
Abstract
Background:
The misuse of antibiotics is fueling antimicrobial resistance (AMR), a critical public health threat. In settings of severe economic crisis, these challenges are often amplified, impacting public access to and appropriate use of medications. This study assessed the knowledge, attitudes, and practices (KAP) of the Lebanese population regarding antibiotic use and AMR, contextualized within the nation’s ongoing economic crisis.
Design and Methods:
A cross-sectional study was conducted from July to December 2023 using an anonymous questionnaire distributed online and in-person across Lebanon. Data were analyzed using t-tests, ANOVA, and Pearson correlation.
Results:
Among 409 participants, significant knowledge gaps and common misconceptions were evident: only 44.74% knew antibiotics are ineffective against viruses, just 24.69% recognized the lethality of AMR, and many incorrectly used antibiotics for a fever (36%) or cough (26.41%). Critically, these knowledge gaps translated into high-risk behaviors shaped by the economic crisis; 42.06% reported financial constraints influenced their antibiotic use, leading to cost-avoiding practices like using leftover medications (41.81%) and sharing them (31.05%). Demographically, higher educational levels and female gender were associated with better knowledge (p = 0.043 and 0.010, respectively). Statistically, a moderate positive correlation was found between knowledge and practice (r = 0.455, p < 0.001), linking lower knowledge to riskier behaviors.
Conclusions:
This study reveals a dual challenge in Lebanon: widespread misconceptions about antibiotics are compounded by economic pressures that shape patient behavior. Our findings indicate that financial constraints directly influence antibiotic access and self-medication practices. Therefore, effective interventions require a two-pronged approach: strengthening public health education to address knowledge gaps, while simultaneously developing policy solutions to ensure equitable antibiotic access and mitigate the impact of economic hardship on appropriate use and the fight against AMR.
What this study adds
This is the first study to reflect the impact of economic crises on antibiotic consumption, showing that financial difficulties led 42.06% of participants to reduce antibiotic use.
The study provides insights into the knowledge, attitudes, and practices regarding antibiotics among the Lebanese population, covering all regions across Lebanon.
A significant portion of the population lacks adequate knowledge about antibiotics, with misconceptions such as the belief that antibiotics are effective against viruses and should be used for symptoms like fever and cough.
Implications of the study on policy and practice
Public health interventions should target misconceptions about antibiotic use, focusing on education regarding their ineffectiveness against viral infections.
Stricter regulations are needed to limit self-medication, including measures to restrict access to antibiotics without proper medical guidance.
Healthcare providers should be encouraged to conduct educational campaigns to improve public knowledge on the safe use and disposal of antibiotics, thereby reducing the risks associated with antimicrobial resistance.
Introduction
The widespread and injudicious use of antibiotics without adherence to evidence-based and protocol-driven medicine has resulted in the emergence of a significant challenge, which is Antimicrobial Resistance (AMR).1,2 This occurs when microbes evolve resistance to standard treatments, making medicines less effective and infections more difficult to treat and prevent.3,4
Antimicrobial resistance represents an urgent global crisis and an established public health threat, a status recognized by the World Health Organization (WHO). Far from an emerging risk, this “Silent Pandemic” is a current reality responsible for millions of deaths worldwide.1,5 Global estimates indicate that the number of deaths directly attributable to AMR reached over 1.2 million in 2019. Without adequate measures to control AMR, the WHO report on antibiotic resistance projects that this figure could surge to around 10 million deaths annually by the year 2050. 6
The multifaceted nature of AMR progression necessitates the adoption of the One Health approach, a unified framework recognizing the intrinsic linkage between human, animal, and environmental health. This approach informs comprehensive mitigation strategies by targeting the drivers of resistance across each domain.
In human medicine, this involves optimizing clinical prescribing practices; including appropriate drug selection, dosing, and duration; and addressing patient behaviors such as self-medication. In the animal sector, it requires regulating antibiotic use in agriculture and aquaculture for growth promotion and disease prophylaxis. Finally, it addresses the environment as a critical reservoir for resistant genes, focusing on strategies like the proper disposal of unused medications to prevent the contamination of soil and water systems with selective antibiotic residues.4,7
Within the human medicine domain, the drivers of antibiotic misuse are complex, reflecting a dyadic interaction between patient behaviors and clinical prescribing practices. Patient-driven factors include non-adherence to prescribed regimens, such as premature treatment cessation upon symptomatic improvement, and the practice of self-medication.8,9 Concurrently, prescriber decision-making is a significant contributor; in clinical settings with limited consultation times or diagnostic resources, there may be a lower threshold for issuing an antibiotic prescription. Furthermore, a physician’s prescribing habits can be influenced by the need to manage perceived patient expectations for medication.10–12 This interplay between patient non-adherence and suboptimal prescribing patterns can culminate in treatment failure and the selection of more resistant microbial strains. 7
These challenges are exacerbated by systemic issues in many Arab nations. For instance, a recent study conducted in the infectious diseases department encompassing seven Arab nations revealed that 28.3% of hospitalized patients were affected by infections, with 98.2% of these patients receiving antibiotic therapy. Moreover, certain Arab countries permit over-the-counter availability of antimicrobials, including substandard generic versions, with minimal prescription regulations in community settings. Furthermore, in some Arab countries, particularly those in regions of political conflict such as Lebanon and Syria, there is a significant presence of low-quality generic antibiotics in the market. 13
With the number of antibiotic resistances increasing worldwide, a global effort has been implemented to decrease this burden, leading to the development of several precautions regarding how antimicrobial agents are dispensed to the public. In Lebanon, a country with a complex healthcare system composed of both public and private institutions and influenced by variable socioeconomic, multicultural, and religious factors, these challenges are particularly pronounced. 14 Previous antibiotic resistance-based research in Lebanon reveals the presence of the same principal issues of antibiotic misuse as seen internationally, where significant knowledge gaps have also been identified in regions like Southeast Asia and Europe.15,16
The threat of AMR extends far beyond clinical outcomes, posing a significant danger to global economic stability. International bodies, including the World Bank, have forecasted that without effective containment, AMR could reduce the annual global Gross Domestic Product (GDP) by as much as 3.8% by 2050, pushing millions into extreme poverty. This economic burden manifests through increased healthcare expenditures, prolonged hospital stays, and losses in labor productivity, straining even the most resilient health systems. 17
This global economic threat is critically amplified in Lebanon, a nation grappling with one of the most severe economic crises in modern history. Since 2019, the country has experienced a catastrophic financial collapse, characterized by a GDP contraction of over 40%, hyperinflation that has decimated the value of the local currency, and the disintegration of the banking sector. This has led to a dramatic decline in public and private spending on health, leaving the healthcare system under-resourced and fragmented.18,19
The convergence of this profound economic crisis with persistent political instability has had a direct and detrimental impact on antibiotic access and use in Lebanon. The state’s diminished capacity for regulatory oversight has weakened controls over the pharmaceutical market, while currency devaluation has made high-quality, imported antibiotics prohibitively expensive for a large segment of the population. Consequently, there is an increasing reliance on cheaper, often lower-quality or inadequately regulated generic alternatives. These conditions foster an environment where patients may be unable to afford a full course of treatment and where the integrity of the medication supply chain is compromised, creating a fertile ground for the acceleration of AMR.20–22
In response to this escalating threat, Lebanon has initiated several strategic actions, although their implementation has been challenged by ongoing socio-economic pressures. A key component of the national strategy was the development of the National Action Plan (NAP) for Combating Antimicrobial Resistance (2019–2023). 23 This multi-sectorial plan, guided by the “One Health” approach, brought together the ministries of health, agriculture, and environment to address the multifaceted nature of AMR. Its core objectives included strengthening surveillance, improving public and professional awareness, and promoting infection prevention and control. 23 On the clinical front, the Lebanese Ministry of Public Health has mandated the implementation of Antimicrobial Stewardship Programs (ASPs) through its hospital accreditation process. 24 Consequently, many healthcare institutions have established ASPs to optimize antibiotic prescribing, and professional bodies, such as the Order of Pharmacists of Lebanon (OPL), have launched educational initiatives to empower community pharmacists in this domain. 25 These efforts are complemented by periodic public awareness campaigns, often aligned with the World Antimicrobial Awareness Week, aimed at educating the general population on the appropriate use of antibiotics. 26
Despite these top-down initiatives, research exploring the public’s knowledge, attitudes, and practices (KAP) on antimicrobial use reveals significant inadequacies specifically within the Lebanese context. Multiple studies conducted in Lebanon have consistently highlighted critical gaps in public understanding and behavior.14,27–29 For instance, a substantial portion of the population incorrectly believes that antibiotics are effective against viral infections like the common cold, and practices such as self-medicating, storing antibiotics for emergencies, and not completing the full prescribed course remain widespread.28,29 This is further evidenced by studies showing that non-health-related university students demonstrated suboptimal KAP scores, indicating a significant knowledge gap. 30 These locally-observed deficiencies in public knowledge and practice underscore the deep-rooted challenges that national strategies must overcome to effectively reduce the spread of AMR in Lebanon.
These findings highlight the urgent need for a One Health approach, which recognizes the interconnectedness of human, animal, and environmental health in addressing AMR. In the context of Lebanon, where over-the-counter antibiotics are available, political instability persists, national-level AMR data is limited, and low-quality generic antibiotics are often favored, further studies are crucial. These studies should adopt a One Health perspective, investigating not only human antibiotic use but also its interplay with veterinary practices and environmental factors, to comprehensively address the complex challenge of AMR in the country.
Aligning national efforts with international frameworks is crucial for success. The WHO Global Action Plan provides a roadmap, calling for a multisectoral response to combat AMR. This plan emphasizes the need to improve public awareness (Strategic Objective 1), strengthen the evidence base through surveillance (Strategic Objective 2), and optimize the use of antimicrobial medicines (Strategic Objective 4). Fulfilling these objectives in Lebanon requires targeted research that can generate the necessary local data and insights, especially given the country’s unique challenges. 31
Therefore, the primary aim of this study is to provide a recent, comprehensive examination of the KAP of the Lebanese population regarding antibiotic use and AMR, particularly within the context of the nation’s severe economic crisis.
Methods
Study design
This cross-sectional study collected data between May 2023 and December 2023 using a self-administered, anonymous questionnaire. The data collection strategy was twofold. First, an electronic version of the questionnaire was created using Google Forms and distributed online by sharing the link on various social media networks. Second, for in-person data collection, printed paper copies of the same questionnaire were distributed to participants at community pharmacies and primary healthcare centers.
Inclusion and exclusion criteria
The study included adult individuals aged 18 years and above who reside in Lebanon. Participants were required to be non-healthcare providers (HCPs) to ensure the sample reflects the general public’s KAP regarding antibiotic use. To enforce this, a screening question was implemented at the beginning of the questionnaire to identify and exclude HCPs prior to their participation, thereby avoiding potential bias from their specialized professional knowledge on the study outcomes.
Sample size
The sample size was calculated using Raosoft®, an online sample size calculator, which determined that a minimum of 385 participants was needed to obtain a representative sample with a 95% confidence level and a 5% margin of error.
Questionnaire development and data collection
The development and validation of the questionnaire followed a multi-stage process to ensure its relevance, clarity, and reliability.
Content development and validation
The initial pool of questions was adapted from previously published international studies investigating knowledge, attitudes, and practices related to antibiotic use and resistance.14,16,32 To ensure high content validity for the local context, this draft was then rigorously refined using the Delphi method. This structured technique involved five iterative rounds of anonymous feedback with a panel of experts in the field. After each round, feedback was collated, summarized, and redistributed to the panel. This process continued until a high degree of consensus was reached on the relevance, appropriateness, and comprehensiveness of the items for achieving the study’s objectives.
Clarity assessment and pilot testing
After the questionnaire was developed in English, it was translated into Arabic, the native language of the target population. To assess the clarity, comprehensibility, and length of the translated instrument, pilot testing was conducted with 20 participants. These participants were representative of the study population, and their data were excluded from the final analysis. Feedback from the pilot phase was used to make minor adjustments to the wording and formatting, ensuring the final questions were unambiguous and easy for respondents to understand.
Reliability analysis
To evaluate the internal consistency and reliability of the questionnaire’s main scales, Cronbach’s alpha (α) was calculated for each section. Knowledge Section: α = 0.82, Attitude Section: α = 0.79, and Practice Section: α = 0.76.
Final questionnaire structure
The final, validated questionnaire was structured into four distinct sections. The first section collected demographic information through six questions. This was followed by the knowledge section, which contained 15 yes/no and true/false questions to assess participant understanding of antibiotic use and AMR. The third section evaluated attitudes using 10 yes/no questions on topics such as completing antibiotic regimens, handling missed doses, and self-medication. Finally, the fourth section examined practices with seven multiple-choice questions regarding antibiotic use in the past 6 months, common reasons for use, prescribers, disposal of leftovers, and the impact of the economic crisis on usage patterns.
Data quality assurance
During data collection, several measures were implemented to ensure data quality. For paper-based questionnaires distributed in person, research assistants checked for completeness upon collection. For the online Google Form, key questions were set as “required” to prevent incomplete submissions. All collected data were subsequently reviewed for logical inconsistencies or outliers before the final statistical analysis.
Data analysis
Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to describe the demographic information and the knowledge, attitude, and practice data of the study participants.
Participant responses in the KAP sections were scored to facilitate quantitative analysis. A score of 1 point was assigned to each correct answer, while incorrect/inappropriate or “I don’t know” answers received a score of 0 points. This method yields a summative score for each domain, where a higher total reflects a greater level of knowledge or more appropriate practices. This objective, dichotomous scoring protocol is a standard convention in KAP research and is consistent with the methodology used in numerous previously validated studies on AMR.33–35
Normal distribution of continuous variables, including KAP scores, was verified mainly by visual inspection of histograms, Q-Q plot, and absolute values less than 1.96 for skewness and kurtosis. Moreover, the Shapiro-Wilk test with a non-significant p-value (> 0.05) was used to confirm normality.
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS®) version 27. After verifying normality and homogeneity of variances using Levene’s test, bivariate analyses were conducted. Specifically, independent samples t-tests were employed to compare mean KAP scores between binary demographic groups (gender, presence of comorbidities), while one-way ANOVA with Bonferroni post-hoc analysis was used to compare mean KAP scores across sociodemographic variables with more than two categories (age groups, educational level, residency region, and medical coverage). Also, Pearson’s correlation test was applied between the scores. A p-value of less than 0.05 was considered statistically significant.
As for the multivariable analysis, multiple linear regressions were conducted using the General Linear Model (GLM) multivariable MANCOVA framework. This approach assessed the association of various independent variables with the KAP scores simultaneously.
All relevant sociodemographic and other independent variables were included in the model. The model’s validity was confirmed by verifying key assumptions, including the linearity of relationships, normality of residuals, homoscedasticity, and the absence of multicollinearity. For each predictor, the results are presented as beta coefficients (β) with their 95% confidence intervals (CI) and corresponding p-values.
Results
Participants characteristics
A total of 500 individuals were invited to participate in the study. However, only 409 consented and completed the surveys, resulting in a response rate of 81.8%.
The demographic characteristics of the study participants are summarized in Table 1. Among the total sample, almost one-third of the participants (29.83%) were aged between 37 and 50 years, and the majority (65.04%) were female. In terms of educational attainment, more than half of the participants (61.86%) held a Bachelor’s degree. Geographically, a significant proportion of respondents (58.92%) were from Beirut. Regarding healthcare coverage, most of them (69.44%) reported having medical insurance. Additionally, just over half of the participants (50.61%) did not report any chronic illnesses.
Demographic characteristics of the participants.

Knowledge part
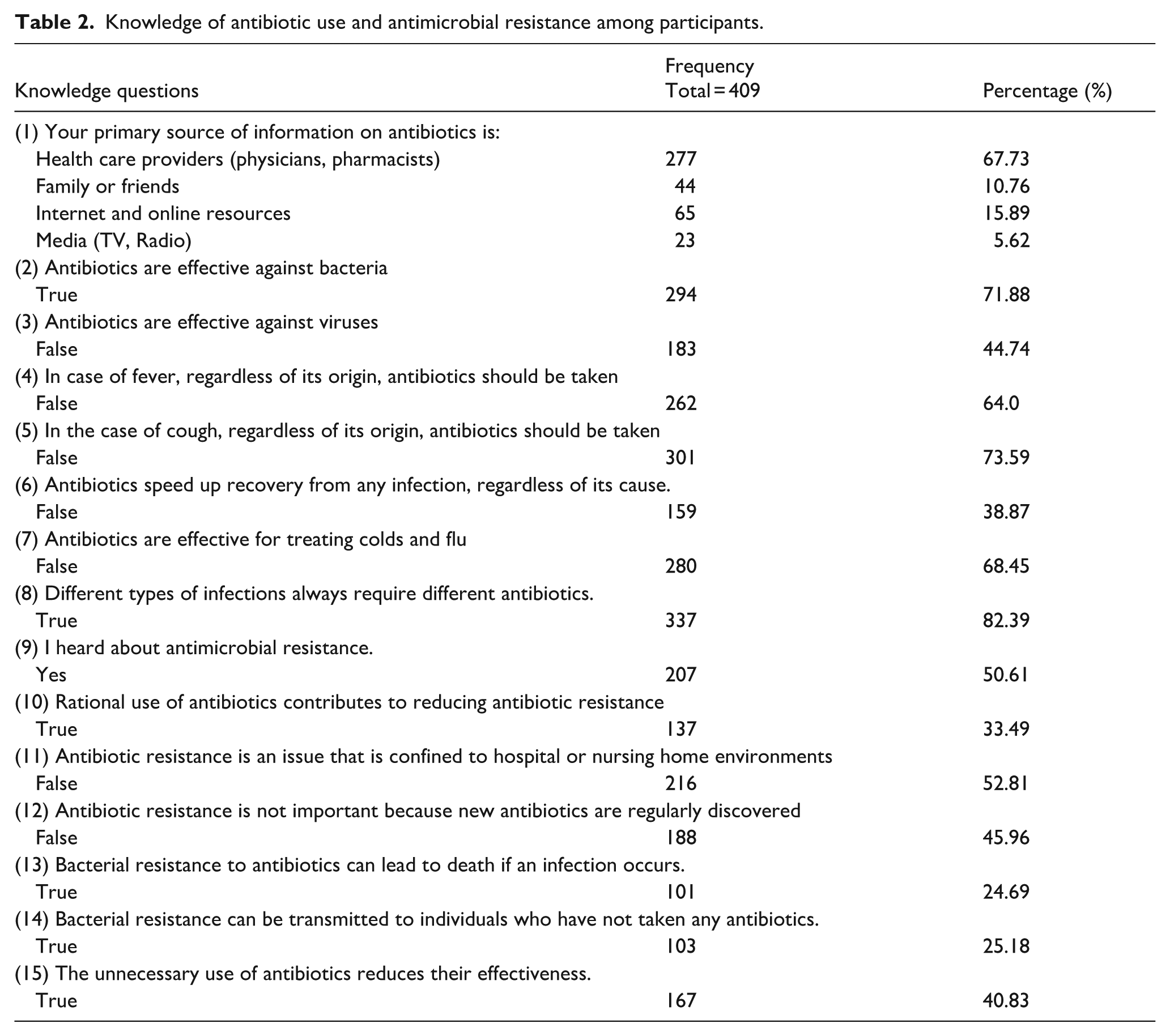
Table 2 presents the responses of participants on knowledge-related questions, including the correct answers. HCPs were the primary information source on antibiotics for 67.73% of participants. The majority (71.88%) of participants understand that antibiotics are effective against bacteria. However, only 44.74% recognize their ineffectiveness against viruses. Concerningly, 36% and 26.41% still believe antibiotics should be taken for fever or cough, respectively, regardless of cause. Awareness of AMR is particularly low, with only 24.69% recognizing its potential to cause death and 25.18% understanding that resistance can spread to others. Only 33.49% of participants understand that rational antibiotic use helps combat AMR, and just 45.96% are aware that new antibiotics are not regularly discovered. Moreover, almost half (50.61% and 59.17% respectively) of participants have heard about AMR, and are unaware that unnecessary antibiotic use reduces their effectiveness.
Knowledge of antibiotic use and antimicrobial resistance among participants.
Attitude part
The survey results on attitudes toward antibiotic use reveal a mix of correct understanding and concerning misconceptions. Positively, a large majority (88.75%) trust their doctor’s decisions about antibiotic prescriptions, and 85.57% recognize the importance of completing a full course of antibiotics. However, several problematic attitudes are prevalent. A significant portion (41.81%) believe it’s safe to keep and reuse leftover antibiotics. Alarmingly, 31.05% think it’s appropriate to share antibiotics with family or friends who have similar symptoms, although fewer (10.02%) consider it appropriate for different symptoms. Many participants (26.41%) believe it’s acceptable to miss a dose, and 37.41% think it’s okay to stop prescribed antibiotics for alternative remedies. Only 46.45% understand that using antibiotics as prescribed helps reduce antimicrobial resistance. The results are demonstrated in Figure 1.

Percentage representation of participants’ attitudes toward antibiotic use.
Practice part
The study shows several important findings about participants’ practices regarding antibiotic use. Only 22.73% of participants reported consuming antibiotics in the past 6 months, with the majority (14.91%) using them once. Notably, 42.06% of participants reported a decrease in antibiotic consumption due to the current economic crisis, primarily citing higher prices as the reason. The majority (88.5%) stated they would not obtain antibiotics without a prescription if their doctor didn’t prescribe them, and 73.83% claimed they do not use antibiotics without consultation. Doctors remain the main antibiotic prescribers (61.13%), though a significant portion rely on pharmacists (21.76%) or family and friends (17.11%). Concerning disposal practices, only 8% properly return leftover antibiotics to healthcare centers, while many throw them in the bin (42.56%) or store them at home (36.84%). The main reasons for antibiotic use were sore throat (32.17%), influenza and common cold (21.39%), and dental infections (20.34%). The results are presented in Table 3.
Practice-related questions on antibiotic use among participants.

Association between demographic factors and knowledge, attitude, and practice scores on antibiotic use among participants
The study found that educational level and specific medical conditions significantly influenced knowledge about antibiotic use. Participants with only a school education and those holding a bachelor’s degree had lower knowledge scores compared to postgraduates (p = 0.011 and 0.043, respectively). Additionally, females exhibited higher knowledge than males (p = 0.010), while individuals with diabetes demonstrated significantly lower knowledge than those without the condition (p = 0.033).
Attitudes toward antibiotic use were affected by age, gender, and certain medical conditions. Participants aged 37–50 and over 50 showed more positive attitudes compared to those aged 18–25 (p < 0.001). Furthermore, females and individuals with hypertension reported more favorable attitudes (p = 0.014 and 0.021, respectively).
Practices regarding antibiotic use varied by region of residence, with residents of Mount Lebanon displaying lower practice scores than those in Beirut (p = 0.021). The results of the bivariate tests are presented in Table 4.
Association between demographic factors and knowledge, attitude, and practice scores on antibiotic use among participants: a bivariate analysis.
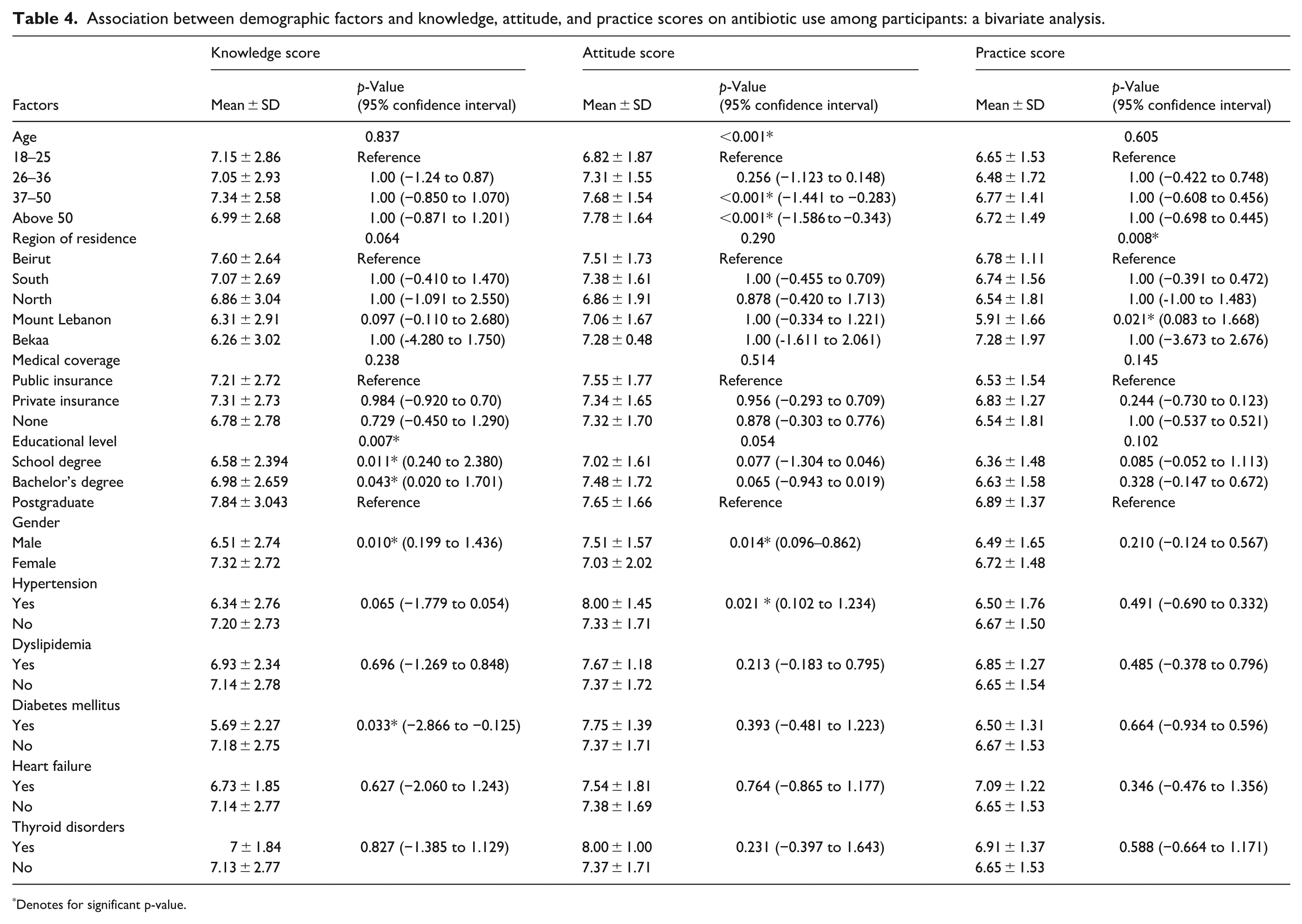
Denotes for significant p-value.
Moreover, the study highlights significant relationships between knowledge, attitude, and practice regarding antibiotic use. A moderate positive correlation (r = 0.455, p < 0.001) was found between knowledge and practice, indicating that greater knowledge about antibiotics is associated with more appropriate use. Additionally, there was a significant low positive correlation (r = 0.156, p = 0.002) between attitude and practice, suggesting that a more favorable attitude toward antibiotics correlates with a higher likelihood of rational use. Finally, the study revealed a weak, non-significant correlation (r = 0.058, p = 0.244) between knowledge and attitude scores, indicating that increased knowledge about antibiotics does not necessarily result in a significantly different attitude toward their use. The results of the correlation tests are summarized in Table 5.
Correlation between knowledge, attitude, and practice scores of participants regarding antibiotic use.

R: correlation coefficient.
Denotes for a significant p-value.
The multivariable analysis identified several significant predictors for KAP scores. A higher knowledge score was associated with being female (β = 0.977). Conversely, lower knowledge scores were linked to residing in Beqaa (β = −2.095) or Mount Lebanon (β = −3.056) compared to Beirut, and with having a school (β = −1.236) or bachelor’s degree (β = −0.934) compared to a postgraduate degree. For the attitude score, younger age (18–25) was the only significant predictor, associated with a lower score compared to those over 50 (β = −0.756). Finally, a lower practice score was significantly associated with residing in Mount Lebanon (β = −1.482) and having a school-level education (β = −0.571). The detailed results are illustrated in Table 6.
Multivariable analysis using the GLM method.

represents the reference group.
Bold represents significant p-values.
Discussion
This study offers a critical snapshot of antibiotic KAP in Lebanon, revealing a public health landscape where persistent, deep-seated knowledge gaps are dangerously amplified by one of the most severe economic crises in modern history. Our findings indicate that while trust in healthcare professionals (HCPs) remains high, this crucial asset is not being fully leveraged to prevent high-risk behaviors like self-medication, premature treatment cessation, or the improper disposal of unused antibiotics. The knowledge deficits observed are, in many ways, a continuation of a challenging regional trend; our finding that only 44.74% of participants correctly identified antibiotics as ineffective against viruses is consistent with previous local studies and mirrors results from neighboring countries.32,36 This knowledge deficit extends beyond the use of antibiotics for viral infections to a more fundamental misunderstanding of the AMR crisis itself. Our findings indicate that public awareness of AMR is critically low and superficial. Although half the population has heard the term, this familiarity does not translate into understanding the threat. For instance, only a minority recognized that AMR could be lethal (24.69%) or transmissible (25.18%), and just one-third (33.49%) knew that rational antibiotic use helps combat resistance. This regional struggle with public understanding, which lags significantly behind that of European nations,37,38 underscores a systemic issue where patient education is often overshadowed by patient expectations for a quick cure and the time pressures faced by clinicians.
However, these behaviors can no longer be analyzed in a vacuum; they are now profoundly shaped and exacerbated by the nation’s ongoing economic collapse. The fact that over 42% of respondents have reduced their antibiotic use due to price increases is a seismic shift, highlighting how cost has become a primary determinant of care. This price sensitivity is acutely magnified by the near-total collapse of Lebanon’s health insurance safety net. Even before 2019, most private insurance plans did not cover outpatient medications, placing the burden on individuals. Post-crisis, public coverage through institutions like the National Social Security Fund (NSSF) has become largely defunct, unable to reimburse patients for purchased medications. This leaves the vast majority of the population facing the full, unsubsidized out-of-pocket cost for medicines, creating a direct barrier to proper care.
This economic reality has fundamentally and perilously altered health-seeking patterns. The prohibitive cost of a physician’s consultation fee alone is enough to deter many from seeking a formal diagnosis. This leads to a predictable cascade of informal care practices: patients may first turn to self-medication with leftover antibiotics from a previous illness, seek advice from family members, or proceed directly to a community pharmacy, bypassing the physician entirely. This positions the community pharmacist as the primary care provider for many, transforming their role from dispenser to diagnostician and counselor. This shift, born of economic necessity, creates a high-risk environment where antibiotics may be dispensed based on symptoms rather than a diagnosis, a practice that directly fuels the development of AMR. This dynamic creates a vicious cycle of poverty and resistance: when patients cannot afford a full course of a quality antibiotic, they may take a suboptimal treatment that leads to a resistant infection, which is then far more difficult and expensive to treat, pushing them deeper into financial distress.
The consequences of this convergence of crises extend beyond patient care and into the environment, directly threatening the One Health framework. Our finding that 42.56% of participants discard antibiotics in regular waste is not merely an individual knowledge gap but a glaring symptom of a systemic failure. Without any national infrastructure for pharmaceutical take-back programs, the public has no responsible alternative. These discarded medications leach into Lebanon’s soil and water systems, creating environmental reservoirs of resistance that can re-enter the human food chain through agriculture and livestock. 39 This environmental degradation completes a dangerous feedback loop, making the fight against AMR exponentially more complex.
These systemic gaps are further reflected in key demographic findings. The fact that women demonstrated significantly higher knowledge scores highlights their crucial role as primary caregivers and health managers within the household. This suggests that while women may be more receptive to public health messaging, men constitute a distinct, harder-to-reach population, necessitating fundamentally different communication strategies to address their specific knowledge deficits. 40
Educational attainment emerged as a key determinant of both antibiotic knowledge and practices. Specifically, individuals with postgraduate qualifications demonstrated significantly higher knowledge scores compared to those with either a bachelor’s or school-level education. This advanced education was also linked to better practice scores when compared to participants with a school degree. This strong association suggests that higher education likely fosters greater health literacy and a more nuanced understanding of appropriate antibiotic use.41,42
Age played a significant role in shaping attitudes, with older participants demonstrating more positive attitudes toward antibiotic use. This finding may be attributed to the fact that older age is often a risk factor for various illnesses, leading to more frequent and sustained interactions with the healthcare system. These repeated encounters provide more opportunities to receive professional guidance from physicians and pharmacists, which can foster more informed and conservative views on antibiotics over time. In contrast, younger participants (18–25 years), who likely have fewer such interactions, represent a key demographic for targeted interventions aimed at improving attitudes toward rational antibiotic use. 43
Regional differences were evident in antibiotic use practices, with residents of Beqaa and Mount Lebanon displaying lower knowledge scores than those in Beirut. This could reflect regional disparities in access to healthcare information or services. Urban areas like Beirut may have better access to healthcare facilities and information, leading to better antibiotic use practices. This finding suggests the need for region-specific interventions to improve antibiotic use practices across different areas of Lebanon. 29
Given this complex interplay of individual behavior, economic desperation, and systemic gaps, a multifaceted and pragmatic response is urgently required.
The following recommendations are designed to be context-specific, moving beyond general advice toward actionable, systemic change. First, community pharmacies must be officially empowered and regulated as centers for ASPs. This requires a two-part approach: the Ministry of Public Health and the OPL should co-develop a mandatory continuing education module focused on patient counseling for AMR, equipping pharmacists with standardized visual aids and communication strategies. Simultaneously, regulatory enforcement against illegal OTC antibiotics sales must be strengthened, shifting the focus from punitive measures to a supportive framework that enables pharmacists to refuse sales while providing safe, evidence-based advice.
Second, a National Medication Take-Back Initiative must be established to address the environmental threat. This program could be launched annually during World Antimicrobial Awareness Week, designating pharmacies, primary care centers, and hospitals as official collection points. Partnering with environmental NGOs and industrial facilities capable of high-temperature incineration would ensure the safe destruction of these hazardous materials, providing a clear, accessible solution for the public.
Third, educational interventions must become more sophisticated and demographically targeted, as generic campaigns are no longer sufficient. Particular focus is needed for reaching younger populations to instill responsible habits early, residents of densely populated urban areas where transmission risks are higher, and, most critically, populations with lower levels of formal education, who demonstrated significant knowledge and practice gaps. Beyond these broad groups, campaigns must also be tailored by gender. Public health initiatives should be designed to empower women as “household health guardians,” providing them with the information and confidence to advocate for rational antibiotic use for their families. To reach men, campaigns should be deployed in non-traditional settings—such as social media channels, sports clubs, or workplaces—using direct messaging that links responsible antibiotic use to personal and family health security.
Finally, any long-term solution must address the root economic drivers. This involves a high-level policy commitment to strengthening national AMR surveillance to track resistance patterns and guide clinical decisions. Critically, Lebanon must leverage international partnerships to secure aid for a subsidized supply of essential, first-line antibiotics. Ensuring that quality medications are affordable and accessible is the only sustainable way to prevent the population from being forced into choices that compromise both their health and the future efficacy of these life-saving drugs.
Limitations
This study has several limitations that should be acknowledged. First, its cross-sectional design limits the ability to assess causality between variables. Additionally, the sample included a smaller number of participants from the Beqaa region compared to other areas, partly due to the fact that the population in Beqaa is smaller than in other regions, which may affect the generalizability of the findings. The study also did not assess the crowding index or the economic status of individuals to reduce respondent discomfort or social desirability bias. Another limitation is the potential for recall bias, which is inherent in the study’s cross-sectional design. Since data on past antibiotic use and adherence were self-reported, inaccuracies in participant memory could have led to an under- or overestimation of certain practices, thereby affecting the validity of our findings.
Despite these limitations, the findings provide valuable insights into the population’s KAP toward antibiotic use and AMR during Lebanon’s economic crisis, highlighting the urgent need for further research to explore associated factors and implement targeted interventions.
Conclusion
In conclusion, this study reveals that Lebanon is facing a perilous convergence of crises, where persistent gaps in public knowledge and high-risk behaviors regarding antibiotic use are being dangerously amplified by a catastrophic economic collapse. Our findings demonstrate that economic constraints are not merely an influencing factor but a primary driver of suboptimal health-seeking behaviors, forcing individuals into a vicious cycle of self-medication, incomplete treatments, and reliance on informal care that fuels AMR. This reality underscores the urgent need for a multi-pronged intervention strategy focused on targeted public education, particularly for younger and less-educated populations; stronger regulation of over-the-counter antibiotic sales; and the establishment of a national program for the safe disposal of unused medications. These evidence-based recommendations align directly with the core objectives of Lebanon’s National Action Plan for Combating AMR, particularly those aimed at improving awareness and optimizing antimicrobial use. Addressing this challenge, therefore, requires a renewed, context-specific commitment from policymakers and public health bodies to implement these critical measures and mitigate the compounded threat to public health.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
The study received ethical approval from the Institutional Review Board (IRB) at Beirut Arab University (approval number: 2023-H-0095-P-R-0611). It was conducted anonymously, ensuring strict patient confidentiality.
Consent to participate
Participants provided their consent before completing the questionnaire and were informed of their right to withdraw from the survey at any time without consequences. Consent forms were included on the first page of the online Google Form and in the written surveys for those who participated in person. Participants who chose not to participate were automatically excluded from the survey.
Author contributions
All authors have read and approved the submitted version and are personally accountable for their respective contributions. DR was responsible for manuscript preparation and data analysis. BM conducted data collection, developed the questionnaire, and composed the initial draft. SH and SD revised and refined the final manuscript and contributed to the study’s questionnaire development and conceptualization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.