
Abstract
Background:
The aim of this study was to analyze the influence of sociodemographic and clinical variables as determinants of mortality and survival in patients with ST-segment elevation acute myocardial infarction in the Eastern Amazon.
Design and methods:
This observational, longitudinal, and retrospective study was conducted at the Gaspar Vianna Clinical Hospital Foundation in patients hospitalized from January 2017 to June 2020. Patients were divided into two groups: those who survived (G1) (n = 646) and those who died (G2) (n = 37). Sociodemographic and clinical variables associated with mortality and survival in these two groups were analyzed.
Results:
Patients with STEMI who had the highest risk of death were often the oldest (G1: 61.58 ± 10.74 years; G2: 69.57 ± 9.02 years; t = −4.492; p = 0.001), with Killip III-IV classifications (OR = 0.13; 95% CI = 0.02–0.71; p = 0.03), and with diseases such as heart failure (OR = 0.07; 95% CI = 0.004–1.50; p = 0.168) or renal failure (OR = 0.03; 95% CI = 0.006–0.16; p = 0.0001). In addition, female sex (hazard ratio = 2.073; 95% CI = 1.413–5.170), Killip III-IV classifications (hazard ratio = 4.041; 95% CI = 1.703–18.883) and the presence of heart failure (hazard ratio = 34.102; 95% CI = 4.410–263.684) or renal failure (hazard ratio = 14.278; 95% CI = 3.275–62.248) shortened in-hospital survival.
Conclusions:
Specific sociodemographic and clinical aspects influenced mortality and survival in patients with acute ST -elevation myocardial infarction.
Introduction
ST-segment elevation myocardial infarction (STEMI) is an acute coronary syndrome (ACS) under the umbrella of cardiovascular diseases (CVDs) that requires special attention. A STEMI is characterized by occlusion and interruption of all blood flow in one or more coronary arteries. The reason for this sudden interruption of blood flow is usually plaque rupture, erosion, rupture, or dissection of the coronary artery leading to obstructive thrombosis. This condition requires short-term initiation of treatment, preferably by primary percutaneous coronary intervention (PCI). 1
Recently, CVDs, particularly ischemic heart disease, has become a leading cause of death worldwide2,3 and the World Health Organization indicates that the burden of cardiovascular disease has increased recently, particularly in low- and middle-income countries. Approximately 80% of deaths and 88% of premature deaths due to cardiovascular disease occur in these countries,3,4 which is due to increased life expectancy and thus higher exposure to risk factors for chronic noncommunicable diseases. 5
ACS is the third leading cause of hospitalization in Brazil; according to previous studies, mortality after STEMI ranges from 15% to 20%. Compared with other underdeveloped countries, there is a significant delay from the onset of symptoms to presentation to the emergency department and the first electrocardiogram examination. Thus, sociodemographic levels and initial care in nonspecialized health facilities are associated with worse outcomes. In general, these aspects contribute to the lack of improvement in the treatment of STEMI according to national and international guidelines. 6
The sociodemographic context of the Eastern Amazon makes access to health care difficult for people in this region. With a vast territory and highly complex health services concentrated in the main cities, access to specialized emergency cardiology care is difficult for vulnerable populations, including the poorest, members of the quilombola, residents of the riverbanks, and indigenous communities.7,8 Therefore, these individuals end up moving through areas of forests, mangroves and rivers and, most of the time, depend on the availability of ambulances, boats or air medical transport to travel long distances. 9
Patients with STEMI require attention for their condition during and after treatment due to the high mortality risk. 2 Several studies have shown reduced survival according to patient-related factors; hence, understanding these factors better can contribute to improved case management and reduced morbidity and mortality.10–12
Currently, in Brazil and in the Amazon region, there is a lack of recent studies on the impact on mortality and survival of patients with STEMI, with no similar studies on the subject in the population of the Eastern Amazon, perhaps due to the scarcity of cardiology reference centers linked to research in this region. Therefore, more studies specific to the population in this region are necessary for the implementation of public health policies and healthcare strategies for patients with STEMI.
This study aimed to analyze the influence of sociodemographic and clinical variables as determinants of mortality and survival in patients with STEMI in the Eastern Amazon.
Methods
Ethical aspects
The study was conducted in compliance with all ethical principles for research according to the Declaration of Helsinki. All patients gave informed, written consent to participate in the study. This study was approved by the Ethics and Research Committee of the Gaspar Vianna Clinical Hospital Foundation (protocol no. 1,879,297).
Study design
This was an observational retrospective case-control study with descriptive and inferential analyses.
Study setting
This study was conducted in Gaspar Vianna Clinical Hospital Foundation based on the records of the Good Clinical Practices in Cardiology program. 13 This hospital is a public reference in cardiology in the state of Pará, in the Eastern Amazon region in Brazil. 14
Sampling
The sampling was non-probabilistic, and all individuals in a given population were studied.
Sample size
The sample size was calculated according to Cosentino et al. 15 for difference between two independent means. The variables “Age (year)” were used as references. The values were: Effect size d = 0.78, error probability α = 0.05, β = 0.20, and allocation ratio N2/N1 = 1.65 for two-tail test. The minimum sample size defined was 56 participants included in the study (G1 [n = 34] and G2 [n = 22]).
Study population
The sample consisted of 683 medical records of patients with acute STEMI aged >18 years that were hospitalized from January 2017 to June 2020 in the Gaspar Vianna Clinical Hospital Foundation. Patients were categorized into two groups: those who survived (G1) (n = 646) and those who died (G2) (n = 37). The clinical outcomes in these two groups were analyzed.
Inclusion criteria
Patients over 18 years of age, had a principal diagnosis of acute coronary syndrome, gave informed consent to participate in the study, and were admitted to Gaspar Vianna Clinical Hospital are included in the “Good Clinical Practice in Cardiology” program. 13 Of these patients, those who were diagnosed with STEMI, had chest pain within 12 h <, and were referred to the primary PCI were included in the study.
Exclusion criteria
Patients who were diagnosed with other types of myocardial infarction or presented with other factors not indicative of urgent coronary reperfusion and those without determinant variables for the survival analysis (length of hospital stay and mortality) were excluded.
Study variables
Sociodemographic and clinical variables were also assessed. The collection of data of medical records from the hospital was manually performed. The sociodemographic variables analyzed were the sex, age, ethnicity, schooling, and family income (minimum wage, considering that Brazil is a country with upper middle income according to The World Bank 16 ). The clinical variables analyzed were lifestyle habits, hemodynamic variables, comorbidities, values of enzymes related to cardiac function, Killip classification, 17 door-to-balloon time, 18 hospital stay, and mortality.
The lifestyle habits evaluated were smoking history, alcoholism, sedentary lifestyle, and dependency levels on activities of daily living. The hemodynamic variables considered were the heart rate (HR), 19 systemic blood pressure, and diastolic blood pressure. 20 The comorbidities analyzed were systemic arterial hypertension, type 2 diabetes mellitus, dyslipidemia, stroke, unstable angina prior to infarction, chronic heart failure (HF), and chronic kidney disease (CKD) (for patients undergoing dialysis). The biomarkers analyzed were creatinine, 21 initial troponin, initial total creatine kinase (CK), initial creatine kinase-MB isoform (CK-MB), 18 low-density lipoproteins and high-density lipoproteins. 22 Regarding the door-to-balloon time, patients (n = 558) who had successful angioplasty of the artery responsible for the STEMI were considered.
Statistical analysis
Descriptive numerical data were presented according to the normality of the data (mean and standard deviation [parametric data] or median and 95% confidence interval [95% CI] [nonparametric data]). Normality of the data was tested with the Kolmogorov-Smirnov test. Mean age between groups was compared with the unpaired t test. Medians of hemodynamic variables and biomarkers were compared with the Mann-Whitney test.
Descriptive categorical data were presented as absolute and relative frequencies (%). The level of association between categorical variables was analyzed by the chi-square (χ²) test with Yate correction. The level of association was determined by odds ratio (OR) and 95% CI.
Log-rank, Breslow, and Tarone-Ware tests were used to analyze the independent variables along with Kaplan-Meier survival curves. Significant variables were presented in graphs and analyzed with the Cox regression model to estimate the prevalence of the event during the study period using Exp analysis (B) and 95% CI.
A statistical significance level of p ≤ 0.05 was set for all analyzes. These were performed using SPSS Statistics for Windows (version 21.0; IBM Corp., Armonk, New York, USA).
Results
Determinants of mortality in patients with STEMI
The results of the sociodemographic data analysis are presented in Table 1. There was a significant difference in sex, with a higher proportion of men in G1 and women in G2. It was observed that the mean age of the patients who died was higher than those who survived (G1: 61.58 ± 10.74 years; G2: 69.57 ± 9.02 years; t = −4.492; p 0.001). The other variables were not statistically significant.
Sociodemographic variables of patients with ST-segment elevation myocardial infarction that survivors (G1) or who died (G2).
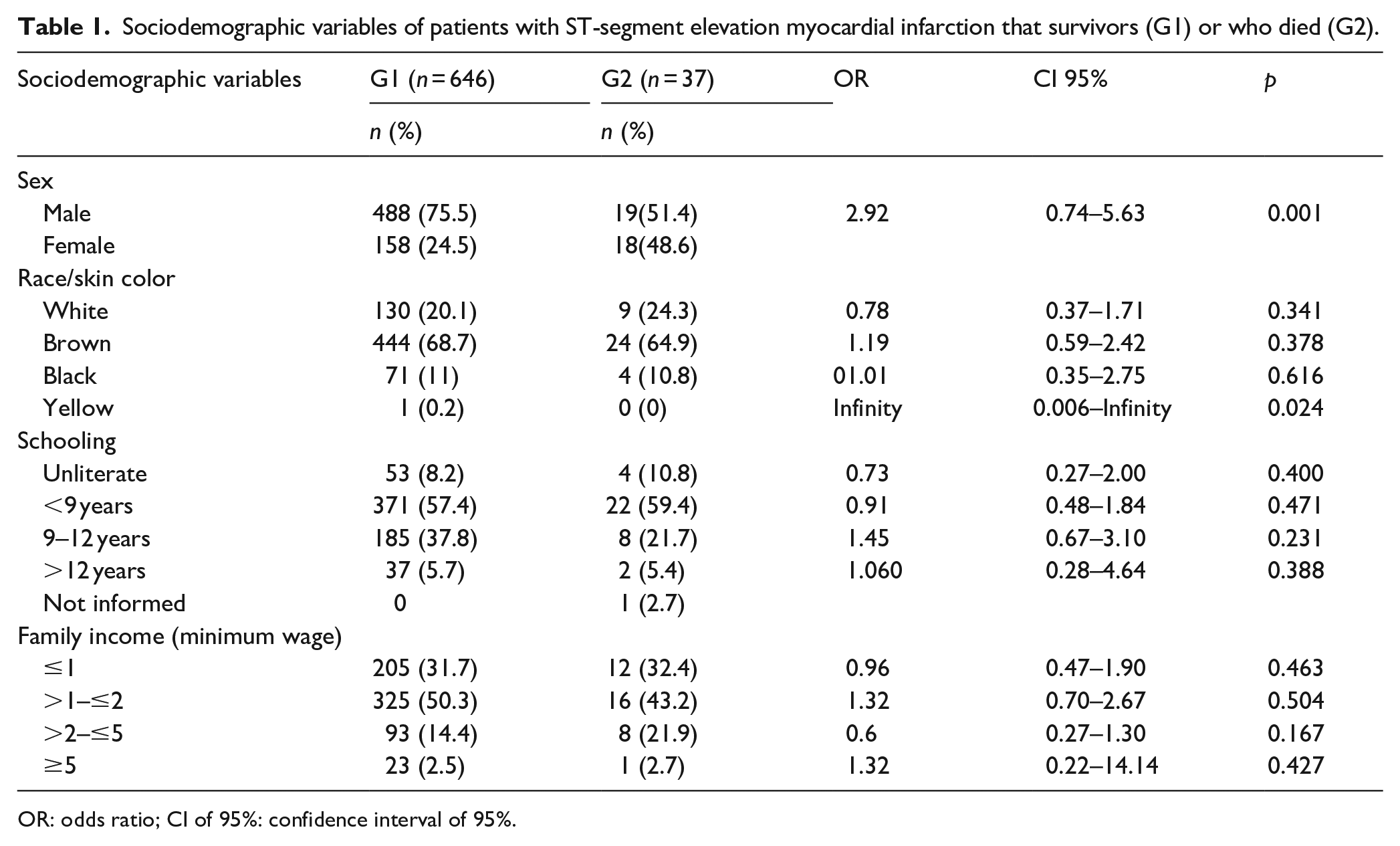
OR: odds ratio; CI of 95%: confidence interval of 95%.
The clinical variables are shown in Tables 2 and 3. Regarding lifestyle habits, alcoholism was more prevalent in G1. In addition, patients in G1 were able to perform activities of daily living independently, whereas patients in G2 were partially dependent in these activities (Table 2). The HR at hospital admission was significantly higher in patients who died than in those who survived (Table 3). CKD (patients undergoing dialysis) and Killip classifications III-IV were associated with in-hospital mortality (Table 2). Serum creatinine levels were higher in patients who died than in those who survived (Table 3). The other variables were not statistically significant.
Categorical clinical variables of patients with ST-segment elevation myocardial infarction that survivors (G1) or who died (G2).

OR: odds ratio; CI of 95%: confidence interval of 95%; SAH: systemic arterial hypertension; DM: type 2 diabetes mellitus; HF: chronic heart failure; CKD: chronic kidney disease.
Numerical clinical variables of patients with ST-segment elevation myocardial infarction that survivors (G1) or who died (G2).

CI of 95%: confidence interval of 95%. Variables (Normal values): HR: heart rate (50–100 bpm) 19 ; SBP: systemic blood pressure (120–129 mmHg); DBP: diastolic blood pressure (80–84 mmHg) 20 ; Creatinine (0.6–1.3 mg/dL) 21 ; LDL: low density lipoproteins (<130 mg/dL); HDL: high density lipoproteins (>40 mg/dL) 22 ; Initial troponin (<0.01 ng/mL), Initial total CK: total creatine kinase (female: <150 U/L; males: <200 U/L); CK-MB: creatine kinase-MB (<5 ng/mL). 18
Determinants of survival in patients with STEMI
Figure 1 shows the survival curves. It was observed that women (hazard ratio = 2073; 95% CI = 1.413–5.170), HF (hazard ratio = 34.102; 95% CI = 4.410–263.684), CKD (patients undergoing dialysis) (hazard ratio = 14.278; 95% CI = 3.275–62.248), and Killip classifications III–IV (hazard ratio = 4.041; 95% CI = 1.703–18.883) were with lower survival at all times in the Kaplan–Meier survival curves.

Kaplan-Meier survival curves of patients hospitalized with ST-segment elevation myocardial infarction, according to sex (a), heart failure (b), chronic kidney disease (c) and Killip classification (d), being performed Cox regression (e).
Discussion
CV CVDs are linked with several risk factors. However, many of these factors, both nonmodifiable and modifiable, may also be associated with mortality in patients with acute myocardial infarction. A prospective multinational cohort study examined the associations of 14 potentially modifiable risk factors with mortality and CVDs in 155,722 participants with no history of CVDs in 21 high-, middle-, or low-income countries and indicated an association with factors such as smoking, alcoholism, and low educational level. 23 Other studies have also found an association with comorbidities such as diabetes, hypertension, peripheral arterial disease, impaired renal function, history of stroke, and Killip classification, as well as nonmodifiable risk factors such as sex and advanced age.24–26
This study showed a slight difference in the number of deaths associated with sex; in-hospital mortality tended to be higher in men than in women. This was consistent with other studies that indicated a higher incidence of STEMI and consequently higher mortality in men than in women. In a study by de Medeiros et al., 27 a high mortality rate was found in men. In addition, Santos et al. 25 showed that in most Brazilian regions, the male sex was associated with a higher number of reported deaths, which was related to the fact that women receive more care and use more health services than men because of sociocultural issues and issues related to the construction of the identity of both. 24 Historically, women were taught from an early age to take care of their own health for sexual and reproductive reasons, while men have been encouraged to grow up with a false notion of invulnerability. 28
Regarding the effect of age, this study found a higher mortality rate in older patients, in line with the study by Santos et al. 25 that found a progressive increase in mortality rates with advancing age in both sexes in Brazil and in all regions. This may be directly related to the accumulation of exposure to risk factors throughout life, which in turn may increase the incidence in more advanced age groups. 23
According to a study by Fonseca and Freire, 29 the presence of CKD has been found to be one of the strongest risk factors for mortality in patients with STEMI undergoing PCI. The development of CKD is associated with reduced survival and increased risk of adverse events. It is worth noting that the risk of cardiovascular events in patients with CKD has been shown to be 20–100 times higher than in the general population and that the risk of mortality in patients with end-stage CKD is approximately 50%. 30 This also reflected in this study, as it was found that patients undergoing dialysis have a higher mortality rate.
Regarding Killip classification, patients with a Killip classification III or IV were found to have higher mortality, which is consistent with the study by Paiva et al. which found that patients with a Killip classification III or IV had larger areas of necrosis, remodeling and ventricular systolic dysfunction and probably a greater extent of coronary artery disease. This highlights the association between higher Killip classification and increased risk of death. It is worth noting that Killip classification has been shown to be a strong predictor of prognosis, with the risk of death increasing twofold with each worsening of the class. 31
Among the factors related to lifestyle in this study, alcoholism was more prevalent in patients who survived. However, it is known that alcoholism is one of the major risk factors for cardiovascular disease 32 and may also be associated with mortality in patients with AMI. This was demonstrated in a study of 610 963 patients, which showed a 5.3% in-hospital mortality rate, and alcohol-related diagnoses were associated with an increased risk of death in patients with AMI; this association was significant in patients with STEMI (adjusted OR = 1.7; 95% CI = 1.4–2.2; p < 0.001) and in patients without ST -elevation myocardial infarction (adjusted OR = 1.3; 95% CI = 1.0–1.7; p = 0.025). 33 However, other studies have also shown the association of other lifestyle factors with mortality, such as smoking 34 and physical inactivity. 35
In addition to the factors already presented, Hou et al. pointed out other factors associated with in-hospital mortality, such as cardiogenic shock, increased serum levels CK-MB, and increased risk scores. 26
The factors that determined higher or lower survival in patients with STEMI were consistent with other national 36 and international26,37,38 studies that showed worse survival in women with conditions such as HF and CKD and in women with a high Killip classification at hospital admission.
This study showed that men had better survival rates during hospitalization. Previous studies examining differences in survival between the sexes also showed higher short- and medium-term survival in men than in women.36,37,39 A study conducted in Rio de Janeiro that examined the survival of 19,263 patients with STEMI indicated that women had worse survival than men when followed up at 30 days and 1 year. However, they had better survival rates at 15 years, particularly in the age group ≥70 years 36. Studies from Europe have shown similar results. A study by Berg et al., which considered a population of 658,110 hospitalized patients at AMI, showed that women aged <65 years had a higher risk of death at 28 days than men. 37 Although this study did not consider long-term survival of patients with STEMI, longitudinal studies conducted over a period of up to 10 years have also shown a similar trend.36,37,39,40
The poorer survival rate in women can be explained by the fact that concomitant diseases, especially diabetes, are more common in young women than in men of the same age who develop AMI. Women are more likely to have atypical symptoms and non-obstructive coronary artery disease on angiography. These patients are less likely to receive guideline-based therapies. Women also have higher rates of periprocedural complications associated with PCI and are less likely to be referred for cardiac rehabilitation, increasing their risk for poorer survival over time.37,39,41
Regarding the presence of concomitant diseases, patients with HF and CKD had poorer survival during hospitalization. These are chronic diseases associated with a worse prognosis in hospital in patients with AMI. 38 As shown in an analytic cohort study of patients in the United Kingdom (n = 693,388), patients with chronic HF (hazard ratio = 1.87,95% CI = 1.81–1.93; mean time to death = 131.49 days, interquartile range, IQR = 18.3–518.0), cerebrovascular disease (hazard ratio = 1.77,95% CI = 1.72–1.82; mean time to death = 142.5 days, IQR = 14.6–573.4) and CKD (hazard ratio = 1.73,95% CI = 1.67–1.79; mean time to death = 116.9 days, IQR = 18.3–449.3) were independently associated with lower survival and higher risk of death. 12 Another study conducted in the same country (n = 210,392) showed that the comorbidities that negatively affected survival were CVDs and HF. 10
In terms of Killip classification at hospital admission, this study showed that those classified as Killip III and IV had poorer survival. Other studies have shown similar results, such as that of Mello et al., which demonstrated that Killip classifications II (hazard ratio = 1.47; 95% CI = 0.99–2.17), III (hazard ratio = 1.93; 95% CI = 0.918–4.05) and IV (hazard ratio = 2.32; 95% CI = 1.19–4.50) had poorer survival outcomes at 30-day follow-up with increasing classification. 17 Similarly, the study by Hou et al. that Killip classifications III-IV were associated with worse survival and higher in-hospital mortality (hazard ratio = 5.33; 95% CI = 1.53–18.62). 26 Although this study did not include assessment of medium- and long-term survival, similar results were observed in studies with 6-month 42 and 3-year follow-up regarding the association between increasing Killip classification class and higher mortality risk. 26
It is important to emphasize that the determining factors are not limited to those presented in this study. Hou et al. also identified cardiogenic shock and high GRACE risk scores 43 as responsible for poorer survival in patients after AMI. 26 This highlights the importance of conducting further national studies with a larger number of variables and longer follow-up periods.
Limitations of this manuscript include the concentration of STEMI cases in a population from a specific region of the Brazilian Amazon in a single center, which means that the results are not generalizable. In addition, the study was conducted using secondary data from the Good Clinical Practise in Cardiology program registry, taking into account the risk of failure in the primary collection of patient information and the fact that there are few studies on this topic in Brazil. This shows the importance of conducting multicenter studies taking into account the population profile.
Conclusions
In conclusion, the patients with STEMI who had the highest risk of mortality were often the oldest and had HF and CKD. As for lifestyle-related factors, alcoholism was more common in patients who survived, which contradicts the results of previous studies. In addition, female gender, Killip classification III-IV and the presence of HF and renal failure influenced the reduction in hospital survival.
Most of the results of this study were consistent with those of larger international studies. Despite the vulnerability of the study population and regional characteristics, no other sociodemographic factors were identified as determinants of mortality and survival in patients with STEMI, with the exception of gender, which was generally related to clinical conditions.
Therefore, identifying and understanding these determinants can contribute to the development of public policies aimed at strengthening cardiac care in the context of the Eastern Amazon population, prioritizing multidisciplinary care for prevention and reducing determinants of health in places with greater social inequalities. Aiming to promote better adherence to health guidelines and healthy lifestyle habits to reduce hospitalizations and readmissions.
Footnotes
Author contributions
Conceptualization: TA, JMN. Data curation: TA, KP, CZ, SO. Formal analysis: TA, TM, GM. Methodology: TA, JMN. Project administration: JMN. Visualization: TA, KP, CZ, SO. Writing – original draft: TA, TM, GM, RS. Writing – review & editing: TA, JMN, TM, GM.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study was conducted in compliance with all ethical principles for research according to the Declaration of Helsinki. All patients gave informed, written consent to participate in the study. This study was approved by the Ethics and Research Committee of the Gaspar Vianna Clinical Hospital Foundation (protocol no. 1,879,297).
Significance for public health
The sociodemographic context of the Amazon region makes access to health care difficult for the people who live there. Given the vast territory made up of these forests and rivers, and the highly complex health services concentrated in the main cities, access to emergency care specialized in cardiology is difficult for vulnerable populations, including the poorest, quilombolas, riverbanks, and indigenous communities. In general, these problems contribute to the lack of improvement in the treatment of STEMI according to national and international guidelines for the management of this disease. This can be a serious public health problem in a region of continental proportions. Understanding the epidemiology of acute myocardial infarction in this reality contributes to the development of targeted public policies that strengthen the public health system in the region.
Availability of data and materials
The data presented in this study are available upon request from the corresponding author.