
Abstract
Background
Around half of the world's population is infected with Helicobacter pylori (H. pylori), according to data from a recent systematic review. H. pylori infection is extremely common around the world. It is the most prevalent disease in Ethiopia and contributes to both morbidity and mortality. Patients with gastritis, peptic ulcers, and stomach cancer have been reported to harbor H. pylori.
Objective
The aim of this study was to determine the trends of Helicobacter Pylori infection among patients attending the Bule Hora University Teaching Hospital from 2018–2022, Bule Hora, Ethiopia.
Method
A hospital-based retrospective study design was conducted to recruit 314 sampled data from the logbook, which were five-year data (2018-2022) from the Bule Hora University Teaching Hospitals. Data were extracted using structured checklists. The sample size was calculated using the single-population proportion formula. Study participants were selected using a systematic random sampling technique. Data were entered in EpiData 4.6 and exported to SPSS Version 26 for analysis.
Results
Approximately 314 complete data from selected participants were collected and evaluated for the present study. The mean age was 29.01 (SD ± 4.93). Most of the respondents (39.2%) were in the age group of 21 to 30 years. The general prevalence of H. pylori observed in this study is 28% (95% confidence interval [CI], 23-32.9). The prevalence was higher in women (71.6%) than in men (28.4%). In terms of age category, those over 60 years of age were observed with the highest positiveness for H. pylori with 38.1% and the trend of H. pylori prevalence fluctuated from 2018 to 2022.
Conclusion
In total, 28% of the study participants had H. pylori, but there was variation in the prevalence of H. pylori infection between 2018 and 2022. Compared to other age groups, the 60-year-old age group had a higher prevalence of H. pylori and this prevalence continued to increase annually. The concerned parties must be interested in raising awareness and establishing criteria for the eradication of these bacteria.
Introduction
The motile rod Helicobacter pylori (H. pylori) is positive for urease, catalase, and oxidase. Along with small spirals of 1-2 wavelengths, it measures 2.5 nm by 0.51. Through methods of acid resistance and colonization factors, it survives in the harsh environment of the stomach by colonizing the antrum and the body of the stomach. It possesses four unipolar sheath flagella that show bulbous tips and may show bipolar flagella when dividing. 1
Worldwide, 50% of people have H. pylori infection. However, the frequency of this bacterium differs between age groups and between national borders. The frequency of H. pylori infection is higher in developing nations and environments with limited resources. 2
Helicobacter pylori has been found to play a major etiological and pathological role in chronic gastritis, peptic ulcer disease, and gastric cancer, its importance for many types of additional gastric disease needs to be further investigated. 3 H. pylori infection is mainly acquired during childhood and may persist throughout life and its prevalence is found to be high in developing countries; this is related to low socioeconomic status, overcrowding, poor housing, poor sanitation, and unclean water supply and Intestinal parasitic infections. 4
In general, developing nations have a higher rate of infection than industrialized nations.1,5 The pooled prevalence of H. pylori infection was highest in Africa (70.1%) and lowest in Oceania (24.4%). The frequency of H pylori infection differs significantly between nations, ranging from 18.9% in Switzerland to 87.7% in Nigeria.6,7 In poor countries, H. pylori infections were associated with 60–90% of stomach ulcers and 90–100% of duodenal ulcers, respectively. 8
In Ethiopia, Helicobacter pylori infection remains a significant public health issue. It is still widespread.5,9 Caretakers and medical professionals can prevent most negative effects and effectively manage their patients by evaluating the trends of Pylori infection. Additionally, policymakers can use our findings as a guide and source of information when planning and implementing an intervention program for controlling programs. The purpose of this study was to determine trends and prevalence in five consecutive years at The Bule Hora University Teaching Hospital because currently no studies are being carried out on trends in H. pylori infection in serial years.
Method and Materials
Study Setting, Design, and Study Population
An institutional-based retrospective study was conducted at Bule Hora University Teaching Hospital, West Guji, Ethiopia, on January 20, 2023. The city of Bule Hora is located 475 km from the capital Addis Ababa in the West Guji Zone of the Oromia region. Bule Hora University teaching hospital was established in 1998. Today, the hospital provides a healthcare service for more than 1.3 million people in the population of the area around the town of Bule Hora and the neighboring provinces of the SNNP Regional State. The hospital provides services including emergency, outpatient, inpatient, internal medicine, gynecology and obstetrics, pediatrics, maternal and child health (MCH), TB and HIV (TB/HIV), mental health care, dermatology and includes follow-up for chronic diseases, such as DM and hypertension, pharmacy and different laboratory services, and others.
Data Selection Criteria
Patients who were tested for H. pylori infection and had complete data in the hospital before 5 years were included in the study. However, the inconclusive test results were excluded from the study.
Sample Size and Sampling Techniques
The sample size was calculated using a single-population proportion formula ((n) = (Ζα/2)2pq/d2) and a correction formula for a finite population (n = n/1 + n/N). Then, the final sample size was 314. To enroll, the data met the criteria: first, the total number of completed patient data was gathered, which was 3926. The total recorded data was allocated proportionately to five years. Therefore, the total patient data of the study period (3926) was divided by the sample size (314) to obtain the Kth value, which was 12. The data were then extracted at every 12th data in the log book. Finally, the collected data were included in this study using systematic random sampling to obtain the data required for this study.
Data Collection and Quality Assurance
Data were collected by reviewing clinical records of patients tested for H. pylori infection from 2018 to 2022 using a pretested and standardized checklist. Data was collected through an English-version checklist, which was adapted from different reviews of the literature. 6 The age, sex, years, residence, and results of the participant for H. pylori were among the generated data. All H. pylori stool antigen test results were extracted from the medical record. Data quality was ensured during the data collection, recoding, and analysis phases. Before the actual data collection period, a data collection tool was tested on 5% of the entire sample. After the data are collected, it is verified for completeness, accuracy, clarity, and consistency.
Statistical Analysis
For analysis, data were coded, cleaned, entered into Epi Data version 3.1, and analyzed using SPSS version 26 (IBM® SPSS®, IBM Corp., Armonk, NY, USA). Descriptive analysis was performed and the results are presented as numbers and percentages, or means ± SD. Statistical significance was established at p < 0.05.
Ethical Consideration and Consent
This study was approved by the Institutional Ethics Review Committee (IERC) of the Department of Medical Laboratory Sciences, Bule Hora University. Ethical clearance was granted by letter number IERC 076/MLS/2021. Then, the letter of cooperation was sent to Bule Hora University Teaching Hospital. The importance and risk of the study was explained to the head of the BHUTH laboratory unit and the information obtained during the study was kept confidential. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Result
Sociodemographic Characteristics of Study Participants
A total of 314 individual data was included in the study, who attended from January 2018 to December 2022 at Bule Hora University Teaching Hospital, Laboratory Department for Helicobacter pylori infection detection by H. pylori stool antigen test. The mean age was 29.01 (SD ± 4.93). Most of the respondents, 39.2%, were found to be in the age group of 21–30 and most of the participants, 55.4% (n = 174), were women. (Table 1).
Sociodemographic Characteristics of the Respondents with helicobacter Infection in the University Teaching Hospital of Bule Hora, Bule Hora, Ethiopia, 2022.

Prevalence of H. pylori Infection among Study Subjects at Bule Hora University Teaching Hospital
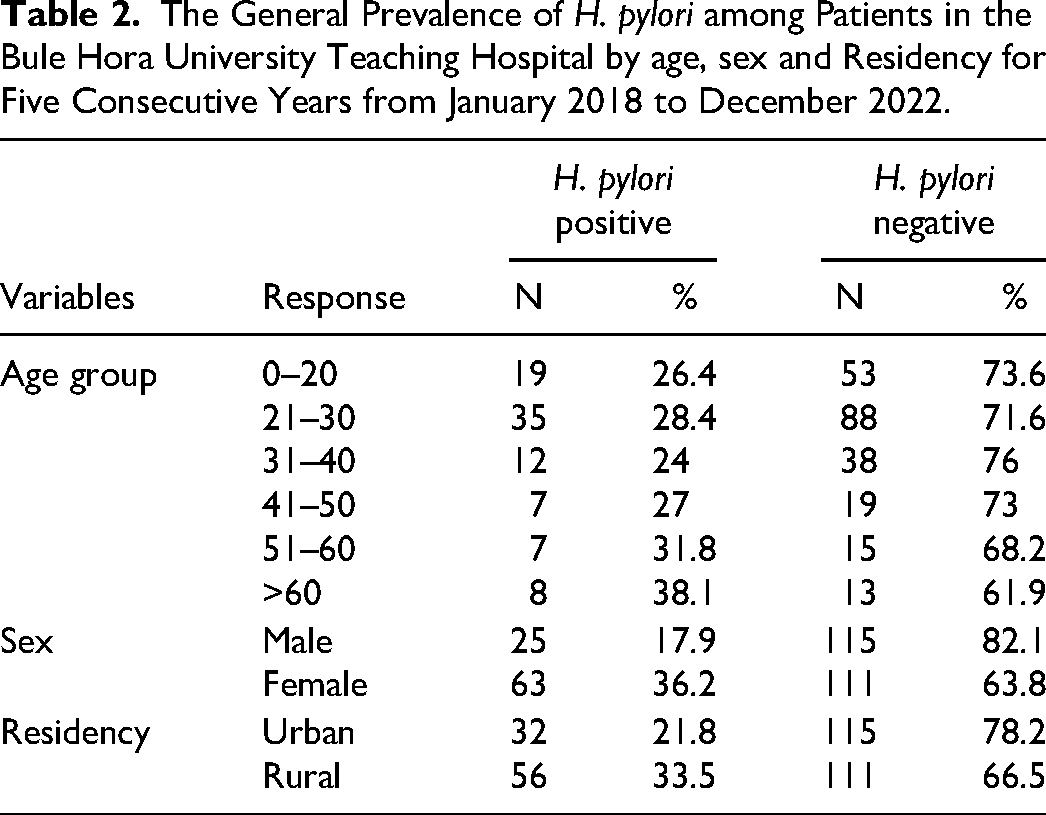
The study participants who were positive for H. pylori were 28% (88) (95% CI, 23-32.9). However, the prevalence by sex was a positive 36% (n = 63) rate in the female participants. Participants in the age category over 60 years of age were observed with the highest positivity of H. pylori with 38.1%, while in the age category of 31–40 were the lowest positivity with 24%. Regarding the residence of the patient data, higher proportions of H. pylori infection were found among rural residents with 33.5% (n = 56) (Table 2 and Figure 1).

The overall prevalence of H. pylori among different age categories of patients in Bule Hora Teaching Hospital for five consecutive years (2018–2022).
The General Prevalence of H. pylori among Patients in the Bule Hora University Teaching Hospital by age, sex and Residency for Five Consecutive Years from January 2018 to December 2022.
Proportion of Patient Data Within Study Years
Of the total 314 data, H. pylori test results found in Bule Hora University Teaching Hospital included in the study; 19.7% (n = 62), 15.9% (n = 50), 17.8% (n = 56), 22.9% (n = 72) and 23.6% (n = 74), from 2018, 2019, 2020, 2021 and 2022, respectively. Therefore, the highest proportion of H. pylori test results recorded data was in 2022 (23.6%) and the lowest in 2019 (15.9%) (Figure 2).

Proportion of patient data within study years in Bulehora University Teaching Hospital from January 2018 to December 2022.
Trends in H. pylori Prevalence
The study shows that the trends of the prevalence of H. pylori infection fluctuated in 5 years. It was lower in 2018 with 25.8%, increased to 39.2% in 2019, then decreased slightly to 33.9% and 16.7% in 2020 and 2021, respectively, before slightly increasing 28.4% (Figure 3).

Graphical presentation of year-based trends of H. pylori infection over the last five years (2018–2022) at the Bule Hora University Teaching Hospital, Bule hora, Ethiopia.
In this study, out of the total H. pylori positive patients, 28.4% (n = 25) were male patients and 71.6% (n = 63) were female. Therefore, the prevalence of H. pylori infection among female patients was higher compared to that of male patients (Table 3).
Sex-Specific Trends of H. pylori Prevalence in the Last Five Years (2018–2022) at Bule Hora University Teaching Hospital, Bule Hora, Ethiopia, 2022.

Discussion
The overall prevalence of H. pylori observed in this study is 28% (95% CI 23-32.9). This finding was consistent with the study conducted in turkey. 10 However, the finding is lower than the findings of studies conducted at Gondar University (65.7%), Iran (35%), and Nigeria (93.6%).11–13 A possible reason for this variation might be the sample size. The sample size to determine Helicobacter pylori training used in this study was small, but the sample size used in those studies was large. The other possible reason for this discrepancy might also be due to study years. In this study, the previous 5-year data were used, but in those studies only 3-year data were used.
Contrary to this, the study finding is higher (14.6%) compared to a study conducted in Addis Ababa. A possible reason for this gap may be a lack of health education regarding H. pylori.
In this study, the trend of Helicobacter pylori fluctuates year to year compared to other studies, in those studies the helicobacter trend has increased year to year regularly. 8 In this study, the prevalence of H. pylori infection in the age group 41–50 and 51–60 years was very low (8%); compared to the study conducted in the Arada sub city which was reported 59%,. 8 The difference may be related to the health-seeking behavior of the old-age patients, and lifestyle could also contribute to their difference.
In this study, infection was significantly higher among younger ages, which is nearly consistent with other investigations. 14 This may be due to the fact that the H. pylori bacterium is acquired in childhood, especially when one of the family members becomes infected with this bacterium and then transmits it to others at an early age because of sharing food tools, and it can last for life.
In this study, in contrast to other studies conducted in southern Ethiopia, the prevalence of Helicobacter infection is high among women than men. 13
In the present finding, the prevalence of Helicobacter infection is higher among rural residents, this is almost in line with the finding of other study which is conducted in Iraq. 12
Conclusions and Recommendations
The overall prevalence of H. pylori was 28%. The study implies that the prevalence of H. pylori infection varied from 2018 to 2022. The prevalence of H. pylori was higher in the age group 21–30 years than in other age groups, and the prevalence continued to increase yearly. The trend of Helicobacter infection increases year over year; therefore, hospitals and clinical cares should evaluate the validity of test tools and testing across younger populations to eradicate infections earlier. The health offices should provide and promote continuing health education for rural residents, since there is a higher prevalence of Helicobacter infection in this community. Finally, researchers should conduct large-scale studies to evaluate H. pylori infection in terms of sex and age specificity.
Footnotes
Lists of Acronyms and Abbreviations
Acknowledgments
We would like to thank Bule Hora University teaching Hospital staff, especially data collectors and laboratory staff, for their valuable contributions.
Authors’ Contributions
All authors involved in conceptualization, proposal development, project management, research and monitoring, data analysis, supervise, the data collection process, performed, document preparation, interpretation, wrote, and manuscript preparation. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data Availability
All required datasets from which the conclusions of the findings concluded are included in the manuscript.