
Abstract
Introduction:
The Iraqi pharmacy code of practice and ethics enables pharmacists to resolve conflicts between the code and patient demands and satisfy their needs. This study evaluates pharmacists’ knowledge, attitude, and practice toward the pharmacy code of practice and ethics.
Design and Methods:
This cross-sectional study was conducted in three different provenances (Baghdad, Al-Diwaniya, and Wasit) from October 1st to December 31st, 2022.
Results:
Among 202 Iraqi pharmacists, the mean age was (30.4 ± 6.8) years old, and about (59%) of the participants were aware of the Iraqi Code of Practice and Ethics; similar results were found regarding their practice. About two-thirds of the participants agreed that modifying the Iraqi Pharmacy Code of Practice and Ethics will enable pharmacists to resolve the conflict between the code and patient demands, satisfy their needs, and raise healthcare standards. More than two-thirds of the participants thought that they don’t need training courses to give vaccines for addiction, smoking cessation, obesity, or sleeping problems.
Conclusion:
According to the study, more than half of the Iraqi pharmacists exhibited good knowledge, attitude, and practice regarding the pharmacy code of practice and ethics. However, it is recommended that Iraqi pharmacists engage in comprehensive training programs covering different aspects of healthcare, such as vaccination and smoking cessation, to further improve their contribution to the healthcare system.
Significance for public health
The role of pharmacists in healthcare management varies depending on the country and their code of practice and ethics. Pharmacists effectively use their knowledge and skills in developed countries, while in developing countries, their activities may lack transparency to health policymakers, other healthcare professionals, and patients. Evaluating pharmacists’ knowledge, attitude, and practice regarding the pharmacy code of practice and ethics in Iraq and among low-income, rural, or underserved populations lacks resources. Pharmacists have proven to be beneficial during the COVID-19 pandemic, and their role has been reshaped to meet the needs of patients better. We acknowledge the vital role of pharmacists in healthcare management and appreciate their continued efforts in providing quality care to patients.
Introduction
The code of practice and ethics differs from country to country, so even pharmacist roles would vary. According to the Iraqi Pharmacy Code of Practice and Ethics, number 86 in the Iraqi regulations and legislation, was first created in 1956 and updated six times. The last one was in 1998, which stated that the pharmacist has the right to compose, decompose, supply, and own any drug or chemical that treats humans or animals, with no other services. However, he is prohibited from changing or replacing a medication or changing the dose without referring to the prescriber; also, he is prohibited from making agreements with the prescribers or drug companies. In some developed countries, there is a better understanding of the role of pharmacists in healthcare management and the use of their knowledge and skills. 1 In some countries, especially the US and UK, In the UK, pharmacists receive training to become independent prescribers. Thus, they face new concerns and responsibilities, which need technical skills and consideration of values and relationships. 1 According to the UK code of ethics for pharmacists, there are essential services a pharmacist is allowed to give if he takes the appropriate training; the pharmacists are permitted to offer advice and provide complementary therapies, homeopathic or herbal medicines, domiciliary oxygen services, services to drug misusers, aseptic dispensing services as well as advisory services that apply to any service intended to facilitate the safe, effective, and appropriate usage of medicines, dressings, and appliances, their storage, stock control or disposal. 2 Many pharmacists’ activities to deliver optimum pharmaceutical care to individuals may not be transparent to health policymakers, other healthcare professionals, and patients. Pharmacists are essential in providing comprehensive medication therapy, targeted chronic disease management, and improved medication adherence. Despite pharmacist interventions being shown to improve outcomes and access to care among the sub-population of low-income, rural, or underserved populations.3–9 Nonetheless, pharmacists are rarely integrated into a primary care setting. It is well recognized that primary care services can be a means to improve health outcomes and decrease unnecessary health care utilization. Yet, access to high-quality primary services by low-income, rural, or underserved populations is limited in the current healthcare landscape.10–12 Limited resources were available to evaluate pharmacists’ knowledge, attitude, and practice toward the pharmacy code of practice and ethics in Iraq and low-income, rural, or underserved populations. In a cross-sectional study among pharmacists working in chain community pharmacies in Indonesia, the majority of pharmacists showed a good score in knowledge and attitude, which is in contrast to practice as the majority only obtained a moderate score. 13 However, a mixed-method study conducted at the Tehran University of Medical Sciences recommended raising pharmacists’ knowledge and awareness about pharmacy practice, professionalism, and pharmacy ethics and considering a special place for pharmaceutical consultation. 14 Another cross-sectional study conducted in Zagreb, Croatia found that (94.4%) of Croatian community pharmacists are familiar with the current professional code of ethics in Croatia, but only 47.6% think that the code reflects the changes that the pharmacy profession faces today. 15 In addition, a descriptive-observational cross-sectional study among students of the Pharmacy Faculty of Shiraz University of Medical Science shows a necessity to focus on the development of plans and policies required to perform plans for the teaching of pharmacy ethics to enhance the pharmacist’s ethics in the professional practice of pharmacists. 16 Over the past two decades, there has been a significant surge in the number of pharmacists. Despite this increase, there has been a failure to effectively harness the skills and expertise of these youthful and knowledgeable professionals. This has resulted in a situation where the roles and responsibilities of pharmacists have remained stagnant, even amidst the urgent demands placed on them during the COVID-19 pandemic in Iraq. The country found itself in dire need of pharmacists who could play a critical role, but unfortunately, they were not adequately prepared to fulfill these crucial responsibilities. This study evaluates pharmacists’ knowledge, attitude, and practice toward the pharmacy code of practice and ethics. This study evaluates pharmacists’ readiness to advance their careers, assume more responsibility, and revise the pharmacy’s code of ethics to reflect their broader responsibilities and highlight the barriers that can prevent them from providing healthcare to their patients.
Design and methods
This cross-sectional study was conducted among 202 pharmacists in three different provenances (Baghdad, Al-Diwaniya, Wasit) from October 1st to December 31st, 2022. Pharmacists were asked about their willingness to participate in the study and signed the participant’s consent form; they read and filled out the questionnaire physically and independently.
The researcher developed a new tool called “Questionnaire” to evaluate pharmacists’ familiarity with and their adherence to the Iraq pharmacy code of practice and ethics and whether pharmacists are ready to advance their careers, assume more responsibility, and revise the pharmacy’s code of ethics to reflect their broader responsibilities in addition to highlighting the barriers that can prevent them from providing healthcare to their patients. To ensure face and content validity, the questionnaire was reviewed by six specialized pharmacists, five of whom were faculty members with experience and expertise in survey instrument development and research. Modifications suggested were considered, and changes were made accordingly. Reliability analysis of the questionnaire using Cronbach’s
alpha showed an internal consistency reliability of 0.9. Demographic information was settled, and a few questions related to the pharmacist’s knowledge, attitude, and practice regarding the pharmacy code of practice and ethics were adapted and rephrased according to the aim of the study from the literature review,17,18 some were added according to the Iraqi pharmacy code of practice and ethics19,20 and some were suggested by the experts who reviewed the questionnaire. The questionnaire was evaluated and translated according to the Translation and Cultural Adaptation – Principles of Good Practice. 21 After preparing the questions, the researcher started forwarding translation to Arabic language, reconciliation, back translation, back translation review, harmonization, cognitive debriefing, review of cognitive debriefing results and finalization, proofreading; and the final report was prepared.21,22
The sample was randomly selected from pharmacists in (Baghdad, Al-Diwaniya, and Wasit). Any Iraqi pharmacist with an Iraqi license working in the public or both public and private sectors was eligible to participate in the study if they wished. The data were analyzed using SPSS version 20; the age of the participants and the duration of their work as community pharmacists were presented as mean ± SD. Other variables were categorical and presented as numbers and percentages; the score for each knowledge, attitude, practice, and barrier was calculated, and all the results were presented in tables as appropriate. The KAP and barriers scoring method is illustrated in Table 1.
KAP and barriers scoring according to Bloom’s cut-off point.

The sample size needed for the study was calculated by using the equation below23–26:

Where n = the sample size; Z = the statistic for the 95% level of confidence used in the power analyses, which was 1.96; p = the expected prevalence or the proportion used, which was (7%) = 0.07 according to the world bank Iraq population about 42,000,000 27 and the number of Iraqi pharmacists is about 31,000 pharmacists 28 according to the Syndicate of Iraqi Pharmacists; and d = the precision used, which was 0.035 (according to Niang d = 1/2 p). 29 Applying these values in the equation, the sample size is equal to 192. By adding an extra population to avoid bias and missing data, it will be 202 pharmacists.
Results
Two hundred and two Iraqi pharmacists participated in the study randomly from three different provenances (Baghdad, Al-Diwaniya, and Wasit). Their mean age was (30.4 ± 6.8) years old, which is reasonable compared to the 71.8% of the Iraqi population range 15–64 years old. 30 The mean duration of their work as a community pharmacist was (6.7 ± 6.2) years.
Table 1 illustrates the knowledge data of the participants. About half of the participants were from Al-Dewanya (48%), and the rest were from Baghdad (27.2%) and Wasit (24.2%). Results were found among different genders who participated in the study (males (44.1%) and females (55.9%)).
Table 2 shows that more than half of the participants were aware of the Iraqi code of practice and ethics (58.9%), and similar findings (54%) in those who were aware that pharmacists can’t measure a patient’s blood pressure, blood sugar, or oxygen levels. According to the Code, agreements between a pharmacist and a doctor are prohibited and known by more than two-thirds of the participants (64.4%). Pharmacist is not permitted to substitute a drug prescribed by one brand for another unless the prescribing physician has given his or her consent were known by (56.4%) of the participants.
Study participant’s knowledge (N = 202).

Table 3 shows that about half of the participants (51%) agree that the Iraqi pharmacy code makes it difficult for them to give services. More than two-thirds (60.9%) think that modifying the Iraqi pharmacy code of practice and ethics will enable pharmacists to resolve the conflict between the code and patient demands, satisfaction, and their needs, and raise healthcare standards. More than two-thirds of the participants in this study believed they could administer vaccines, treat addiction and smoking cessation, manage obesity, or address sleeping problems without training; however (58.9%) think training courses in nutrition would help them serve better.
Study participant’s attitude (N = 202).
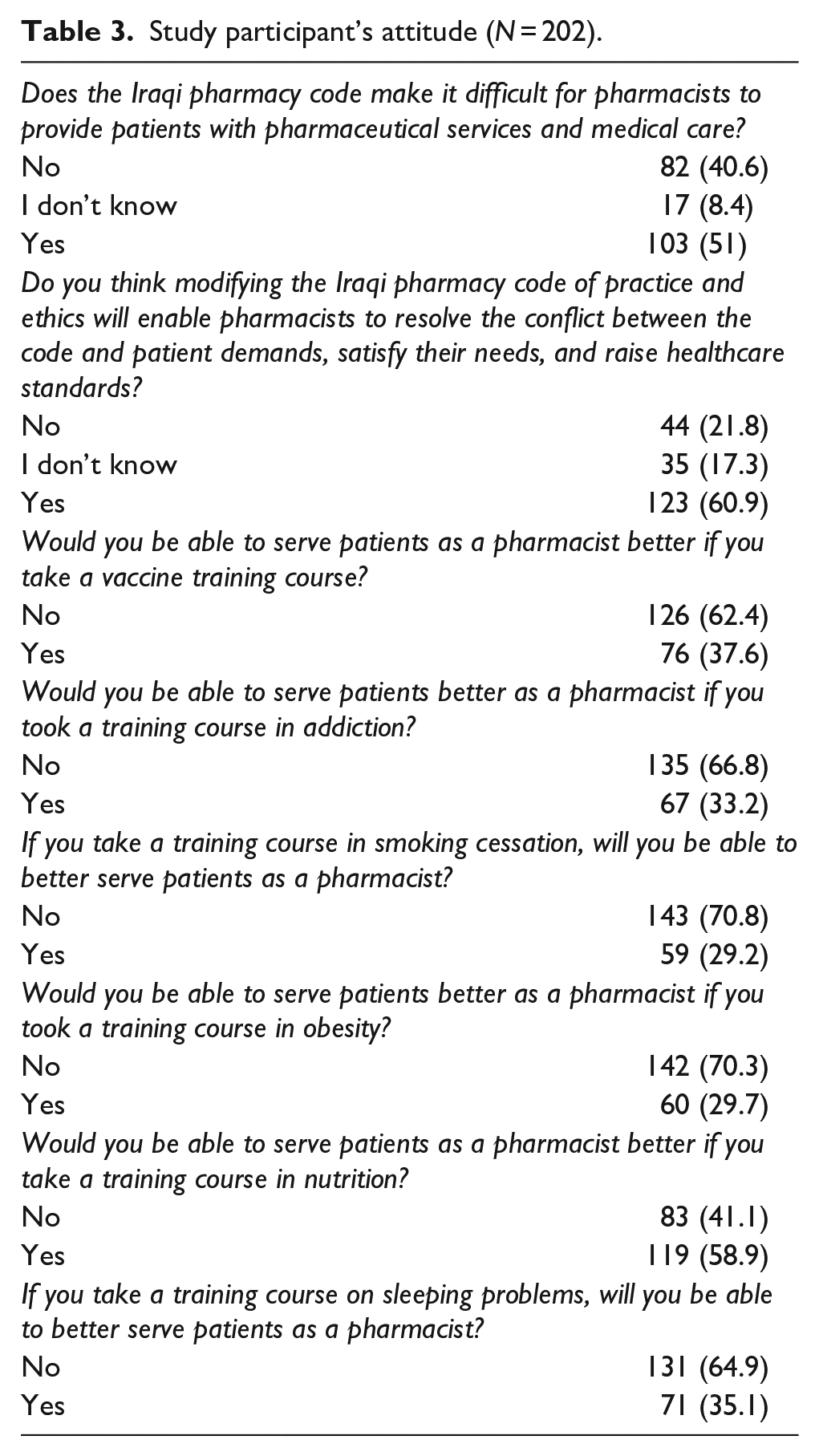
Table 4 illustrated that more than two-thirds (75.2%) of the participants agreed that increasing the pharmacist’s involvement in various aspects will allow them to serve more patients and improve the healthcare system at medical facilities, and (77.7%) of the participants found differences between work protocols used in medical facilities and the educational curriculum that had been studied for 5 years in college as a pharmacist. Similar results were found among participants who reported that they follow the law of the Iraqi pharmacy code of practice and ethics, which states that making agreements between a pharmacist and a doctor to dispense a particular drug or coding a prescription is prohibited. The pharmacist is not permitted to substitute a drug prescribed by one brand for another unless the prescribing physician has given his or her consent.
Study participant’s practice (N = 202).
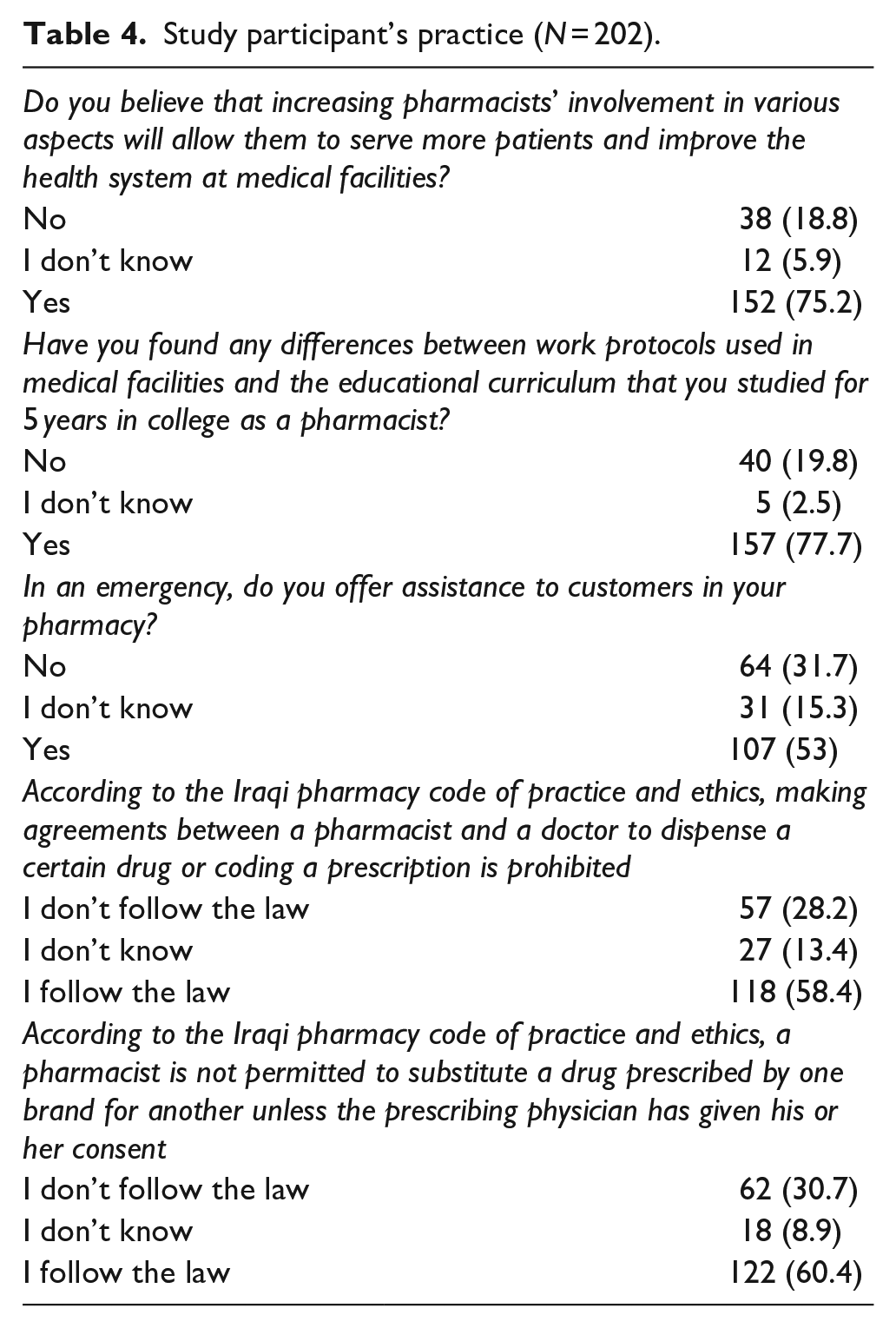
Table 5 results show that about one-third of the participants thought that risks and lack of patient cooperation prevented them from giving medical care to the patients. However (43.1%) thought that their responsibility prevented them from giving medical care to the patients.
Study participants’ barriers (N = 202).
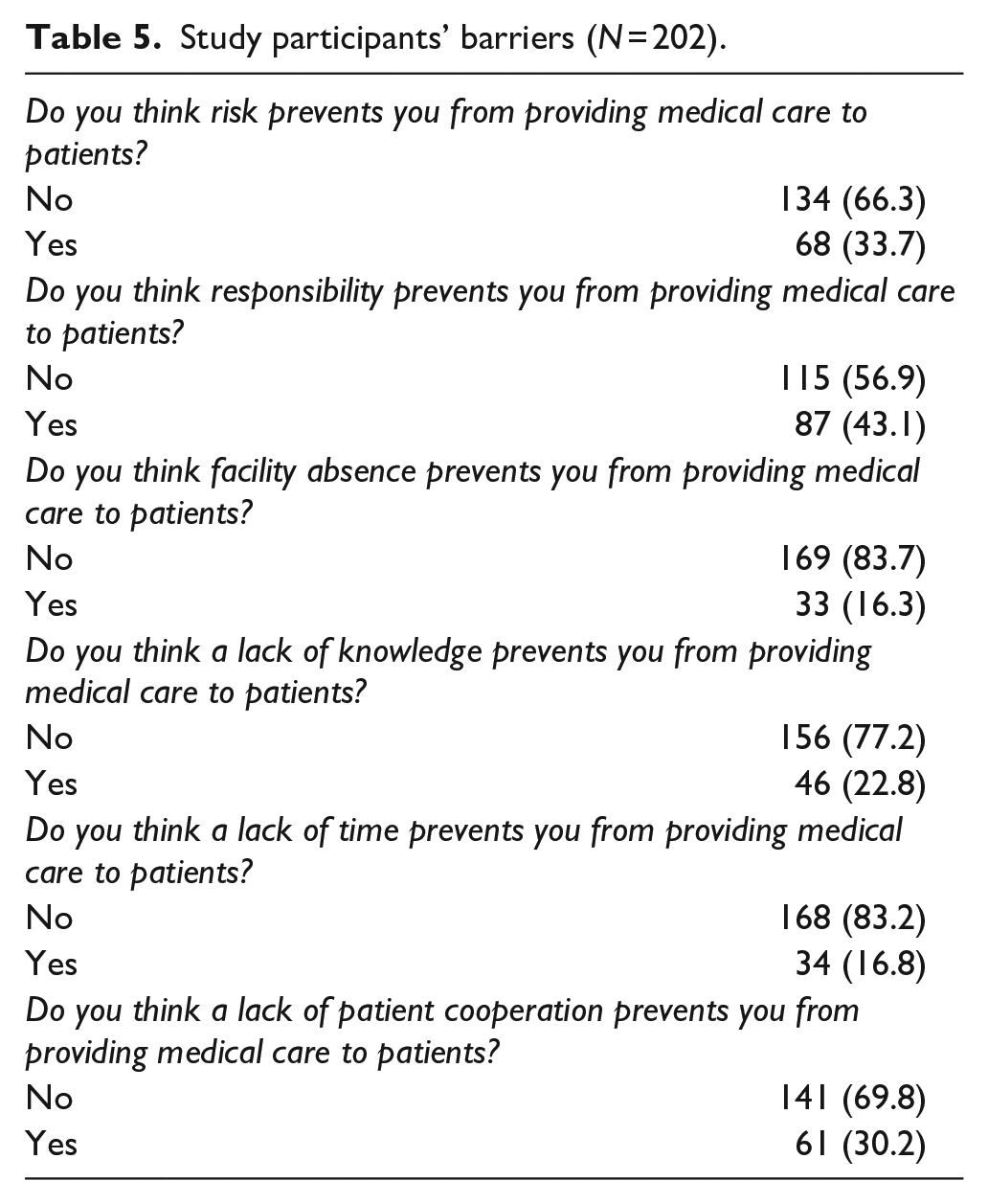
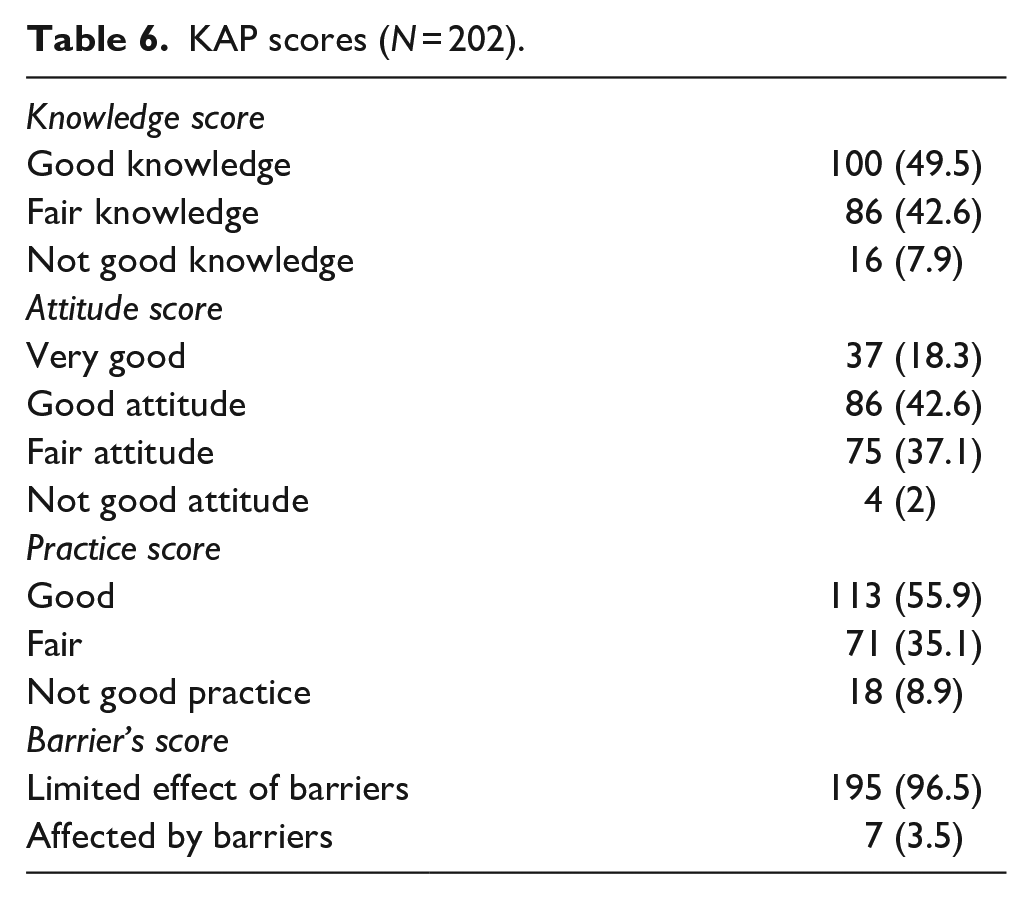
Table 6 illustrates the participants’ scores; the results showed that majority of participants had good and fair knowledge and good attitude scores were found among (42.6%) of the participants. About 56% of the participants had good practice scores, and results show a limited effect of the barriers among the majority of them (96.5%).
KAP scores (N = 202).
Furthermore, participants’ common suggestions regarding Iraqi code of practice and ethics to make it fit within the requirements of work and services provided were mainly on five aspects, which were: Resolve the problem of pharmacist number increment; educate the pharmacist in a specific area of expertise so he can prescribe/offer first aid/give injections/measure blood sugar and blood pressure; stop deals between pharmacists and physicians regarding specific medication; printing prescriptions so no misunderstanding; controlling drug companies in the Iraqi markets.
Discussion
In the current study, majority of the participants demonstrated familiarity with both the Iraqi Code of Ethics and Practice, as well as their respective job descriptions. This indicates that over half of the participants exhibited good knowledge, attitude, and practice. This study is the first of its kind to be conducted in Iraq. Considering achieving higher potential for Iraqi pharmacists, the questionnaire involved asking them certain questions in different aspects to help enlighten pharmacists about the Iraqi pharmacy Code of Ethics and obtain their knowledge, attitude, and practice of the laws, underlining certain obstacles restraining pharmacists from providing healthcare services. Few studies have reviewed pharmacy practices and ethics from 1990 to 2020. Pharmacy students and pharmacists are exposed routinely to ethical situations that need a response. 31 Worldwide, especially in developed countries, pharmacists have responded smartly and quickly. Similar studies have been conducted in different parts of the world.13,15,16 These studies viewed similar needs and agreed to modify specific aspects to help improve the current pharmacist status and pave the way for a better future. The scope of practice varies between countries as determined by the governing board of pharmacy. Many countries’ laws allow pharmacists to play a part only within specific areas of the medication use process, while in other countries, pharmacist practice is so wide-ranging. 2 The pandemic highlights the vital importance of initiating pharmacist involvement, being the link between the physician and patient, and the cornerstone of a healthcare revolution. Some studies show how pharmacists can serve patients, health practitioners, and the whole community.32,33
In this study, more than half of the participants were aware of the Iraqi Code of Ethics and Practice as well as they were aware of their job description and that the Iraqi law prohibits making agreements between a pharmacist and a doctor to dispense a certain drug or coding a prescription is prohibited as well as there is no permission to substitute a drug prescribed by one brand for another unless the prescribing physician has given his or her consent. Participants’ knowledge findings were consistent with their practice findings; it is very good that Iraqi pharmacists still obey the Iraqi Code of Ethics and Practice law. This study’s findings shows that more than half of the participants had good knowledge, attitude, and practice, which is consistent with the other study findings. In this study it reveals that more than three-quarters of participants found differences between work protocols used in medical facilities and the educational curriculum that you studied for 5 years in college as a pharmacist; that comes consistent with their recommendation and suggestion to update Iraqi pharmacy school educational curriculum to be suitable with other Iraqi markets requirement and needs.
Majority of the participants had no barriers that refrain them from giving medical care to patients except those who complained about their responsibilities that interfere with giving medical care to patients (43.1%), and about one-third of participants thought that risks and patient lack of corporation can refrain them from giving medical care to patients. However, lacking knowledge represents a constraint for (22.8%) of them. The findings of this study necessitate future application to a larger sample size to comprehensively evaluate participant perceptions of the challenges encountered in practice. This approach will facilitate the development of interventions to address these challenges considering the increasing number of Iraqi pharmacists and decreasing responsibilities. It is conceivable that the lack of trust in the abilities and knowledge of pharmacists by Iraqi patients contributes to the observed lack of cooperation. The increment in pharmacist numbers should be used to benefit by widening the pharmacist’s involvement, which can be achieved in many ways by increasing their knowledge and practice in different aspects as well as receiving the appropriate training like participation in bedside rounds as part of multidisciplinary health care system, prescribing, vaccination, sleep disorder management, nutrition, obesity, treating addiction, and smoking cessation counseling. This expansion of pharmacists’ roles can be particularly valuable during crises such as COVID-19, war, and displacement, where the demand for pharmacists is greater than ever. To deal with this challenging situation, it reshaped the front-line pharmacist activities and job responsibilities.32,33 These practices go beyond the pharmacist’s routine activities, like reviewing patient medication profiles, providing prescribing support to physicians, and counseling patients. It is essential to note that this study is limited in that it only covers three provenances in Iraq: Baghdad, Al-Diwaniya, and Wasit. Therefore, to provide a more comprehensive analysis, it is highly recommended that future studies encompass the entire country. This will enable researchers to obtain a more accurate and robust understanding of the topic under investigation.
Conclusion
Considering this study’s current findings over half of the Iraqi pharmacists who participated exhibited a good knowledge, attitude, and practice toward the pharmacy code of practice and ethics. However, there is a need to undergo training courses in different aspects to increase their involvement in the healthcare system in parallel to updating the Iraqi Code of Ethics and Practice and pharmacy school’s educational curriculum to be suitable with the Iraqi market’s requirement and needs. future studies are highly recommended.
Footnotes
Acknowledgements
The author would like to thank all the pharmacists who participated in and facilitated our work.
Authors’ contributions
Albaroodi K.A.I. set the study design, data collection, data analyses, reporting results, and preparing the manuscript, read and approved the final manuscript.
Availability of data and materials
All data generated during this study are included in this article and its supplementary information files.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Approval for the conduct of this study was approved by the Institutional Review Board of Al-Zahrawi University College (ZUC 013 Approval at 01-06-2022). All participants agreed to participate and signed an informed consent form upon participation in the study. All methods were conducted following relevant guidelines and regulations in compliance with the STROBE Statement
Consent for publication
Not applicable.