
Abstract
Background:
Community pharmacists can play a significant role in optimizing depression care. This study sought to assess the practices, attitudes and perceived barriers of Lebanese community pharmacists toward depression care along with the associated factors.
Design and method:
A cross-sectional study was conducted among community pharmacists in Lebanon using a self-administered online questionnaire. Descriptive and bivariate analyses were done followed by linear regression analyses to examine the association between pharmacists’ practices and attitudes with different socio-demographic and professional factors.
Results:
The study revealed a good level of engagement and relatively positive attitudes toward depression care, among the 275 participating community pharmacists. Those with higher attitudes scores (beta = 8.079, p ≤ 0.001) and higher percentages of weekly prescriptions of antidepressants (1%–10% antidepressants, beta = 3.160, p = 0.047; >10% of anti-depressants, beta = 2.829, p = 0.019) were significantly more involved in depression care practices. Besides, being a female (beta = 0.165, p = 0.002), having personal experiences (beta = 2.239, p = 0.001), and the presence of private counseling area (beta = 11.183, p = 0.01) were significantly associated with more positive attitudes. Conversely, pharmacists with more than 10 years of community experience (beta = −20.369, p = 0.021) and those with higher daily encounters with patients (beta = −7.243, p = 0.001) exhibited significantly lower attitude scores. The most reported perceived barriers to depression care were insufficient time for patients (48.7%), inadequate mental health education (46.9%), insufficient data (41.5%), and lack of privacy (37.1%).
Conclusions:
Lebanese community pharmacists generally demonstrate favorable good practices and positive attitudes toward depression care. Several areas for improvement are still desired through broader strategies, training and awareness programs, and effective collaborations.
Introduction
Depression is a common mental disorder with a global estimated prevalence of 3.8%, including 5% of adults and 5.7% of those over the age of 60. 1 This condition has a profound impact on the patients’ quality of life with significant economic repercussions, including diminished productivity and increased mortality. 2 Though effective treatments are available, the current state of depression care is far from optimal. 3 Inadequate screening, diagnosis, and treatment of depression by healthcare providers, stigma toward those affected, and patients’ limited understanding of their disorder lead to poor medication adherence, 4 contributing to higher rates of relapses and increased healthcare costs. 5
An essential aspect of optimizing depression care involves directing attention toward community pharmacists, who represent an underutilized healthcare resource despite being the most accessible. 6 This is especially important considering that the role of pharmacists has undergone a significant transformation, shifting from a traditional focus on merely dispensing drugs to adopting a more patient-centered approach. 7 Community pharmacists regularly interact with patients with depression, considering that up to 20% of the prescriptions they fill include an antidepressant. 8 Hence, they can play an instrumental role in addressing antidepressant nonadherence issues and responding to patients’ information needs. 9
Patients with depression often lack understanding of the condition and antidepressant medications, leading to low adherence. 10 Community pharmacists can offer information, address misconceptions, assess understanding, and positively influence patients’ attitudes; hence improving adherence and treatment outcomes. 11 Community pharmacists also play a role in monitoring patients with depression, focusing on assessing medication adherence, effectiveness, and side effects, 12 and referring patients experiencing treatment resistance or severe side effects back to their prescribing physicians. 13 In addition, community pharmacists can assist in screening patients who are unaware of or hesitant to seek help for depression by recognizing symptoms of untreated depression. 14
However, several barriers may hinder the effective role of pharmacists in depression care. At the system level, pharmacists may encounter challenges like unclear role definitions, conflicts among healthcare professionals, inadequate compensation for pharmacists, time limitations, and privacy issues. 15 At the individual pharmacist level, barriers include unprofessional conduct, discomfort in patient interactions, and inadequate communication skills for discussing sensitive topics. 16
Mental disorders are among the leading causes of disease burden in Lebanon. 17 In the absence of a recent nationwide research on mental health, data from 2002 to 2003 revealed that 17% of the population experienced a mental disorder. 18 This aligns with WHO estimates indicating that 22% of individuals exposed to conflict in the preceding decade may have a mental disorder, including 11% with depression. 19 Recent events in Lebanon including the economic collapse, the COVID-19 pandemic, and the Beirut port explosion have exacerbated the country’s challenges. 20 Knowing that the Lebanese population is under severe distress, and given the vital role that community pharmacists can play in depression care, it is of utmost importance to understand how Lebanese community pharmacists perceive their role. Hence, this study was conducted to assess the practices, attitudes, and barriers of depression care among community pharmacists in Lebanon. Furthermore, the study aims to identify the factors associated with the pharmacists’ current practices and attitudes.
Design and methods
Study design and sampling
A cross-sectional study was carried out between December 2022 and July 2023 to survey community pharmacists across the six governorates of Lebanon (Beirut, South, North, Beqaa, Nabatieh, and Mount Lebanon). Participants were approached through an anonymous self-administered online questionnaire sent by the investigators via social networking platforms. The sample was collected using a snowball-sampling technique where participants were encouraged to pass on the questionnaire link to their acquaintances. The CDC Epi-info software was used to calculate the minimal sample size. 21 According to the registration database of the Order of Pharmacy in Lebanon (OPL), 4112 community pharmacists were actively practicing at Lebanese pharmacies at the time of the study. With the population size being set at 4112 community pharmacist and the expected frequency at 25%, a minimum sample of 269 pharmacists was required to allow for statistical analysis, and produce a 95% confidence interval (CI), with a 5% margin of error.
Ethical approval
The study was approved by the Ethical and Research Committee at the Lebanese International University (LIU) under the number 2022ERC-131-LIUSOP. Written informed consents were obtained prior to study inclusion where the participants have to agree to participate in the study before survey access. The anonymity of respondents was preserved in the study, as the names of the participants were not included.
Eligibility criteria
Licensed Lebanese pharmacists currently working in community settings in Lebanon were included in the study. Pharmacists practicing in settings other than the community, those not currently working in Lebanon, and non-pharmacists working in community pharmacies were excluded.
Data collection and measures
A survey questionnaire was prepared and administered in English as the vast majority of pharmacists in Lebanon speak English. It was developed based on previous pharmacy practice guidelines and validated tools assessing pharmacists’ attitudes, practices, and barriers toward depression care.22 –27 Two faculty members at LIU school of pharmacy reviewed the questionnaire to ensure readability, content validity, clarity, relevance, and completion time. The questionnaire was pretested by five community pharmacists, whose responses were not included in the survey. Minor adjustments were made based on their feedback, resulting in the final version of the survey comprising four main sections.
The first part of the data collection sheet retrieved data regarding socio-demographic and professional characteristics, such as age, gender, level of education, region, years of community experience, position in the pharmacy, number of clients encountered, number of daily prescriptions, and percentage of weekly prescriptions of antidepressants. The second section included 10 items that assessed on a 5-point Likert scale (1 = never, 2 = rarely, 3 = sometimes, 4 = usually, 5 = always) the practice activities toward depression care. The practice score was computed with the sum of the 10 items and ranges between a minimum of 10 and a maximum of 50. A practice score of at least 25 is required for good depression care practices, while a score below 25 is considered poor practice. The scale displayed high internal consistency with a Cronbach alpha coefficient of 0.89. The third part investigated the extent of agreement of pharmacists with statements related to their attitudes toward depression care on a 5-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). The attitude scale encompassed three subscales related to attitudes toward the disease (10 items), attitudes toward patients with depression (10 items), and pharmacists’ attitudes toward their role in depression care (10 items). The total attitude score was computed by summing the scores of the three subscales and ranges between a minimum of 30 and maximum of 150. Attitudes score of at least 75 is required for positive attitude toward depression care, while a score below 75 is considered negative attitude. The total attitudes scale demonstrated high internal consistency with a Cronbach alpha coefficient of 0.93. Statements that indicated higher levels of practice and more positive attitudes received higher scores. Lastly, the fourth part was designed to identify perceived barriers and addressed possible approaches that might help to overcome barriers toward depression care. A list of barriers (such as insufficient time to be given to each patient, inadequate mental health education, insufficient data about patients/treatment, absence of private counseling area in the pharmacy. . .) and a list of approaches (such as align efforts with broader strategies, specialized training programs for pharmacists, awareness campaigns. . .) to overcome barriers were provided. The participants were asked to add other barriers or strategies they consider relevant or appropriate.
Statistical analysis
Data were analyzed using the IBM Statistical Package for Social Sciences program version 25 (IBM-SPSS Statistics 25). A descriptive analysis was performed using absolute frequencies and percentages for categorical variables and means with standard deviations for quantitative variables. Cronbach alpha was used to test for the internal consistency of the scales used. Bivariate analysis was conducted to assess the association between practice and attitudes scores with various sociodemographic and professional characteristics. Bivariate analysis utilized independent sample T-test for the comparison of two groups, and one-way ANOVA for the comparison among multiple groups. The Levene’s test was applied to assess variance homogeneity, resorting to the corrected T-test when variances were not homogeneous. Post-hoc analysis was performed to identify which groups significantly differ among multiple groups. Additionally, the Pearson correlation coefficient (r) was used to compare continuous variables. Linear regression analysis was performed taking the practice and attitudes scores as the dependent variables. All the predictor variables that showed a p-value < 0.2 in the bivariate analysis were included in the models. The significance level was set at p < 0.05, with a predetermined margin of error of 5%.
Results
Socio-demographic and professional characteristics of the participants
A total of 275 Lebanese community pharmacists participated in this study. The mean age of the participants was 31.37 ± 6.66 years with more than half of them being females (57.1%). The majority are pharmacy employees (69%) residing in the South of Lebanon (54.2%) followed by Beirut (32%). Most of the pharmacies have two pharmacists employed (54.5%), with one pharmacist working in each shift (68.4%). Furthermore, 7.3% of the investigated pharmacists reported suffering from a mental health illness, and 19.6% declared having a family member or friend with a mental health illness. However, only 16.4% of the participants work in pharmacies with a private confidential counseling area.
Around half of the studied pharmacists reported a community pharmacy experience of 5–10 years (48%). They mostly encountered 50–100 clients per day (48%), with the majority spending an average of 5–8 h per day in the pharmacy (80.4%). Most of the pharmacists processed 20–30 prescriptions per day (52%), and the bulk (77.1%) dispensed weekly prescriptions of 1%–10% anti-depressants content. Table 1 summarizes the sociodemographic and professional characteristics of the participants.
Socio-demographic characteristics of the participants.

Community pharmacists’ practices toward depression care
The pharmacists’ involvement in depression care practices was good with a total score of 32.06 ± 8.69. The most frequently practiced activities were providing information about depression (38.5%) and providing verbal counseling about anti-depressants (38.5%). The only two activities that were “rarely” implemented among the majority of pharmacists were following up with patients on anti-depressant medications (34.2%) and screening patients for major depression or other mental health illnesses (37.8%). The community pharmacists’ practices toward depression care are illustrated in Table 2.
Community pharmacists’ practices toward depression care.

Pharmacists’ attitude toward depression care
Community pharmacists enrolled in this study demonstrated positive attitudes toward depression care with a total score of 108.32 ± 20.48. The highest mean score among the three subscales was for pharmacists’ attitudes toward their role in depression care (38.48 ± 6.01), followed by the attitudes toward the disease (35.94 ± 8.59) and the lowest for attitudes toward patients with depression disorder (30.87 ± 7.22).
Pharmacists generally endorsed a relatively positive attitudes toward depression nature, treatment and causes, which was evident in seven out of 10 items listed in this subscale. However, the majority disagreed that “there will be periods of depression and periods of improvement” (40.7%), and that “antidepressants are effective in managing depressive symptoms” (59.6%). Also, most pharmacists agreed that “weakness of character can cause depression” (81.5%) reflecting a negative attitude in this instance. As for attitudes toward patients with depression, items that most of the pharmacists agreed on were “anyone can have depression” (80.7%), and that “patients with depression do not put unnecessary strain on the pharmacist” (52.7%). However, most pharmacists agreed that “patients with depression have themselves to blame” (60.4%) and around one-quarter believed that “depression patients are unreliable” (26.9%) and that antidepressants change the patients’ personalities” (27.2%); hence, revealing negative attitudes toward patients with depression. The pharmacists’ attitudes toward their role in depression care was mostly positive with the majority agreeing on 9 out of 10 items listed in this subscale. Nevertheless, 34.6% of the pharmacists believed that “patients with depression do not want to talk about their disease with pharmacists.” The distribution of responses on the attitudes’ subscales are shown in Table 3.
Community pharmacists’ attitudes toward depression care.

Reversely coded items (1 = strongly agree; 2 = agree; 3 = neutral; 4 = disagree; 5 = strongly disagree).
Factors associated with pharmacists’ practices and attitudes toward depression care
Bivariate analysis
Higher practices scores were significantly found among pharmacists working in pharmacies with at least three employees (p = 0.002), or having more than two pharmacists working in one shift (p = 0.01), those encountering more than 10% of weekly prescriptions containing anti-depressants (p = 0.005), and those reporting a mental health illness (p = 0.006) or having a family member or friend with mental health illness (p = 0.006). In addition, higher total attitudes score (p < 0.001) was significantly associated with higher practices score.
Besides, higher attitudes scores were found among pharmacists having less than 5 years of community pharmacy experience (p < 0.001), those encountering less than 50 patients per day (p = 0.003), those suffering from a mental illness (p = 0.007) or having a family member or friend with mental health illness (p < 0.001) and among pharmacists working in pharmacies with a private counseling area (p = 0.021). The bivariate analysis table is available in the Supplemental Material.
Multivariable analysis
The results of the two linear regression analysis models with the practices and the attitudes scores as the dependent variables are displayed in Table 4. Community pharmacists with higher attitudes scores were significantly more involved in depression care activities with practices scores of 8 units higher as compared to those with lower attitude scores (beta = 8.079, p ≤ 0.001). Furthermore, practices scores increased significantly with the increasing percentages of weekly prescriptions that contain antidepressants whether 1%–10% of antidepressants content (beta = 3.160, p = 0.047) or more than 10% of anti-depressants (beta = 2.829, p = 0.019) as compared to weekly prescriptions with less than 10% of antidepressants.
Multivariable analysis.

Reference group.
Female pharmacists showed significant but slightly higher attitudes scores by 0.165 units as compared to male pharmacists (p = 0.002). In addition, there were positive significant associations between higher attitudes scores and having a family member or friend suffering from a mental illness (beta = 2.239, p = 0.001), and having a private counseling area (beta = 11.183, p = 0.01). On the contrary, pharmacists with more than 10 years of community experience (beta = −20.369, p = 0.021) and those encountering a higher number of patients per day (beta = −7.243, p = 0.001) have significantly lower attitude scales.
Pharmacists’ perceived barriers toward depression care
The top four perceived barriers to depression care reported by the community pharmacists were insufficient time to be given to each patient (48.7%), inadequate mental health education (46.9%), insufficient data about patients/treatment (41.5%), and absence of privacy in the pharmacy (37.1%). Figure 1 illustrates the participants’ perceived barriers toward depression care.

Pharmacists’ perceived barriers toward depression care.
Overcoming barriers to depression care
The top three perceived approaches to overcome barriers for optimization of depression care, as reported by the participants, were aligning efforts with broader strategies for improving the care of other chronic conditions (37.5%), specialized training programs for pharmacists (36.4%), and awareness campaigns about depression and the importance of seeking help (35.6%). Figure 2 represents the different approaches that community pharmacists perceived to overcomes barriers for adequate depression care.
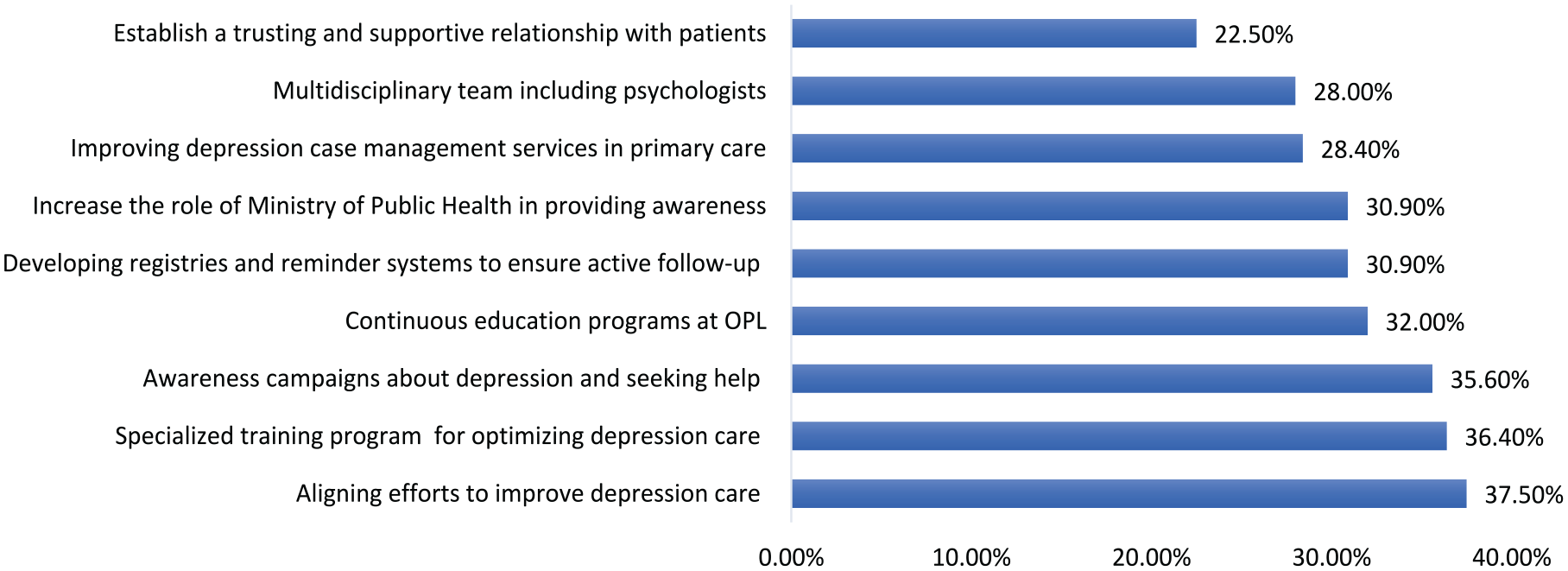
Pharmacists’ approach to overcome barriers to depression care.
Discussion
Despite the huge impact of depression on patients and society,2,28 there is still a lack of emphasis on depression care in Lebanon. The high prevalence of depression along with the current crises and challenges in Lebanon, necessitates the urgency of addressing this issue and the need for involvement from various healthcare professionals, including pharmacists.17,20 The findings of this study provide insights on how Lebanese community pharmacists view depression care including their practices, attitudes, and perceived barriers. The study revealed a good engagement and relatively positive attitudes of community pharmacists in Lebanon toward depression care. Nevertheless, the findings revealed remarkable gaps suggesting several areas for improvements and interventions to optimize depression care.
Community pharmacists in this study demonstrated a good level of involvement in depression care practices. Contrary to our results, most Qatari pharmacists reported not to be actively involved in any of the depression-related activities described in the literature. 29 Moreover, other studies in some developed countries have also revealed that pharmacists are not providing basic pharmacy services needed by depression patients.22,23 Pharmacists’ variable involvement in depression care practices can be explained by the organizational and environmental barriers related to the nature of the healthcare system in each country. Although providing information about depression and antidepressants was common practice as reported in this study, activities such as following up with patients and screening for mental health illnesses were infrequently implemented. Unlike our findings, a study have demonstrated that Bulgarian pharmacists were able to detect mild to moderate depression in 55% of the tested patients. 30 Actually, screening for depression and patients’ follow-up are key roles of pharmacists in depression care. 14 Hence, those tasks that should receive more attention from Lebanese community pharmacists.
This study revealed, as well, greater engagement in depression care practices among pharmacists with higher attitudes scores. The results align with research papers from other countries.15,22,26,29,31,32 Indeed, having positive attitudes toward depression care may motivate pharmacists to actively participate in providing support and assistance to patients with depression.13,15 Additionally, the study demonstrated higher practices scores among those exposed to higher weekly prescriptions containing antidepressants, emphasizing the influence of practical exposure to antidepressants on pharmacists’ active participation in depression care activities.
Community pharmacists participating in this study exhibited relatively positive attitudes with a favorable inclination toward pharmacists’ role in depression care. In concordance with our results, various studies from Qatar, 29 Egypt, 16 Kingdom of Saudi Arabia, 33 and Belgium, 26 reported high self-efficacy and positive perceptions of community pharmacists toward depression care. However, there were discrepancies in the attitudes toward patients with depression, with some pharmacists holding negative beliefs such as attributing depression to personal weakness or perceiving patients as unreliable. These findings highlight the importance of targeted interventions to address misconceptions and stigma surrounding depression among pharmacists. 34
Female pharmacists exhibited significantly higher attitudes scores compared to male pharmacists. Though the difference was relatively small, this might suggest a potential gender-related difference in pharmacists’ perception of depression care. Contrary to our results, regional studies have found that female pharmacists have higher stigmatization views toward depression.35,36 Nevertheless, there is no conclusive evidence regarding the effect of gender on attitudes toward depression 37 and further research exploring this gender disparity may be warranted. Moreover, pharmacists having a family member or friend suffering from mental health issues showed significantly higher attitudes scores. In fact, pharmacists’ experiences of depression within their social circles decreased their distance from patients, 38 as they foster greater empathy and understanding toward patients with depression. 13 Additionally, the presence of a private counseling area was positively associated with higher attitude scores. Unlike developed countries, pharmacies in Lebanon are not mandated to have a private counseling area. However, an adequate infrastructure within the pharmacy can empower pharmacists to provide confidential patient care and improve their willingness to engage in depression care activities. 39 Conversely, pharmacists with more community pharmacy experiences and those encountering more patients per day exhibited significantly lower attitudes scores. Pharmacists with extensive experience or high workload may face greater challenges or burnout that might reflect negatively on their attitudes and willingness to engage in patient care. A study from the United States revealed that 75% of community pharmacists experience burnout due to job demands and working conditions. 40 Also, an alarming prevalence of burnout was revealed among Lebanese community pharmacists. 41 This warrant policy interventions to reduce burnout levels as community pharmacists’ workload might impact the quality of their patient-care services.
This study revealed that insufficient time, inadequate mental health education, and privacy concerns were among the top barriers reported by pharmacists. The results are in agreement with findings from Qatar, 29 Egypt, 16 and Belgium. 25 Accordingly, these findings emphasize the need for systemic changes to reduce the burnout, address structural barriers and create a supportive environment for pharmacists to engage effectively in depression care activities. In addition, several studies have identified lack of remuneration as an important barrier to patient care provision by pharmacists. 42 This barrier was not mentioned by the participating pharmacists in this study, as community pharmacists in Lebanon are generally not being paid for any patient care services that they provide. Paying for pharmacy services including depression care could provide an incentive or motivation for community pharmacists to involve more and invest in these services. One of the approaches reported by community pharmacists in this study to address barriers, was aligning depression care with broader chronic disease management initiatives. This allows pharmacists to utilize existing resources and infrastructure to enhance the delivery of depression care services. Also, specialized training programs for pharmacists were highlighted since training correlates positively with the pharmacists’ confidence to offer services related to depression care. 22 For instance, a Mental Health Academy was established by the department of psychiatry at the American University of Beirut to provide culturally sensitive rigorous training for healthcare professionals and stakeholders in Lebanon and the Arab region. 43 However, such a training program was a one-off initiative rather than an ongoing effort and is limited to healthcare professionals excluding the general public. Hence, more continuous training initiatives for both the Lebanese healthcare professionals and the public is required similar to the Mental Health First Aid program in Australia that provides training to pharmacists and the general public. 44 Such initiatives would improve the competencies, skills, and confidence of Lebanese pharmacists in providing depression care. In addition, awareness campaigns aimed at reducing stigma and promoting help-seeking behaviors were suggested as they advocate for public education. Furthermore, Lebanese community pharmacists can adopt several strategies to overcome the absence of private counseling areas including scheduling consultations during off-peak hours, designating quiet zones, employing digital platforms for confidential consultations, or utilizing written materials.
Limitations
The current study has a number of limitations, even though it is the first to examine community pharmacists’ practices and perceptions of depression care in Lebanon. There is potential for selection bias, as pharmacists more concerned about depression patients may have been more inclined to participate. In addition, the cross-sectional study design does not allow the behavioral analysis over time nor help determine cause and effect relationships. Another limitation could be due to social desirability bias as participants may report what they think researchers want to see. Moreover, non-response bias was not measured, potentially skewing results toward more positive attitudes and practices. Furthermore, the study’s representativeness might be compromised as a significant portion of the participants were from the south of Lebanon. Also, the relatively small sample size might further limit the generalizability of the results.
Conclusion
This study highlights the significant yet underutilized role of Lebanese community pharmacists in depression care. Lebanese community pharmacists demonstrated good practices and positive attitudes toward depression care. However, several barriers were identified such as time constraints, inadequate training, and lack of private counseling areas. Addressing these obstacles through continuous professional training, policy reforms, and structural improvements is vital to enhancing pharmacists’ contributions to depression care. Future research should explore patient perspectives and interdisciplinary collaborations to further optimize depression care delivery in Lebanon.
Supplemental Material
sj-docx-1-phj-10.1177_22799036251349641 – Supplemental material for Practices, attitudes, and perceived barriers toward depression care among community pharmacists in Lebanon
Supplemental material, sj-docx-1-phj-10.1177_22799036251349641 for Practices, attitudes, and perceived barriers toward depression care among community pharmacists in Lebanon by Iqbal Fahs, Mariam Dabbous, Faten Ezzeddine, Sahar Nasser, Jana K AlWattar, Jihan Safwan, Fouad Sakr and Mohamad Rahal in Journal of Public Health Research
Footnotes
Author contributions
I.F., M.D., J.S., F.S., and M.R. conceptualized the study. I.F. had the responsibility of the project administration, planned the methodology, and carried out the statistical analyses. I.F., F.E., S.N., and J.W. wrote the manuscript text. All authors reviewed and edited the text, and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.