
Abstract
Background:
Breast cancer patients with post-chemotherapy had self-care deficit problems. The patient is unable to perform activities of daily living which can decrease the quality of life. One of the factors that affected self-care deficit among breast cancer patients was inadequate information. This study aimed to determine the effects of peer support psychoeducation based on experiential learning on the self-care demand.
Design and methods:
This study used a quasi-experimental design with pretest and posttest. The independent variable of the study was the application of peer support psychoeducation based on experiential learning and the dependent variable was the self-care demand. The inclusion criteria in this study were breast cancer patients with post-chemotherapy. The exclusion criteria in this study were patients who were unconscious. We selected the experimental and control group randomly. The total sample in this study was 60 people, 30 respondents for the experiment group and 30 respondents for the control group. Peer support psychoeducation based on experiential learning was developed from Wauchope’s psychoeducational theory, Orem’s self-care, and David Kolb’s experiential learning. We used a self-report questionnaire to measure self-care demand. Data were analyzed using Wilcoxon signed rank and Mann–Whitney U tests.
Results:
Peer support psychoeducation based on experiential learning has a significant effect on self-care demand, namely ADL (p = 0.002), pain management (p = 0.002), nutritional management (p = 0.000), and rest and sleep (p = 0.000).
Conclusion:
Psychoeducation based on experiential learning was recommended for nursing care or physician to increase self-care demand.
Introduction
Based on data from The Global Cancer Observatory, there were 18.1 million new cases of cancer with a mortality rate of 9.6 million. One in five men and one in six women in the world also experience cancer. 1 Meanwhile, in Indonesia, the number of breast cancer patients was 42.1 per 100,000 population with an average death rate of 17 per 100,000. 2
Breast cancer patients undergoing chemotherapy had problems especially related to self-care.3,4 The patient is unable to perform activity daily living which can decrease the quality of life and lead to anxiety and depression. 5 A previous study mentioned that in breast cancer patients, almost 50% of respondents need assistance from other people to fulfill their nutritional and fluid needs mobilization, toileting, bathing, and personal hygiene supervision. 6
Factors that affect self-care deficit among breast cancer patients were inadequate information about the disease, management of the disease, and side effects of the chemotherapy received from health care providers.7–9 Lack of information and knowledge had a negative effect among patients. 10
Psychoeducation can improve cognitive abilities 11 and is a process of providing psychological understanding and education to individuals or groups that is offered professionally by integrating psychotherapeutic and educational interventions. 12 Peer support can enhance the effect of psychoeducation intervention, by providing information and education carried out by the same group. 13 A previous study mentioned that peer support psychoeducation had a positive influence on health outcomes.13,14 Nurses or physicians can take measures to overcome the problem of independence in breast cancer patients by providing psychoeducation with peer support.
Psychoeducation is still focused on advice or suggestions in order to maintain personal health and advises patients to accept the conditions. Various interventions of psychoeducation have been developed, but most of them only cover physical and psychological aspects, while the skills aspects are still not developed.15–17
Peer support psychoeducation based on experiential learning combines health education in post-chemotherapy cancer patients by considering psychological conditions and using experiential learning methods. Experiential learning aims to improve skills so the patient will be independent in dealing with the side effects of chemotherapy. Experiential learning emphasizes a holistic learning model in the learning process, building knowledge, and skills through direct observation.18,19 There were several studies about the effectiveness of psychoeducational intervention in patients with breast cancer.20–22 This study focused on the psychoeducational element to increase knowledge about the disease as well as skills that can help patients to increase their self-care deficit. Based on this phenomenon, the aim of this study was to determine the effects of peer support psychoeducation based on experiential learning on the self-care demand of post-chemotherapy breast cancer patients.
Methods
Research design
The purpose of this study was to determine the effects of peer support psychoeducation based on experiential learning on the self-care demand among post-chemotherapy breast cancer patients. Two groups will be involved in this research, namely the experimental and the control group. A quasi-experimental design was used in this study and it was conducted with a pretest and posttest. The independent variable of the study was the application of peer support psychoeducation based on experiential learning and the dependent variable was the self-care demand among post-chemotherapy breast cancer patients.
Participants
The inclusion criteria in this study were post-chemotherapy breast cancer patients. The exclusion criteria were unconscious patients. We selected the experiment and control group randomly. The previous references recommended a minimum sample size of 10–30 respondents.23,24 The total sample in this study was 60 people, 30 respondents for the experiment group and 30 for the control group.
Intervention programs
Peer support psychoeducation based on experiential learning was developed from Wauchope’s psychoeducational theory, 25 Orem’s self-care, 26 and David Kolb’s experiential learning. 27 Peer support psychoeducation has five stages: opportunity and choice, reflection, listing options and decision-making, formal documentation, and activating and utilizing. Each stage has four steps of experiential learning, namely concrete experience, reflective observation, abstract conceptualization, and active experimentation (Table 1).
Topics of intervention.

Data collection
We selected respondents according to the inclusion criteria. The respondents were divided into two groups, the control group and the experimental group. Initially, we collected the pre-test data regarding self-care demand using a self-report questionnaire. The intervention was conducted in 5 sessions with a duration of 30–60 min each. There were one to five respondents in one group. The control group only received the intervention carried out by the hospital. At the end of the session, we collected the final data using a questionnaire.

Method of the research.
Instruments
Self-care demands have several indicators, namely: activity daily living, pain management, nutrition management, and rest and sleep.
Activity day living was measured by Lawton’s Instrument Activity Day Living (IADL). 28 The dimensions of this questionnaire were worship, doing housework, shopping, managing finances, transportation, preparing medicine, making decisions in the family, and doing leisure activities.
Pain management was measured using a modified questionnaire from Pain Management for patients with cancer. 29 It had 20 items using a Likert scale, 4: always, 3: often, 2: sometimes, and 1: never. The total score was categorized into: independent pain management >75%, need assistance 56%–75%, and dependent <56%.
A nutrition management questionnaire was asked regarding nutrition, consuming healthy foods, managing food, and fulfilling balanced nutrition. 30 It had 20 items using a Likert scale, 4: always, 3: often, 2: sometimes, and 1: never. The total score was categorized into: independent nutrition management >75%, requiring assistance 56%–75%, and dependent <56%.
Rest and sleep assessed rest and sleep. It had 20 items, using a Likert scale, 4: always, 3: often, 2: sometimes, and 1: never. The total score was categorized: independent >75%, need assistance: 56%–75%, and dependent <56%.
The questionnaires were examined using content validity and corrected item-total correlation. They fulfilled the requirements (r > 0.5). 31 They were also tested using reliability, and the results of the Cronbach’s alpha were >0.7.32,33
Data analyzed
All the data were keyed in SPSS. A descriptive analysis was used to measure the distribution and percentage of each variable. An inferential analysis was used to analyze of the effect of the intervention whether distributed normally or not. We used Wilcoxon signed rank test if the data had an abnormal distribution and paired t-test with normal distribution to measure the difference between the pre-test and the post-test in the experiment and control group. We used Mann–Whitney U test statistical test on data with abnormal distribution and an independent t-test on data with normal distribution to measure the difference in post-test scores between the experiment and control groups. Furthermore, we used statistical significance (p < 0.05).
Ethical clearance
This study was granted ethical clearance from Nursing Faculty, Universitas Airlangga, number 2135-KEPK.
Significance for public health
The factors that lead to decreased self-care among post-chemotherapy breast cancer patients were inadequate information about the disease, management of the disease, and side effects of the chemotherapy received from health care providers. Psychoeducation is a public health strategy to increase knowledge and skills among post-chemotherapy breast cancer. Knowledge, skill, and information are needed to increase self-care among breast cancer patients. This study provides the effectiveness of peer support psychoeducation based on experiential learning. It was expected to increase health outcomes as well as the quality of life
Results
Participants’ characteristic
Table 2 showed the characteristic of respondents. Most of the respondents were predominantly between 46 and 55 years old (56.67%), had senior high school degree (50%), were unemployed (56.67%), married (86.67%), with mastectomy (63.3%), and suffering from breast cancer in stadium 3 (83.3%). Most of the respondents used intravenous chemotherapy (100.0%) and had been suffering from breast cancer for about 6–12 months (56.67%). The results of the study showed no significant statistical difference between the experimental and control groups regarding the respondents’ characteristics.
Characteristic of respondents.

p < 0.05.
Table 3 showed the descriptive statistic of variables. In the treatment group, the post-test results showed that most of the respondents in the independent category increased in variable ADL pain management, nutrition management, activity and rest as well as in the control group.
Descriptive statistic of variables.

Table 4 showed the results of the Wilcoxon analysis or paired t-test for the control group on the self-care demand indicators, namely ADL (p = 0.132), pain management (p = 0.414), nutrition management (p = 0.887), and rest and sleep (p = 0.609). The results showed no significant effect of providing education given by the hospital on the self-care demand among respondents. Meanwhile, the experiment group showed ADL (p = 0.002), pain management (p = 0.001), nutrition management (p = 0.000), and rest and activity (p = 0.000). It was shown that there was a significant influence of peer support psychoeducation based on experiential learning on the self-care demand among post-chemotherapy breast cancer patients. The average results of the post-test on the indicator of self-care demand were greater than the pretest.
The results of control group on the self-care demand indicators.

Paired T Test.
Wilcoxon signed rank test.
p < 0.05.
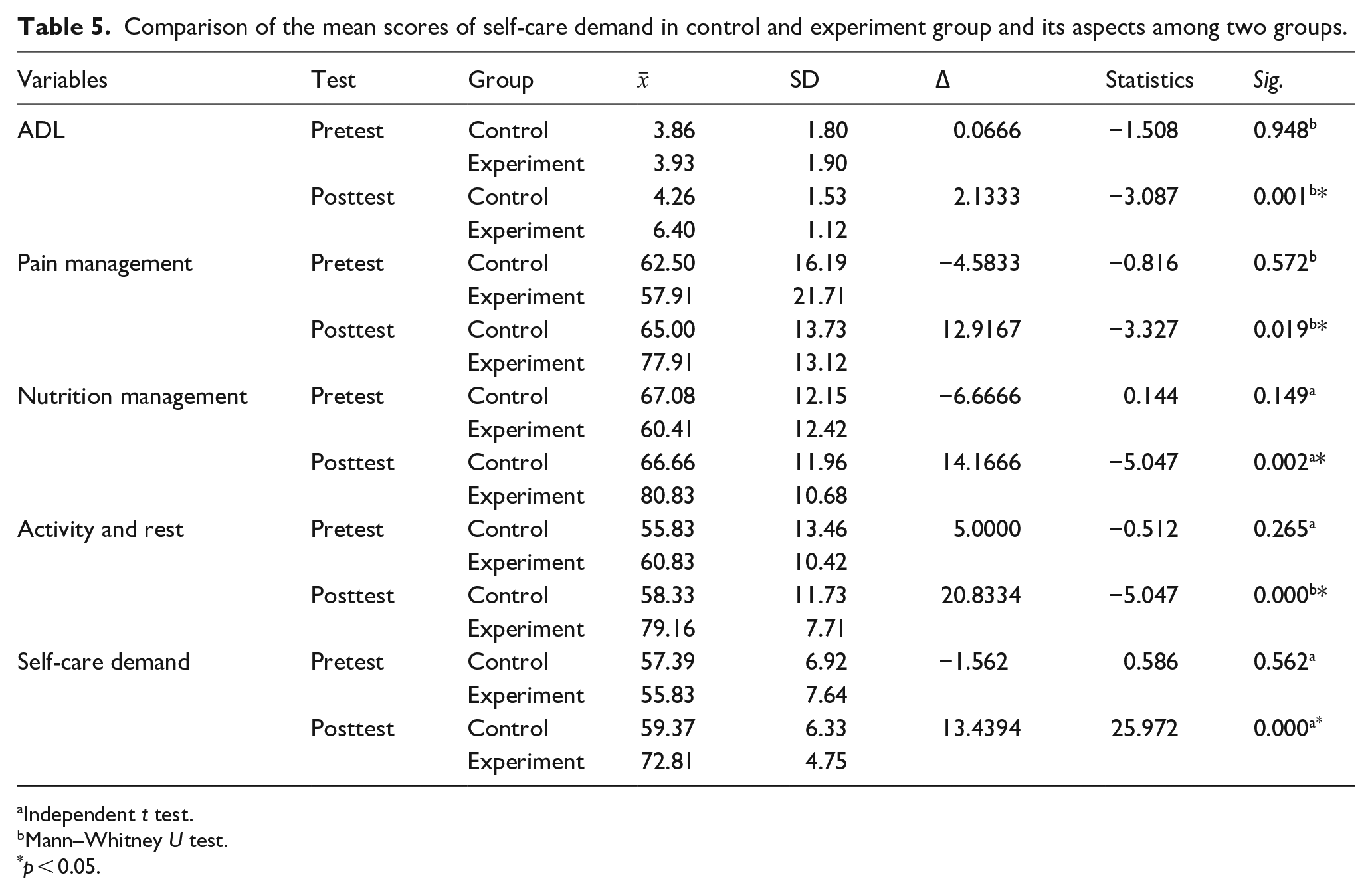
Table 5 showed that the results of the independent t-test or Mann–Whitney U test on the self-care demand had these indicators: ADL (p = 0.948), pain management (p = 0.572), nutrition management (p = 0.149), and rest and sleep (p = 0.265). It showed that there was no significant difference. Meanwhile, in the experiment group, there was a significant difference in the indicators of self-care demand: ADL (p = 0.001), pain management (p = 0.019), nutrition management (p = 0.002), and rest and sleep (p = 0.000). The average post-test score in the treatment group was greater than in the control group, indicating that self-care demand and its indicators in the treatment group were higher than in the control group. Thus, it can be concluded that peer support psychoeducation based on experiential learning was significantly more effective in increasing the self-care demand compared to hospital treatment.
Comparison of the mean scores of self-care demand in control and experiment group and its aspects among two groups.
Independent t test.
Mann–Whitney U test.
p < 0.05.
Discussion
The effect of peer support psychoeducation based on experiential learning on self-care demand: Activity daily living (ADL)
This study showed that the intervention of peer support psychoeducation based on experiential learning increases self-care demand, activity daily living for breast cancer patients with post-chemotherapy. Peer support psychoeducation based on experiential learning in this study includes sharing about activity daily living. The intervention aimed to develop skills and knowledge to fulfill ADL in everyday life post-chemotherapy. In this section, the participants were evaluated on their performance and clarified their ability as well as their perception. So, this intervention emphasizes the patient’s readiness to deal with the effects of chemotherapy. This study is in line with previous research which states that psychoeducational interventions increase ADL independence among cancer patients 34 .
The effect of peer support psychoeducation based on experiential learning on self-care demand: Pain management
This study showed the treatment group’s effectiveness in pain management. Cancer patients in developing countries often suffer from various problems, such as pain. 35 Pharmacotherapy is needed to reduce it. 36 Pain management affected health outcome and patients’ quality of life. 37 Providing health education can increase patient knowledge in terms of pain management. 38
Research on Cancer Health Empowerment for Living without Pain (Ca-HELP) exhibited that patient-centered intervention is effective in improving cancer pain management and the patient’s clinical condition. 39 Peer support psychoeducation based on experiential learning in this study includes pain assessment and explanation of several non-pharmacological interventions that can be implemented by patients at home. The most frequently used non-pharmacological therapy by respondents was warm compresses with aroma therapy and progressive relaxation therapy. Warm compresses can reduce pain because heat stimulates thermoreceptors in the skin and underlying tissue and causes vasodilation of blood vessels. Aromatherapy can activate the olfactory receptors in the nose and send chemical signals to the limbic system through the olfactory nerves which can affect the patient’s emotions, blood pressure, pulse, and breathing patterns. Relaxation techniques were reported to be effective in reducing pain. 39 The technique used in this study is relaxation technique and guided imagery.
The effect of peer support psychoeducation based on experiential learning on self-care demand: Nutrition management
This study showed that peer support psychoeducation based on experiential learning treatment had an effect on nutrition management. Chemotherapy has side effects, such as nausea and vomiting which affect the nutritional status. 40 The side effects of chemotherapy depend on the type of drug, drug dose, and the duration of the therapy.41,42 Nausea and vomit can reduce patients; quality of life. 43
Peer support psychoeducation based on experiential learning in this study includes progressive muscle relaxation techniques, guided imagery, hypnosis, and exercises. These interventions were effective in reducing the side effect of chemotherapy.44–46 Progressive muscle relaxation includes tension training and muscle relaxation. This exercise is combined with massage for 20 min during chemotherapy. Guided imagery is a technique to increase the patient’s concentration on an object related to sensory experience. The combination of these techniques and anti-emetics had a positive effect among respondents.
The effect of peer support psychoeducation based on experiential learning on self-care demand: Rest and sleep
This study showed that peer support psychoeducation based on experiential learning had an effect on rest and sleep management. Sleep disturbances often occur in patients undergoing chemotherapy.47–49 They were suffering a decrease in duration of sleep, less than 5 h, long sleep latency, and decreased sleep efficiency. In addition, they also experienced depression and fatigue.50,51
Peer support psychoeducation based on experiential learning for rest and sleep management includes the application of non-pharmacological therapies, such as music therapy, massage, cognitive behavioral therapy, and physical activity therapy. These interventions were similar to previous studies.52,53 Further study was needed to manage hospital environmental factors such as noise to increase sleep quality among patients.
Since the patients had various characteristics, further studies are needed to homogeneity the stadium of disease as well as the length of the disease. Several studies showed that psychoeducation intervention could increase the knowledge and skill among patients and this knowledge is needed to increase self-care. This study exhibited that using peer support psychoeducation based on experiential learning has an effect on self-care demand and its indicators, namely: ADL, pain management, nutrition management, and rest and sleep. This intervention was recommended for nursing care or physicians to increase self-care demand.
Conclusion
Psychoeducation based on experiential learning was recommended for nursing care or physicians to increase self-care demand; it is also a public health strategy to increase knowledge and skill among post-chemotherapy breast cancer patients. The intervention provides information, motivation, and self-care training on the topics: activity day living (ADL), pain management, nutrition management, and rest and sleep management. This intervention was recommended in clinical practice as well as for family caregivers.
Footnotes
Acknowledgements
We would like to thank all the respondents Indonesia Cancer Foundation and Shelter House, Surabaya, Indonesia. Also, the oncology nurses from William Booth Hospital, Universitas Airlangga Hospital, Vincentius A Paulo Hospital, and Indonesia Cancer Foundation and Shelter House for helping and high contribution to this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contribution
The authors contributed equally.
Ethical consideration
This study was granted ethical clearance number 2135-KEPK by Health Research Ethics Committee, Faculty of Nursing, Universitas Airlangga.
Patient consent for publication
We asked participants to fill the informed consent.