
Abstract
Introduction:
Neonatal Sepsis is a significant leading cause of infant death around the world, particularly in developing nations. The study aimed to identify maternal and neonatal risk factors linked to neonatal sepsis.
Methods:
A hospital-based case-control study was conducted in the ICU. Cases were neonates diagnosed as having sepsis by clinical criteria and laboratory findings. Controls were admitted neonates who were neither suspected nor diagnosed with sepsis. Data on mothers and babies, as well as laboratory findings, were gathered and analyzed.
Results:
A total of 174 cases and 348 controls were included in the study. Maternal age, parity, route of delivery, PROM, prematurity, birth weight, neonatal gender and age were significantly associated with the risk of sepsis (p < 0.05). However, the bivariate logistic model revealed that the most influential predictors of neonatal sepsis were premature rupture of membranes, Gestational age, Neonatal age, birth weight, and mode of delivery.
Conclusion:
Both maternal and neonatal variables were found to have a significant association with the risk of neonatal sepsis; thus, empowering mothers to pursue antenatal care may allow the detection of risk factors for undesirable delivery consequences such as neonatal sepsis, as well as appropriate management to mitigate those risks.
Introduction
Neonatal sepsis remains a global problem causes high neonatal morbidity and mortality in industrialized and developing countries, killing more than 3 million neonates annually, in spite of advances in health care facilities.1,2 A systematic review revealed that, the survivors of neonatal sepsis are at twice the risk of short and long-term neurodevelopmental morbidity. 3
Neonatal sepsis is a clinical syndrome presented by systemic signs of infection affects infant aged 28 days or younger and confirmed by isolation of bloodstream bacterial pathogen. 4
Neonatal sepsis classified as early onset (in the first 3 days of life) or late onset (after third day of life). Of neonates with early-onset sepsis, 85% occurred within 24 h, 5% are within 24–48 h, and a lower percentage is within 48–72 h. In premature neonates, it is mostly rapid onset. 5
Neonatal Sepsis diagnosis and treatment are a significant challenge facing neonatal health care provider. Due to vary, subtle, nonspecific manifestations, the clinical diagnosis is very difficult. Moreover, laboratory diagnosis is time consuming. This problem necessitates the starting of excessive and empirical antibiotic use till the suspected sepsis is excluded. At the same time, increased multidrug resistant species limit therapeutic options and hinder effective treatment. 6
The variety of sepsis-causing species ranges from developing to developed countries and from region to region and differs also in the same area over time Gram-positive and Gram negative bacteria and Candida are responsible for neonatal sepsis with majority caused by gram-negative organisms in low resources region. This is due to the emerging antimicrobial resistance trend of antibiotic use and lifestyle changes.7,8
Several maternal and neonatal factors had been contributed to the susceptibility of the neonate to sepsis. Maternal variables include socioeconomic status premature rupture of membranes (PROM), intrapartum infection and fever, amniotic fluid turbidity and meconeal amniotic fluid, and multiple gestations.9,10 Neonatal variables are sex, premature (gestational age <37 weeks), low birth weight, long hospital stay in neonatal intensive care unit (NICU), asphyxia, ventilation, invasive procedure, congenital anomalies, parenteral nutrition.11,12
The study aimed was to identify maternal and neonatal risk factors associated with neonatal sepsis.
Methods
Study design and setting
A hospital based retrospective case control study carried out during the period from June 2020 to May 2021. The study included 522 neonates aged <28 days who were delivered in the study hospital and admitted to neonatal intensive care unit (174 neonates with sepsis (chosen as cases) and 348 neonates without sepsis (chosen as controls)).
Epi program (version 7.2.1) was used to determine the appropriate sample size. 95% confidence interval, 80% power of the study, 1:2 ratio of case to control to reveal an assumed odds ratio of 2 with 10% nonresponse rate. As a result, 174 cases and 348 controls (522 was a total sample size) were suitable.
Inclusion and exclusion criteria
Cases were neonates having clinical picture of sepsis and who had a positive blood culture.
Temperature instability, lethargy, feeding intolerance, respiratory distress, hemodynamic instability, convulsion, hypotonia, irritability, or bleeding diathesis were all signs of sepsis. 13 Prematurity (37 weeks), low birth weight (2000 g), history of resuscitation at birth, rupture of membrane for more than 18 h (PROM), antepartum fever, foul-smelling liquor, and frequent (three or more) dirty per vaginal inspections were all considered risk factors for neonatal sepsis.
Neonates who were delivered in the study hospital and admitted to the neonatal intensive care unit for reasons other than neonatal sepsis, such as low birth weight, neonatal jaundice, diarrhea, and so on. During the research period, they were selected as controls.
Exclusion criteria: Neonates who were delivered outside or who were clinically suspected of having sepsis but whose diagnosis was not confirmed by a hematological test or a positive blood culture were excluded from our study.
Statistical analysis
SPSS version 21 was used for data analysis and chi-square test was used to test any differences between the categorical variables. The predictors variables of neonatal sepsis were also determined using a multivariate regression analysis and p-value of less than 0.05 was considered statistically significant.
Results
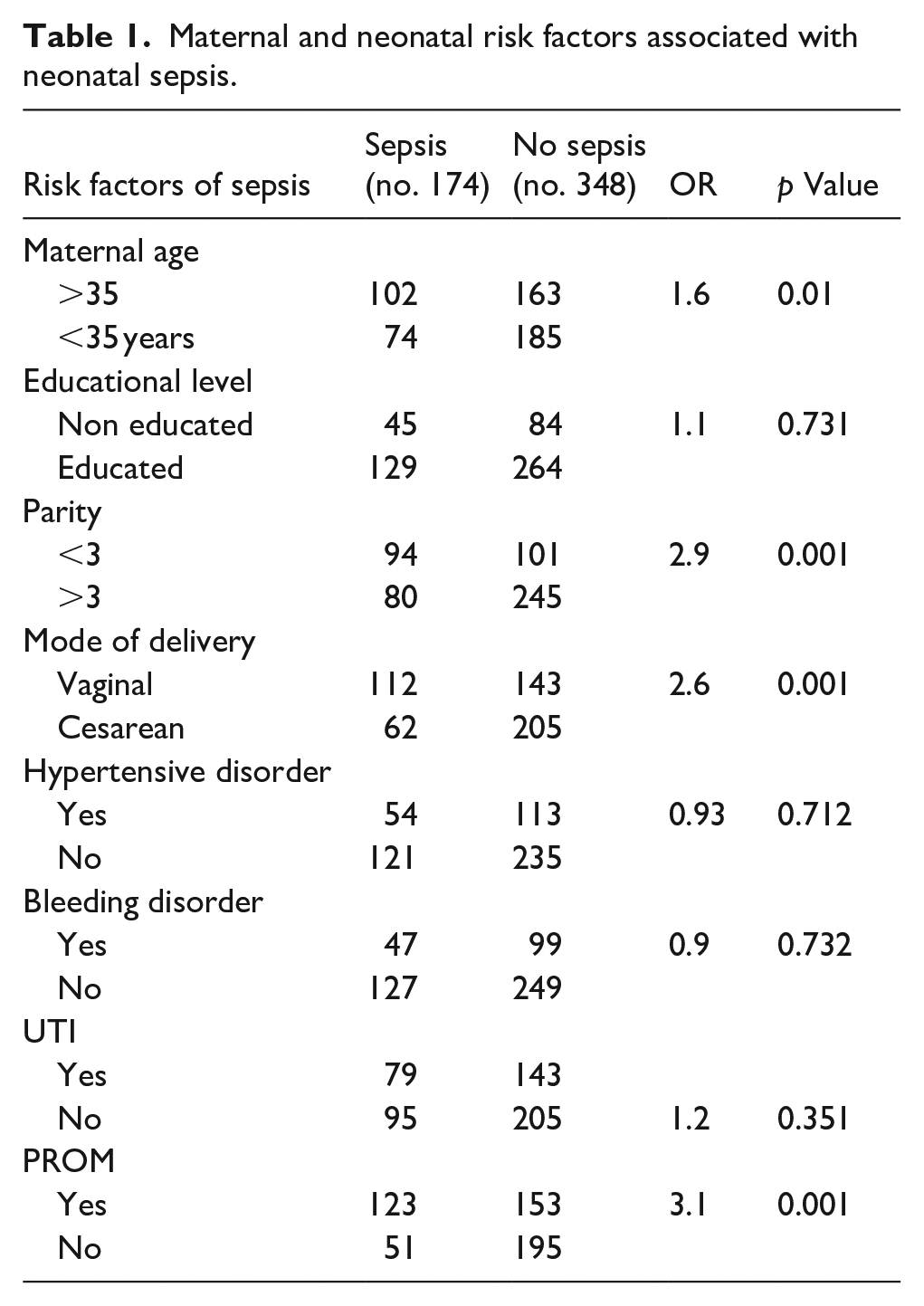
A total of 522 neonates with their mothers were enrolled (174 neonates who had sepsis (chosen as cases) and 348 newborns who did not have sepsis (chosen as controls)). The risk of newborn sepsis was significantly related to parity (p < 0.027). The study found that primiparous mother was 2.9 times more likely to having neonates with sepsis as compared to multiparous mother. Regarding the route of delivery the CS highly associated with neonatal sepsis (p < 0.001) and neonates delivered through CS were 2.5 times more risk to having sepsis compared to those vaginally delivered neonates. Premature rupture of membrane (PROM) has been associated with a higher risk of newborn sepsis (p < 0.001) (Table 1).
Maternal and neonatal risk factors associated with neonatal sepsis.
Regarding neonatal factors, our study showed that, males were at 1.7 times more risk to show neonatal sepsis compared to females. Also low birth weight neonate was 3.5 times more likely to neonatal sepsis (p < 0.001). Prematurity (<37 weeks of pregnancy) associated with 3.4 time more risk of neonatal sepsis compared to maturely neonate. Also APGAR scores (<7) showed significant link with the risk of newborn sepsis (p < 0.001). Neonatal age associated with the risk of developing neonatal sepsis (p = 0.03) (Table 2).
Neonatal risk factors associated with neonatal sepsis.

No significant association was revealed between urinary tract infection, vaginal bleeding during pregnancy, and Hypertensive disorder and the risk of neonatal sepsis (Table 1).
However, bivariate logistic model revealed that the most influential predictors of neonatal sepsis were premature rupture of membranes (OR = 5.2, CI = (1.8–6.2)), Gestational age (OR = 4.4, CI = (1.4–7.3)), Neonatal age (OR = 3.6, CI = (1.2–5.7)), birth weight (OR = 2.7, CI = (1.8–6.9)), and mode of delivery (OR = 2.2, CI = (1.5–7.8)) (Table 3).
Multivariate logistic regression analysis of risk factors for neonatal sepsis.

Adj. OR: adjusted odds ratio; CI: confidence interval.
Discussion
The risk of neonatal sepsis was statistically related to Cesarean section delivery, which is in line with Utomo’s study 14 who reported cesarean section delivery related to the develop of neonatal sepsis. Although newborns delivered via CS are not exposed to vaginal or fecal bacteria, they often have a longer hospital stay and a later start to breastfeeding. The current study finding showed that premature rupture of membrane (PROM) was significantly associated with the risk of neonatal sepsis which in agreement with other study in Bangladesh and Nepal.15–17 That is may explained by increased the risk of the chance of ascending infection from the birth canal into the amniotic fluid.
The present study is in line with Adatara et al. 15 and Siakwa et al., 10 they found parity (primiparous) significantly linked with the occurrence of neonatal sepsis, as parity increases neonatal sepsis decreases. It may be explained by prolonged delivery duration among primiparous compared to multiparous, which increases exposure to infection.
Maternal age above 35 years was a predisposing risk factor for neonatal sepsis, which as reported by Mogollón et al. 18 study. Maternal age (more than 35 years) is linked to a higher risk of poor baby outcomes. It may explained by, maternal age greater than 35 years is linked to the occurrence of significant medical health problems related to pregnancy, such as gestational hypertension, diabetes, cardiac disease, congenital abnormalities and genetic problems, multiple pregnancies, premature birth.
Our study revealed that neonates gender significantly associated with neonatal sepsis, which in agreement with Adatara et al. 15 results which reported that, males neonates were at more risk compared to females. But our results inconsistent with a hospital based cross-sectional study in Nepal. 16
APGAR scores was associated with the risk of neonatal sepsis. This is supported by previous studies with the results of a previous study conducted in Ghana and Ethiopia.15,18
Prematurity predispose to high risk of neonatal sepsis which is in agreement Yismaw et al. 19 and Manandhar et al. 20 results that is may due to underdeveloped innate immune responses as well as a lack of maternally produced, passively acquired antibodies.
Our study illustrated that neonates age associated with a risk of sepsis which in consistency with Yadav et al. 17 result but in contrast to Rafi et al. study. 16
Our study found no significant relation between maternal education level and the risk of neonatal sepsis. This result agrees with Adatara et al. 15 and Siakwa et al., 10 but differs from previous study by Shah et al., 21 who found that maternal education was statistically associated to the risk of newborn sepsis in a case control study in Nepal. In comparison to their non-educated mother, maternal education is intended to boost mothers’ awareness of healthy infant care and improve hygiene habits in order to prevent sepsis.
Conclusion
Both maternal and neonatal variables were found to have a significant association with the risk of neonatal sepsis; thus, empowering mothers to pursue antenatal care may allow the detection of risk factors for undesirable delivery consequences such as neonatal sepsis, as well as appropriate management to mitigate those risks.
Footnotes
Correction (March 2024):
Affiliations order for author Basem Salama has been updated since its original publication. No change has been made in the affiliations.
Author contributions
Authors responsible for all parts of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.