
Abstract
Background:
Patient-reported outcomes (PROs) are increasingly recognized in hematology, yet clinician awareness remains limited. In immune thrombocytopenia (ITP), an autoimmune disease, symptoms like fatigue impact quality of life (QoL).
Design and Methods:
This Italian survey evaluated hematologists’ knowledge of PROs within the Italian ITP NET network. Between April 4–20, 2023, 63 hematologists from 49 centers were invited to complete a 63-item online questionnaire on demographics, QoL understanding, and attitudes toward clinical use.
Results:
Thirty-nine responded, treating a median of 50 ITP patients in the prior year. PROs were used in research by 51% and applied clinically by 56%. Greater PRO knowledge was found among hematologists with over 17 years’ experience (72%) and extensive ITP exposure (64%) (p=0.033 and p=0.037). Larger centers reported more trial involvement (p=0.035) and regular QoL tool use.
Conclusion:
Results highlight knowledge gaps and emphasize how clinical experience and exposure support effective PRO implementation in ITP.
Introduction
Immune thrombocytopenia (ITP) is an autoimmune hematological disorder characterized by low platelet counts due to the destruction of platelets by the immune system. 1 The annual incidence and the prevalence of primary ITP in adults have been estimated to be 3.3 per 100,000 and 9.5 per 100,000, respectively, 2 The Orphanet database estimates a prevalence of ITP of 1–5 per 10,000 and an annual incidence of 1 in 25,600–37,000 in Europe. 3 In Italy, recent estimates from 2023 to 2025 are 1,741 patients/national population (∼50 million); that is, equating to 3.5/100,000 individuals. 4 This condition can lead to symptoms such as spontaneous bruising, bleeding, and, in severe cases, life-threatening hemorrhages. 1 While bleeding complications are a hallmark of the disease, ITP also has significant non-bleeding manifestations that negatively affect patients’ quality of life (QoL). 5 Fatigue is one of the most commonly reported symptoms that impact patients with ITP, often underestimated by clinicians despite its profound effects on patients’ daily lives. 5 Other symptoms that affect QoL include anxiety, depression, and headaches. 6 It has also been recently reported that concurrent hypersomnia is also an important, underestimated factor negatively influencing the QoL of patients with ITP. 7
Patient-reported outcomes (PROs), which capture patients’ perspectives on their symptoms and daily functioning, are increasingly used in clinical practice to assess the broader impact of diseases like ITP. 8 Despite their growing recognition, the integration of PROs into routine practice, particularly in hematological diseases, remains inconsistent. Recently, specific barriers to implementing PROs in clinical settings have been highlighted. 9 Furthermore, their role in improving patient management, by linking patient-reported outcome measures (PROMs) scores to care pathways in oncological care leading to improved outcomes in a significant percentage of studies has been documented. 10 PROs can provide a more comprehensive understanding of the burden of ITP beyond traditional clinical measures such as platelet counts. 11
Despite the availability of disease-specific tools, PRO instruments are primarily used in research settings rather than in clinical practice. 8 One of the main reasons why clinicians do not extensively use PROs to assess QoL is the lack of awareness.9,12–15 While PROs are increasingly recognized in international guidelines and research, their use in routine hematological care in Italy remains limited. To date, no study has systematically examined how Italian hematologists, particularly those treating ITP, understand and apply PROs in clinical practice.
This knowledge gap highlights the need for a national survey to assess clinician awareness, identify implementation barriers, and explore how clinical experience and patient volume influence PRO integration.
By focusing on the Italian ITP NET network, this study highlights current practices and challenges in the management of ITP.
This national survey aims to assess the understanding and implementation of PROs among hematologists treating ITP patients within the Italian ITP NET network, with the goal of identifying gaps and opportunities for future educational interventions.
Methods
Study design
From April 4 to 20, 2023, 63 hematologists from 49 Italian centers were invited to complete an online survey hosted on the SurveySparrow platform (SurveySparrow Inc., Palo Alto, CA, USA).
Participants accessed the survey via a unique link provided in the email invitation, with responses collected directly on the platform. Hematologists were selected from centers in the ITP Net network as of March 2023, based on the extent of expertise of each center in managing ITP. A delegate with direct experience in the management of ITP patients was identified to participate. Accordingly, inclusion criteria for this study were: hematologists affiliated with ITP NET centers, actively involved in ITP patient management, and designated by their center director as the clinical lead for participation. Exclusion criteria included physicians not directly involved in ITP care, individuals from non-participating centers, and hematologists who declined or did not complete the survey. The reporting of this study conforms to the CROSS statement 16 (Supplemental Material S1). Written Informed Consent to publish the findings of this study was obtained from all participants as per General Data Protection Regulation (GPDR) prior to survey completion.
Survey
The 63-item survey was developed by a multidisciplinary team with experience in the design and development of PROs within the ITP NET network with input from both hematologists and health outcomes researchers. It was initially developed and then pre-tested and pilot-tested internally among a small sample of hematologists (n = 5) to ensure clarity and relevance. Feedback from this pilot testing was used to refine the final version prior to dissemination. The 63-item survey addressed demographics, professional characteristics, and physicians’ knowledge, attitudes, behaviors, and willingness to use QoL data in ITP clinical practice (Supplemental Material S2). Results presented in the present study focus on a subset of questions, including years of practice (Q1.8), experience in ITP management (Q1.9), patient volume (Q1.11, Q1.12), knowledge of QoL studies (Q2), participation in QoL research (Q4), departmental practices (Q6), and attitudes toward QoL assessments (Q8.1, Q9.5, Q9.10).
This survey was confidential; no personally identifiable information was collected beyond demographic data such as age, gender, and region. All data were rendered anonymous prior to analysis. Since this study involved an anonymous survey among physicians and did not collect personal or health-related data, ethics approval was not required according to Italian national legislation (Legislative Decree n. 101/2018).
Statistical analysis
No formal sample size calculation was performed, as all hematologists from the ITP NET network were invited to participate based on their clinical role and expertise. The sample therefore reflects the full eligible population within the network.
Descriptive data were obtained from questions regarding demographic information and professional profiles of the participants and summarized as mean ± SD, number and percentage, or median and range. Categorical variables were reported as frequencies and percentages.
To assess differences in knowledge and use of QoL assessments across different subgroups of hematologists, for categorical variables chi-square or Fisher’s exact test, were used as appropriate. Categorical variables were compared using chi-square or Fisher’s exact test, as appropriate. For continuous variables, differences between groups were analyzed using the Mann-Whitney U test. The probability of a type I error was set at the 5% level (p ≤ 0.05).
Results
Demographic and professional characteristics of hematologists
Thirty-nine hematologists completed the survey (Table 1). Most respondents were female (n = 28, 72%), with an average age of 44 ± 11 years. The majority of hematologists (54%, n = 21) had ≤17 years of practice, while 72% (n = 28) had over 4 years of experience specifically in management of ITP patients. The median number of years in practice was 15 years (IQR 9–24). Experience in managing ITP patients ranged from 4 to 16 years, with a median of 6 years. Over the past 12 months, hematologists saw a median of 50 ITP patients (IQR 20–150) and treated a median of 40 ITP patients (IQR 20–77) with at least one ITP treatment (Table 1).
Demographic and professional characteristics of surveyed hematologists (n = 39).
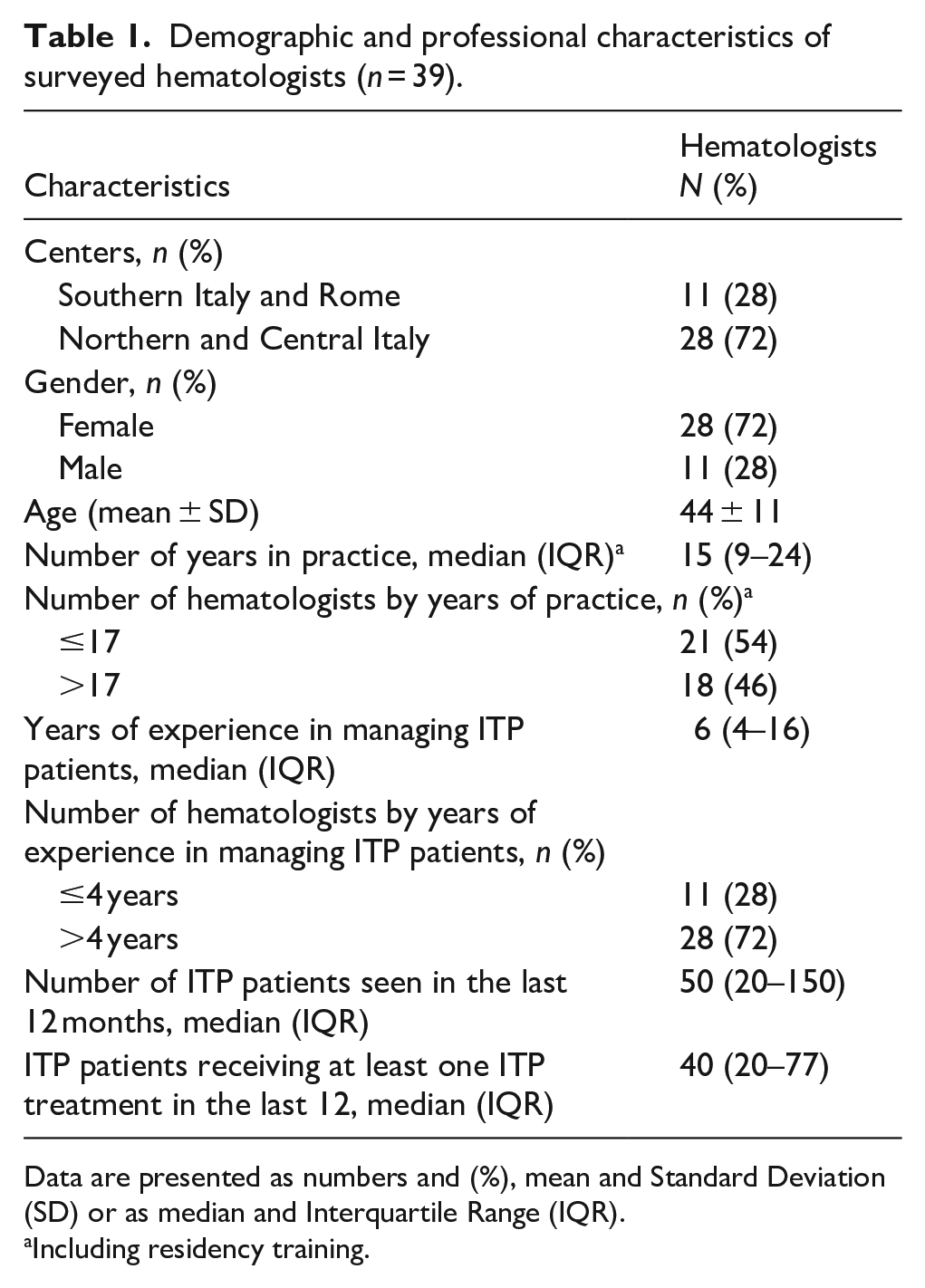
Data are presented as numbers and (%), mean and Standard Deviation (SD) or as median and Interquartile Range (IQR).
Including residency training.
Discrepancy between hematologists’ knowledge and use of QoL assessments
The survey revealed discrepancies between hematologists’ knowledge and use of QoL assessments (Table 2). Regarding their knowledge of QoL studies and trials, 10% (n = 4) reported no knowledge and 36% (n = 14) unspecific knowledge. Among those who were familiar with QoL, 15% (n = 6) reported specific knowledge without research activity. Additionally, 31% (n = 12) reported using QoL assessments for research purposes, and 8% (n = 3) reported using QoL assessments in clinical practice.
Physician’s knowledge of QoL issues (questions 2,4 and 6 of the survey) (n = 39).
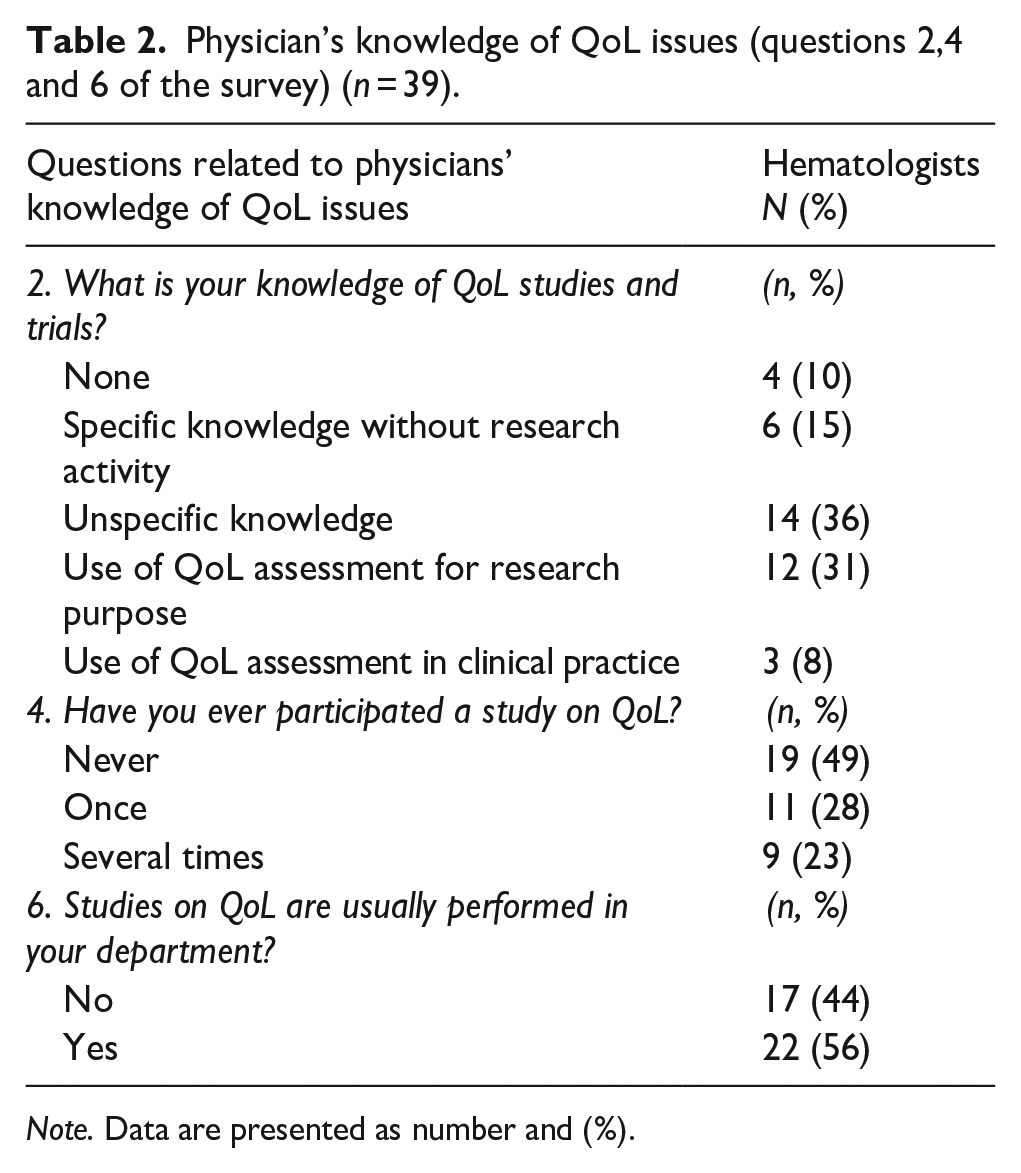
Note. Data are presented as number and (%).
When asked about participation in QoL studies, 49% (n = 19) had never participated, while in the remaining 51%, 28% (n = 11) had participated once, and 23% (n = 9) had participated several times. Just over half (56%; n = 22) of hematologists indicated that QoL studies are routinely performed in their departments. These findings highlight a discrepancy between the knowledge of QoL issues (36%) and the application of QoL assessments.
Factors influencing knowledge and utilization of PROs in ITP clinical practice
Clinicians with more than 17 years of practice demonstrated significantly greater knowledge of PRO studies compared to those with 17 or fewer years of practice (13/18, 72% vs 8/21, 38%; p = 0.033; Figure 1(a)). Similarly, clinicians with more than 4 years of experience specifically in managing ITP patients exhibited higher familiarity with PROs, with 64% (18/28) reporting knowledge compared to 27% (3/11) among those with fewer years of such experience (p = 0.037; Figure 1(b)).
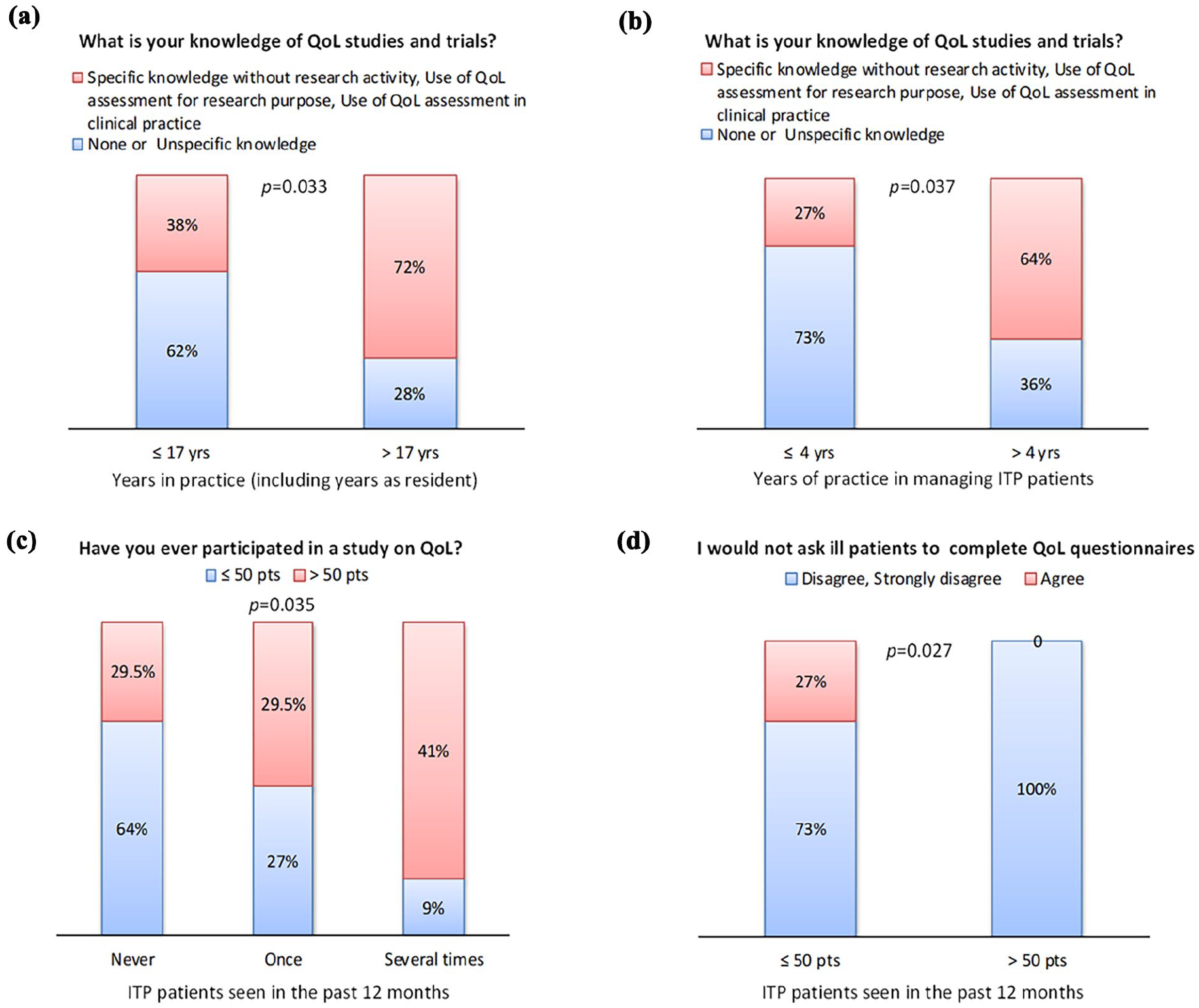
Clinicians’ knowledge and attitudes toward PROs in ITP clinical practice: (a) knowledge of PRO studies by years of clinical practice, (b) knowledge of PRO studies by years of experience with ITP patients, (c) participation in PRO-based clinical trials based on the number of ITP patients treated in the last 12 months, and (d) recognition of PROs’ importance in severely ill patients based on the number of ITP patients treated.
The frequency of ITP patient encounters also influenced engagement with PRO-based trials. Clinicians who saw fewer than 50 ITP patients in the past year were significantly more likely to report no participation in trials on QoL compared to those treating more than 50 patients (14/22, 64% vs 5/17, 29.5%; p = 0.035; Figure 1(c)). Among the latter group, all disagreed with not asking ill patients to complete QoL questionnaires (17/17, 100%), compared to 73% (16/22) of those who saw fewer than 50 patients (p = 0.027; Figure 1(d)). This suggests that clinicians in larger centers routinely propose the use of QoL instruments in clinical practice (Table S1 in Supplemental Material 1).
Most clinicians stated they would be more inclined to use QoL data if it were easier to understand.
Discussion
Despite the growing recognition of PROs as critical tools for assessing QoL, their adoption remains inconsistent. This national survey provides valuable insights into the knowledge and use of PROs in the management of ITP patients. The survey revealed significant gaps in QoL understanding among hematologists, with about half reporting limited or no knowledge and a third using QoL assessments in research. Participation in QoL studies was uneven, with about half indicating routine departmental involvement. Furthermore, our findings revealed that experienced clinicians and larger ITP centers more frequently integrate QoL tools into practice.
Limited awareness among clinicians and patients regarding PROs and their potential impact on care quality has been identified as a significant barrier to integrating PROs into clinical practice.9,12–15 In our study, about half of the hematologists (10% reported no knowledge, and 36% had only unspecific knowledge of PROs) lacked in-depth familiarity with these tools. This highlights that PRO knowledge remains insufficient among hematologists. Similarly, a study exploring hospital physicians’ familiarity with QoL assessments found that less than two-thirds had any experience with QoL evaluation in oncology. 17
Regarding the use of PROs, about half (51%) of the hematologists in our study reported employing them in research while 56% indicated that QoL studies were regularly conducted in their departments. This aligns with reports emphasizing the growing recognition of PROs as valuable tools for improving healthcare quality and promoting patient-centered care. 18 Similarly, an Italian study found that only 30% of physicians reported that at least one QoL study had been conducted in their department, and 23% had participated in such studies. 17
Our data also reveal discrepancies between knowledge and practice. Among the 36% of hematologists who declared a lack of specific knowledge, some had nevertheless used PROMs in research, suggesting that practice is not solely knowledge-driven. The adoption of PROs is increasingly accepted across various clinical settings, 19 likely because many healthcare workflows include predefined care pathways where PRO use is integrated as standard practice. This allows hematologists to utilize these tools without requiring an in-depth understanding of their principles.
Moreover, technological advancements, such as increased internet access, the widespread availability of smartphones and tablets, and electronic health records, have facilitated PRO implementation by streamlining communication and data collection.19,20
Our findings that clinicians with more years of experience had greater knowledge and were more likely to use QoL tools highlight the importance of professional expertise. Limited awareness and the perception of low value are more prevalent among less experienced clinicians, who may fail to recognize the utility of PROMs in improving care. Multiple reviews consistently report that insufficient awareness of PROMs hampers their implementation12,13,21 and that improved education and training are key to enabling their successful adoption.9,15,22
A notable finding from this study is the higher participation in QoL studies among larger centers, which may be attributed to greater resource availability. Larger centers typically have more staff, infrastructure, and access to research funding, enabling more consistent engagement with QoL studies. Addressing resource constraints in smaller centers through targeted support could foster broader participation and engagement. 9
Another significant result of this study is the increased use of QoL tools among clinicians managing a greater number of ITP patients. Repeated exposure to these tools likely fosters familiarity, facilitating their integration into routine care pathways. Clinicians who treat higher volumes of ITP patients are more accustomed to incorporating QoL assessments into their workflows, promoting their sustained use. Studies frequently cite insufficient resources, including lack of time and personnel, as significant obstacles to integrating PROs into routine clinical practice.15,22 Investment in health information technology, such as electronic databases, web-based platforms, and smartphone applications, has been identified as a key enabler, as these tools reduce the workload for clinicians and administrators.9,14 In addition, adequate administrative support for patients and clinicians, as well as statistical resources for analyzing PROMs data, are frequently cited as essential for successful implementation.14,23
The increased use of QoL tools among clinicians managing a greater number of ITP patients highlights the importance of repeated exposure and integration into care pathways. Reviews emphasize that when the burden of PROs falls on a small number of staff, it may lead to burnout and stress.12,14,24 Embedding PROs into clinical workflows and utilizing digital tools could facilitate their adoption. As highlighted in the Anderson et al. umbrella review, 9 integrating PROs into routine clinical processes is an effective means to develop their widespread use.
Our data show that PROM use in clinical practice is limited, with only 3 out of 39 respondents (8%) reporting routine application. Lack of awareness and infrastructure are major barriers. Failure to incorporate PROMs can result in the under-detection of issues like fatigue, anxiety, and psychosocial burden, symptoms that significantly affect ITP patients’ QoL and functioning, such as work, study and other activities, which ultimately may have a “social cost,” but are not routinely captured by standard clinical metrics. 18 As a result, treatment decisions may not fully align with patient needs or preferences, potentially compromising outcomes and satisfaction. Including PROMs promotes shared decision-making, enhances patient–clinician communication, and supports more personalized care.
Based on the results of our survey, several steps can be taken to improve awareness and understanding of PROMs among hematologists. Many respondents, especially those with fewer years of experience or working in smaller centers, reported limited knowledge and less frequent use of PROMs. To address this, we recommend targeted training programs that explain how PROMs can support patient care, particularly for clinicians who have less experience in the management of ITP. Our findings also suggest that some clinicians find PROM data difficult to interpret. In this regard, it is important to note that, in clinical practice, the application of algorithms to calculate summary scores of PROMs is less useful than focusing on the single items that communicate details of patient’s issues (impact of disease and treatment and symptoms). To address summary scores, used more frequently in research, the development of simple, user-friendly tools to display this information would be helpful. Investing in digital tools, such as electronic health records may help support PROM use in smaller settings and help integrate them into everyday clinical practice.
Study limitations
This study has several limitations. First, the response rate was 62% (39 out of 63 invited hematologists), which may introduce selection bias. It is possible that respondents may be more interested or experienced in QoL-related issues than non-respondents, potentially influencing the apparent level of knowledge. Second, the survey relied on self-reporting, which is subject to social desirability bias and recall inaccuracies. Third, the cross-sectional nature of the survey precludes assessment of temporal trends or causal relationships. Last, a formal sample size calculation was not conducted, which may limit the generalizability of findings beyond hematologists within the ITP NET network and may not reflect broader Italian or European practices.
Conclusions
This study highlights the gap in clinician awareness and use of PROs in managing ITP. While PROs are increasingly recognized as essential tools for assessing QoL, our survey found inconsistent knowledge and application among hematologists. It is important to highlight that even without extensive PRO knowledge, clinicians are using these tools through established patient pathways, where PROs are integrated into routine care. This highlights the potential for system-level QoL assessments, independent of clinician expertise. Targeted education is needed to enhance PRO awareness, particularly among hematologists in smaller centers or with less ITP experience. By promoting knowledge-sharing and providing necessary resources, broader PRO integration can improve the quality of life for ITP patients.
Supplemental Material
sj-docx-2-phj-10.1177_22799036251361377 – Supplemental material for Clinician’s knowledge and awareness of patient-reported outcomes in immune thrombocytopenia: Results of a national survey (ITP NET, GIMEMA Working Group Anemia and Thrombocytopenia)
Supplemental material, sj-docx-2-phj-10.1177_22799036251361377 for Clinician’s knowledge and awareness of patient-reported outcomes in immune thrombocytopenia: Results of a national survey (ITP NET, GIMEMA Working Group Anemia and Thrombocytopenia) by Esther Natalie Oliva, Fabio Efficace, Maria Rosa Valvano, Paola Arcuri, Roberta Battistini, Elisa Buzzatti, Cristina Clissa, Cristina Danesin, Alessia Salemme, Francesco Sparano, Francesco Ramundo, Ugo Consoli and Federico Chiurazzi in Journal of Public Health Research
Supplemental Material
sj-pdf-1-phj-10.1177_22799036251361377 – Supplemental material for Clinician’s knowledge and awareness of patient-reported outcomes in immune thrombocytopenia: Results of a national survey (ITP NET, GIMEMA Working Group Anemia and Thrombocytopenia)
Supplemental material, sj-pdf-1-phj-10.1177_22799036251361377 for Clinician’s knowledge and awareness of patient-reported outcomes in immune thrombocytopenia: Results of a national survey (ITP NET, GIMEMA Working Group Anemia and Thrombocytopenia) by Esther Natalie Oliva, Fabio Efficace, Maria Rosa Valvano, Paola Arcuri, Roberta Battistini, Elisa Buzzatti, Cristina Clissa, Cristina Danesin, Alessia Salemme, Francesco Sparano, Francesco Ramundo, Ugo Consoli and Federico Chiurazzi in Journal of Public Health Research
Footnotes
Acknowledgements
We thank all the participants in the ITP NET, Italy and Mattioli Health, Italy, for supporting the study. Medical writing support was provided by Colin Gerard Egan (CE Medical Writing SRLS, Pisa, Italy).
Ethical considerations
This study did not require Ethics Committee approval. This was an online survey. Hematologists were informed of the research and freely agreed to participate in the study, and signed an informed consent. All personal data was blinded to protect clinicians’ privacy. The database did not contain sensitive data, according to the data protection law (Legislative Decree n. 101/2018).
Consent for publication
Informed consent to publish the findings of this study was obtained from all participants as per General Data Protection Regulation (GPDR) prior to survey completion. Participation was voluntary, and no identifying data were collected. Consent was implied in the submission of the completed survey.
Author contributions
ENO, FE, MRV, PA, RB, EB, CC, CD, AS, FS, FR, UC and FC participated in the conception, design, and implementation of the study. ENO, FE, MRV, PA, RB, EB, CC, CD, AS, FS, FR, UC, and FC were involved in the interpretation of the analyzed data, review of the draft manuscript and the decision to submit for publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ENO received fees for Consultancy and Honoraria from Daiichi Sankyo, Consultancy, fees for Honoraria and Speakers Bureau from Bristol Myers Squibb, Alexion, Sobi, Amgen and Novartis, Consultancy, Honoraria and Patents & Royalties from Ryvu, Patents & Royalties from Halia Therapeutics and Speakers Bureau from Jannsen. FE received consultancy fees for Incyte, AbbVie, Novartis, and Jazz Pharmaceuticals. All other authors have no financial interest to declare.
Data availability statement
All results are reported in the present manuscript. Additional supporting data can be made available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.