
Abstract
Highlights
Communication and interaction are the fundamental goals of patient involvement in practice, regardless of which patient involvement intervention is being used.
Clinical reasoning is often an unconscious process using tacit knowledge, but the use of patient involvement interventions may be a way for health care professionals (at both individual and group levels) to become more explicit about and aware of their reflections.
Clinical reasoning can be viewed as a mechanism of change in the development and implementation of patient involvement interventions.
Keywords
This study investigates the current use of patient involvement interventions (PII) by health care professionals when delivering care across several departments in a large university hospital in Denmark. PII are designed to innovate people’s use and experience of health care through the implementation of practices aimed at enhancing people’s health literacy, shared decision making (SDM), and self-management support (SMS).1–3 These types of interventions have several components to target 1) the knowledge, skills, and actions of multiple stakeholders making decisions in health care; 2) the interaction and communication points between stakeholders; and 3) the service infrastructure and system pathways (see Figure 1). For example, SDM interventions include patient decision aids (PDAs) to enhance reasoning, training enabling health professionals to support people’s informed decision making between options, and resources to integrate components in the care pathway; SMS interventions include resources enabling people to cope and manage illness at home, patient-reported outcome measures (PROM) for use in consultations, and training enhancing health professionals’ person-centered care and communication skills. Research illustrates that the integration of PII within clinical practice increases patient knowledge and engagement with health care, reduces decision regret, and affects outcomes such as quality of life, health literacy, experience of care, and use of services.4–6
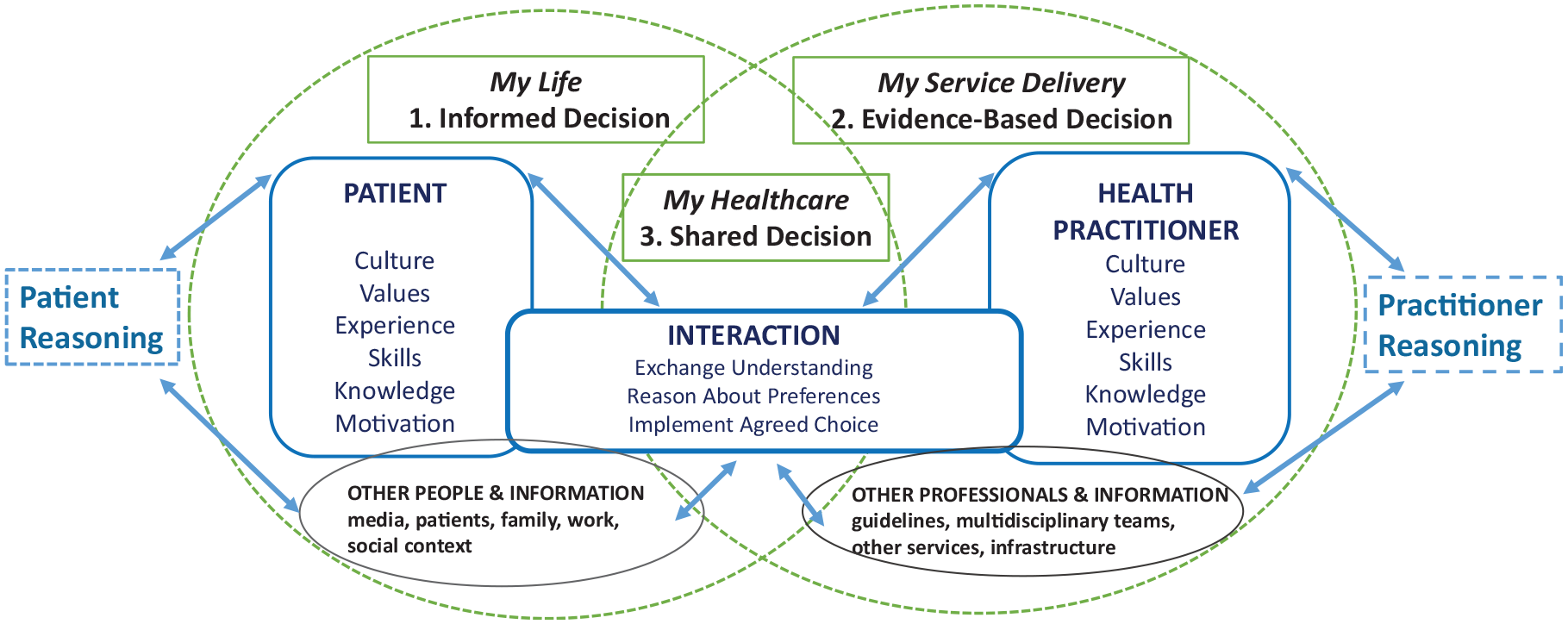
Making Informed Decisions Individually and Together (MIND-IT) in health care: multiple stakeholder decision makers’ intervention framework.
There is variation in the adoption of PII within health services.7–10 Unpacking health professionals’ views toward PII and understanding why and when health care professionals use them in everyday practice are key to understanding this variation.11,12 Although health care professionals recognize the value of PII for patients, there is less research exploring how the use of PII affects their clinical reasoning. Clinical reasoning is the cognitive process health care professionals engage in when managing a clinical problem concerning a patient.13,14 Clinical reasoning is used interchangeably with terms such as clinical decision making, diagnostic reasoning, clinical judgment, critical thinking, or problem solving.15–17 Health care professionals’ clinical reasoning draws on both intuitive and analytic processes and includes gathering and interpretation of patient data, retrieval of experiences, tacit knowledge about care, treatments and service delivery, an action or intervention, and a final evaluation of the care or treatment provided. 14 Health care professionals involve patients’ perspectives at different stages of this problem-solving cycle.14,18 However, there is little research understanding whether PII support health care professionals’ awareness of the patient perspective and how this is integrated within their clinical reasoning.
In Denmark, the User-Involving Hospital project at Aarhus University Hospital (AUH) has developed, evaluated, and implemented several PII since 2014.19–21 An initial survey found that health professionals’ views toward involving patients in care and treatment significant improved after these implementation initiatives. 21 Barriers for adoption of the PII focus on contextual and patient-related aspects but not directly on the health care professionals. A more recent interview study with health care professionals from AUH identified that a combination of top-down and bottom-up approaches, establishment of multidisciplinary teams, and information sharing with colleagues, support from managers, skill-building courses, and insights into the patient perspective were associated with the implementation of PII in their clinical contexts. 19 Missing from these evaluations is evidence of what health professionals consider to be PII and why or how they are used to support their clinical reasoning. Unless these mechanisms are understood, it is unlikely that PII interventions will be adopted by health care professionals consistently in their delivery of health care. 22
The aim of this study was to investigate health professionals’ use of PII in their everyday practice. We defined PII as any method and tool health professionals employ to involve patients in their care and treatment and enhance their patient-centered care and communication. 1 We draw on components within SDM, PROM, PDAs, SMS, and patient-centered communication to guide our questions and prompt professionals to explain how the interventions affected their clinical decision making and delivery of care. The study objectives were to:
map the PII used by health care professionals across clinical settings,
explore health care professionals’ views toward the value of PII impact to patients, and
describe how health professionals’ views about PII are associated with their clinical reasoning.
Design
This study was informed by 2 frameworks guiding intervention development, implementation, and evaluation in health care: the Medical Research Council’s (MRC’s) framework 23 for developing and evaluating complex interventions (methodological) and the Making Informed Decisions Individually and Together (MIND-IT) framework for multiple stakeholder decision-maker interventions (theoretical).1,24 We used MIND-IT (Figure 1) to provide a structure in identifying the roles, goals, values, skills, and knowledge of health care professionals when making health care decisions about, and with, patients in their service delivery context and understanding when and why PII tools and methods are integrated in practice.
The study was a mixed-methods study guided by Creswell. 25 We were guided by the exploratory sequential mixed-methods design. 25 This method included several steps as illustrated in Table 1. Integration of qualitative and quantitative data occurred at 2 points: 1) the themes that emerged during the inductive analysis were used to revise the preliminary survey, and 2) data from the survey and interviews were brought together during the final deductive analysis. This integration ensured that knowledge from the qualitative interviews was embedded in the process of developing the survey, which supported its relevance for the specific context. Also, the deductive analysis enabled an interpretation of the quantitative data, which otherwise would have been vague. The Good Reporting of a Mixed Methods Study (GRAMMS) checklist was used for the reporting of the study. 26
Mixed-Methods Study Design

PII, patient involvement interventions.
Setting and Population
The study was conducted at AUH, a large hospital in the Central Region of Denmark with patients from all medical and surgical specialties. All patient pathways (acute, nonacute, outpatient clinics, etc.) and all ages (from birth to geriatric) are represented in the hospital setting. Approximately 8,500 health care professionals are employed at AUH (somatic and psychiatric departments), including medical doctors, psychologists, social workers, nurses, midwives, medical secretaries, and allied health professionals (e.g., physiotherapists and occupational therapists, dietitians, medical laboratory technicians, and radiographers), from those in training to experts. All qualified medical doctors, nurses, midwives, dietitians, physiotherapists, and occupational therapists with direct contact with patients during daily care and treatment were eligible to participate in this study. Managers, researchers, and other health care professionals who did not have daily patient contact, and students, were excluded.
Data Collection
Qualitative data were collected using semistructured interviews 27 between April and June 2022. Participants were recruited via the authors’ network at the hospital. Colleagues were informed of the study purpose and inclusion criteria and asked to forward the study invitation to others with an interest in PII. Those who expressed an interest in participating contacted AH and were assessed for study eligibility using an interview sampling matrix. The aim was to recruit a broad group of health care professionals with different levels of experience, from different departments and across varied professions, making the recruitment procedure purposeful. A.H., who conducted the interview, did not know any of the informants prior to the interview. The interview guide was designed with 2 purposes: 1) to explore participant experiences of patient involvement in practice, use of PII, and views on the association between PII and clinical reasoning and 2) to give feedback on the preliminary questionnaire content and structure. The interview guide was pilot tested; no changes were made to the questions. Interviews were audio recorded and transcribed verbatim. No new colleagues were approached to take part in the interview study at the point where interviewees gave descriptions of their perspective that was replicating the perspectives of preceding participants.
Quantitative data were collected via an online survey. The survey content was informed by the themes that emerged on basis of the interview findings, prior research,1,19–21 theory explaining clinical reasoning, 14 and items from a previous questionnaire concerning patient involvement sent out via the Danish nurses’ organization and the Danish medical doctors’ association in 2014. 28 Questionnaire responses were either multiple choice or items rated on a 5-point Likert scale ranging from strongly agree to strongly disagree, with a possible “do not know” option. The questionnaire included brief descriptions of the survey purpose and type of interventions of interest; the survey did not explore views on clinical decision support such as algorithms, flowcharts, and guidelines.
As illustrated in Table 1, a preliminary questionnaire was designed and adjusted following analysis of the feedback of 12 interviewees. The revision of the survey included alterations in structure and variables. Afterward, it was pilot tested and adjusted for clarity and minor spelling or grammatical errors. Pilot testing was performed by 10 health care professionals who had a mean completion time of 8 min.
The link to the Web-based questionnaire was sent via an e-mail distributed to hospital staff, and data were managed via SurveyXact. The open questionnaire link was sent out by e-mail via a secretary at the top level of hospital management, supported by the director of quality improvement and staff leaders. It was sent once to staff e-mails and remained open for completion for a 6-wk period in October and November 2022. As the questionnaire was sent out via large e-mail groups and open links, the number of health care professionals who received the questionnaire is not known.
Data Analysis
Content analysis was used as the overall analytical approach of the qualitative data generated by the interview study. 29 Transcripts were first analyzed inductively; during the final interpretation, interview data and qualitative survey responses were analyzed deductively. NVivo (QRS) was used to manage the interview data and the themes generated following inductive content analysis. In this process, the “memos” function was used in NVivo to ensure that analytical reflections were logged. Based on this analysis, themes emerged that brought new perspectives to the preliminary questionnaire, and adjustments to the questionnaire were made as a result. The final deductive analysis was conducted in a Word table, constructed for the purpose and with the aim of explaining the quantitative survey results. All data coding was performed by A.H. and later discussed with the research team to enhance the validity of the findings.
Stata (version 17.0) was used for the descriptive statistical analysis of survey data. Demographic data were presented in a table with numbers and percentages as well as mean and standard deviation. Furthermore, all Likert scale responses were presented in figures to give an overview of the results graphically.
Qualitative and quantitative findings were merged during the deductive analysis phase of the study to synthesize findings for the final interpretation of the data to address the study objectives. The “Results” section presents the quantitative findings first and uses quotes from the qualitative analysis to elaborate.
Ethical Considerations
Under Danish law, interview and questionnaire studies of this type do not require ethical approval from the regional ethics committee. The Department of Quality Improvement and hospital management approved the study and the distribution of the questionnaire. All study participants were informed of the study verbally and/or in writing. Interviewees provided written consent; survey participants consented by filling in the questionnaire. Study participants were informed that the data would be anonymized. All data were stored and analyzed in secure hospital systems. The study received no external funding, but A.H., L.O.R., and H.L.B. were employed through a Central Denmark Region start-up grant (2019–2023). The article was drafted in accordance with the principles of the Committee of Publication Ethics.
Results
Sample and Setting
Of the 1,725 health care professionals who replied to the questionnaire, the final sample for the analysis was 420. Participants excluded from the analysis were those who reported having no direct contact with patients in their daily practice or who did not use PII and those who submitted incomplete questionnaires. Characteristics of the survey respondents can be found in Table 2.
Characteristics of Survey Respondents (N = 420)

A purposeful sample of health care professionals (n = 12) from different hospital departments was selected for the interview study (Table 3); interviews lasted between 40 and 75 min.
Characteristics of Interview Participants (n = 12)
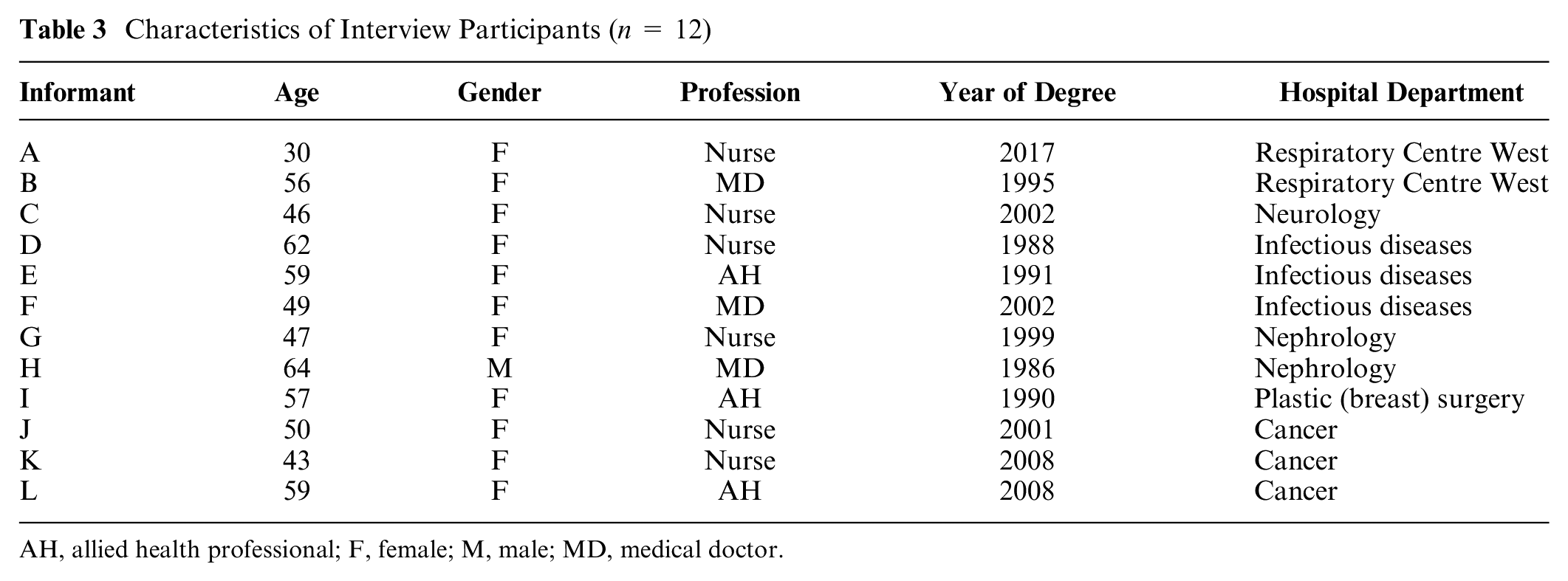
AH, allied health professional; F, female; M, male; MD, medical doctor.
Health care professionals from across specialties, professional areas, and experience levels were included in the study (Tables 2 and 3). Numerous hospital departments were represented, from acute settings to long-term hospital wards and outpatient clinics. PII were used in different situations to support health care professionals’ daily interactions with patients during care and treatment. As patient involvement is affected by patient capacity to engage in interactions, health care professionals in different settings adapted the use of PII to meet factors such as level of consciousness, cognitive impairments, delirium, fatigue, mental problems, and communication difficulties to ascertain patient wishes and enable engagement in decision-making processes.
PII Used by the Health Care Professionals
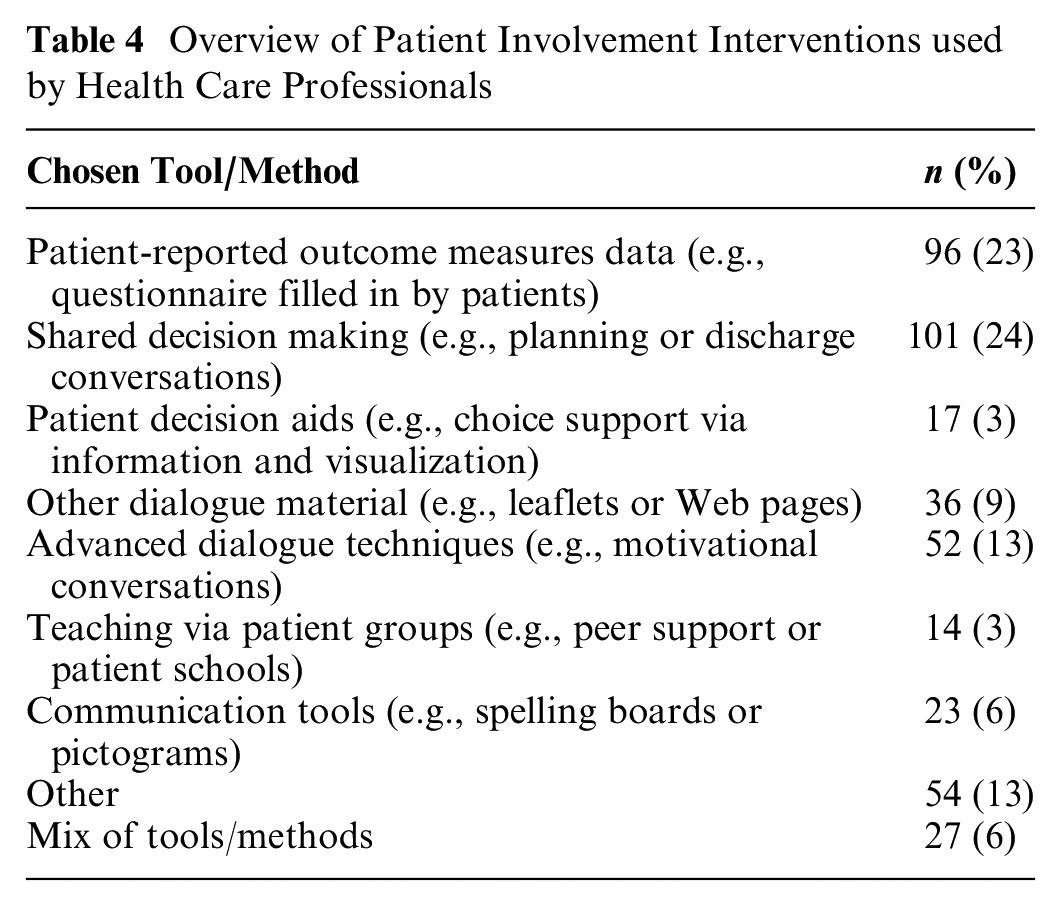
Health care professionals reported the use of various PII to support communication with patients, such as PROM, SDM, PDAs, communication tools, or a mix of methods (Table 4). Health care professionals reported their use of established communication skills to “listen to the patient” and engage in conversations without needing a formal structure. An app-based patient pathway guide to support information giving and approaches such as advanced care planning, person- or family-centered care, and fundamentals of care were also mentioned in the questionnaire. More than half of the respondents (67%) reported receiving some training on a tool or method.
Overview of Patient Involvement Interventions used by Health Care Professionals
Interviewees described communication and interaction as being umbrella terms for patient involvement and the use of PII. Being with the patient and trying to understand their situation, needs, and experiences was seen as the core of patient involvement, with different tools and methods providing concrete ways to reach a common understanding about care and, sometimes, a joint decision about treatment and management:
It is very much about how we communicate, so that we ensure that the patients are involved in what is going to happen. And here we have some methods that we can use. (C) We have worked with PRO data, where patients have received a questionnaire before a consultation. And that is a way of making people actively decide what is important for them and prepare for their consultation. So, it facilitates the process of the patients thinking about what is important to them to talk to our team about. And sometimes this means that I do not waste time on unnecessary subjects. (F)
The health care professionals stated that they could support patient involvement via their established communication skills and interactions with patients. PII were seen as supporting patient involvement but were not viewed as tools or methods that could stand alone. Sincere presence and the associated dialogue were seen as the necessary components for patient involvement in care and treatment:
First of all, it is always important for me to be present when I am with another human being. I think that, as a health care professional, it is an important tool because it is within that contact that there is a presence with the human being that I am sitting in front of, and to me that is a caring act, but it is also a way that I can guide the person with my experience and knowledge much faster. (E) I think that people use it differently. The tool is the same, but the conversation can be shaped in all the ways that people are. It’s being read and used differently by the many patients. And I think that it is our role as health care professionals to be the guides on the journey that we are embarking on. (B)
Health Care Professionals’ Views on How PII Affect Patient Experiences and Pathways
Health care professionals viewed PII methods and tools as impacting positively on patient experiences and pathways, although there was variation in responses to items, with up to one-third of health care professionals stating that they were uncertain (“do not know”) about some benefits (Figure 2). This uncertainty may be indicative of mixed feelings about PII or a lack of knowledge about their impact on patient experiences and pathways or service benefit within the health care system. The qualitative findings suggest those with a positive attitude toward PII perceived the hospital, their service, and their identity as motivated to include these tools and methods within their everyday practice to improve the delivery and experience of care at both group and individual levels:
I think that we have a culture here [in the department] where we very much care about what the patients think. Because they are the experts on how they are doing and how they experience the treatment, and we are experts on other things. . . . And that is our attitude. (K) Patient involvement is an integrated part of my identity. (E)

Health care professionals’ evaluation of how patient involvement interventions affect patient experiences and pathways.
Health Care Professionals’ Views on How PII Affect Their Clinical Reasoning
Health care professionals saw PII as being associated positively with their clinical reasoning and process of care. PII were seen as supporting their communication with patients, identifying patient needs, involving patients in their own care, and enhancing the clinical judgment of health care professionals (Figure 3). There was less variation in items, with 5% to 10% of participants being uncertain about the impact of PII on aspects of their clinical reasoning. The qualitative findings illustrate that PII helped enhance participants’ professional reasoning, often unconsciously and in brief encounters:
Yes, it is just like these types of communication like mirroring or active listening. You are actually not always conscious of this, it just happens. It is a bit unconscious. (G) It is short encounters where you have to provide a lot of information and quickly build a trusting relationship with the patients. (C)

Health care professionals’ evaluation of how patient involvement interventions affect their clinical reasoning process.
PII were seen as more supportive in cases in which the patient category was new or unfamiliar. Where health care professionals had extensive knowledge and experience of specific patient groups, they felt able to disengage from a specific structure for an intervention:
It is useful when it is a new patient category you don’t know that well. But with the other patients, I know it like the back of my hand, I don’t need the structure that the diagram gives me. (A) I actually don’t fill it out with patients, as I think it was intended. But I know it so well that we engage in a dialogue around it. (B)
Discussion
The findings of this study contribute novel insights into the use of PII by health care professionals as a cohesive set of strategies supporting patient involvement in clinical practice. PII, while not operating in isolation, play a crucial role in facilitating communication, interaction, and relationship building between patients and health care professionals. These interventions offer tangible tools and methods to support such interactions. Health care professionals perceive that PII have a positive impact on patients’ experiences and pathways. Furthermore, PII contribute to enhancing health care professionals’ clinical reasoning processes, even though these are often unconscious. Understanding the link between PII and health care professionals’ clinical judgment is crucial for implementation, especially considering that this connection has not been previously elucidated across various hospital departments and when considering PII as a unified set of interventions throughout the continuum of care and treatment.
These findings illustrate that health care professionals see communication and interaction with patients as the fundamental goals of patient involvement practices; they felt that patient involvement was achieved through their communication skills. Health care professionals used a range of interventions to inform their patient involvement practices across departments and specialties at AUH. The study classified the tools and methods health care professionals defined as supporting patient involvement in health care, rather than drawing on categories used by researchers to classify PII.1–3 Health care professionals perceived that patient involvement practices affected their clinical reasoning and enabled their care planning and communication with patients, although this was not always a conscious process.
From the health care professionals’ perspective, communication was seen as a fundamental aspect of patient involvement. The overall goal of patient involvement was to reach a joint understanding about care and treatment, to share reasoning about plans, and, in some cases, to make a joint decision. The health care professionals described how patient involvement could be achieved using efficient and holistic communication, without the need for PII. However, having PII tools and methods that supported communication and interaction processes was seen as valuable. They provided ways to structure the interaction and, in some cases, to visualize aspects of the communication. Family- and/or patient-centered care models were mentioned by some participants, but none mentioned explicitly patient- or person-centered communication skills or training. However, many of their descriptions aligned with these principles of placing the patient at the center of their care and communication. 30 To ensure knowledge translation of person-centered communication skills into clinical practice, it is important to implement training programs that, for example, underpin health care professionals’ self-reflection of their clinical reasoning. 31 This would affect health care professionals at a group level but also the culture of a department, enhancing reasoning and knowledge sharing between novice and expert health care professionals and within the group.
Results from this study revealed that the use of PII spans the continuum of care and treatment in all hospital departments. In keeping with other studies, SDM, PDAs, SSM, and PROM interventions were more likely to be adopted in outpatient clinics or nonacute hospital wards.8,32,33 In intensive care and emergency department settings, the use of PII is particularly impaired when patients are not fully conscious, have communication difficulties due to intubation, or experience cognitive impairments and delirium. 34 In these settings, PII aimed to enable proxy decision makers (e.g., relatives or care assistants) to contribute to care plans, with patients involved once they have capacity to engage with the health care professionals. Several communication tools were developed and used widely to meet the challenges of involving patients within intensive care units. 35 These findings illustrate that health care professionals adopt diverse methods to communicate with patients who have complex needs to deliver patient-centered care. This is also the case in clinical settings where patients have capacity issues related to a mental health problem illness 36 or dementia. 37 Health literacy has been shown to be associated with patients’ ability to be involved in care and make medical decisions. 38 This was not specifically described in our results, but many of the aforementioned factors affect patients’ health literacy and the applicability of PII. To ensure that PII fit all patient populations, there is a need to focus on specific patient characteristics and levels of health literacy when developing and implementing PII. It is also relevant to include perspectives on the e-health literate patient. 39
The health care professionals’ clinical reasoning was found to be a process that they were not consciously aware of and can be thought of as “tacit knowledge.” As clinical reasoning is a cognitive process that is both intuitive and analytic, it is not surprising that it could be hard for the health care professionals to articulate this part of their practice. The dual process theory40,41 defines how these 2 systems interact within clinical decision making: system 1 involves heuristic, automatic, intuitive, nonanalytic, and rapid decision making, whereas system 2 involves systematic, deliberate, conscious, analytic, and slow decision making.42,43 Learning to communicate the clinical reasoning process explicitly may be an important step in communication skills training as it enables professionals to share their rationale linking the evidence base for treatment, appraisal of patient need, and inclusion of patient perspective explicitly with colleagues, managers, patients, and relatives.14,15 Use of PII could be a way of enhancing system 2 thinking, with health care professionals following the systematism of specific PII and reasoning explicitly. However, this requires further study. The PII evaluated in the current study were found to fit with the clinical reasoning of health care professionals and the need to build trust quickly with patients to support communication within patient-professional interactions.
By using the MIND-IT multiple decision makers and MRC complex intervention research frameworks, we were able to illustrate a gap of knowledge between PII researchers and health care professionals and between health care professionals and organization-level quality improvement. Health professionals seemed unaware of 1) the intrinsic benefits of PII in supporting patients in making sense of their health problems and illness management in the context of their life and 2) the impact of patient involvement on health service outcomes and wider patient benefits beyond the delivery of evidence-based, patient-centered care. These findings underline the importance of including the values, experience, knowledge, and motivational factors of health care professionals when considering variations in patient involvement practices and mechanisms to innovate services. It seems likely that the following mechanisms may increase the systematic adoption of PII by health professionals: training for health professionals on the intrinsic value of PII to patients in the context of their lives, collaboration between PII innovators to adapt well-researched tools and methods for integration within their practice, and providing feedback to clinical teams about the impact of using PII on longer-term outcomes and patient benefit. However, there is a need for the inclusion of robust measures to capture change in service and care delivery 1 as well as for support infrastructure to ameliorate organizational barriers to using PII and monitoring their impact.
Integrating PII into health care requires consideration at the policy (macro), management (meso), and delivery of care (micro) levels 44 and using a combination of top-down and bottom-up approaches. 19 Based on our results and discussion, we suggest a schema to link clinical reasoning with PII, other stakeholder goals, and service infrastructure with an emphasis on understanding the importance of their purpose of the PII and how it affects practice (Figure 4). Furthermore, we need to move the narrative of PII implementation as a “simple” intervention of staff training or resource use in practice toward a more “complex” intervention recognizing the need to support the reasoning of multiple decision makers delivering, and accessing, health care. If the current paradigm continues to emphasize the health care professional providing expertise and the patient sharing their preferences, we are going to continue in this same implementation loop. The barriers to adoption of PII innovation will continue to be health care professionals 1) perceiving their current practices as sufficient to involve patients in their care and treatment and 2) making judgments about whether or not an innovation will enhance their communication with patients and patient involvement in their own care. Interaction, communication, and shared reasoning are at the core of the necessary movement.

Schema linking clinical reasoning about patient involvement interventions, other stakeholder goals, and service infrastructure.
Limitations
This study used a mixed-methods design including a cross-sectional survey to provide a snapshot of how health professionals are using PII in their service delivery. The distribution strategy of the survey does not allow for an exact calculation of response rate but was based on what was pragmatically possible to ensure both reach and anonymity of participants. The qualitative interview and free-text questions in the questionnaire provided context to interpret these descriptive responses and identify what enables, and hinders, health professionals’ integration of PII, which is a strength. However, we are unclear about how representative the participants are of health professionals in the hospital delivering patient-facing services. It is likely participants are more inclined to use patient involvement practices or have a favorable attitude toward their benefits. Interviewees were recruited from the coauthors’ networks at the hospital; A.H. did not know any participants prior to the interviews. It is possible that health professionals at AUH may have different knowledge, views, and skills from others across Denmark due to active quality improvement initiatives around patient-centered care and SDM at the hospital over the past 10 y. However, we are confident that these findings captured how health care professionals reason about ways to involve patients in their care and the consequences of patient communications for informing management and treatment plans.
Conclusions
This study provides novel findings illustrating that PII as a collected group of interventions are used across the spectrum of care and treatment services and that health care professionals are motivated to use them. This is partly because PII are viewed as being beneficial for patients’ experiences and pathways and partly because they fit with health care professionals’ clinical reasoning process. PII provide concrete tools and methods to optimize care and service delivery, but communication was seen as the core aspect affecting health care professionals’ interaction with patients and relatives. Results show an interrelation between clinical reasoning and PII, but the exact mechanisms need further exploration. Our results suggest clinical reasoning is an active ingredient in the implementation of PII, and finding ways for health care professionals to describe explicitly their reasoning could be a way of identifying possible mechanisms of change when developing and implementing complex PII in health care.
Implications
The results of this study have a number of implications for both practice and research. In terms of practice, the results emphasize the need for training in person-centered communication and the use of PII relevant to the health care professional’s specific setting. This should include training in articulating their clinical reasoning reflections and tacit knowledge. Furthermore, health care professionals would benefit from knowledge about the longer-term benefits of care and treatment, to enhance their understanding of the impact of PII along patient pathways beyond their own department. As far as research is concerned, we need a more in-depth understanding of how clinical reasoning and PII are interrelated. This includes perspectives on whether clinical reasoning can be considered an active ingredient or mechanism of change in the development and implementation of PII.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683241229987 – Supplemental material for Integrating Patient Involvement Interventions within Clinical Practice: A Mixed-Methods Study of Health Care Professional Reasoning
Supplemental material, sj-docx-1-mpp-10.1177_23814683241229987 for Integrating Patient Involvement Interventions within Clinical Practice: A Mixed-Methods Study of Health Care Professional Reasoning by Anna Holm, Lotte Ørneborg Rodkjær and Hilary Louise Bekker in MDM Policy & Practice
Footnotes
Acknowledgements
We would like to thank Lisbeth Kallestrup and Ditte Lucia Heltberg Melgaard from the Department of Quality and Patient Involvement at Aarhus University Hospital for their help designing and distributing the questionnaire.
Correction (April 2024):
Article updated to include attribution for Figure 4.
CRediT Contribution statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by the Research Centre for Patient Involvement via a Central Denmark Region start-up grant (no award/grant number). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report. The following authors are employed by the sponsor, Research Centre for Patient Involvement.
Data Availability Statement
Data are not available due to legal restrictions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.