
Abstract
Objective
Integrating artificial intelligence (AI) in healthcare presents significant opportunities and challenges for nurses and other healthcare professionals. AI adoption may influence nurses’ work environment and overall healthcare. This study aimed to describe the level of knowledge, attitudes, practices, and barriers of AI among nurses in Jordan and describe their influence on nurses’ intent to stay in their job positions.
Methods
A descriptive correlational cross-sectional study was conducted among nurses working in governmental hospitals in Jordan. Data were collected using two validated instruments and were analyzed using descriptive statistics, Pearson correlation, and multivariate regression.
Results
The results showed that the mean scores of AI knowledge, attitudes, practices, barriers, and intent to stay were as follows: 3.91 (0.67), 4.15 (0.51), 3.98 (0.56), 3.93 (0.62), and 4.17 (0.49), respectively. While AI attitudes (r = .64, β = .34, P < .001) and practices (r = .58, β = .29, P < .001) significantly predicted intent to stay, barriers to AI were negatively correlated with it (r = −.42, β = −.14, P < .05).
Conclusion
A positive attitude and practical engagement with AI Could significantly enhance nurses’ intent to stay, while barriers undermine retention. Addressing these factors through targeted training and policy reforms is crucial for nursing workforce stability.
Introduction
Integrating artificial intelligence (AI) into healthcare has become a defining characteristic of the modern era, presenting both opportunities and challenges for the nursing profession. AI technologies are widely regarded as transformative tools that enhance the quality and efficiency of healthcare delivery. 1 They include clinical decision support systems, remote monitoring devices, and diagnostic tools, which offer vast amounts of clinically relevant data to improve patient outcomes and reduce medical errors. 2
The adoption of AI has also introduced complexities into the healthcare sector, particularly regarding its implications for nurses’ roles and their intent to remain in their positions. 3 The increasing reliance on AI technologies has created uncertainties among nurses, raising concerns about job security, workload changes, and the adequacy of AI in addressing patient care needs. 4 These concerns often influence nurses’ attitudes toward AI, which, in turn, affect their job satisfaction and engagement. 5
A previous study revealed a significant knowledge deficit about AI among Chinese nurses, with 64.7% of participants reporting a limited understanding of AI applications in nursing, and 68.5% expressed a desire to acquire more knowledge about AI (N = 270). 6 In Syria, a low-income country, a study revealed that only 23.7% of nurses and physicians understood the practical application of AI in healthcare (N = 1500). 7 Moreover, AI affected nurses’ decisions to stay or leave their workplaces, 8 and contributed to a sense of insecurity that can influence their intent to stay in their roles. 9
The attitudes and perceptions of nurses toward AI play a significant role in determining its successful adoption. While some Chinese nurses demonstrated enthusiasm for integrating AI into their practice, others expressed skepticism due to limited knowledge and experience with these technologies. 6 While some nurses perceived AI as a valuable tool that enhances clinical decision-making and reduces errors, 8 others expressed concerns about job security, reduced autonomy, and the potential for AI to undermine their professional judgment. 4 This may paradoxically create additional stress due to fears of being replaced or undervalued. 3
Despite the potential of AI to improve healthcare outcomes, its adoption is hindered by several barriers that affect nurses’ engagement and retention. It was revealed that the following were significant barriers to the widespread use of AI in nursing: regulatory uncertainties, liability risks, organizational resistance, 10 data privacy concerns, the fear of AI replacing human judgment in critical decision-making scenarios,11,12 lack of clear guidelines for using AI in clinical settings, 10 and lack confidence in AI's ability to empathize with patients or address complex emotional needs. 13 These barriers not only hinder the adoption of AI but also affect nurses’ job satisfaction and commitment, making it critical to address these concerns to foster a supportive work environment.
The dynamic interplay between AI knowledge, attitudes, practices, and barriers underscores the complexity of integrating technology into nursing. While AI has the potential to transform healthcare delivery, its success depends on addressing the concerns and expectations of nurses who are at the forefront of patient care. 2 It was revealed limited knowledge and understanding of AI systems could create a sense of resistance among nurses toward AI implementation. 6 This highlights the need to examine how AI knowledge, attitudes, and practices interact to shape nurses’ intent to remain in their job positions.
In the healthcare context of Jordan, a middle-income country, integrating artificial intelligence (AI) technologies into healthcare remains a relatively new and under-researched area. While AI is rapidly transforming global healthcare systems, its implementation in Jordan faces distinct challenges due to economic, infrastructural, and systemic constraints. 9 Unlike high-income countries where AI-driven solutions are more widely adopted, Jordanian healthcare institutions are still in the early stages of AI integration, with limited digital infrastructure and inconsistent access to advanced technologies. 5
A key concern is whether Jordanian nurses—who form the backbone of the healthcare workforce—are adequately prepared to engage with AI-driven healthcare systems. Studies suggest that Jordanian nurses face significant barriers, including limited exposure to AI applications, insufficient training programs tailored to emerging technologies, and a lack of institutional support for digital transformation. 14 Moreover, cultural and systemic factors, such as hierarchical decision-making structures and resistance to change within healthcare institutions, further complicate the adoption of AI-based tools in clinical practice. 2 These challenges create uncertainty about how AI might impact nurses’ roles, job satisfaction, and decision-making processes.
Given that Jordan, like many middle-income countries, is experiencing increased demand for healthcare services alongside a growing shortage of skilled nursing professionals, workforce retention is a critical issue. 15 High nurse turnover rates place additional strain on the healthcare system, leading to reduced quality of care and increased workload for remaining staff.16,17 Understanding how AI adoption influences nurses’ intent to stay in their roles is essential for developing targeted interventions that support workforce stability. Addressing this knowledge gap will provide healthcare policymakers, educators, and hospital administrators with insights to design AI training programs, improve workplace readiness, and create strategies to enhance nurse retention in AI-driven healthcare environments. While previous research has addressed some aspects of AI adoption in healthcare, there remains a significant gap in exploring how these factors collectively impact workforce retention in the nursing profession. Therefore, this study aimed to describe the level of knowledge, attitudes, practices, and perceived barriers of AI among nurses in Jordan and their influence on nurses’ intent to stay in their job positions in Jordanian hospitals.
Methods
Study design
A descriptive correlational cross-sectional design was used in this study.
Study setting
The current study was conducted in four governmental hospitals in Jordan (Princess Basma Teaching Hospital, Princess Raya Governmental Hospital, Ramtha Governmental Hospital, and Yarmouk Governmental Hospital). These hospitals together have a capacity of 570 beds.
Population and sampling
The target population for this study includes all hospitals in Jordan, encompassing 50 hospitals. These hospitals collectively represent the diverse landscape of the healthcare system in the country. However, for logistical feasibility and to maintain a focused approach, the accessible population was narrowed to four governmental hospitals only.
A convenience sampling method was employed to recruit participants for this study. This non-probability sampling technique allowed the selection of readily available participants who met the inclusion criteria. It facilitated the efficient collection of data from nurses working in accessible hospitals. This approach allowed for capturing relevant data without being constrained by geographical or logistical limitations. The inclusion criteria included being a nurse working at a hospital in Jordan, directly involved with patient care, and managing medical records and files. However, the exclusion criteria were nurses in the preceptorship or orientation period, as their experience with AI and healthcare systems is limited.
Sample size
To determine the appropriate sample size, a power analysis was conducted using G*Power software, 15 a statistical tool widely used in research to calculate the minimum number of participants required to achieve sufficient statistical power. By selecting a linear multiple regression analysis with a small effect size of 0.15, an alpha level of .05, Power level of 0.90, and four predictors, the G*Power calculation indicated that a minimum sample size of 111 participants is needed to ensure adequate statistical power. An additional 25% was added to the required sample size to account for potential non-responses or incomplete data. This adjustment brought the total sample size to 148 participants.
Data collection procedure
The researchers collected the data using a paper-based questionnaire between September 15, 2024, and November 30, 2024. After obtaining approvals from the administration departments of the selected hospitals, the researchers approached nursing managers, seeking their help in determining the eligible participants. Then, the researchers approached them, explained the study, asked them to sign an informed consent, and distributed the questionnaires to them. The participants were allowed to fill out the questionnaire in a quiet room in the hospital and handed the filled questionnaire to the researchers directly.
Questionnaire
Sociodemographic characteristics such as gender, age group, and years of experience were assessed using a questionnaire designed specifically for this study. An additional questionnaire was developed to assess nurses’ knowledge, attitudes, practices, and barriers to AI, as well as their intent to stay in their positions.
The first part of the questionnaire consisted of 40 items divided into four subscales, each measuring a distinct dimension of AI engagement. Previous studies provided foundational insights into the questionnaire dimensions and informed the formulation of the items.3,5,6 The knowledge subscale (10 items) included items about basic principles of AI, clinical application, and the ability of AI to improve diagnostic accuracy and reduce human error. In addition, the attitudes subscale (10 items) included items covering these areas: optimism about AI's ability to enhance efficiency and decision-making, concerns about job security, ethical issues, data privacy, and willingness to engage with AI technologies. Furthermore, the practices subscale (10 items) assessed the perceived integration of AI into patient care and the use of AI tools for diagnostic purposes. The barriers Subscale (10 items) included items about limited training and institutional support, concerns about algorithmic bias, lack of empathy in AI systems, and privacy and regulatory challenges. Each item in the questionnaire was scored on a 5-point Likert scale ranging from “1” (strongly disagree) to “5” (strongly agree). The total questionnaire score could range from 40 to 200.
A panel of five domain experts (AI specialists, nursing educators, and psychometricians) reviewed the questionnaire items to ensure clarity, relevance, and representativeness. All items were deemed appropriate and understandable by the target population. The questionnaire achieved an overall Content Validity Index (CVI) of 0.91. Moreover, Cronbach's alpha reliability index of internal consistency for the different subscales ranged from 0.85 to 0.92. In addition, the overall Cronbach's alpha reliability index of internal consistency was 0.91, indicating excellent reliability. A pilot study was conducted with 10 nurses to assess the clarity, relevance, and feasibility of the questionnaire. Based on feedback from the pilot study, minor modifications were made to enhance item clarity and response accuracy. This pretesting phase further strengthened the validity of the instrument by ensuring that items were well understood by the target population.
The second part of the questionnaire was developed to assess nurses’ intent to remain in their job positions. It contained 10 items to capture intrinsic and extrinsic factors influencing workplace commitment. The items were crafted based on a synthesis of previous research studies.14,18,19 They assessed personal commitment to the nursing profession, organizational loyalty, satisfaction, and resilience in the face of job dissatisfaction. Each item was scored on a 5-point Likert scale with a total score ranging from 10 to 50. A panel of experts confirmed the relevance and clarity of all items. The tool achieved a CVI of 0.93, indicating strong expert agreement about item relevance. Cronbach's alpha reliability index of internal consistency was .89.
Data analysis
The SPSS version 26 was used to analyze the data. Descriptive statistics were used to describe the characteristics of the study sample, including means, standard deviations, frequencies, and percentages. Inferential statistical analyses were then performed, beginning with Pearson correlation analysis to explore bivariate relationships between variables, such as knowledge, attitudes, practices, and barriers of AI, and nurses’ intent to stay. This analysis provided an initial understanding of the strength and direction of associations. To further assess the predictive relationships between independent variables (knowledge, attitudes, practices, and barriers of IA) and the dependent variable (intent to stay), a multivariate linear regression analysis was conducted; it enabled the researchers to examine the effects of independent variables on the dependent variable. Moreover, the regression model was adjusted for potential confounding factors, enabling the identification of significant predictors of nurses’ intent to stay. The statistical significance level was set at P < .05 for all statistical tests.
Research ethics
Approval to conduct the study was obtained from the Institutional Review Board (IRB) at Zarqa University with IRB approval No (30/2023). Participants were informed about the study through detailed paper informed consent forms, which explained the study's purpose, procedures, and other relevant information. Participants were fully aware of the study and consent voluntarily before participating. All personal identifiers were removed from the dataset or securely stored to protect their confidentiality and anonymity. Access to this sensitive information was restricted to the researchers and protected using advanced encryption methods to prevent unauthorized access.
Results
While 142 nurses agreed to participate in the study, only 116 nurses returned the filled questionnaires, representing a 78.3% response rate. The majority of the nurses were males (66.4%, n = 77), while females constituted 33.6% (n = 39) of the sample. Regarding age distribution, the largest proportion of nurses (61.2%, n = 71) were between 26 and 39 years, followed by 19.8% (n = 23) aged 40–54 years. In terms of years of experience, 40.5% (n = 47) of nurses had 6–10 years of experience, and 25.9% (n = 30) had 16 years or more (see Table 1).
Demographic characteristics of the study participants (N = 116).

Note. N = sample size.
Regarding the level of knowledge, attitudes, practices, and barriers of AI among the nurses, attitudes towards AI had the highest mean score of 4.15 (SD = 0.51), followed by AI practices with a mean score of 3.98 (SD = 0.56). While AI barriers had a mean score of 3.93 (SD = 0.62), AI knowledge scored the lowest among the variables with a mean of 3.91 (SD = 0.67). The total score of all items together was 3.99 (SD = 0.47), indicating high overall levels across all subscales (see Table 2).
Descriptive statistics of knowledge, attitudes, practices, and barriers of artificial intelligence among nurses (N = 116).

Note. N = sample size, SD = standard deviation.
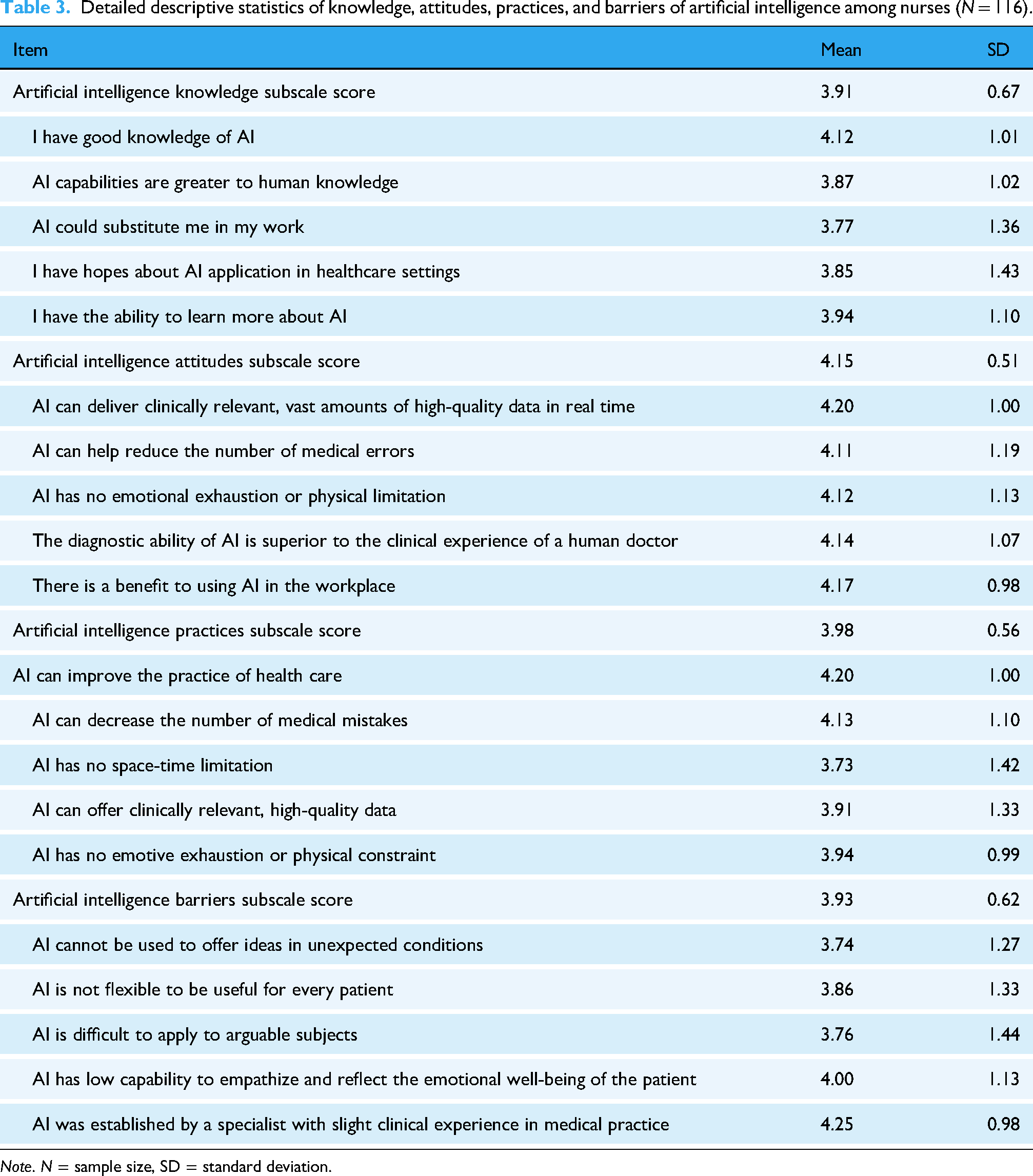
Regarding nurses’ knowledge of AI, the highest mean score was recorded for the item “I have good knowledge of AI” with a mean of 4.12 (SD = 1.01). Nevertheless, the item “AI could substitute me in my work” scored the lowest mean score of 3.77 (SD = 1.36). Concerning the attitudes subscale, the item “AI can deliver clinically relevant, vast amounts of high-quality data in real-time” had the highest mean score of 4.20 (SD = 1.00), followed by the item “There is a benefit to using AI in the workplace” with a mean of 4.17 (SD = 0.98). With regard to the items of the AI practices subscale, the highest mean score was for “AI can improve the practice of healthcare” with a mean of 4.20 (SD = 1.00). However, the item “AI has no space-time limitation” scored the lowest mean of 3.73 (SD = 1.42). Finally, regarding the subscale of AI barriers, the item “AI was established by a specialist with slight clinical experience in medical practice” had the highest mean score of 4.25 (SD = 0.98) (see Table 3).
Detailed descriptive statistics of knowledge, attitudes, practices, and barriers of artificial intelligence among nurses (N = 116).
Note. N = sample size, SD = standard deviation.
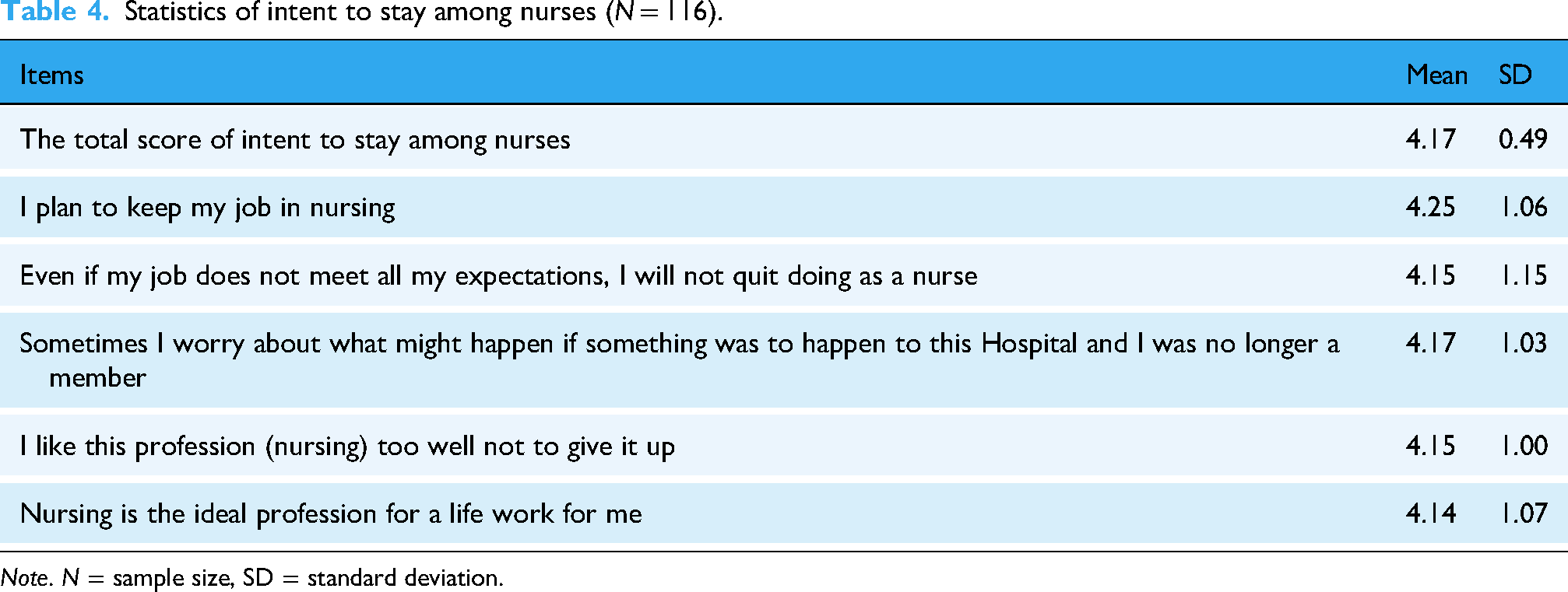
Regarding the intent to stay among nurses, the highest mean score was recorded for the item “I Plan to keep my job in nursing” with a mean of 4.25 (SD = 1.06). The overall mean score for the intent to stay among nurses was 4.17 (SD = 0.49), reflecting a high level (see Table 4).
Statistics of intent to stay among nurses (N = 116).
Note. N = sample size, SD = standard deviation.
The results also showed that attitudes toward AI had the strongest correlation with the intent to stay (Pearson r = .64, P < .01), indicating that positive attitudes toward AI are associated with a stronger intent to stay. Also, perceived practices of AI demonstrated a significant positive correlation with the intent to stay (Pearson r = .58, P < .01), highlighting that integrating AI into the nursing workflow could enhance the retention of nurses. Furthermore, nurses’ knowledge of AI was positively correlated with their intent to stay (Pearson r = .58, .52, P < .05), indicating that a higher level of knowledge of AI is linked to greater intent to stay among nurses. Conversely, barriers to AI had a negative correlation with the intent to stay (Pearson r = −.42, P < .05), emphasizing that barriers to AI adoption may detract from nurses’ willingness to remain in their roles. The total AI score, which combines all four domains, showed a significant positive correlation with the intent to stay (Pearson r = .61, P < .01), which underscores the collective impact of knowledge, attitudes, practices, and barriers of AI on nurses’ intent to stay (see Table 5).
Pearson correlation coefficients between subscales, total AI score, and intent to stay (N = 116).

Note. N = sample size, *P ≤ .05, **P < .001.
The results of the linear multiple regression model for the predictors of nurses’ intent to stay exhibited a strong correlation coefficient (R = .75), indicating a substantial association between the independent variables and the dependent variable (R2 = .56, F-value = 34.72, P < .001). This indicates a robust model fit and confirms the explanatory power of AI-related factors in predicting nurses’ intent to remain in their roles. Additionally, the Durbin-Watson statistic is 1.89, suggesting that there is no significant autocorrelation in the residuals, thereby reinforcing the reliability of the regression results. Multicollinearity diagnostics reveal that the model is free from significant multicollinearity issues, as all tolerance values exceed 0.1, and the Variance Inflation Factor (VIF) for each predictor is below 10. The level of knowledge about AI, Attitudes toward AI, practices of AI, and barriers of AI were statistically significant predictors of intent to stay among nurses (β=−.14, P < .05, β=.22, P < .01, β=.34, P < .001, β=.29, P < .001), respectively. These results reflect the critical role of these variables in enhancing the intent to stay among nurses. On the other hand, barriers of AI influenced the intent to stay, negatively (see Table 6).
Predictors of intent to stay among nurses (N = 116).

Note. N = sample size, t = t-test value, VIF = variance inflation factor.
Discussion
This study described the level of knowledge, attitudes, practices, and perceived barriers of AI among nurses in Jordan and described their influence on nurses’ intent to stay in their positions in Jordanian hospitals. The results showed a high mean score of knowledge about AI among nurses (M = 3.91, SD = 0.67). Using the developed cut points for interpretation, scores above 3.75 indicate a high level of knowledge, reinforcing the notion that nurses in this sample are well-informed about AI. This indicated that nurses in the sample generally possessed a strong understanding of AI. This high level of knowledge about AI is congruent with global trends where some researchers revealed that nurses who possess a robust understanding of AI are better equipped to leverage these technologies in improving patient outcomes, streamlining workflows, and enhancing decision-making.2,20 While the high level of AI knowledge observed in this study is encouraging, it contrasts with findings from some previous studies, which have documented significant knowledge gaps among nurses. For instance, it was reported that only 45% of nurses in Saudi Arabia, demonstrated basic awareness of AI applications in healthcare. 8 This discrepancy could be attributed to regional differences in education systems, access to resources, and institutional support for AI training. Also, it was revealed that only 40% of nurses in the United States felt confident in their understanding of AI algorithms and big data analytics. 21 However, the focus of their study was on the use of AI in mental health only. The present study's findings also contradicted the findings of a study conducted in Syria and showed that only 23.7% of healthcare providers understood its practical applications in clinical settings. 7 The difference could stem from the specific focus on nurses in the present research and the difference in the healthcare systems between the two countries.
The results of the present study showed a high mean score of attitudes toward AI among nurses (M = 4.15, SD = 0.51). According to the preset cut points, scores above 3.75 indicate a high level of attitude. This highlights nurses’ readiness and openness to use AI technologies in their professional roles. This corresponds to the findings of a study among 200 nurses in Egypt, where 64% of participants expressed positive attitudes toward AI, particularly regarding its role in improving efficiency and reducing workload. 3 The results are also relevant to what was found in another study, in which 72% of nurses in India acknowledged the benefits of AI-enabled systems in enhancing decision-making and streamlining workflows. 22 On the other hand, moderate attitudes toward AI were reported among healthcare professionals in Saudi Arabia, with a mean attitude score of 3.8 (SD = 0.9). 8 Moreover, it was reported that 35.3% of healthcare workers in China expressed skepticism about AI's relevance in nursing. 6 This discrepancy may be attributed to differences in training opportunities, exposure to AI technologies, and institutional support for AI adoption. Training programs should focus not only on AI knowledge but also on experiential learning to enhance familiarity and reduce apprehensions. AI education should go beyond technical training to include discussions on ethical concerns, professional roles, and success stories of AI integration in nursing.23,24
The results of the present study showed a high mean score of practices of AI among nurses (M = 3.98, SD = 0.56). According to the developed cut points, scores above 3.75 signify a high frequency of AI utilization in practice. This level was higher than the moderate levels of AI utilization among nurses in China, with a mean practice score of 3.6. 6 The study attributed this to limited access to AI tools and insufficient training opportunities, which constrained nurses’ ability to fully integrate AI into their workflows. Nevertheless, the results were relevant to the moderate to high level of AI practices among healthcare professionals in Saudi Arabia, with a mean score of 3.85. 8 These differences reflect regional differences in AI adoption driven by factors such as healthcare infrastructure, availability of AI tools, and organizational culture. Nursing policies should address AI-related concerns, such as ethical use, job security, and equitable access to AI resources. Institutional investment in user-friendly AI tools and ongoing support can enhance AI adoption and satisfaction.25,26
The results of the present study showed a moderate-to-high mean score of barriers to AI among nurses was high (M = 3.93, SD = 0.62). Despite the high overall knowledge, attitudes, and practice scores, this reflected significant reported barriers associated with AI technologies. Some of these barriers are the perceived lack of humanistic qualities in AI systems, the inflexibility of AI in catering to individual patient needs, and challenges in applying AI to arguable clinical scenarios. This is relevant to what was about nurses’ struggles with AI systems that lack the adaptability required to handle diverse clinical scenarios. 13 The findings are also comparable to the previously reported limitations of AI in addressing the emotional and psychological aspects of patient care that were reported in another study. 4 absence of humanistic qualities in AI as a primary factor contributing to resistance among healthcare professionals, 12 AI's perceived inflexibility and limited emotional engagement were viewed by 62% of nurses as significant barriers, mirroring the moderately high scores observed in this study. 3 In addition, 61% of nurses expressed concerns about the lack of clear guidelines and accountability frameworks for AI technologies. 10 Similarly, it was found that 64.7% of healthcare professionals in China cited limited training opportunities as a significant deterrent to engaging with AI technologies, further substantiating the relevance of the barriers identified in this study. 6 Furthermore, 72% of nurses in a study in India encountered challenges related to integrating AI into existing workflows. 22 These results are consistent with the high barrier scores observed in this study, particularly concerning the item “AI is difficult to apply in arguable clinical scenarios.”
The results of the present study showed a high mean score of intent to stay among nurses (M = 4.17, SD = 0.49). These results are consistent with what was reported in a study conducted in Egypt which reported that nurses with high levels of job satisfaction were significantly more likely to express a strong intent to stay, with a mean retention score of 4.5 (SD = 0.4). 14 This was also consistent with the rate of 85% of nurses in the United States who rated their work environment as supportive and expressed a strong intention to remain in their roles. 17 The high score of intent to stay in the present study could also be partially attributed to the high scores of knowledge, skills, and attitudes of AI, as reported in the results.
Attitudes toward AI strongly correlated with intent to stay (Pearson r = .64, P < .01). They were the strongest predictors of nurses’ intent to stay (β = .34, P < .001). These findings align with previous studies. For instance, it was found that positive attitudes toward AI were strongly associated with job satisfaction and retention among nurses, reporting a similar correlation coefficient of (Pearson r = .63, P < .01) 6 (Pearson r = .62, P < .01). 8 These studies reinforced the idea that fostering positive attitudes toward AI is crucial for leveraging its potential to enhance workforce stability. While knowledge of AI is undoubtedly important, it does not necessarily translate into behavioral intent or willingness to remain in the profession. Nurses may possess theoretical knowledge of AI but still harbor skepticism or apprehension about its practical implementation, particularly if they perceive AI as a threat to job security or professional autonomy. Attitudes, on the other hand, encompass emotional and cognitive responses to AI, influencing motivation, job satisfaction, and overall career commitment. Positive attitudes can mitigate fears of job displacement and reinforce AI's role as a supportive tool rather than a replacement for human expertise. 25
The finding showed that practices of AI were also significant predictors of intent to stay (β = .29, P < .001). This correlates with the findings of a study that revealed that nurses who actively engaged with AI-enabled tools for clinical decision-making and patient monitoring reported higher levels of job satisfaction and retention intentions (β =.30, P < .001). 27 The findings are relevant to the findings of another study that found that nurses who utilized AI for decision support and patient monitoring exhibited a 25% increase in retention intentions compared to those who did not, underscoring the practical benefits of AI engagement. 21
The results also showed that knowledge about AI significantly predicted intent to stay. This is consistent with the results of a study that reported that nurses with higher levels of AI knowledge were more likely to express confidence in their roles and a stronger intent to stay (β=.21, P < .01). 11 Similarly, it was documented that knowledge of evidence-based practices, which often incorporate AI, was positively associated with retention intentions among Jordanian nurses (β=.21, P < .05). 5
The results revealed a significant negative correlation between AI barriers and intent to stay (Pearson r = −.42, P < .05) (β = −.14, P < .05). This indicated that perceived barriers to AI adoption, such as inflexibility, ethical concerns, and lack of institutional support, detract from nurses’ willingness to remain in their roles. This is consistent with the negative correlation reported between perceived barriers and retention intentions among nurses (r = −.45, P < .05). 12 It is also compatible with the findings that nurses who perceived AI as unreliable or fraught with risks were significantly less likely to express a commitment to their roles. 28 Similarly, It was reported that nurses who encountered barriers such as insufficient training and technical difficulties were more likely to experience frustration and disengagement, with a negative correlation between barriers of AI and retention (r = −.42, P < .05). 14 Furthermore, algorithmic bias and ethical concerns were significant deterrents to retention, with a negative correlation (r = −.43, P < .05) between barriers of AI and intent to stay. 29
Strengths and limitations
This study provided substantial findings by describing the combined effect of predictors on nurses’ intent to stay. The findings offer significant insights into AI integration in healthcare and its effects on the nursing workforce. However, the study has limitations that should be acknowledged. While suitable for exploring associations, the cross-sectional design does not allow for causal inferences, limiting the ability to determine the long-term impact of AI-related factors on nurses’ intent to stay. Additionally, the reliance on self-reported data may introduce response biases, as participants may overestimate or underestimate their knowledge, attitudes, or practices. Furthermore, the use of a convenience sampling method may limit the generalizability of the findings, as the sample may not fully represent the broader nursing population. This approach could introduce selection bias, as nurses who are more interested or knowledgeable about AI may have been more likely to participate. Future studies should consider using probability-based sampling techniques to enhance the representativeness of the sample and strengthen the reliability of the findings.
Implications and recommendations
The findings underscore the need for addressing nurses’ concerns about AI, such as its limitations in providing flexible and empathetic care. By addressing these concerns, the study empowers nurses to view AI as a complementary tool rather than a threat to their professional identity. Also, nursing administrators should invest in infrastructure and resources to support the adoption and application of AI tools, ensuring they are user-friendly, accessible, and aligned with the clinical needs of nurses.
Nursing educators are encouraged to prioritize targeted educational initiatives to enhance nurses’ understanding of AI's benefits, capabilities, and potential to improve clinical workflows and patient outcomes. Tailored training programs should emphasize the practical applications of AI and address common misconceptions. Additionally, the findings provide a basis for revising teaching methods and content to foster positive attitudes toward AI.
Policymakers are encouraged to address the barriers to AI adoption. These efforts should include the development of clear policies and robust technical support systems to mitigate resistance and foster a culture of technological acceptance. It is recommended to consider the implications of these findings when designing workforce retention strategies, focusing on the dual objectives of leveraging AI to enhance healthcare delivery and supporting the professional development of nurses.
A future research study is recommended to explore the longitudinal effects of AI integration on retention and to provide actionable insights for continuous improvement in nursing management and technological adoption. Researchers can also build on this study to investigate the effectiveness of specific interventions to improve nurses’ engagement with AI technologies.
Conclusion
This study described the level of knowledge, attitudes, practices, and barriers of AI among nurses in Jordan and described their influence on nurses’ intent to stay in their job positions. The results showed high mean scores of knowledges, attitudes, practices, and barriers of AI. While positive attitudes, practice, and knowledge of AI could significantly enhance nurses’ intent to stay, barriers to AI were negatively correlated with it. Addressing these factors through targeted training and policy reforms is crucial for nursing workforce stability. The study underscores the need for targeted interventions to keep fostering positive attitudes and address systemic barriers to AI adoption. These insights provide a valuable foundation for policymakers, healthcare administrators, and educators to support workforce retention and effectively integrate AI into nursing practice.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076251336106 - Supplemental material for Knowledge, attitudes, practices, and barriers of artificial intelligence as predictors of intent to stay among nurses: A cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076251336106 for Knowledge, attitudes, practices, and barriers of artificial intelligence as predictors of intent to stay among nurses: A cross-sectional study by Islam Ali Oweidat, Mohammad Alkhatib, Mohammed ALBashtawy, Saleh Al Omar, Saleem Al-Rjoub, Khitam Alsaqer, Khalid Al-Mugheed and Sally Mohammed Farghaly Abdelaliem in DIGITAL HEALTH
Footnotes
Acknowledgments
The authors extend their appreciation to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R844), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Author contributions/CRediT
Conceptualization: IAO, MA; Data curation: KM, MAB, SAA, and MA; Formal analysis: IAO, MAB, and SAA; Investigation: IAO, MA, MAB, and SAA; Methodology, Project administration, Resources, Software, Supervision, and Validation: SAA, SAR, and KA; Visualization, Writing—original draft: SMF, IAO, MA, MAB, SAA, SAR, and KA; Writing—review & editing: SAR, MA, and KA. IAO is responsible for the overall content as guarantor. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2025R844), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.