
Abstract
Background:
The cost of maternal complications is considered as an important factor hindering the utilization of maternal health care services. However, information of estimate of spending on maternal complication was lacking. This study was aimed to estimate the cost of maternal complications and associated factors among mother’s attending Hawassa public hospitals, Sidama Regional state, Ethiopia.
Methods:
A cross-sectional study design was conducted among 348 randomly selected mothers attending public hospitals in Hawassa from November 15 to December 15, 2021. Data was coded and entered into Epi Data version 3.1 and exported to STATA version 16.0 for analysis. Simple and multiple linear regression analysis was done. Correlation coefficient along with 95% CI was used to present the finding and p < 0.05 was used to declare statistical significance.
Results:
This study found that total median cost of maternal complications was 4895.5 (IQR = 3779) ETB. The total median direct medical cost was 1765.5 (IQR = 1649.5) ETB. Number of days absent [(R = 0.028; 95% CI: (0.023, 0.033)], distance from facility [(R = 0.001; 95% CI: (0.000, 0.002)], site of laboratory diagnosis [(R = 0.230; 95% CI: (0.140, 0.320)], number of laboratory test conducted [(R = 0.045; 95% CI: (0.021, 0.069)] were found to be significance predictors of maternal complications costs.
Conclusions:
Total median cost of maternal complications in current study was high. Respondents’ site of diagnosis, number of days missed from work, number of laboratory tests, and distance from hospitals were independent predictors of maternal complications cost. Thus, we will recommend governments to introduce strategies that specifically help mothers with maternal complications.
Introduction
Any sickness or injury that develops during pregnancy, childbirth, or is connected to either of those events is referred to as a maternal complication. It involves obstructed labor, infection, unsafe abortion, hemorrhage, and eclampsia.1–3 It is well acknowledged that emergency care is a crucial and useful component of obstetric treatments used to prevent maternal problems. However, studies show that inadequate care is one of the main causes of high rates of morbidity, death, and the expense of complications.1,2
Despite significant progress in recent years, the worldwide maternal mortality ratio (MMR) remains unacceptably high. 4 Around 800 women worldwide pass away every day as a result of complications during pregnancy or childbirth. The primary causes of death and disability among women in poor nations are problems related to pregnancy and delivery. A total of 295,000 women died in 2017 from complications connected to pregnancy and childbirth; 94% of these deaths took place in low- and middle-income countries, with Sub-Saharan Africa accounting for almost two-thirds (196,000) of maternal deaths. Ethiopia has one of the worst maternal mortality rates in Sub-Saharan Africa, at 412 deaths per 100,000 live births.2,5,6
The majority of complication in Ethiopia are caused by a lack of access to expert care and institutional delivery. Poor care quality is also associated with high rates of morbidity, death, and the expense of maternal complications. 7 Obstetric hemorrhage, sepsis, anemia, hypertensive disorders of pregnancy, and dystocia (obstructed labor) have been identified as the main causes of maternal near-misses.3,8
It might be challenging to use hospitalized maternal health care services due to the financial burden that maternal complications place on families. The financial consequences of maternal complications might take many different forms. First, poor health is probably linked to greater out-of-pocket (OOP) medical care costs, which depletes household finances. Second, poor health may result in a loss of labor and, as a result, a reduction in household income.9,10 Any expense incurred as a result of maternal concerns affects the overall amount typically spent by household members. Therefore, expenses resulting from health shocks that only affect one family member can have an impact on the wellbeing of other family members.9,11 Despite the fact that maternal health care are free, women just pay large expenditures when complications develop, and they risk incurring catastrophic health costs, according to the findings of a study done in northern Ghana. 11 A study conducted in Ethiopia found that spending on maternal complications is closely connected to poverty. 7 The cost of treating a Maternal Complication is influenced by a number of factors, including direct medical costs (registration, consultation, laboratory test, drugs, transportation, and other related expenses), non-medical direct costs (Transportation and food), costs incurred indirectly (absenteeism), delivery method.9,11
Ethiopia’s government enacted an exemption policy that guarantees free maternity healthcare from public providers. Organizing and mobilizing the Health Development Army at all levels to promote behavioral change, distributing ambulances to all districts in Ethiopia, providing free maternity services at various health care levels, training human resources and equitable placement of health professionals in health facilities, and providing adequate drugs, medical supplies, and equipment are just a few of the actions taken so far. Despite these efforts, the expense of treating a maternal complication at the national level remains considerable.5,7 Reliable estimates of spending on treating maternal complications are necessary for efficient budgeting and decision-making in the health-care system, but data on the cost of maternal complications in Ethiopia is limited. As a result, this study attempted to address this gap by assessing the overall cost and factors related with the expenditures associated with running the treatment of maternal complication at Hawassa public hospital, Sidama, Ethiopia.
Methods
Study area and period
This study was conducted in Hawassa University Comprehensive Hospital, Adare General Hospital and Tula Primary Hospital, Sidama Regional State, Southern Ethiopia. These three public Hospitals were selected purposively. The Hospitals found in Hawassa city which is located 275 km away from the Addis Ababa, capital city of Ethiopia. In addition to these public hospitals the city has six private hospitals, seven health centers, 47 private clinics and 15 health posts. The study period was from November 15 to December 15, 2021.
Study design
An- institutional based cross-sectional study design was conducted.
Population and eligibility criteria
All mothers admitted to Hawassa University Comprehensive Hospital, Adare General Hospital and Tula Primary Hospital to seek service for maternal complications were a source population, while all eligible mothers diagnosed with maternal complication and obtained service from Hawassa University Comprehensive Hospital, Adare General Hospital and Tula Primary Hospitals were included in the study. Pregnant laboring and delivered mothers who were diagnosed with maternal complications at the public hospital during the data collection period were included in the study. However, mothers who were referred from the private health facilities after getting partial and full treatment were excluded.
Sample size determination and sampling techniques
The sample size was estimated using a single population mean formula with an assumption on normal distribution 95% of all data points will be within +2 SD from the mean with margin error of 5%.
Based on these assumptions, the sample size was estimated by the formula shown below.
n = 6147. Since the total population of 348 is < 10000, the population correction formula was used to get the final sample size.

After adding 5% for non-respondents, the calculated final sample size was given as 347. All mothers (348) diagnosed with maternal complications during the study period were included to increase the precision of the study as well as to have a better estimate of the magnitude of the cost of maternal complications. The sampling frame was developed from the record by assigning ID numbers for all MRNs and a simple random sampling techniques was used to recruit the study participants.
Data collection procedure and instruments
Data were collected using a structured questionnaire that was adopted from different literature.4,11–13 The questionnaire was prepared in English and translated to Amharic and then back to English to check for its consistency. The questionnaire contains four parts. Socio-demographic characteristics, clinical status, time spent to traveling to the antenatal clinic as well as transport times, and distance from the facility to home in km or minute, and medical costs (direct medical cost and non-medical cost).
Five BSs nurses for data collections and two BSc nurses for supervision recruited and 1 day training about the overall objective of the study was given. Data was collected from participants through face-to-face interviews. The data collectors were responsible for interviewing all mothers who met the selection criteria and were willing to participate in the study.
Variables and measurements
Cost of maternal complications was the dependent variable of this study. The maternal complication is when the mothers develop at least one of the following; hemorrhage (Abortion, Antepartum hemorrhage, Post-partum hemorrhage, Ectopic pregnancy), preeclampsia, sepsis, ruptured uterus, and prolonged labor.14,15 Cost of maternal complication was measured from direct medical cost and non-medical costs. For this specific study, direct medical cost was measured from patient’s perspective which includes the costs of diagnosis/laboratory and treatment costs.7,16 Direct non-medical costs included all food purchases, lodging for the patient and her caregiver during the health-seeking process, and transportation to and from the hospital.7,11 The summation of costs from all resources utilized was considered to comprise all medical costs for women per month.
Data quality control
To assure the quality of data, the following activities were done before the starting of actual data collection. The questionnaire was translated to Amharic and translated back to English to check for consistency. Pretesting was carryout on 5% of the sample size in the Kuyera referral hospital. The training was given to the data collectors and supervisors before data collection. Collected data was checked for its completeness and clarity daily. Close follow up and supervision by supervisor and investigator throughout the data collection process were undertaken.
Data processing and analysis
Data were cleaned and coded before entry and entered Epi-data version 3.2 and exported to STATA version 164.01 for data cleaning and analysis. Descriptive statistics like percentage, frequency, mean median, standard deviation and IQR were undertaken to show a pregnancy-related cost of complications. By adding up the money spent on the complications during treatment follow up, the total cost of maternal complications was calculated. To identify factors independently associated with the outcome variable, simple linear regression with a p-value < 0.25 was initially used. Multiple linear regression analysis was then used to control the effect of confounding. A p-value of <0.05 with a 95% confidence interval was used to determine statistical significance.
The basic assumptions for the linear regression model were checked. Those assumptions include: A linear relationship exists between the independent variable and dependent variable (checked by scatterplot), little or no multicollinearity between variable (checked by variance inflation factor values), normality of the data (checked by histogram or a QQ Plot), No auto-correlation (checked by plotting), Homoscedasticity (scatterplot with the residuals against the dependent variable) and No Hidden or Missing Variables.
Ethical approval and consent to participate
The study was approved by the Institutional Health Research Ethics Review Committee (Ref no: IHRERC/195/2021/YYY) of College of Health and Medical Sciences, Haramaya University, Ethiopia. Before data collection, the study participants were informed clearly about the objective, benefit, and rights to participate or refuse or withdraw from the study. Their privacy was respected and confidentiality was maintained throughout the research process by giving codes for participants and omitting the names of the respondents. The informed voluntary consent with a written signature was obtained upon the agreement. The privacy and confidentiality of the participants were assured.
Results
Socio-demographic characteristics
The study enrolled 348 mothers with maternal complication, resulting in a 100% response rate. There were 39.4% Sidama ethnic background and 52% protestant religion followers among the total 348 respondents interviewed in the study. The majorities, 92.8% of the participants were married and 44.5% were house wife. Four out of five participants were urban residents, and the mean (±SD) age of respondents were 27.82 ± 6.294 (±SD) years. Three fifth of the participant had an income of <1000 birr per month, with the overall median of income of 500 ETB (Table 1).
Socio-demographic characteristics of mothers with complications attending Hawassa public hospital from November 15 to December 15, 2021 (N = 348).
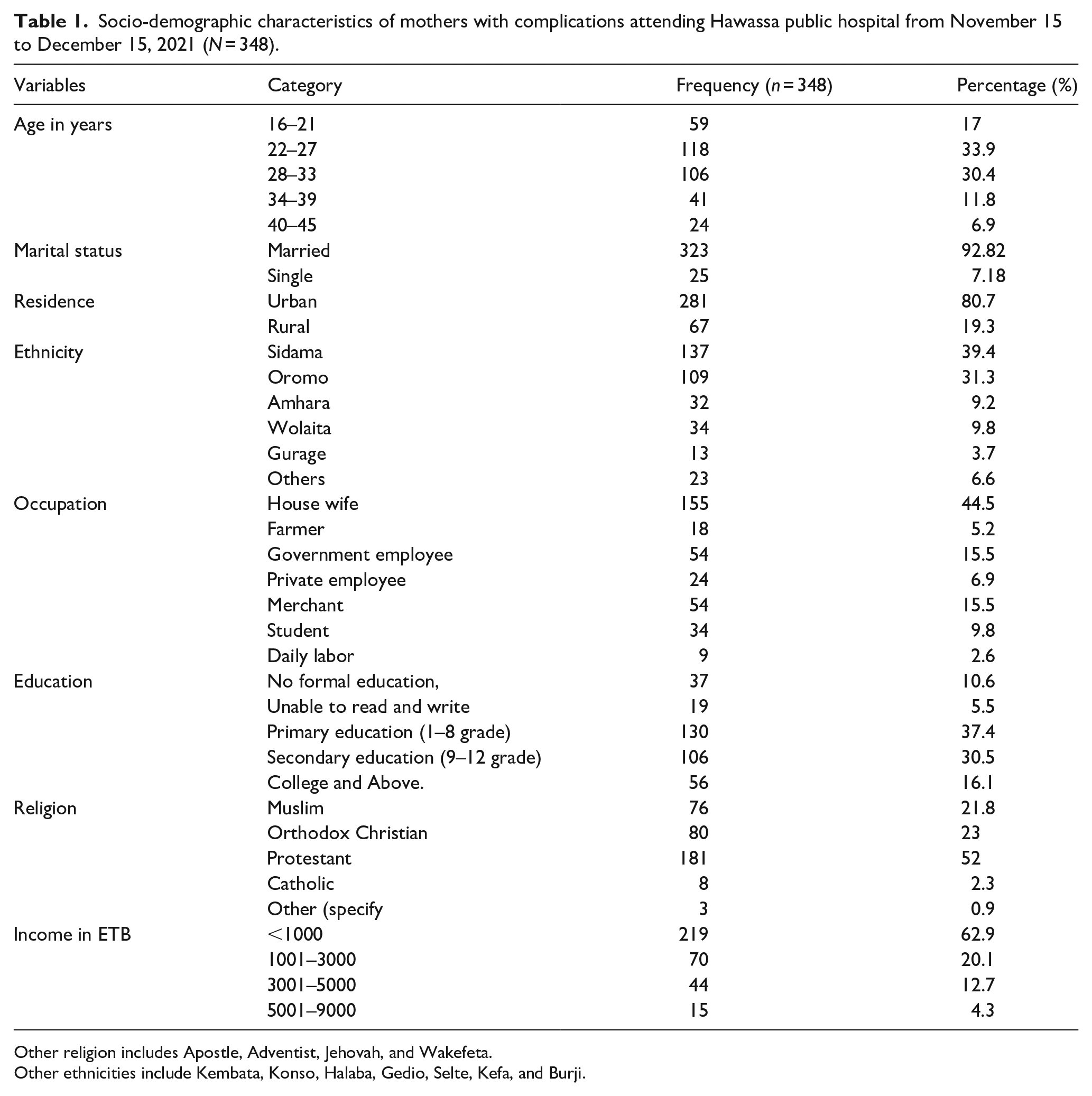
Other religion includes Apostle, Adventist, Jehovah, and Wakefeta.
Other ethnicities include Kembata, Konso, Halaba, Gedio, Selte, Kefa, and Burji.
Clinical and obstetrical characteristics of the study participants
Among the participants admitted to the hospitals with maternal complications, more than quarter (26.4%) were diagnosed with hemorrhage and three-fourth of the participants were delivered by C/Ss, almost all (97.6%) of mothers were newcomers and 2.4% have repeated hospitalizations due to their current maternal complications. Around 70.7% of the participants were multigravida and 29.3% multiparous (Table 2).
Clinical and obstetrical characteristics of maternal complications attending Hawassa public hospital from November 15 to December 15, 2021 (N = 348).

Other complications includes: PROM, Hyperemesis gravid a, Uterine rapture, Polyhydaminus,and, Oligohydaraminus.
Hospital service-related factors
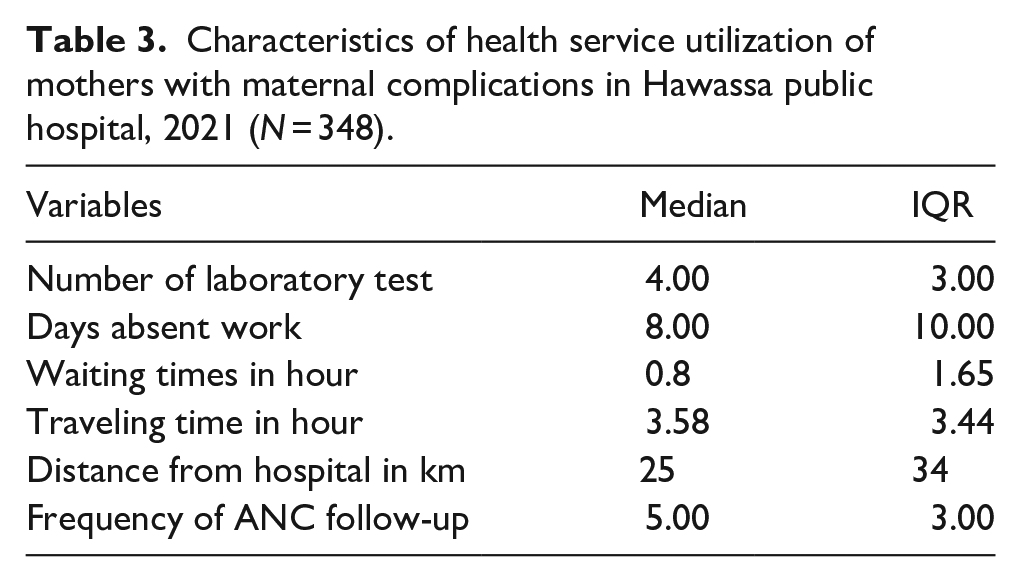
The average number of laboratory tests conducted for the study participants (N = 348) were four (IQR = 3), the number of days missed at work as a result of a complication was eight (IQR = 10), the number of ANC follow up was five (IQR = 3), the average distance from the hospital was 25 (IQR = 34) kilometer, the average traveling 3.58 (IQR = 3.44) hours and waiting time was 0.8 (IQR = 1.65) hours. More than half (55.5%) of the participant were diagnosed in the hospital and (44.5%) was diagnosed out of the hospital (Table 3).
Characteristics of health service utilization of mothers with maternal complications in Hawassa public hospital, 2021 (N = 348).
Costs for maternal complications
In this study, the median total cost of maternal complication was 4895.5 ETB (US$97.91). Direct medical cost accounted for most of the total costs which was ETB 4807.5
The median total direct medical cost of complication treatment was 1765.50 (IQR = 1649.5) ETB for all patients and, the median direct costs of the investigation was ETB 164 (IQR = 650). The median total direct medical costs spent for medication was ETB 1450.00 (IQR = 1257.5).
The median total direct non-medical costs were ETB 2840 (IQR = 2470). The direct non-medical cost includes transport costs (median, ETB 250(IQR = 225), bed /accommodation costs (median, ETB 300 (IQR = 555), food and drink ETB 1500 (IQR = 1685) and cost for a nutritional supplements ETB 490 (IQR = 450) (Table 4).
The median direct and indirect medical costs of maternal complications in Hawassa public hospitals South Ethiopia, (N = 348).

1US$ = 50ETB (US Dollar (USD) to Ethiopian Birr (ETB) Historical Exchange Rates on 11th November 2021 (11/11/2021).
According to the finding of the current study, the median total cost was ETB 4550.5. When costs were broken down by type of complication, women who experienced uterine and premature rapture of membrane spent more ETB 6838 (IQR = 2356.1) than those who experienced other types of complications. Women who had obstructed labor paid the least with ETB 3245; IQR = 2124.3.
Factors predicting the cost of maternal complications
Simple linear regression was performed to assess the crude/bivariate associations of each independent and dependent variable thereby estimating crude/unadjusted regression coefficient (β) with 95% CI. Accordingly, age, income, household income, type of visit, site of diagnosis, gravidity, parity, no of ANC follow up, distance from the hospital, waiting time, no of laboratory test and no of days missing from work were showed p-value < 0.25 with the cost of maternal complications. Consequently, these variables were selected to multivariable analysis.
Multiple linear regressions were run to control for confounding factors by estimating the adjusted regression coefficient (β) with 95% CI. In multivariable linear regression analysis variables including site of laboratory diagnosis, number of laboratory test, number of days absent from works and distance from hospital were found to be significantly associated with the cost of complication. The cost of maternal complication increases by 2.8% as the number of the mothers absent from work increase by one unit [R = 0.028; 95% CI (0.023, −0 0.033)]. Moreover, the cost of maternal complication increases by 4.5% as the number of laboratories requested increases by one unit [R = 0.0451; 95% CI (0.021, −0 0.069)]. It is founded that one unit kilometer distance increase the cost of complication by 0.1% [R = 0.001; 95% CI (0.0002, −0.002)]. Mothers who diagnosed laboratory test out of the hospital (private hospital) had 23.0% more expense compared to mothers who diagnosed in the hospital [R = 0.230; 95% CI (0.140, −0.320)] (Table 5).
Factors predicting cost of maternal complications by using multiple linear regression analysis at Hawassa public hospital from November 15 to December 15, 2021, (N = 348) Hawassa city, South Ethiopia.

Discussion
This study was conducted to estimate the cost of maternal complications and associated factors among mothers attending Hawasa public hospitals, Sidama Regional State, Ethiopia. In this study, the overall median cost of maternal complication was (median = US$97.91 or ETB 4550.5). Site of diagnosis, transport modality, number of laboratory test, number of days absent from works and distance from hospital were found to be significantly associated with the cost of complication.
The overall median cost of maternal complication in this study was (US$97.91 or 4895.5 birr). This amount exceeded the cost of a maternal complication in Northern Ghana and Central Kenya, which were (US$32.03, and 71 US$). 11 One reason for this could be the country’s present inflation, and another could be that many mothers in this study go outside of public health facilities for laboratory and medication services. However, this is lower than a study conducted in Northern Ethiopia, Uttar Pradesh and Northern Nigeria (US$176.78, US$155 and US$99.7,10 The possible reason for this might be due to the difference of complication types, because depending on types of complication lengths of stay in hospital increase, this cause increases in cost of maternal complications.
According to the findings of this study, the median direct medical cost was US$ 35.01. This finding was greater than prior studies in Northern Ghana and rural Ethiopia (Butajira), which were (US$8.68, US$26.83, and US$7.30).11,17 But lower than a study done in Mekelle, Ethiopia which was US$120.23. 7 This may be due the difference between availability of drag and laboratory service at health facility of study area.
The medians of direct non-medical cost for this study was ETB 2800 or US$ 56 these result is higher than study conducted in northern Ethiopia which was US$21. 7 This may maybe due to current inflation in Ethiopia.
In this study the distance to health facility was founded to be significantly associated with cost of maternal complication. Cost of maternal complication was high for mothers who came from long distance compared with mothers who come from short distance. Other studies in northern Ethiopia support the current study by reporting statistically significant association with the cost of treating complication. 7 This is since transportation cost increase with distance and mothers who come from long distance also expose for more cost such as bed/accommodation, food and drink costs.
Another Significant factor observed to influence cost of maternal complication was number of laboratory test requests; those who had more laboratory test requests had higher complication costs. Other studies in northern Ethiopia and Nigeria support this study, which found that the cost of a patient’s complication was higher for mother who requested more laboratory tests.7,10 The possible reasons for this might be due to the mothers were paying for laboratory when they go outside of the hospitals as well as for transportations of the sample.
When compared to patients who did not miss work due to a complication, patients who missed work increased the cost of complications. This is consistent with the research conducted in Ethiopia and Nigeria.7,10 The possible reasons for this could be that mothers who are absent from work are assumed to be very ill, need greater follow-up, medication, and hospitals. Another explanation could be that patient absences cause missed production and hence increase indirect costs.
Place of diagnosis was another factor of cost of maternal complications. Mothers who diagnosed outside of the hospital had increased the cost of maternal complication compared to their counterpart. This findings is in line with the studies conducted in Mekele northern Ethiopia, Ghana, and Uttar Pradesh, India.7,12 This might be mothers who diagnosed out of hospital were likely to expense for laboratory and for transportations of the sample.
Limitations of the study
The limitations of this study were recall bias might be overestimated or underestimate the results. The other limitation of the study was that the study was carried out only in public health facility, Intangible and non-medical costs are not included in the study which might lessen or override the burden of the cost of maternal complication.
Conclusion and recommendation
Conclusion
Respondents’ site of diagnosis, number of days missed from work, number of laboratory tests, and distance from hospitals/facility were independent predictors of maternal complications cost. Based on the finding of this study the overall median cost of maternal complications was higher than four times the monthly minimum salary which was very difficult for many households. In Ethiopia, a minimum monthly pay is US$22. There should be policies and strategies that specifically help complicated mothers, policymakers should have to give more emphasis for cost of maternal complications. Also, we recommend health sector and health professionals should regularly check the availability of maternal health drugs, equipment, and laboratory reagents to reduce maternal expenses outside of public health facility which increase cost maternal complications.
Footnotes
Acknowledgements
My heart felt thank also goes to Hawassa Specialized University Hospital, Adare hospital and Tula primary hospital public health facilities administration office for their priceless co-operation during data collection and my deep acknowledges goes to my data collectors, study participant and supervisor for their interest and commitment in carrying out the data collections.
Acronyms and abbreviations
AC: Average Cost, AFV: Average Fixed Cost, ANC: Antenatal Care, C/S: Cesarean Section, EDHS: Ethiopian Demographic Health Survey, HUCSH: Hawassa University Comprehensive Hospital, IHRERC: Institutional Health Research Ethics Review Committee, IQR: Inter-Quartile Range, MC: Marginal Cost, MNIH: Maternal-Newborn Illness- Health, MSc: Masters of Science, OOP: Out of Pocket Payment, SPSS: Statistical Package for Social Science, SVD: Spontaneous Vaginal Delivery, TC: Total Cost, TFC: Total Fixed Cost, TVC: Total Variable Cost, USD: United State Dollars, WHO: World Health Organization.
Authors’ contribution
DL, YD, BH, AA, and GA conceived the idea and designed the study, led the data analysis and interpretation, developed the first draft of the manuscript, and made all revisions. AA and TT critically revised the manuscript for important intellectual content and ensured that the requirements for submission of the manuscript were met. DL, YD, BH, AA, GA, and TT contributed to the analysis and data interpretation and revised and edited the manuscript. AA, BH and YD reviewed the expert opinions and revised the manuscript for important intellectual content. DL, YD, BH, AA, GA, and TT supervised study design and wrote the manuscript. All the authors have read and agreed to the final version of the manuscript for publication.
Availability of data and materials
All data analyzed during this study are included in the manuscript.
Consent to publish
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study was approved by the Institutional Health Research Ethics Review Committee (Ref no: IHRERC/195/2021/YYY) of College of Health and Medical Sciences, Haramaya University, Ethiopia. The informed consent with a written signature was obtained upon the agreement from participants after purpose of study had been explained. There were informed to withdraw at any time and/or to refrain from responding to questions. Study participants were also informed that all the data obtained from them could be kept confidential using code instead of any personal identifiers. Furthermore, the research procedures were conducted in accordance with the principle expressed in The World Medical Association’s Declaration of Helsinki.