
Abstract
Introduction
This study examined relationships between patient reported quality of life and demographic, disease related, and clinician–patient communication variables in people with leukaemia, using a validated haematological malignancy specific patient-reported outcome measure to provide insights to help improve care and enhance patient well-being.
Methods
A prospective global cross-sectional online questionnaire study was conducted, with people self-identifying as patients with leukaemia, that included 100 items on demographics, information on communication, disease and treatment and the Haematological Malignancy Patient-Reported Outcome (HM-PRO) instrument. The HM-PRO scores were analysed using Kruskal-Wallis tests and Gradient Boosting Decision Trees (GBDTs) to identify key factors associated with patient outcomes.
Results
2,260 patients with leukaemia participated, from 64 countries, of whom 1,993 completed the HM-PRO Part-A (measure of QoL) and 1,951 completed Part-B (signs and symptoms). The HM-PRO scores varied significantly by demographic factors, with younger patients (18–25) and people with acute leukaemia reporting the highest scores. Communication about treatment decisions and side effects was significantly associated with HM-PRO scores (η2: 0.012–0.063). GBDT models had high Area Under Curve but low accuracy: isolation and depression emerged as key predictors of QoL classification.
Conclusion
Improved clinician-patient communication and psychosocial support may mitigate the burden of leukaemia. Tailored, person-centred approaches integrating medical and emotional care could improve QoL, treatment adherence, and outcomes, particularly for younger patients and people facing significant treatment challenges. However, given the cross-sectional design, causal inferences cannot be made. We note our findings are presented strictly as associations observed in cross-sectional data, and we acknowledge the potential for bidirectional relationships between QoL and the variables explored. The findings primarily reflect the experiences of individuals who are more engaged, digitally included, or connected to advocacy organisations, rather than the broader leukaemia population.
Plain Language Summary
Keywords
Introduction
Background
Leukaemia is a haematological malignancy characterised by the abnormal proliferation of white blood cells, which impairs the production of normal blood cells. Acute leukaemia (AL) progresses rapidly and poses life-threatening risks if not treated promptly, whereas chronic leukaemia (CL) typically progresses slowly and requires long-term management.1-3 The quality of life (QoL) of patients with leukaemia is impacted by the diagnosis and subtype, its treatment, demographic characteristics such as age and gender, comorbidities, and psychological conditions.1-11
There is a link between enhanced clinician communication and patient involvement in decision-making leading to improved patient QoL and clinical outcomes.12-16 Nonetheless, embedding this approach into everyday clinical practice remains slow.17,18 It is paramount that clinicians and healthcare staff communicate in a way that is person-centred and deliver care in a way that meets the needs of the individual.19,20
To inform evidence-based patient information and support, and to drive improvements in care quality and experience for patients with leukaemia, a large-scale cross-sectional observational study using a questionnaire methodology was conducted. The study was initiated in 2023, with a global population of patients with leukaemia and assessed patient experience from diagnosis onwards, as a follow up to a previous study. 4
Objectives
The aim of this study was to assess the association of demographics, disease type, and clinician-patient communication, and patient-reported outcomes (PROs) to provide evidence-based insights to inform clinical practice and policy.
Methods
The study was a prospective global, cross-sectional, online, open questionnaire hosted on Qualtrics survey platform. The study participants were recruited from the members of the national leukaemia patients advocate support groups as convenience sampling. Before starting the questionnaire, the participants were informed of the purpose of the questionnaire; that completing the questionnaire was anonymous and voluntary; and how the results would be used and reported.
The reporting of this study conforms to the STROBE guidelines for observational studies. 21
Ethics
This study involved an anonymous, noninterventional, online patient-reported outcome questionnaire and did not involve clinical interventions, biological samples, or access to identifiable healthcare records. The study was funded by a global network of patient organisations registered in Switzerland, with questionnaire implementation and data analysis undertaken by UK based organisations. In line with governance applicable to noninterventional research using anonymous data, formal approval by an Ethics Committee or Institutional Review Board was not required. Ethical conduct throughout the study followed relevant professional standards and internationally recognised ethical principles, including the Declaration of Helsinki. Personal identifiable data were not collected, and all data were collected, processed, and managed in accordance with the European General Data Protection Regulation 2018; ISO 20252; and Market Research Society Code of Conduct.
Before starting the questionnaire, respondents were informed of the purpose of the questionnaire; that completing the questionnaire was voluntary; and how the results would be used. Agreeing with these terms allowed respondents to proceed.
Questionnaire Technique
The patient questionnaire was substantially revised from previous work, and covered the following areas: demographics, diagnosis, active monitoring (only asked to patients with chronic lymphocytic leukaemia, CLL), treatment, testing and monitoring, information and support, QoL, and views on potential new treatments. Routed questions were used in the questionnaire to ensure respondents were only shown relevant questions. Following review and feedback by patients, caregivers, and patient advocates, the final patient questionnaire had 100 items. Other questionnaire design elements are available (Supplement SM1).
To measure the emotional and physical impacts associated with the disease, the Hematologic Malignancy Patient-Reported Outcome (HM-PRO) measure was incorporated into the study. The HM-PRO instrument is a validated measure, developed specifically to allow meaningful comparisons across different blood cancers, and designed to account for the unique symptom and functional burdens experienced by patients with both acute and chronic haematological malignancies. The tool consists of two components: HM-PRO Part-A, which evaluates general physical, emotional, and social well-being (impact), and HM-PRO Part- B, which focuses on disease-specific symptoms and treatment adverse events (signs and symptoms). The HM-PRO has 24 items in Part-A and 18 in Part-B. The score range for Part-A is 0-48 and for Part-B is 0-36. The higher the total score, the worse effect on a patient’s QoL and higher symptom burden. 6
Perceived satisfaction with clinician–patient communication was assessed through items addressing clarity of information, sensitivity of disclosure, involvement in treatment decisions, and understanding of test results, which together reflect patient-reported communication quality.
Data Collection
The study participants were self-selected. The study participants were recruited through global patient advocacy networks (Acute Leukemia Advocate Network, ALAN; Chronic Lymphocytic Leukaemia Advocates Network, CLLAN; and Chronic Myeloid Leukemia Advocates Network, CMLAN), via branded advertisements in email, online forums, social media, newsletters, and active contact to network members (Supplement SM1). The advertisements distributed an open QR code or URL link with customised name to the questionnaire as hosted on an online portal (Qualtrics). The questionnaire was available to complete between 19 August 2023 and 05 January 2024 (inclusive).
The study participants were patients with leukaemia aged 18 and above. People who answered they had a condition other than leukaemia were directed to the end of the questionnaire and were excluded from the analysis. The questionnaire was available to complete in the following 14 languages: Brazilian Portuguese, Chinese (simplified), Czech, Danish, Dutch, English (UK), English (US), French, German, Hebrew, Italian, Korean, Russian and Spanish. Completion was voluntary, without incentives. Respondents could submit responses without all questions completed. Survey responses were anonymous at the point of collection.
These approaches aimed to give a wide range of response, with a view to mitigating some of the biases inherent in open surveys.
A formal a priori sample size calculation was not performed, as the study was exploratory and used an open, global convenience sample recruited via patient advocacy networks, with unknown true population proportions. Therefore, the design did not lend itself to a priori calculations.
Statistical Analyses
Questionnaires that were submitted through the portal where at least 14 questions were answered entered the data set. Data were downloaded from Qualtrics and Python 3.9.20 invoked via Spyder 5.5.1 was used for analyses. No statistical adjustments were made, as the true population proportions were unknown. Demographics and reported experiences were summarised with descriptive statistics. Inferential statistics were used to explore the study questions.
The HM-PRO Parts-A and -B were set as the dependent variables, and the score values were used as a discrete numeric variables. Only data for patients who provided an HM-PRO score were included in analyses.
The primary analyses were conducted on the pooled dataset. This approach was prespecified because the HM-PRO is a validated haematological malignancy specific patient reported outcome measure designed to enable meaningful comparisons across haematological malignancies, irrespective of disease subtype. Leukaemia type was therefore examined as an independent variable to provide empirical findings of any associations.
For independent variables, priority was given to 13 “focus” variables: demographic and communication-related items identified in advance of the analysis as relevant to the research question. Broader analytic interest was acknowledged, and so additional testing was conducted on an extended set of demographic and healthcare-related independent variables. All independent variables are listed in Supplement SM2. With low ability to determine respondent number in advance, we anticipated an ability to detect moderate effect sizes using non-parametric tests. 22 Kruskal–Wallis tests were used for the analysis. 23 Within variable group medians were calculated. A Bonferroni-adjustment to mitigate Family Wise Error Rate was applied. 24 This is a conservative adjustment, meaning that although true positives may be missed, the false positives are less likely to be accepted. Eta-squared (η2) was used as a measure of effect size, to quantify how much variability in the HM-PRO scores can be explained by the variable in question. 22
Classification and Prediction Approach
The dependent variables were set as grouped scores of the HM-PRO Parts-A and -B, thus using categorical data. The grouped scores were rescaled to 0-100 using an anchor-based approach, taking a percentage by dividing an individual’s score by the maximum attainable (48 or 36).25,26 The remaining variables were included in the data set, except for the constituents to the HM-PRO measures, as candidate independent variables.
A Gradient Boosted Decision Tree (GBDT) approach was used, 27 invoked via the LightGBM package to predict and classify the outcome.28,29 The GBDT approach combines multiple decision trees to improve predictive accuracy, as such it is an “ensemble machine learning” method. 30 In LightGBM, the models optimise classification tasks by penalising incorrect predictions across several outcome categories (minimising “multi-class log loss”). Each individual decision tree is built sequentially, with each new tree attempting to correct the errors of the previous ones by focusing on the gradients of the log loss function. This is suited for efficiently handling survey data, especially when dealing with categorical variables and missing values. The LightGBM method has built-in regularisation techniques to help mitigate overfitting, so that the model can be more easily generalised to new, unseen data. The models were tuned via “hyper-parameter optimisation”, setting parameters such as maximum tree depth and stopping rounds for information gain via the HyperOpt package. 31
The model performance was evaluated by splitting the data into train (two thirds) and test (one third) subsets and using the test set to create diagnostic metrics (accuracy, precision, recall, F1-score) and plots of Receiver Operating Characteristic (ROC) with the derived Area Under the Curve (AUC) for model performance, a “confusion matrix” of classification patterns, and a “gain importance” graph to find the most influential features in the model’s predictions. The focus was placed on accuracy, F1-score, AUC, and the key factors from the “gain importance” graphs as accuracy measures overall correctness, F1-score shows the trade-off between precision and recall, and AUC evaluates the model’s ability to distinguish between classes across different thresholds, 32 while “gain importance” graphs highlight the most influential features, aiding interpretability and feature selection. 33
Results
Demographic Characteristics of the Study Participants
Demographic Characteristics of the Study Participants
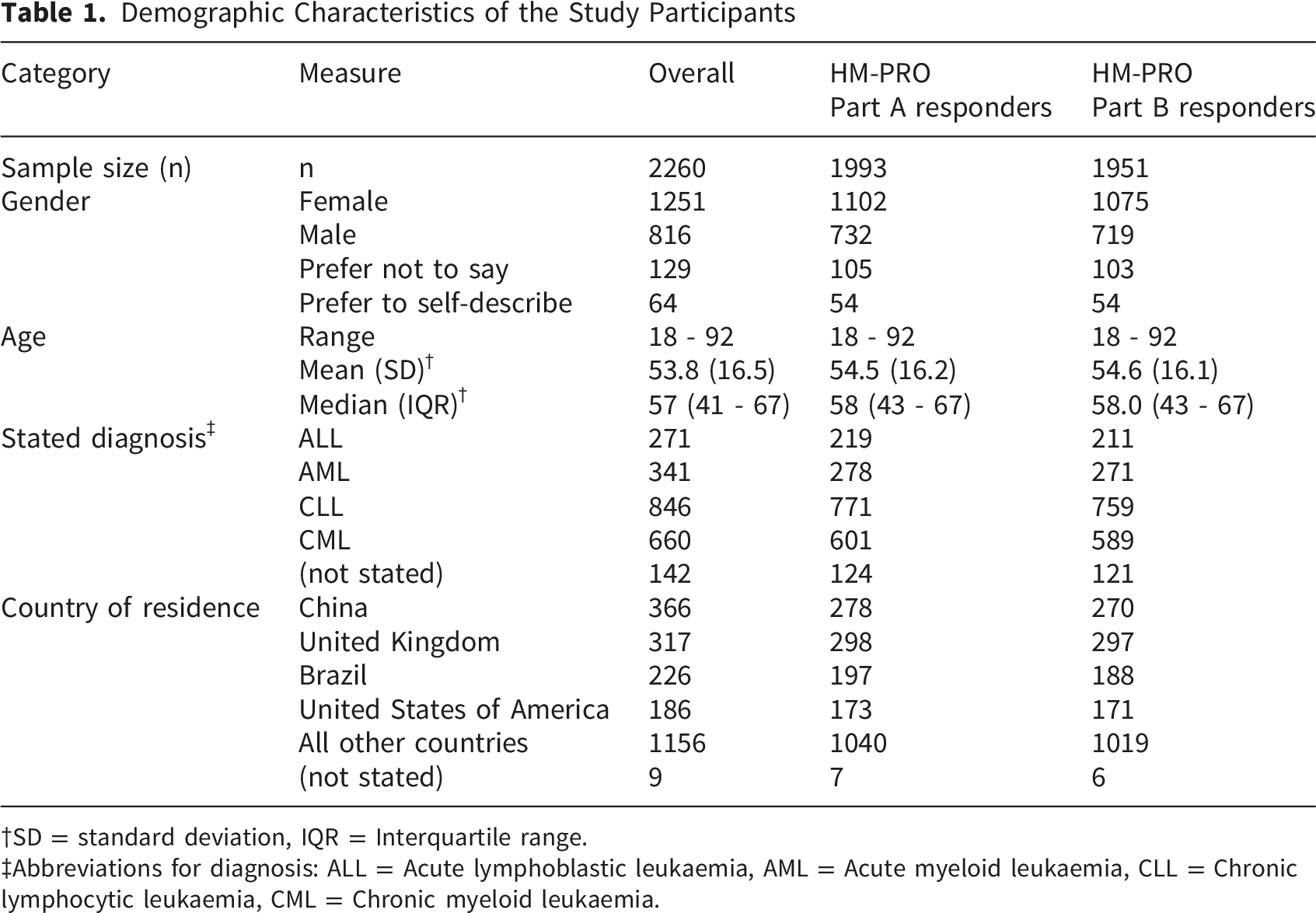
SD = standard deviation, IQR = Interquartile range.
Abbreviations for diagnosis: ALL = Acute lymphoblastic leukaemia, AML = Acute myeloid leukaemia, CLL = Chronic lymphocytic leukaemia, CML = Chronic myeloid leukaemia.
For patients completing the HM-PRO Part-A (n=1993), scores had a median of 14 (interquartile range, IQR, 8-22). The reported diagnoses were the highest for CLL (n=771), followed by chronic myeloid leukaemia (CML, n=601), acute myeloid leukaemia (AML, n=278), acute lymphoblastic leukaemia (ALL, n=219), and “Other types of leukaemia” (n=124). Approximately half of the patients providing HM-PRO Part-A scores came from the group of four countries (Table 1): United Kingdom (n=298), China (n=278), Brazil (n=197), and the United States of America (n=173).
Relationships Between HM-PRO Scores and “Focus” Variables
There were 1,993 people who completed the HM-PRO Part-A, and 1,951 went on to complete the HM-PRO Part-B. The HM-PRO Part-B responders are a subset of people (n=1951) responding to Part-A (i.e., not a separate group) with a median score of 6 (IQR 3-11). The distributions of HM-PRO scores are given in Figure 1. Histograms for the (A) HM-PRO Part-A scores and (B) HM-PRO Part-B scores of respondents with leukaemia to the 2023 Global Leukaemia Experience Survey. Both distributions are right skewed
Although primary analyses focused on 13 “focus” independent variables, tests were conducted across groups of 40 variables. Accordingly, the Bonferroni-adjusted threshold was applied (0.05/40 = 1.25E-03). There were statistically significant differences across most variables using this adjusted threshold, indicating their association with patient-reported outcomes (Supplements SM4 and SM5).
Comparisons of the Socio-Demographics With HM-PRO Part A and Part-B Scores†

Kruskal-Wallis (KW) results for demographic questions against HM-PRO scores. Response number is shown by n; medians and interquartile range (IQR) are reported, and p-values for the KW test are given. Eta-squared (η2), indicates size of effect.
Bonferroni adjusted alpha = 0.05/40 = 1.25E-03. Variables marked with * have a significant result against that threshold.
ALL = Acute lymphoblastic leukaemia, AML = Acute myeloid leukaemia, CLL = Chronic lymphocytic leukaemia, CML = Chronic myeloid leukaemia.
Bivariate analyses were conducted to test for relationships between leukaemia type and HM-PRO scores. For HM-PRO Part-A, people diagnosed with acute lymphoblastic leukaemia (ALL, n=219) and acute myeloid leukaemia (AML, n=278) reported higher medians (ALL median 20 [IQR 13-28]; AML median 18 [IQR 10-24]) than the chronic leukaemias (CLL, n=771, median 11 [IQR 6–17.5]; CML n=601, median 14 [IQR 9–21]). For the HM-PRO Part-B, ALL (n=211, median 8 [IQR 3–13]) and CML (n=589, median 7 [IQR 4–12]) had higher median scores than AML (n=271, median 5 [IQR 2–10]) and CLL (n=759, median 5 [IQR 2–9]). The effect sizes of the relationship between disease type and HM-PRO scores, measured by eta-squared, indicate that diagnosis explains approximately 6% of the variance in Part-A and 4% in Part-B. As a secondary analysis, we classified into Acute and Chronic. For HM-PRO Part A scores for Acute (median 19, IQR 11-26) and Chronic groups (median 12.5, IQR 7-19), using Mann-Whitney U-tests, we reject the null hypothesis of no difference between (U = 246474.5, p < 4.77E-20), with a small effect size (η2 = 0.045). We were unable to reject the null hypothesis of no difference between Acute (median 6, IQR 3-10) and chronic groups for HM-PRO Part B (U = 313491, p = 0.252, η2 = 0.001). Patients aged 18–25 exhibited higher median scores for the HM-PRO Part-A (n=101, median 22 [IQR 12–31]) and Part-B (n=97, median=8 [IQR 3–12]).
Comparisons of the Communication Questions With the HM-PRO Scores (Part-A and Part-B)*

†Kruskal-Wallis (KW) results for communication questions against HM-PRO scores. Response number is shown by n; medians and interquartile range (IQR) are reported, and p-values for the KW test are given. Eta-squared (η2), indicates size of effect.
‡Bonferroni adjusted alpha = 0.05/40 = 1.25E-03. Variables marked with * have a significant result against that threshold.
§ALL = Acute lymphoblastic leukaemia, AML = Acute myeloid leukaemia, CLL = Chronic lymphocytic leukaemia, CML = Chronic myeloid leukaemia.
Responses to involvement in treatment decisions and clarity of information on treatment side effects suggest that increased patient engagement and transparent communication may serve as protective factors against the psychosocial burden of leukaemia.
Classification and Prediction of QoL, as Measured by HM-PRO
The GBDT model for the HM-PRO Part-A was built using a model with 430 decision trees and demonstrated moderate accuracy in predicting the HM-PRO Part-A group (overall accuracy of 51.4% and an F1-score of 0.502). However, the Area Under the Curve (AUC) was notably high at 0.80, which suggests that the model has good discriminatory power. These seemingly contradictory results can be interpreted as the model being less able to predict the exact group of an individual yet able to identify factors important in predicting levels of QoL (Box 1). The model identified several key variables that were most influential in classifying the HM-PRO Part-A score: isolation (Q88_6), worry while waiting (Q71), disease-related anxiety (Q88_2), depression (Q88_5), and year diagnosed (Q09). Model performance diagnostics, including summary statistics and evaluation graphs, are provided in Supplement SM6.
For predicting the HM-PRO Part-B group, the GBDT model was built with 290 decision trees, and had low accuracy at 45.5% with an F1-score of 0.415. Despite this, the AUC was moderately high at 0.73, which, as for the HM-PRO Part-A, suggests that the model is somewhat effective at distinguishing between different levels of QoL, and struggles with individual predictions. The most important predictors for the HM-PRO Part-B score were symptoms (Q11), depression (Q88_5), isolation (Q88_6), year diagnosed (Q09), and fatigue severity (Q54_3). Model performance diagnostics, including summary statistics and evaluation graphs, are provided in Supplement SM7.
In these multivariable analyses, disease type was included as a candidate predictor but was not among the most influential variables in the decision tree models. A decision tree model assigns each person a set of predicted probabilities, one for each potential outcome group. The person is then classified into the group with the highest predicted probability. The The Together, these metrics suggest that whilst the models in this study capture meaningful distinctions in the data (as reflected by the AUC), they struggle with precise classification, as shown by lower accuracy and F1 scores. This may reflect the inherent difficulty of modelling multi-ordinal outcomes, where adjacent categories can be difficult to distinguish. From a clinical perspective, this limitation may affect the reliability of patient-level predictions in borderline cases.Box 1. Interpretation of Some of the Diagnostic Measures for Decision Trees
Discussion
This study provides valuable insights into QoL of patients with leukaemia, emphasising the interplay between demographics, clinical and communication factors. We note our findings are presented strictly as associations observed in cross-sectional- data, and we acknowledge the potential for bidirectional relationships between QoL and the variables explored. The findings reinforce well-documented associations between psychosocial distress and QoL in patients with leukaemia. Similar to prior research,5,7,8 this study highlights that depression, anxiety, and social isolation were significantly associated with reduced QoL; however, this study does not note such a strong effect for fatigue. The findings of this study are consistent with a large-scale international study that have identified mental health as a primary driver of QoL among patients with leukaemia. 4
In line with previous research, there were gender disparities in QoL, with female leukaemia patients reporting worse outcomes compared to males. 4 Our findings further support calls for gender-sensitive interventions that address these disparities and tailor psychological support accordingly. Furthermore, patients who received clear, compassionate, and transparent information about their diagnosis and treatment were associated with lower levels of psychological distress. This reinforces findings that patient engagement in decision-making is associated with better psychosocial outcomes, suggesting a role for structured, patient-centred communication strategies in leukaemia care. 4
However, this study’s findings diverge from some previous work: in general, older patients with cancers report worse QoL9 9 ; however, this study’s findings suggest that younger patients (18–25 years) with acute leukaemia experience disproportionately high burdens on daily functioning, supporting a previous inconclusive finding. 34 This might be partly explained by the fact that older patients and those with longer disease duration do not experience as much interruption in daily living such work, and could have developed tolerance to living with the disease over time. Future work could investigate the impact of age and examine for any need for additional psychosocial, financial, and peer support for younger groups to navigate their diagnosis and treatment.
The results indicate that social isolation, depression, and clinician-patient communication are associated with QoL. This suggests that interventions aiming to improve QoL could go beyond medical management and integrate holistic support strategies that address patients’ emotional and social well-being. The global scope of our study enhances the generalisability of our findings. However, cultural norms, educational background, and access to reliable, non-commercial information may be associated with how patients communicate and what they expect from the respective healthcare. In some cases, expectations may be shaped by exposure to promotional material, which may not reflect what is available within a given healthcare system. This may require clinicians to clarify the rationale for treatment availability and access. This process, coupled with the provision of non-commercial information, initiated by clinicians could adjust a patient’s expectation, which in return could have a positive impact on their QoL. The inclusion of diverse geographic and healthcare system contexts in our analysis provides a broader perspective on how structural factors of healthcare shape leukaemia patients’ QoL.
This study acknowledges the complexity of comparing quality of life across different types of leukaemia. Leukaemia type, either as four groups or as acute and chronic groups, explained only a small amount of the variation in the HM-PRO scores; and for the decision tree models, despite inclusion as a candidate variable, leukaemia type did not emerge as a strong predictor. While the HM-PRO instrument allows for consistent measurement,6,25,26 the clinical trajectories, treatment burdens, and psychosocial impacts differ between acute and chronic forms of leukaemia. An association with more benign diseases in older age and less problems could be an alternative explanation to why QoL differs.
Future longitudinal studies incorporating verified clinical variables such as remission status and treatment intensity are needed to better characterise temporal relationships and disease trajectories, particularly in younger patients aged 18–25 years, who appear to experience a disproportionate quality of life burden.
Implications for Clinical Care, Patients, and Advocacy Networks
From a clinical standpoint, our findings suggest a need for holistic and patient-centred leukaemia care, which balances physical and mental symptom management and enhanced communication. The strong association between psychosocial distress and QoL suggests a need for integrating mental health support into standard treatment pathways. Routine screening for psychological distress, alongside targeted interventions, such as counselling and peer support groups, could help mitigate the negative emotional impacts of leukaemia. There is an association with clinician-patient communication. Clinicians could prioritise transparent, sensitive, and accessible communication, ensuring that patients fully understand their diagnosis and treatment options. Training programmes for healthcare professionals focused on effective patient communication may further enhance QoL outcomes. Patient preferences for involvement in decision-making vary and may be shaped by cultural norms, emotional readiness, and timing within the disease trajectory. For example, individuals recently diagnosed may feel overwhelmed and could prefer a more paternalistic or guided approach. Clinician–patient communication should, therefore, be responsive and negotiated, adapting to the patient’s needs and preferences over time. The communication needs and measured QoL vary between acute and chronic forms, and future work should explore these differences in more depth.
For patients, these findings suggest an association of self-advocacy in healthcare outcomes. Patients who actively engage in their treatment decisions and receive clear, transparent information tended to provide better QoL outcome scores. The HM-PRO offers a way to express how leukaemia affects their daily life and emotional well-being, helping ensure their concerns can be heard and addressed in care. Furthermore, the identification of isolation, depression, and disease-related anxiety as key QoL predictors suggests a role for engaging with support networks. Peer communities, patient advocacy groups, and mental health professionals could all help patients cope with the emotional burden of leukaemia.
This study suggests implications for patient advocacy networks. Disparities in QoL based on income and education levels, suggest that advocacy organisations could intensify efforts to ensure equitable access to information and support services. Advocacy groups could focus on reaching underserved populations, offering educational resources tailored to diverse patient needs, and promoting awareness campaigns that empower individuals to take an active role in their care. Advocacy organisations could work toward addressing these gaps by lobbying for policy changes that improve leukaemia care infrastructure and by fostering international collaborations for resource-sharing and best-practice dissemination. Moreover, patient engagement in treatment decisions emerged as a crucial factor associated with psychosocial well-being. Advocacy groups could promote initiatives that encourage patient empowerment, such as mentorship programmes, educational workshops, and digital resources to equip patients with the knowledge needed to participate in their care actively. Given the vulnerabilities identified among younger leukaemia patients, advocacy networks could look to developing targeted support programmes tailored to the challenges faced by this demographic.
Limitations
This study is subject to several limitations. The cross-sectional design limits the ability to infer causality and cannot assess changes in patient-reported outcomes over time. Communication needs and perceptions may evolve over time, but were not detectable by our study, which is an inherent limitation of the cross-sectional design. Although statistically significant associations were found, the effect sizes were generally small, suggesting that the association with QoL may be modest.
The pooling of all leukaemia types in some analyses may obscure important disease-specific differences. Thus, the interpretation of pooled results should be approached with caution. However, we provide an empirical measure of the association between disease type and QoL score, finding the effect size of the relationship was small to medium, suggesting that other factors may play a more prominent role in shaping patient-reported outcomes. Nonetheless, there is a need for future disease subtype specific and longitudinal analyses.
The geographic distribution of respondents was summarised at the country level (Table 1; Supplement SM3), providing insight into the international reach of the survey. However, the distribution within countries is unknown, as collection of these data were beyond the scope of this study. this does limit our ability to assess representativeness or the association with local healthcare systems, cultural norms, and resource availability. Modelling treatment availability is an important contextual factor that remains unaddressed in this study and is a consideration for future research.
The online, open survey promoted through advocacy networks introduced potential for self-selection bias, so respondents may not be representative of the broader leukaemia population, potentially overrepresenting patients who are more engaged or motivated. Digitally excluded individuals may be underrepresented. There is an over-representation of female respondents and the potential underrepresentation of less-involved patients and the digitally excluded. As a result, the study design limits generalisation: the findings primarily reflect the experiences of individuals who are more engaged, digitally included, or connected to advocacy organisations, rather than the broader leukaemia population. That we could not make statistical adjustments, due to the inability to know the true proportion of the population, reduces the confidence in data inferences, and we may not have been able to detect subtle effects given the lack of power calculations. However, we detected effect sizes below Cohen’s threshold for a “small effect”, 22 providing a post-hoc indication that the study had adequate power to detect small differences.
The absence of clinical verification of diagnosis means that responses rely on self-reported data, which could introduce inaccuracies in disease status or treatment history. Key clinical variables, e.g. remission status, were not available and could not be incorporated into the analyses. The absence of clinician-verified diagnosis, and that these unmeasured factors are likely to exert influence on quality of life, may contribute to confounding on observed associations. As a result, differences in the HM-PRO scores cannot be attributed to communication or demographic factors alone. Future studies should incorporate clinician-verified diagnosis, detailed clinical information, and longitudinal follow-up to minimise confounding.
Treatment being received was included but did not emerge as a strong predictor. Variations in healthcare access, cultural perceptions, and differences in how survey items were interpreted across regions may have influenced responses. These differences were not explicitly modelled, which may limit the applicability of findings to specific national or regional contexts.
In mitigation, it is important to emphasise that self-reporting is the essence of capturing patient-reported outcomes (PROs), particularly in QoL research. PRO methodology prioritises subjective experience because many QoL domains, such as emotional well-being, fatigue, and social functioning, are inherently personal and not directly observable. 35 The HM-PRO instrument used in this study is a validated PRO measure developed specifically for patients with haematological malignancies. Its psychometric properties, including content validity and reliability, have been rigorously established.6,25,26 Whilst clinical verification adds precision for disease classification, it does not replace the need for self-reported data when exploring lived experience and psychosocial burden.
The analysis employed a large, geographically diverse sample to enhance generalisability. Non-parametric statistical methods, the Kruskal-Wallis test with Bonferroni correction, reduce the risk of Type I errors and do not rely on assumptions of normality. Despite challenges with the interpretability and moderate predictive accuracy of the GBDT models, their high AUC scores indicate an ability to identify key predictors of quality of life. Thus, although the models developed may not be directly applicable for individual-level decision-making, they remain valuable for highlighting broader trends, informing clinical strategies, and indicating further research perspectives.
Conclusions
Overall, this study aligns with existing literature on the importance of psychosocial factors, communication, and gender disparities in leukaemia QoL while offering insights into the heightened vulnerability of young adults and the predictive power of communication-related variables. While better communication is associated with improved QoL, the observed differences may reflect less aggressive disease courses and symptom burden in older patients with chronic leukaemia.
These findings suggest that clinician–patient communication and psychosocial factors may be associated with variation in quality of life among people with leukaemia. However, given the cross-sectional design, causal inferences cannot be made. Nonetheless, they suggest a role for patient-centred approaches to leukaemia management and advocacy organisations in promoting equitable access to care, education, and psychosocial support. Furthermore, the findings suggest that beyond clinical treatment, psychological health support should be a core component of leukaemia care. Future research could address our study’s limitations by incorporating longitudinal assessments, integrating additional clinical variables, and expanding investigations into healthcare system disparities to understand patient support worldwide.
Supplemental Material
Supplemental Material - Relationships Between Clinician-Patient Communication and the Quality of Life of Patients With Leukaemia: A Prospective Cross-Sectional Global Study
Supplemental Material for Relationships Between Clinician-Patient Communication and the Quality of Life of Patients With Leukaemia: A Prospective Cross-Sectional Global Study by Samantha Nier, Alan J. Poots, Sarah Gunn, Esther Natalie Oliva, Tatyana Ionova, Sam Salek in Cancer Control.
Footnotes
Acknowledgements
We thank the study participants for providing their responses and the advocacy networks and other supporters for promoting the study and patient participation. We thank our colleague, Ben Armstrong, for advice on data setup and cleaning. We thank the editor and reviewers for their thoughtful comments.
Ethical Considerations
Ethics committee approval was not required for this anonymous, noninterventional online questionnaire study, as it did not involve clinical interventions, biological samples, or the collection of identifiable personal data. Ethical conduct throughout the study followed relevant professional standards and internationally recognised ethical principles, including the Declaration of Helsinki. All data were collected, processed, and managed in accordance with the European General Data Protection Regulation 2018; ISO 20252; and Market Research Society Code of Conduct.
Consent to Participate
Before starting, respondents were informed of the purpose of the questionnaire; that completing the questionnaire was voluntary; and how the results would be used. Agreeing with these terms allowed respondents to proceed.
Author Contributions
SS and SN incepted the idea. All agreed to the study questions. SG designed and implemented the questionnaire. AJP designed and conducted the analytics. AJP and SG created the first draft. All critically reviewed and redrafted the manuscript. All approved this submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Acute Leukemia Advocates Network (ALAN).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data can be made available on request by contacting ALAN (
Supplemental Material
Supplemental material for this article is available online.