
Abstract
Background:
Little is known about the management and mortality rates of ST-segment elevation myocardial infarction patients in developing countries. In this study, to expose independent predictors of early (24 h) in-hospital mortality and ejection fraction, we report our experience with 362 ST-segment elevation myocardial infarction patients admitted to the Istanbul Medical Faculty, Istanbul University, a tertiary referral university hospital, and treated with primary percutaneous intervention.
Methods:
This is a retrospective study that enrolled all patients (362) admitted with ST-segment elevation myocardial infarction to Department of Cardiology, Istanbul Medical Faculty, Istanbul University, between January 2015 and December 2016. The clinical characteristics of patients were collected retrospectively from medical chart review. Collected data were analyzed using IBM SPSS Statistics (version 21).
Results:
In the forward stepwise logistic regression analysis, target vessel diameter (p = 0.001), systolic blood pressure (p < 0.001), and troponin T levels (p = 0.007) were independent predictors for early in-hospital mortality, while target vessel diameter (p = 0.03), troponin T level (p < 0.001), heart rate (p = 0.001), and chest pain (p = 0.001) duration were the independent predictors for ejection fraction of 50% and above.
Conclusion:
Our study is one of the few studies to investigate the predictors of early in-hospital mortality among patients hospitalized with ST-segment elevation myocardial infarction in a tertiary referral university hospital in a developing country. The identified predictors for mortality (including left ventricle ejection fraction and troponin T levels), left ventricle ejection fraction (including troponin T level, chest pain duration), and heart rate are consistent with what has been described in large registries in the United States and Europe.
Keywords
Introduction
ST-segment elevation myocardial infarction (STEMI) represents one of the major causes of morbidity and mortality worldwide. 1 Several recent studies have emphasized a decrease in acute and long-term mortality following STEMI in parallel with more use of reperfusion therapy, such as primary percutaneous coronary intervention (PCI), modern antithrombotic therapy, and secondary prevention.2–4 However, mortality remains considerable; the in-hospital mortality of patients with STEMI in the national registries of the European Society of Cardiology (ESC) countries varies between 4% and 12%. 5 Several investigations in the United States and Europe have examined the predictors of in-hospital mortality following acute myocardial infarction.6–11 Several parameters are known to be related to the clinical characteristics of the patients and their comorbidities.7,8,11–14 Among the parameters that influence a patient’s morbidity, mortality, and life quality, ejection fraction (EF) is one of the most important. Similar reports on acute myocardial infarction patients in developing countries are limited, 15 and little is known about the management and mortality rates of such patients in these countries. 16 In this study, we report our experience with 362 patients who were diagnosed with persistent STEMI and treated with primary percutaneous intervention in our catheter laboratory of Department of Cardiology. We analyzed the clinical spectrum, angiographic characteristics, treatments, and management of patients. Our study aimed to expose independent predictors of early (24 h) in-hospital mortality and EF in patients admitted with STEMI at the Istanbul Medical Faculty, Istanbul University, a tertiary referral university hospital in Istanbul.
Methods
Study design and patients
The Istanbul Medical Faculty, Istanbul University, medical record system and patient’s database of the Catheter Laboratory in the Department of Cardiology were retrospectively reviewed to identify patients with persistent STEMI treated with primary percutaneous intervention. This is a retrospective study that enrolled all patients (362) admitted with STEMI to Department of Cardiology, Istanbul Medical Faculty, Istanbul University, between January 2015 and December 2016.
Inclusion criteria were as follows: we focus on the patients who had STEMI with the appropriate clinical presentation, electrocardiographic (ECG) findings, and raised cardiac biomarkers as per published guidelines. 17 The diagnosis of STEMI was made in patients with a chest pain duration of at least 30 min and a 12-lead surface ECG demonstrating ST-segment elevation of >0.1 mV in ⩾2 contiguous leads.
Exclusion criteria were as follows: (1) myocardial ischemia precipitated by a condition other than atherosclerotic coronary artery disease (e.g. arrhythmia, severe anemia, hypoxia, thyrotoxicosis, cocaine use, severe valvular disease, and hypotension), (2) inflammatory diseases, and/or (3) active malignancies.
A standard 0.014 in. floppy guidewire, used for routine PCI procedures, was passed through the obstruction into a distal position of the infarct-related artery. All angiographic data were evaluated by two cardiologists who were blinded to research. All patients were treated with appropriate guideline recommendations. The pain-to-balloon time and the door-to-balloon time (time elapsed until the restoration of Thrombolysis in Myocardial Infarction (TIMI) flow 3) were recorded for each patient. Coronary diameter stenoses ⩾50% were labeled significant. Transthoracic echocardiography was performed in all patients within 24 h of admission and left ventricular ejection fraction (LVEF) was estimated using biplane method on two-dimensional (2D) images. Levels of high-sensitive troponin T, high-sensitive C-reactive protein (CRP), hemoglobin, creatinine kinase muscle/brain (CK-MB), glucose, creatinine, potassium, total cholesterol, low-density lipoprotein (LDL) cholesterol, and triglycerides were measured using blood samples obtained at admission.
All patients gave written informed consent before inclusion in the study, which complies with the Declaration of Helsinki. The study protocol was approved by the Istanbul University Local Ethics Committee, Turkey.
Statistical analysis
The clinical characteristics of patients, as well as the occurrence of in-hospital death, were collected retrospectively from medical chart review. Collected data were analyzed with IBM SPSS Statistics (version 21). Continuous variables are presented as mean ± standard deviation (SD), and categorical variables are presented as frequencies and percentages. We used Kolmogorov–Smirnov test for normality. The independent samples t-test was used to compare the means of continuous variables. Logistic regression analysis was performed to determine the predictors of in-hospital mortality and LVEF.
Results
The mean age of the study group was 57 years (range, 28–84 years), and 288 of the patients (80%) were male. Accompanying diseases were as follows: diabetes mellitus (18%), hypertension (38%), hyperlipidemia (17%), chronic kidney disease (6%), and peripheral artery disease (4%). Among our cohort, 11% had a history of cardiac arrest, ventricular fibrillation, or cardiopulmonary resuscitation history. The baseline clinical, laboratory, and angiographic characteristics are shown in Tables 1 and 2. Interobserver correlation for determining target vessel diameter measurement was assessed using intraclass correlation (ICC) test, and there was a strong correlation between the observers. In the forward stepwise logistic regression analysis, age, gender, chest pain duration, diabetes mellitus, number of diseased vessels, target vessel diameter, length of diseased segment, systolic blood pressure, fasting glucose, type of myocardial infarction, and heart rate were tested to determine the independent predictors for ejection fraction and early hospital mortality. Target vessel diameter, systolic blood pressure, and troponin T levels were independent predictors for early in-hospital mortality, while target vessel diameter, troponin T level, heart rate, and chest pain duration were the independent predictors for EF of 50% and above (Tables 3 and 4; Figures 1 and 2). There was a significant difference between mean LVEF of the patients with and without early hospital mortality (34% ± 10.9% and 49.6% ± 9.4%, p < 0.001) (Table 5).
Baseline characteristics of the study group.

CPR: cardiopulmonary resuscitation; VF: ventricular fibrillation; CAD: coronary artery disease; CABG: coronary artery bypass surgery; hsCRP: high-sensitive C-reactive protein; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; hsTroponin: high-sensitive troponin.
Categorical variables were expressed as number (%).
Data were expressed as minimum, maximum, mean, and standard deviation.
Baseline angiographic characteristics of study group.

MI: myocardial infarction; LAD: left anterior descending; Cx: circumflex artery; RCA: right coronary artery; LMCA: left main coronary artery; IM: intermediate artery; OM: obtuse marginal artery; PLA: posterolateral artery; TIMI: thrombolysis in myocardial infarction; EF: ejection fraction; CABG: coronary artery bypass surgery.
Categorical variables were expressed as number (%).
Data were expressed as minimum, maximum, mean, and standard deviation.
Forward stepwise (likelihood ratio) logistic regression analysis for independent parameters predicting in-hospital mortality.

Forward stepwise (likelihood ratio) logistic regression analysis for independent parameters predicting EF ⩾50%.

EF: ejection fraction.

(a) Comparison of troponin T levels between patients with <50% EF and with ⩾50% EF, (b) comparison of chest pain duration between patients with <50% EF and with ⩾50% EF, (c) comparison of admission heart rate between patients with <50% EF and with ⩾50% EF, and (d) comparison of target vessel diameter between patients with <50% EF and with ⩾50% EF.
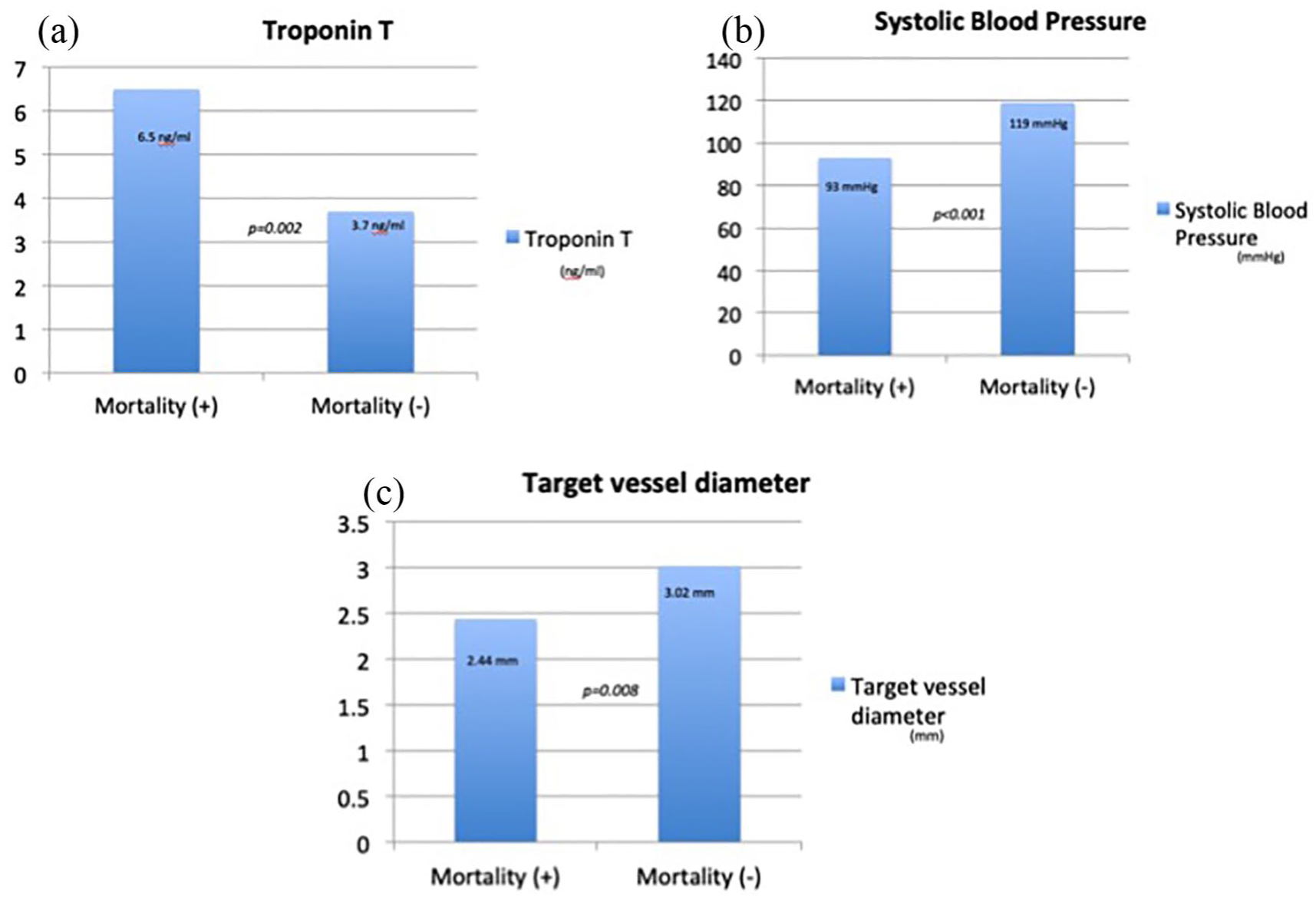
(a) Comparison of troponin T levels between patients who had early in-hospital mortality and patients that did not, (b) comparison of systolic blood pressures between patients who had early in-hospital mortality and patients that did not, and (c) comparison of target vessel diameter between patients who had early in-hospital mortality and patients that did not.
The comparison of ejection fraction average between patients with and without in-hospital mortality.

EF: ejection fraction.
Data were expressed as mean ± standard deviation.
Discussion
In this study, we report our experience with 362 patients who were diagnosed with persistent STEMI and treated with primary percutaneous intervention in our catheter laboratory of Department of Cardiology. We planned this study because little is known about the management and mortality rates of such patients in developing countries. Our study showed target vessel diameter, systolic blood pressure, and troponin T levels as independent predictors for early in-hospital mortality, while target vessel diameter, troponin T level, heart rate, and chest pain duration were identified as the independent predictors for EF of 50% and above.
Unlike other studies,10,11,18 we found that age is not an independent predictor for early in-hospital mortality. Only STEMI patients took part in our study, so the mean age of patients was 57 years. Older patients had less ST-elevation acute coronary syndrome (ACS) and Q-wave acute myocardial infarction, but had more ACS with an undetermined electrocardiographic pattern, which had a poor prognosis, as described in a prior study. 19 Therefore, age was not identified as an independent predictor in our study.
In our study, the early mortality rate (24 h) in STEMI patients was 8%, similar to STEMI patients in the national registries of the ESC countries. 5 Several recent studies have highlighted a fall in acute and long-term mortality following STEMI in parallel with greater use of reperfusion therapy, primary PCI, modern antithrombotic therapy, and secondary prevention.2–4
In a recent study in patients with ACSs, cardiac troponin levels provided useful prognostic information and permitted the early identification of patients with an increased risk of death. 12 Likewise, troponin T level was identified as an independent predictor for early in-hospital mortality in our study.
Heart failure and LVEF are important parameters for predicting early in-hospital mortality and patients’ life quality. 17 We identified LVEF as an independent predictor for early in-hospital mortality. Also, we investigated the parameters that could affect the LVEF in our study. Target vessel diameter and troponin T levels were associated with LVEF and early in-hospital mortality. Also, chest pain duration and heart rate were found to be independent parameters to predict LVEF, distinct from early in-hospital mortality. A longer duration of chest pain means a longer duration of the ischemia of the heart muscle tissue. A longer duration of ischemia means wide loss of heart muscle, ultimately leading to decreased LVEF. Also, a higher heart rate at admission was found to be an independent predictor of short- and medium-term prognosis, which is also independent of left ventricular function in a population with the ACS. 7 Our study showed a similar result for predicting left ventricular function.
Hayiroglu et al. 20 explored the effects of sex, body surface area, and target vessel size on clinical outcomes after angioplasty in their study. They found smaller target vessel size was associated with increased risk of restenosis and repeat revascularization; however, it did not appear to be a predictor for downstream mortality. This study differs in some aspects from our study as design. They included all patients who had coronary interventions done in emergency and elective situations. We got only ST-segment elevation infarction patients. In our study, target coronary vessel diameter was found to be associated with both mortality and LVEF. As the target coronary artery diameter decreases, mortality increases and LVEF decreases. In our opinion, a smaller target vessel diameter is usually associated with multi-vessel disease, diabetes, micro-vessel disease, and long diseased coronary segment. These parameters are also associated with worse outcomes in STEMI.
Our study had some limitations and strengths. This is one of the few studies to have investigated early in-hospital mortality and predictors of LVEF among patients with STEMI in a tertiary university hospital in a developing country. Considering the lack of similar data from these countries, our study fills an important gap of information in the comprehensive perception of STEMI. The important limitations of our study are its single-center nature, retrospective design, and finally, since the nature of the study, sample size cannot be calculated.
We expect that more studies will be provided in these countries to present multicenter prospective investigations that can more accurately describe the population of STEMI patients.
Conclusion
Our study is one of the limited studies in the literature to investigate the predictors of early in-hospital mortality among patients hospitalized with STEMI in a tertiary referral university hospital in a developing country. The identified predictors for in-hospital mortality (including LVEF and troponin T levels), LVEF (including troponin T level and chest pain duration), and heart rate are consistent with what has been described in large registries in the United States and Europe. Target vessel diameter is a new independent parameter that has not been reported before for predicting early in-hospital mortality and LVEF. Large-scale multicenter prospective trials are needed to identify further predictors of early in-hospital mortality and LVEF among patients hospitalized with STEMI.
Footnotes
Acknowledgements
The authors specially thank Ertugrul Cay and Ilker Varol for helping to screen angiographic data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Although this is a retrospective study, ethical approval for this study was obtained from Istanbul University Local Ethics Committee, Turkey (number: 76, dated: 13 January 2017 and 04).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All patients gave written informed consent as we mentioned in the study.