
Abstract
To verify if lethality and diffusivity of Covid-19 correlated with percentage of people vaccinated in different countries and whether results on these indicators were comparable under different types of vaccines. A linear regression analysis was conducted between vaccines/inhabitant, new cases/inhabitants and ratio deaths/cases. A comparison between the three indicators was carried out in countries subdivided by kind of vaccine. The proportion of vaccinations/inhabitants correlates negatively with proportion of deaths × 100 cases (R = −3.90, p < 0.0001), but didn’t on incidence of new cases. Countries with prevalence of mRNA vaccines were similar to others on incidence of new cases; but a lower lethality of Sars-Cov2 was found than in countries with prevalence of viral vehicle vaccines (F = 6.064, p = 0.0174) but didn’t against countries with prevalence of inactivated vaccines. The higher is the proportion of vaccine/inhabitant in a given country, the less is the fraction of infected people who die.
Introduction
Vaccines are today believed as indispensable tool to combat the pandemic. 1 Transnational studies have confirmed that some vaccines lower the case fatality ratio during the Covid-19 Spread even in presence of the new variants of the SAR-CoV2. 2 The data on the effectiveness of vaccines in reducing viral transmission are less enthusiastic. In addition, some answers have arisen about the equal effectiveness and cost effectiveness of different types of vaccines. 3 The interest in monitoring the transnational /global spread is increased since delta variant showed more contagious than previous ones; in fact, even in countries where large proportions of the population were already vaccinated, the pandemic has made new waves of infections. 4 The higher transmissibility of delta variant has also increased the estimate percentage of population needs for herd immunity to be achieved. 5 These considerations raise the interest in collecting and analyzing data about the frameworks in which different vaccines were used. Another point is that the non-homogeneous distribution of vaccines is relevant because unvaccinated fragile populations could constitute a favorable ground for developing new variants. 6 Considering that a highly determining factor in the diffusion and availability of vaccines are costs, from this perspective, any valuable data in terms of cost effectiveness on different vaccines will be precious. 7 It is therefore essential to analyze the trans-national conditions while taking into account the large extent of the variables involved that can influence the spread of the pandemic regardless of the consistency of vaccinations (e.g. weather variables) pollution, 8 distribution of the population by age, 9 different distancing policies adopted.10,11 The variability in the consistency of the official data presented by the different nations can represent another considerable limit and means that this type of analysis has a heuristic rather than a hypothesis value. 12 The aim of this work is to table whether parameters relating to the lethality and diffusivity of the pandemic may negatively/inversely correlate with the percentage of people vaccinated in different countries. We will also try to establish whether the results can be considered comparable in the countries that have achieved higher vaccination rates with the different types of vaccines, the results can be considered comparable.
Design and methods
All the countries with reported at Johns Hopkins Coronavirus Resource Center, COVID-19 Map (retrieved October 27, 2021) 13 : (1) new cases of Sar-Cov2 in the last 4 weeks before October 27, 2021; (2) ratio of deaths to infected people in the last 4 weeks before October 27, 2021; (3) number of vaccines performed and the proportion of doses delivered per inhabitant in each county as of October/27/2021, were selected. In the countries for which these three indicators were collected, the correlation and linear regression were carried out between the proportion of vaccines/inhabitant and: (1) the number of people infected in the last weeks × 1000 inhabitants was calculated; (2) the proportion of deaths/per 100 people infected in the last 4 weeks. “For each county it was ascertained the number of vaccines performed and the proportion of doses delivered per inhabitant at October 27, 2021 and the prevalent kind of vaccines in each country were established according to: (1) official data of ministries of each countries, (2) the Coronavirus (COVID-19) Vaccinations”. Our World in Data/Retrieved 27 October 2021); the red COVID-19 Vaccination 14 ; the WHO, COVID-19 vaccines—WHO | World Health Organization/WHO, COVID-19 vaccines, 15 Retrieved 28 October 2021 (only the states where the sources were in agreement were included in the comparison analysis of the parameters for the type of vaccine predominant in a country). Comparison of efficacy across different types of vaccines was conducted by comparing means and standard deviations in countries with at least one vaccine dose per population between mRNA-predominant countries and all other countries (using one-way ANOVA testing). Countries with a predominance of mRNA vaccines were compared only with those that had mainly adopted viral vehicle vaccines (through 1-way ANOVA tests) and only with those that had adopted inactivated vaccines (through Kruskal Wallis tests given the small sample size).
Results and discussion
Table 1 shows the number of cases during the 4 weeks preceding 27/10/2021 × 1000 inhabitants; the proportion of deaths each 100 cases × 100 in the same week; the number of doses of vaccine delivered in each country/inhabitants in each of the 160 countries of which these parameters were derivable from the Johns Hopkins Coronavirus Resource Center. 13 The vaccine dose per inhabitant correlates weakly with the incidence rate of new cases in the previous 4 weeks (R = 0.1643, p = 0.03788). The vaccine dose per inhabitant correlates negatively with the proportion of deaths × 100/infected in the last 4 weeks (R = −3.9034, p < 0.0001). Figure 1 shows the linear regression between vaccine dose per inhabitant and the incidence rate of new cases in the last 4 weeks. Figure 2 shows the linear regression between vaccine dose per inhabitant and proportion of deaths × 100/infected in previous 4 weeks. The countries with rate doses of vaccination for inhabitants higher than one with a higher proportion of doses of mRNA Covid vaccines were USA, Germany, France, Canada, Netherlands, Singapore, Italy, Belgium, Greece, Poland, Austria, Lithuania, Australia, Israel, Spain, South Korea, Latvia, Ireland, Czechia, Norway, Costa Rica, Slovenia, Estonia, Switzerland, Denmark, Japan, Portugal, Sweden, Finland, Saudi Arabia, Brunei, United Arab Emirates, Cyprus, Luxembourg, Qatar, New Zealand, Iceland, Taiwan, Liechtenstein, Monaco, Bhutan, Malaysia, and Fiji (N = 43). The countries with rate doses of vaccination for inhabitants higher than one, with a higher proportion of doses of Covid vaccines viral vehicle were UK, Thailand, Serbia, Hungary, Peru, Morocco, Cambodia, Equador, Mauritius, Bahrain, Antigua and Barbuda, Seychelles, Malta, San Marino, and Dominicana Republic (N = 15). The countries with rate of doses of vaccination for inhabitants higher than 1, with a higher proportion of doses of inactivated Covid vaccines were Turkey, Brazil, Mongolia, Chile, Sri Lanka, El Salvador, and China (N = 7). Table 2 showed a comparison in those three groups of countries at 27/10/2021, subdivided according to more frequent kind of Covid vaccine used (mRNA, Viral Vehicle, Inactivated Virus) about cases × 1000 inhabitants in the last 4 weeks; deaths/infected × 100 in the last 4 weeks and proportion doses Vaccine/inhabitants. The countries with more prevalent mRNA vaccine showed not difference against the other two groups regrouped concerning cases × 1000 inhabitants in the last 4 weeks but showed lower Case Fatality Ratio (F = 5.861; 1.64 df; p = 0.0182). Similarly when the comparison was conducted between countries with a prevalent mRNA vaccine and countries with a prevalent viral vehicle vaccine, no difference was found about cases × 1000 inhabitants in previous 4 weeks, but a lower Case Fatality Ratio in the mRNA countries were found (F = 6.04; 1.56 df; p = 0.0174). When the comparison was conducted between countries with a prevalent mRNA vaccine and with only countries with a prevalent inactivated vaccine, no differences were found both about cases × 1000 inhabitants in the last 4 weeks and Case Fatality Ratio. All three groups were comparable in order of proportion of doses of vaccines/inhabitants. The study shows the proportion of vaccinations for inhabitants reached in each population correlates negatively with the proportion of deaths × 100 of infected people with SARS-cov2 in the last 4 weeks before to 27/10/21 in that population. Conversely, a similar negative correlation between the proportion of doses of vaccine administered per inhabitant and the incidence of new cases in the last 4 weeks was not found. There was found an apparent paradoxical weakly tendency toward a direct correlation. In countries with a high percentage of doses of vaccine administered (>1 dose per inhabitant), the countries in which the proportion of mRNA vaccines was higher than other kinds of anti-covid vaccines were found like others, in according to the incidence of new cases in the last 4 weeks but in these countries a lower lethality of Sars-Cov2 (calculated as deaths/new cases × 100 in the last 4 weeks) was found than in countries with a higher proportion of viral vehicle vaccines. The same difference does not emerge between countries with prevalence of mRNA vaccines and countries with a prevalence of inactivated vaccines. In this case, however, the small size of the sample of nations that have adopted inactivated virus vaccines and have reached a high proportion of doses administered in the population makes the comparison with a higher risk of rejection of the alternative hypothesis even in the case that this was true (high risk of beta error). The study confirms that the percentage of population vaccinated can play a relevant role in contrasting the pandemic, and specifically, in countering the Case Fatality Rate, confirming previous works. 2 However, the efficacy of vaccines is not confirmed concerning the contrast of the transmissibility of the virus. Furthermore, about the lethality of the virus, the data seem to suggest, with all the methodological limitations that will be underlined, a probable strong impact of mRNA and Inactivated Vaccines. The results of this study must not make us forget that on the spread and lethality of the virus multiple factors other than vaccines could interact. Between these co-factors we can consider the different phases of the pandemic that countries so far away can show, due to different stage of diffusion of the delta variable, 16 or due to different climates, just think of the recognized role of the climate and how the geographic position in the southern or northern hemisphere can vary effect of this factor at the same period of the year in the temperate climates. Other sources of variability can be due to the difference in guidelines and policies adopted in each country about priorities of vaccination/protection for age groups 17 and vaccination/protection for vulnerable groups 18 ; different policies about social distancing closure of public services and use of mask. Finally, the different level of pollution precisely according to PM2-10 particles. 19 Despite this immense variability of factors that interact with vaccination, an inverse relationship clearly emerges between the fraction of vaccine doses administered with respect to the population, indicating that this correlation is really strong. However, it should be noted that it had already been previously indicated that the measure of the lethality of the virus is likely to be less influenced, than the measures relating to the identification of new cases, by the variability in the reliability of the statistics in different countries and in other contexts. In fact, if we analyze the figure relating to the spread of the pandemic with respect to the proportion of vaccination, we note that the curve is unbalanced by an addition of nations in the lower left of the figure, that is, nations that have low doses of vaccine and very few infections. If we look at the list of 160 countries evaluated, it is evident that these characteristics are present in several countries considered doubtful about the ability to produce reliable data (i.e. countries with low mean income with weak health systems often very extensive). This indicates that although the study did not detect a linear effect of the increase in vaccinations versus the decrease in cases, for the above considerations, the study results cannot rule out this type of relationship.
Number of cases during the 4 weeks preceding 27/10/2021 × 1000 inhabitants; proportion of deaths each 100 cases × 100 in the same week; the number of doses of vaccine delivered/inhabitants in each country.

Comparison in countries with more than 1.0 vaccine/inhabitants at 27/10/2021 about cases × 1000 in the last 4 weeks; deaths/infected × 100 in the last 4 weeks and proportion doses Vaccine/inhabit in three groups of countries according of the kind of vaccine.


Linear regression between vaccine dose per inhabitant and incidence rate of new cases in the last 4 weeks.
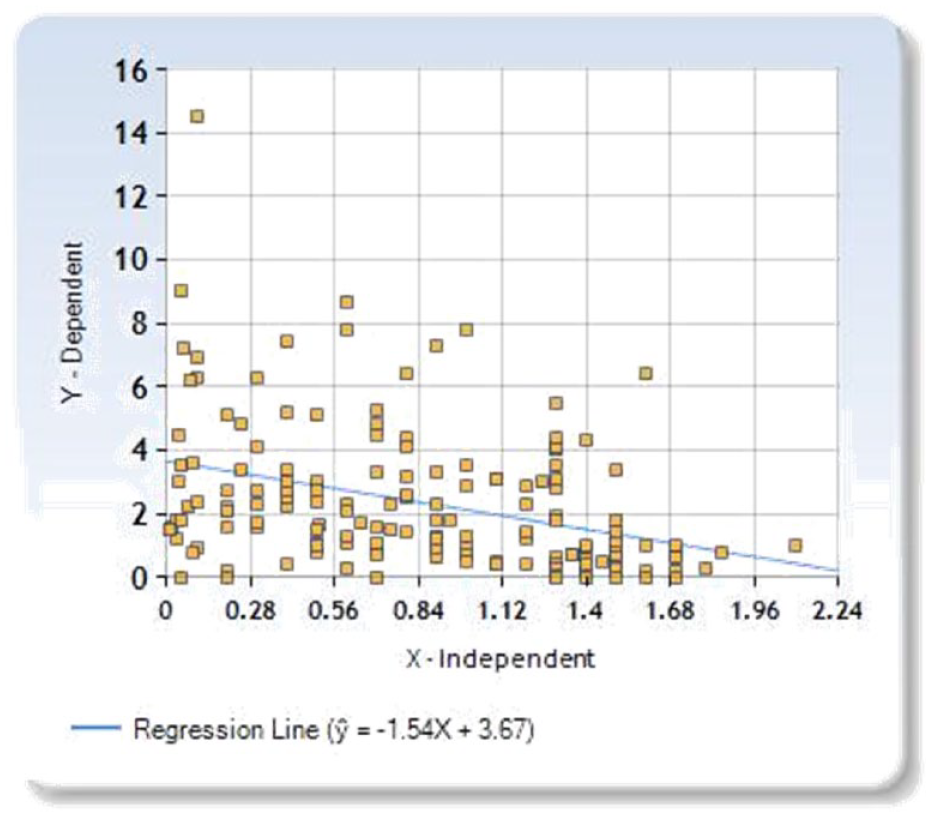
It shows the linear regression between vaccine dose per inhabitant and proportion of deaths × 100/infected in the last 4 weeks.
Limits
The biggest limit of this survey is determined by the different accuracy in the countries in collecting the data about pandemic and by the immense number of covariates influencing the pandemic interacting with the vaccines. However, these factors influence the extent of the spread of the virus more than the extent of lethality.
Conclusions
The results of the survey indicated that the higher is the proportion of vaccine per inhabitant in a given country, the less is the fraction of infected people who die. The study suggests that not all vaccines may have the same efficacy, but it must be confirmed, as well as the highlighted equality of efficacy between mRNA vaccines and vaccines with attenuated virus. This last finding is extremely important to verify because attenuated virus vaccines are less expensive and could maintain a more stable response to new variants. The fact that an inverse linear relationship between the increase in vaccines and the spread of the pandemic has not been found is a confirmation of the extreme variability of co-factors that interact with vaccination. But it requires a further analysis of these aspects through more refined methodologies. The findings indicated, however, that other protective measures to contrast the spread cannot be abandoned.
Footnotes
Contribution
Mauro Giovanni Carta and Luca Saba designed the study; Alessandra Scano, Ambra Peracchia, Giulia Cossu, Fernanda Velluzzi, Laura Atzori, Caterian Ferreli, Davide Firinu, Simona Deidda, Maria Manconi, and Roberto Littera acquired the data; Germano Orrù, Roberto Puxeddu, Luchino Chessa, Ferdinando Romano, Stefano Del Giacco, Cesar Ivan Aviles Gonzalez, Luigi Minerba, Angelo Restivo, Ferdinando Coghe, and Mauro Giovanni Carta conducted the data analysis; Luca Saba and Mauro Giovanni Carta constructed the model and drafted the manuscript. All authors agree with the content of the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The manuscript does not contain any individual person’s data in any form.
Significance for public health
To verify if lethality and diffusivity of Covid-19 correlated with percentage of people vaccinated in different countries and whether results on these indicators were comparable under different types of vaccines. A linear regression analysis was conducted between vaccines/inhabitant, new cases/inhabitants and ratio deaths/cases in 4 weeks before 10/27/2021 In countries with high percentage of vaccine administered, when possible, the prevalent kind of vaccine was established. A comparison between the three indicators was carried out in countries subdivided by kind of vaccine. The proportion of vaccinations/inhabitants correlates negatively with proportion of deaths × 100 cases, but didn’t on incidence of new cases. The higher is the proportion of vaccine/inhabitant in a given country, the less is the fraction of infected people who die. Not all vaccines may have the same efficacy, this must be confirmed.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.