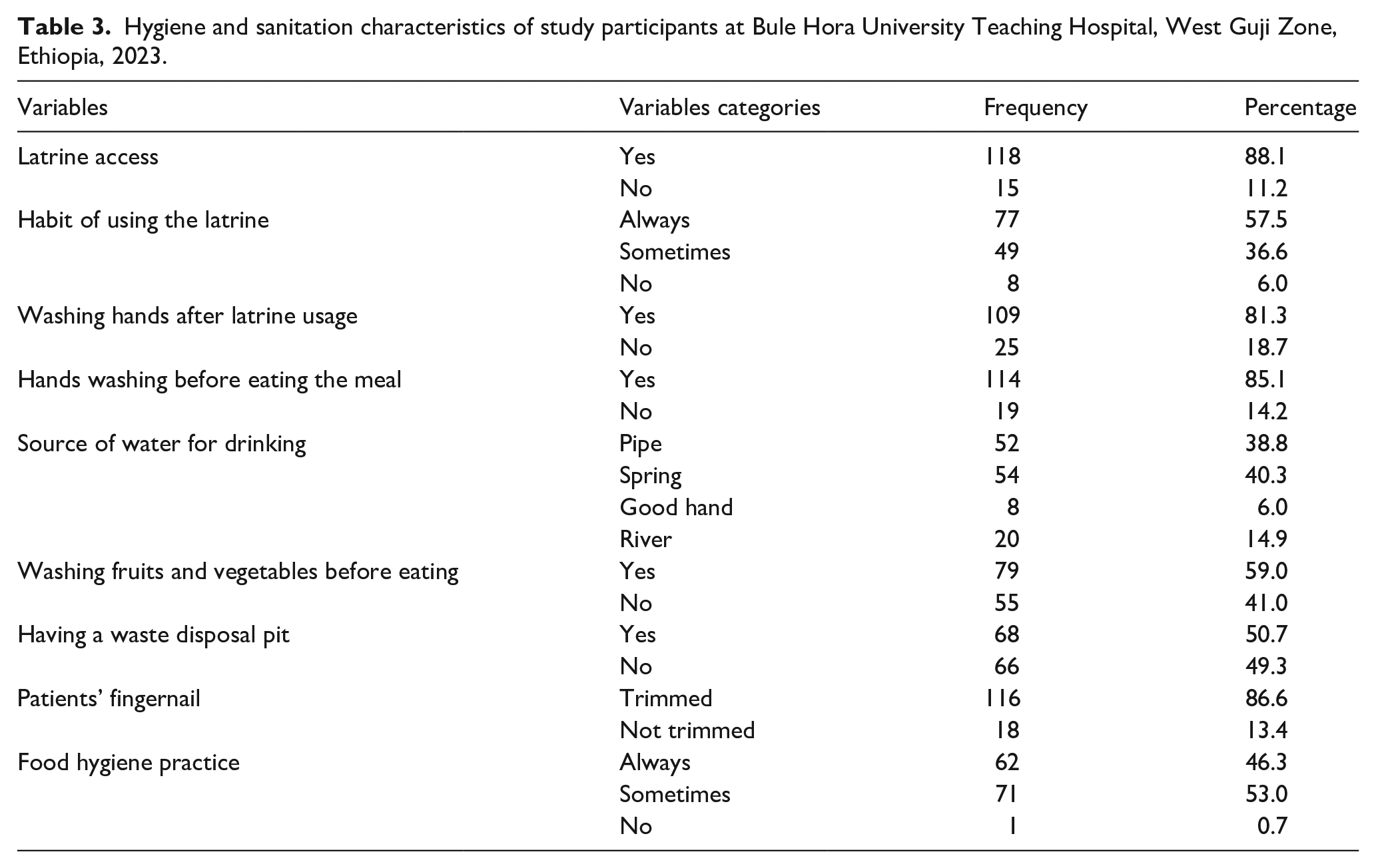
The study findings indicated that the majority of participants, 118 (88.1%), had access to a latrine; however, only 77 (57.5%) used it regularly. Furthermore, 54 (40.3%) of the respondents consumed spring water and 116 (86.6%) maintained trimmed fingernails (refer to Table 3).
Hygiene and sanitation characteristics of study participants at Bule Hora University Teaching Hospital, West Guji Zone, Ethiopia, 2023.
Prevalence of G. lamblia among stool examination seekers
The results of the study indicated that the prevalence of G. lamblia infection was 25/134 (18.7%), with a 95% confidence interval of 12.1%–25.3%. Out of the total, 25.7% of rural residents were diagnosed with G. lamblia. Among those with a history of parasitic infections, 29.3% were found to have G. lamblia. Notably, 38.9% of individuals who did not trim their fingernails were diagnosed with G. lamblia. Additionally, 29.3% of those who did not wash their hands before meals were diagnosed with the parasite. Furthermore, among those who drank river water, 30% of individuals were diagnosed with G. lamblia (Table 4).
Prevalence of G. lamblia among participants seeking stool examination at Bule Hora University Teaching Hospital.

Factors associated with the prevalence of G. lamblia infection
The Chi-square (χ2) test revealed statistically significant associations with G. lamblia. Notable factors included residency (χ2 = 2.82, p = 0.027), adherence to food hygiene practices (χ2 = 6.6, p = 0.03), hand washing before meals (χ2 = 4.25, p = 0.003), drinking water source (χ2 = 12.6, p = 0.0001), and the patient’s fingernail conditions (χ2 = 3.47, p = 0.026) as significantly associated with G. lamblia infection.
Rural residents participating in the study were nearly three times more likely to be infected with Giardiasis compared to urban residents. The likelihood of giardia infection was nearly seven times higher among participants who did not practice food hygiene compared to those who did. Additionally, giardiasis was associated with not washing hands before meals and drinking water from non-piped sources, such as rivers. Lastly, participants who did not trim their fingernails were nearly three times more likely to be infected with giardiasis than those who kept their nails trimmed (as shown in Table 5).
Factors associated with G. lamblia among patients seeking stool examination at Bule Hora University Teaching Hospital, West Guji Zone, Ethiopia, 2023.
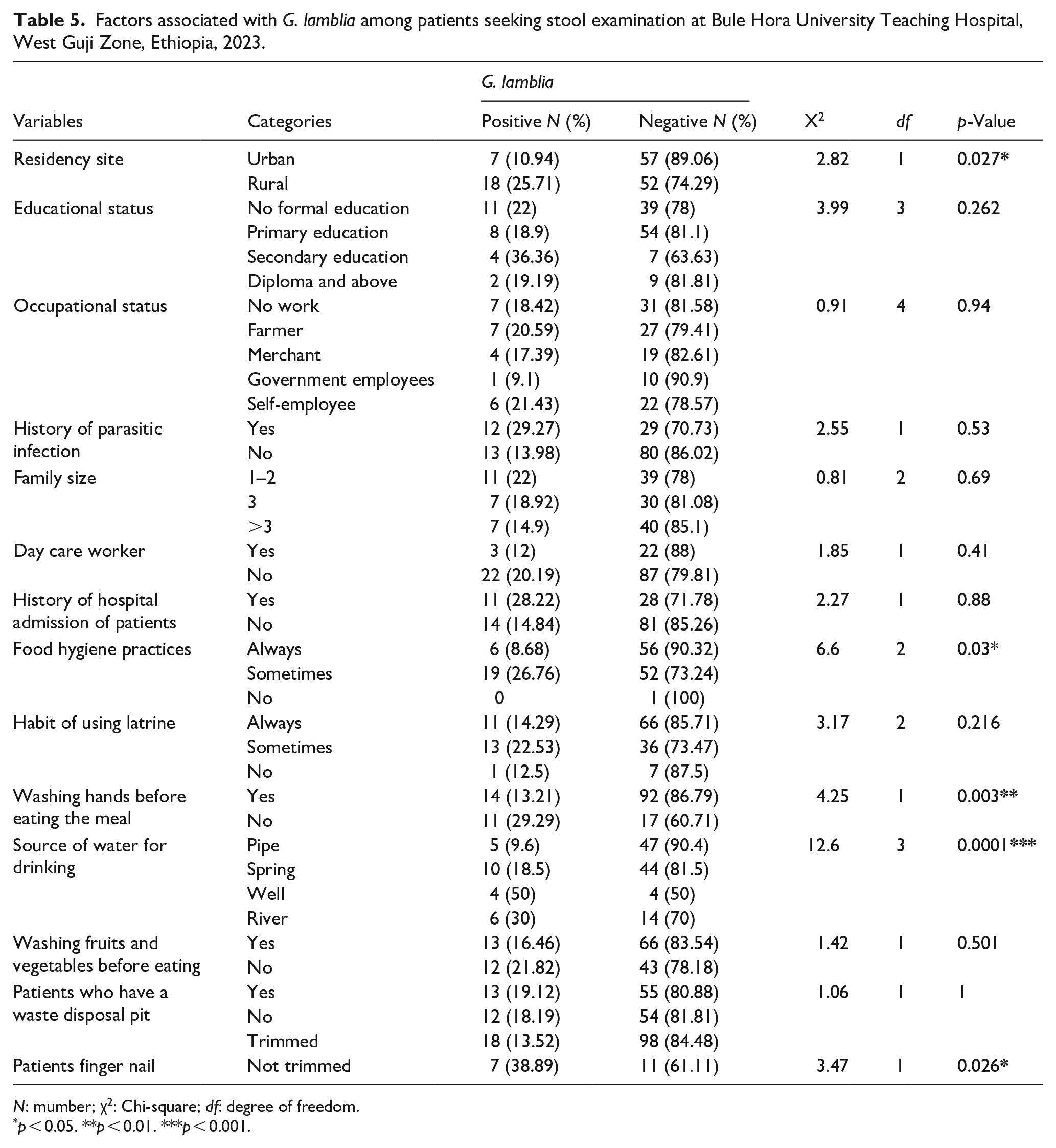
N: mumber; χ2: Chi-square; df: degree of freedom.
p < 0.05. **p < 0.01. ***p < 0.001.
Discussion
This study revealed an 18.7% prevalence of G. lamblia infection (95% CI: 12.1–25.3), aligning with the findings in Ethiopia Borena Yabelo 15.3%, 9 Gambo Rural Hospital in southern Ethiopia 15%, 10 Mekanesalem Hospital Ethiopia 22.3%, 11 Kochore Health center 23.22%. 12 However, the prevalence was higher than that reported in Yemen Al-Manssora 9.95%, 23 Thailand at 6.2%, 24 Shahura Health Center in northwest Ethiopia at 7.4%, 13 and the Gamo Gofa area in southern Ethiopia at 10.6%. 14 These variances could stem from differences in study environments, and cultural and socio-demographic factors. Factors such as stool examination methods, health conditions, water supply, feeding and cultural practices, study periods, age groups, and geographical locations could contribute to the differing results between studies.
On the contrary, the prevalence in this study was lower than those conducted in Sudan (21%), 25 and Sidama (27.1%). 26 Our study, conducted in a university hospital in an urban setting, suggests that changes at the study site might explain these discrepancies. Another possible explanation for the difference could be advances in hospital laboratory services, especially quality. Similarly, the lower prevalence in this study could be attributed to improvements in medical center services and the demographics of the study population. Additionally, the variation might be due to the diverse infrastructure present in healthcare facilities, such as laboratory tests, water, and medical equipment.
The study was revealed the association between the participants’ residency and G. lamblia infection, indicating that rural residents were more likely to contract giardiasis. This finding is supported by the previous studies conducted in Cuba, 16 Portugal, 17 and Thi-Qar, southern Iraq, 18 which indicated a similar trend in the Sidama zone. 26 This finding are significant for global public health strategies aimed at controlling giardiasis. First, it underscores the importance of improving water, sanitation, and hygiene (WASH) infrastructure in rural communities, which is a cornerstone of the World Health Organization’s (WHO) neglected tropical disease (NTD) control programs. Ensuring access to safe drinking water, promoting the use of improved sanitation facilities, and implementing community-wide hygiene education campaigns can significantly reduce the transmission of G. lamblia and other diarrheal diseases. The results of the current investigation also indicated a relationship between G. lamblia infection and poor food hygienic practices. This finding agrees with a previous study done in Goiânia, State of Goiás, Brazil, that linked family size and food hygiene. 20 The association between inadequate food hygiene and G. lamblia infection underscores a critical pathway for parasite transmission and has significant implications for global public health strategies aimed at controlling giardiasis. Poor food hygiene practices, such as improper handling, preparation, and storage of food, create opportunities for contamination with G. lamblia cysts, which are highly resistant and can survive in the environment for extended periods. From a global public health perspective, these findings align with the World Health Organization’s (WHO) emphasis on food safety as a key component of disease prevention. These findings highlight the need for targeted interventions to improve food safety and hygiene practices, particularly in settings where regulatory oversight and public health infrastructure may be limited.
Moreover, this study’s results suggest that hand washing practice before meals was associated with G. lamblia infection. The data indicates that participants who did not wash their hands before eating were more susceptible to giardiasis. This observation is consistent with research conducted in the Sidama zone. 26 This association can be attributed to the crucial role that hand washing plays in removing parasites and other pathogens from the hands, thereby reducing the risk of ingesting them. When individuals wash their hands thoroughly with soap and water before eating, they effectively eliminate any giardia cysts that may be present on their hands due to contact with contaminated surfaces, soil, or fecal matter. This preventive measure is particularly important in environments where hygiene standards are compromised, as it directly interrupts the transmission cycle of the parasite. Additionally, the study identified a relationship between the source of drinking water and G. lamblia infection; individuals who drank non-piped water were at a higher risk of contracting giardiasis, corroborating findings from previous studies at Gonder Hospital 27 and Nekemte Specialized Hospital. 28 The association between unsecured water sources and G. lamblia infection can be attributed to the fact that these water sources often serve as breeding grounds for parasites. When water sources are not properly secured or treated, they can become contaminated with giardia cysts from animal or human feces. Individuals who consume water from these sources are at a higher risk of ingesting the parasites, leading to infection. Furthermore, the study highlighted a significant relationship between fingernail condition of patients and the prevalence of G. lamblia. Parasites that reside under untrimmed fingernails could be ingested during eating. Alternatively, untrimmed fingernails may provide a convenient hiding spot for parasites.
Strengths and limitations of the study
The strength of the study was the primary and laboratory data obtained from randomly selected patients. The design of this study has limitations, as it restricts the ability to establish causal relationships, no multivariate analysis was performed, which prevents controlling for potential confounders; and there is a small sample size that limits the generalizability of findings to the target population. There might be a bias in selection due to the lack of information on symptom status (asymptomatic vs symptomatic) of the study population. Its single-season timeframe and the reliance on microscopy for stool examination, which lacks the precision of molecular diagnostics and multi-seasonal data. Co-parasitization is also not studied.
Conclusion
Giardia lamblia infection was detected in nearly one-fifth of patients. Key risk factors included poor hygiene, unsafe water, untrimmed fingernails, and rural residency. To effectively combat the spread of giardiasis, health extension workers and healthcare providers should prioritize educating the community on maintaining proper fingernail hygiene, practicing safe food handling, and treating unprotected water sources. They should emphasize the importance of keeping fingernails clean and trimmed to prevent the transmission of giardia cysts. Infrastructure improvements and future multicenter studies with molecular diagnostics are recommended. Additionally, it suggests that researchers conduct further studies in various settings, such as health centers and hospitals, with larger sample sizes across different seasons.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251368444 – Supplemental material for Giardia lamblia infections and associated risk factors among patients seeking stool examination at Bule Hora University Teaching Hospital, West Guji Zone, Ethiopia
Supplemental material, sj-docx-1-phj-10.1177_22799036251368444 for Giardia lamblia infections and associated risk factors among patients seeking stool examination at Bule Hora University Teaching Hospital, West Guji Zone, Ethiopia by Alqeer Aliyo, Nebiyu Taye and Girma Ashenafi in Journal of Public Health Research
Footnotes
Acknowledgements
We first express our gratitude to the Bule Hora University Institute of Health for providing us with the opportunity to conduct this study. We also extend our sincere thanks to the Department of Medical Laboratory Science staff for their support in our research. Additionally, we are grateful to our friends and colleagues for their invaluable assistance and support throughout the development of this research article.
Consent for publication
Not applicable.
Authors’ contributions
Alqeer Aliyo contributed to conceptualization, resource gathering, laboratory analysis, and data analysis. Nebiyu Taye and Girma Ashenafi were responsible for the data curve, supervising and visualizing data collection, preparing and editing the manuscript, and approving the final version. All authors have read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Upon reasonable request, the corresponding author will provide the data sets that were used and analyzed during the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.