
Abstract
Background:
Healthcare workers face a significant risk of sharp and needle-stick injuries, which can increase the likelihood of spreading illnesses like hepatitis B, hepatitis C, and HIV. Currently, there is no available information on the prevalence or contributing factors of needle sticks and sharp injuries (NSSI) in hospitals in southern Ethiopia.
Objective:
This study aimed to assess the needle sticks and sharp injuries among health care workers at the BHUTH, Southern Ethiopia.
Methods:
The study was a cross-sectional study conducted at an institution in October 2023, with 164 randomly selected participants. A self-administered questionnaire was used to gather information on sociodemographic factors and exposure status. The data was entered and analyzed using Epi-Data and SPSS. The risk factors were identified by binary and multivariate logistic regression analyses. A P-value less than .05 was considered statistical significance.
Result:
The overall prevalence of at least one Needle sticks and sharp injuries in the last 12 months was 46.4% (95% CI of 39.3% to 53.6%). The majority of injuries 45.8% were due to the syringe needle. Factors such as needle recap (AOR = 3.73, 95% CI: 1.07-12.19), Recapping with two hands (AOR = 2.78, 95% CI: 1.36-10.02), working 40 hours per week (AOR = 2.18, 95% CI: 0.98-6.86), and lack of training in occupational safety practices (AOR = 4.01, 95% CI: 2.60-9.91), were factors significantly associated with the prevalence of needle stick and sharp injuries.
Conclusions:
This study found that nearly half of the respondents experienced a sharp needle poke and injury at least once in the previous year; however, the volume of NSSI remains high in the study area. Healthcare workers should receive on-the-job training, and hospital executives should set aside time for discussions on how to solve the problem.
Introduction
A needlestick and sharps injuries (NSSI) happen when a needle or another sharp object pierces the skin after being in contact with blood or other bodily fluids. 1 The risk of needle stick and sharp injuries at work is increased when employees do not have access to the appropriate personal protective equipment or when they do not use the equipment given. 2 Healthcare professionals often sustain needlesticks and sharps injuries, putting them at risk of contracting bloodborne infections such as HIV, Hepatitis B virus (HBV), or Hepatitis C virus (HCV), which can be fatal or seriously threaten their health. 3
Several dangerous infections can be spread through sharp objects and needle sticks; Healthcare workers may be exposed to more than 30 recognized hazardous bloodborne pathogens due to needlestick and sharps injuries. 3 Hospitals are dynamic environments with a wide range of ongoing activities at all levels of organization, execution, and results. 4 Globally, about 3 million healthcare workers are exposed to blood-borne pathogens through needlestick injuries each year. Of these, 2 million are infected with HBV, 0.9 million with HCV, and 170 000 with HIV, according to the World Health Organization. More than 90% of these infections occur in developing countries. 5 According to a study, developing nations account for almost 90% of NSSI-related infections. 6
The estimated number of needle sticks and sharp injuries in the UK alone is 100 000 per year. 7 According to a German survey, 31.4% of healthcare professionals experienced at least one needle stick or sharp injury in a given year. 8 The limited resources and infrastructure, inadequate personal protective equipment (PPE), and the strain on healthcare professionals contribute to a heightened risk of needle sticks and sharp injuries in African countries, surpassing the global average. This represents a significant public health issue. 9
A study in Addis Ababa, the capital of Ethiopia, revealed that 66.6% of healthcare workers have experienced unintentional needlesticks and sharp injuries. Despite the distribution of personal protective equipment and safety guidelines, as well as training provided by the Ethiopian Ministry of Health, needlestick and sharp injuries (NSSIs) continue to be reported. This persistent issue may stem from the absence of a systematic reporting system, leading to a poor understanding of the prevalence of needlestick injuries and their associated risk factors in Ethiopia. Therefore, this study aimed to determine the prevalence of needle sticks and sharp injuries and the factors associated with them among health professionals at Bule Hora Teaching Hospital in the West Guji Zone of Oromia, Ethiopia.
Methods and Materials
Study area and study period
The study took place at the Bule Hora University Teaching Hospital, located in the city of Bule Hora, which serves as the capital of the West Guji zone. The city is situated 467 km south of Addis Ababa, with coordinates of 5°35′ latitude and 38°15′ longitude. Bule Hora has 8 kebeles, housing 1 governmental hospital, 1 health center, and 8 health posts. BHUTH was established in 1998 and is the largest hospital in the West Guji Zone, providing healthcare services to over 1.3 million people in the region. It functions as a teaching, training, and clinical service center and employs 272 health workers and 255 administrative staff.10,11 The study was carried out from the 1st to the 30th of October, 2023.
Study design and population
A facility-based cross-sectional study was carried out among health workers at Bule Hora University Teaching Hospital.
Inclusion and exclusion criteria
The study included all health workers working in BHUTH who were available at the time of data collection, excluding those whose activities do not expose them to needle injuries.
Sample size determination
The sample size for prevalence was calculated using a single population proportion formula, with the following assumptions: a prevalence of needle sticks and sharp injuries of 31% among healthcare workers at Addis Abeba Hospital, 12 a 95% confidence interval, and a 5% error margin. This resulted in a sample size of 329. Since the total population is less than 10 000, the correction formula was used, and the final sample size for this study was 164 after adding 10% for the non-response rate.
Sampling technique
A stratified random sampling approach was used in the selection of study participants. First, we created six strata based on the occupation of the sample. Then, a proportionate allocation to the strata was used to calculate the necessary sample size for each stratum. Finally, the study participants were randomly selected from each occupational stratum using the lottery method (Figure 1).

Proportionate stratified sampling pocedures of HCW in BHUTH.
Data collection and laboratory processing
Data were collected from healthcare workers who were selected using a pre-tested structured self-administered questionnaire. Data were collected by expert data collectors. The questionnaire included sociodemographic factors such as age, sex, profession, level of education, years of service, hours worked per week, night shifts, needle recapping, availability of personal protective equipment ((PPE) eg, gown, shoes, gloves, mask, face shields, etc.), presence of safety instructions, and suggestions for reporting. Data was collected from health professionals who consented to participate in data collection.
Quality assurance
After being first written in English, the structured questionnaire was translated into Amharic and Afan Oromo. The questionnaire was pre-tested and revised prior to real data collection. Before data processing, the investigators confirmed the accuracy and consistency of the data. The quality of the data and the procedures used to obtain them were evaluated.
Data analysis
Data were exported from Epidata version 3.1 and then coded, cleaned, and analyzed using SPSS software version 25. We calculate means, standard deviations, percentages, and frequencies to describe the study population in relation to relevant factors. To assess the association between dependent and independent variables, we used binary logistic regression analysis. We performed multivariate analysis on bivariate analysis variables with P-values less than .25 to identify independent causes. The stepwise backward method was applied to multivariable analyses. We reported the strength of the link using the adjusted odds ratio (AOR) and considered significance for P-values less than .05.
Results
Sociodemographic characteristics of the study participants
Of the total 164 selected participants, 154 of them voluntarily responded fully to the self-administered questionnaire, resulting in a response rate of 95.2%. The mean age of the study participants was 35.47 years, with a standard deviation of ±6.55. The majority of the participants 79 (51.3%) were in the age group of 25 to 34 years. Of the total study participants, 74% (114) had a degree or higher qualification, and of the study participants, 51.9% were nurses (Table 1).
Distribution of sociodemographic characteristics of health workers in BHUTH (n = 154) West Guji Zone, 2023.

Of the respondents, 27 (17.5%) were currently working in the medical ward departments. Approximately 86 (55.8%) staff had less than 5 years of work experience, and the majority of study participants 97(62.9%) were not trained in occupational safety. Most of the respondents, 152 (98.7%), used personal protective equipment. The highest proportion, 127 (82.5%) of study participants, worked a night shift (Table 2).
Behavioral/services/prevention practices/environmental characteristics of health care workers in the BHUTH (n = 154) West Guji Zone, 2023.

Prevalence and circumstances of needle stick and sharp injury
This study shows that the prevalence of healthcare workers who encountered needle sticks and sharp injuries in the last 12 months on the job was 72 (46.4%). Among the injuries, 30 (41.7%) were superficial skin injuries without bleeding, 35 (47.2%) were mild skin penetrations with bleeding, and 8 (11.1%) were deep injuries. The majority of the reasons for the last injury, 17 (23.6%), were during waste collection. Approximately 19 (26.4%) of the respondents were exposed to disease after NSSI and approximately 67 (93.1%) received medical care. About 13 (18.1%) of the respondents did not report the injury and the majority of those 9 (69.2%) did so for fear of stigma. Of the injured parts of the body, almost two-thirds (63.9%) were on the finger. Of the type of sharps that caused the injury, most of them 33 (45.8%) were due to a syringe needle. Most of the 28 respondents (38.9%) used laboratory investigations after exposure to NSSI (Table 3).
Circumstances in which needle stick and sharps injury occur among healthcare workers in BHUTH.

Determinant factors for needle injuries among healthcare workers
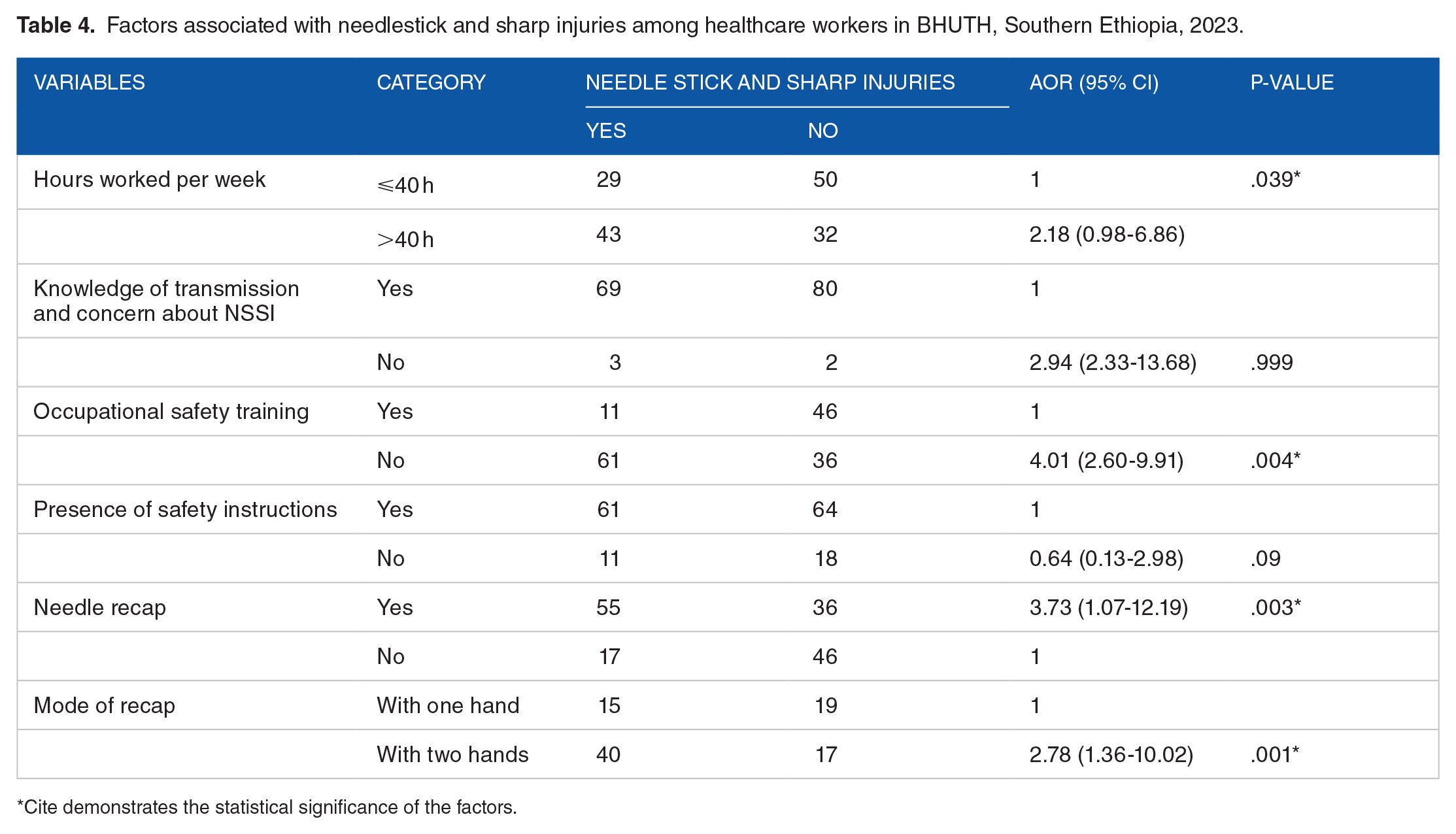
Among the factors examined, the department of work, weekly working hours, occupational safety training, needle recapping after use, and method of recapping were found to be significantly associated with needlestick and sharp injuries. Health workers who worked more than 40 hours per week were twice as likely to be injured compared to those who worked less than 40 hours per week (AOR = 2.18, 95% CI: 0.98-6.86). Health workers who did not receive occupational safety training were 4 times more likely to be injured compared to their counterparts (AOR = 4.01, 95% CI: 2.60-9.91). Participants who recapped needles had almost 4 times greater chance of needle stick injuries compared to those who did not recap needles (AOR = 3.73, 95%CI: 1.07-12.19). Health workers who recapped needles with two hands were nearly three times more likely to be injured with needle sticks compared to those who recapped with one hand (AOR = 2.78, 95% CI: 1.36-10.02) (Table 4).
Factors associated with needlestick and sharp injuries among healthcare workers in BHUTH, Southern Ethiopia, 2023.
Cite demonstrates the statistical significance of the factors.
Discussion
Healthcare workers face occupational health hazards, primarily due to accidental exposure to injuries like needle sticks and sharp materials. 2 Among BHUTH health workers, the prevalence of NSSI was 46.4% (95% CI: 39.3-53.6). This finding aligns with a study conducted in a Ghanaian metropolitan hospital, which reported a prevalence of 47%. 13 This finding was found to be higher than that reported from the Awi zone of the Amhara region 18.7%, 14 Bale 19.1%, 15 Bahir-dar 31.0%, 16 Gonder 30.8%, 3 Hawassa 35.8%. 17 However, the current finding is less than the study conducted in Addis Ababa of 66.6%. 12 The possible reason for the discrepancy may be the level of training received, the availability of safety instructions, and the duration of working hours.
The study indicated that syringe needles were the primary cause of injury at 45.8%, a figure significantly lower than those found in previous research: 77% in Bahir-dar, 16 69.8% in Bale, 15 and 64.5% in Addis Ababa hospitals. 12 This suggests that healthcare workers (HCWs) sustaining injuries from needle-stick and sharps incidents (NSSI) may be linked to improper needle handling. Additionally, the prevalence of procedures requiring syringe needles could increase the risk of injuries among HCWs.
In this study, 4 significant factors are associated with needle sticks and sharp injuries. Participants who practiced needle recapping in the last 12 months were nearly 4 times more likely to experience needle sticks and sharp injuries than those who did not. This finding aligns with a study conducted in Bale which reported that those who practiced needle recapping were 3 times more likely to experience injury than those who did not recap needles after use. 15 Other studies conducted in Northwestern Ethiopia 18 and the Awi zone of Amhara region, 14 reported that workers who recapped needles were more likely to be injured. In the current study, those who recap with 2 hands were approximately 3 times more likely to be injured with a needle stick than those who recap with 1 hand. This finding is similar to studies conducted in Bahir-dar. 16 This may be due to recapping the needle after use, which causes accidental injection of herself/himself while recapping with 2 hands easily injecting one another.
The study found that people who worked more than 40 hours a week were 3 times more likely to engage in NSSI (non-suicidal self-injury) compared to those who worked 40 hours or less. This aligns with a similar study conducted in northern Ethiopia. 18 The increased likelihood of NSSI may be linked to the stress and depression caused by a hectic work environment.
Additionally, the research revealed that health workers who did not receive occupational safety training were 4 times more likely to experience needle stick injuries compared to their trained counterparts. This result aligns with a study from Addis Ababa which found that training is crucial in raising awareness among healthcare workers about the proper use of needles for various procedures. 12
The Limitations of the Study
The sample size was too small, which limits the significance of the study’s findings for generalizing to all health professionals in the population. The study may also be prone to response bias from the participants. Furthermore, the cross-sectional design of the study makes it challenging to establish causal relationships.
Conclusion
The study found that nearly half of the respondents experienced needle sticks and sharp injuries in the last 12 months on the job, indicating a high prevalence of these incidents in the study area. Needle recapping, long work hours per week, and lack of occupational safety training were identified as the main risk factors. Therefore, we recommend policymakers and healthcare planners develop strategies to improve working conditions for healthcare workers and promote adherence to universal precautions. Healthcare workers should receive on-the-job training, and hospital administrators should facilitate discussions on addressing this issue. Further research is necessary to determine the actual incidence of needle-stick injuries and the potential diseases resulting from such exposures.
Footnotes
Acknowledgements
We would like to express our gratitude to Bule Hora University for granting us permission to conduct this research. Additionally, we extend our thanks to the Bule Hora University Teaching Hospital for their support in data collection. Lastly, we are grateful to the participants for their willingness to take part in the study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed significantly to preparing the proposal document, collecting and analyzing data, interpreting the results, critically reviewing the article, and participating in the decision of the important journal to which the article was submitted.
Ethical Approval
The study protocol received approval from the Institutional Review Board (IRB) under reference number IRB09/2023 at Bule Hora University. The approval letter was provided to the Bule Hora University Teaching Hospital prior to data collection. All study participants gave their informed written consent. The information about each study participant was kept private and used solely for research purposes. The data was also treated as confidential.
Consent of Publication
Not applicable.
Data Availability
All required data sets are included in the manuscript based on the conclusion of this article.