
Abstract
The emergence of point-of-care (POC) diagnostics specifically designed for low-resource settings coupled with the rapid increase in need for routine care of patients with chronic diseases should prompt reconsideration of how health care can be delivered most beneficially and cost-effectively in developing countries. Bolstering support for primary care to provide rapid and appropriate integrated acute and chronic care treatment may be a possible solution. POC diagnostics can empower local and primary care providers and enable them to make better clinical decisions. This article explores the opportunity for POC diagnostics to strengthen primary care and chronic disease diagnosis and management in a low-resource setting (LRS) to deliver appropriate, consistent, and integrated care. We analyze the requirements of resource-appropriate chronic disease care, the characteristics of POC diagnostics in LRS versus the developed world, the many roles of diagnostics in the care continuum in LRS, and the process and economics of developing LRS-compatible POC diagnostics.
Keywords
Introduction
Global health is changing. In the past several years, the disease dynamic in global health has evolved, due to both the successes of many global health programs in combating infectious disease and the emergence and recognition of diabetes, heart disease, and cancer in low-resource settings as major causes of morbidity and mortality. The 2010 Global Burden of Disease study highlights these changes, noting that the number of deaths worldwide due to communicable diseases had fallen from 34.1% in 1990 to 24.9% in 2010.1–3 These data show a clear shift of the burden from communicable to noncommunicable diseases, with a change from premature death due to infectious causes to increasing numbers years lived with disability. There is a notable increase in the prevalence of noncommunicable disease, with the greatest burden now in low- and middle-income countries. Individuals living with communicable disease that have increasingly become chronic diseases, such as human immunodeficiency virus (HIV)/AIDS and tuberculosis, are also often at greater risk of developing noncommunicable diseases. This cycle of coexisting communicable and noncommunicable disease challenges the current health care infrastructure in resource-limited settings given that these health systems have evolved in response to the need for primarily acute syndromic care systems.4–6 It is in this setting that point-of-care (POC) diagnostics can play a critical role. Primary care is often the first contact point for individuals and can provide access to a broad range of care and support for preventive and critical care ( Fig. 1 ). 7
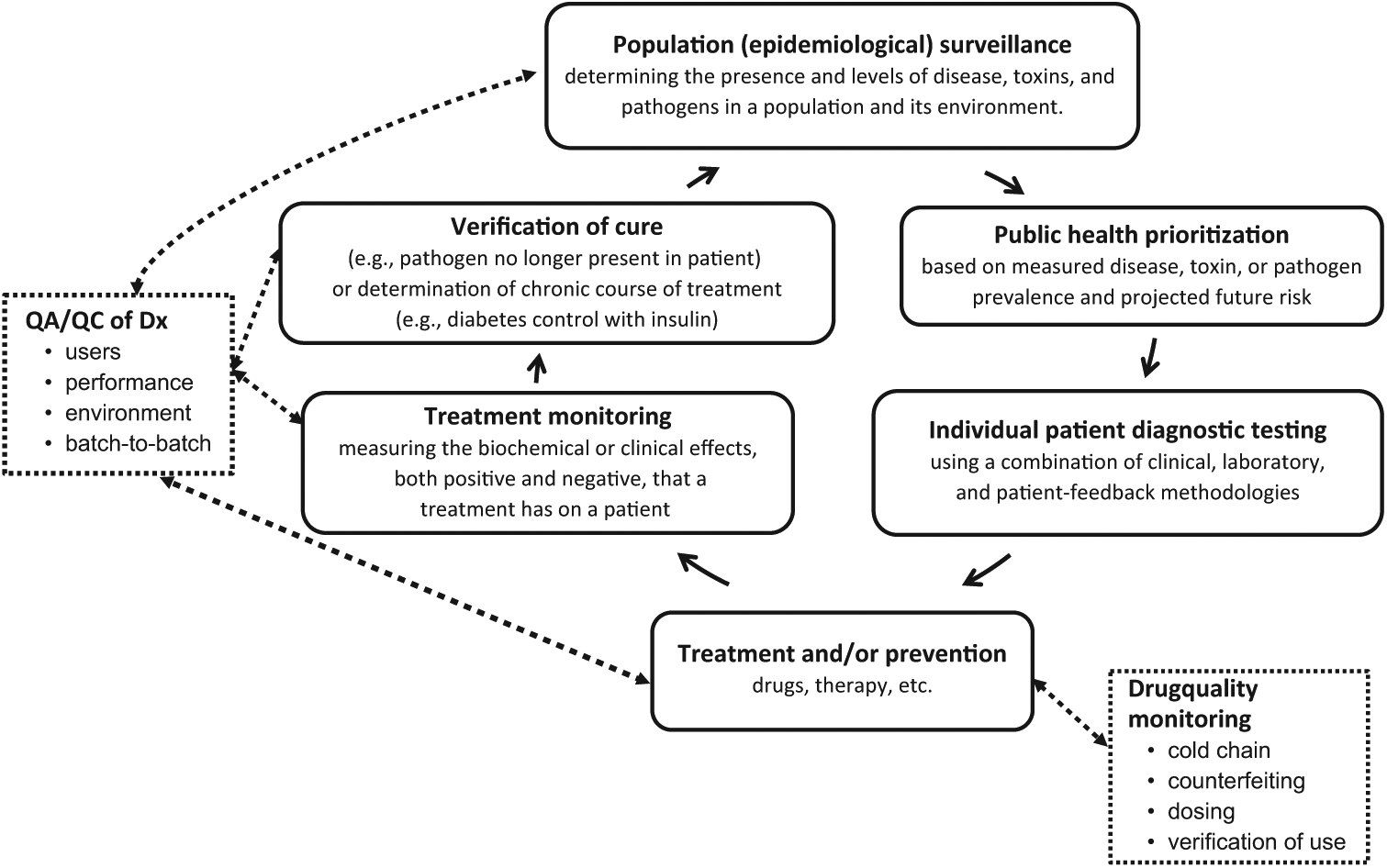
The roles of diagnostic testing in the health care continuum. QA, quality assurance; QC, quality control.
Over the past 30 years, POC diagnostics have become an accepted, if relatively minor, component of most health care systems in developed countries. For reasons ranging from existing infrastructure and entrenched interests to a primarily quality-focused industry facing ever-looming threats of lawsuits, most diagnostic testing remains the domain of the central laboratory. Notable exceptions include blood glucose testing and critical care where home testing with glucose monitors has long been established. As new technologies become available, it can be expected that the POC segment will continue to increase but at a relatively moderate pace, with a significant expansion possible once home testing for a wider range of conditions becomes safe, easy, and affordable.
In developing countries, the opportunities for POC testing and its impact on the quality and quantity of health care that can be delivered are decidedly different and greater than in developed countries. There are few examples of a functioning centralized laboratory infrastructure in the developing world, and those that do exist rarely reach beyond the major urban centers. Historically, whatever diagnostic testing in low-resource settings has been available has been performed at the POC, and although such testing is generally fairly low cost and rapid, the quality is highly variable. As a consequence, providers and health systems often are reluctant to use and introduce POC diagnostics due to concern and perception that many diseases are misdiagnosed or underdiagnosed when using POC diagnostics, leading to excess morbidity and mortality in individual patients and overtaxed health care systems. Examples for such POC tests include serological rapid tests for tuberculosis (TB), 8 for which the evidence base continues to demonstrate that the harms/risks far outweigh the benefits and rapid assays for sexually transmitted diseases (STDs) such as chlamydia, in which the benefits of easier access and lower loss to follow-up for POC tests outweigh their lower sensitivity and specificity. 9 In short, contrary to the use of diagnostics in developed countries, the existing diagnostic capacity generally does not meet the basic needs of patients and the public.
In light of these deficiencies and opportunities, developing countries and the donors that support them now face essentially two options for establishing or expanding their diagnostic infrastructure. They can develop their health care infrastructure by emulating and adapting the centralized health care delivery model augmented by limited local primary care and POC testing currently in place in developing countries, or they can choose a radically different path by focusing first on local strengthening of primary care relying on local POC diagnostics and augmenting that system with limited central reference testing and care delivery.
Research Questions and Results
This article explores the opportunity for POC diagnostics to strengthen primary care and chronic disease diagnosis and management in a low-resource setting to deliver appropriate, consistent, and integrated care.
Discussion
The Need for Chronic Disease Management: Continuity and Integrated Care
The type of health care provided in most resource-constrained settings has arisen out of need for infectious disease and maternal and child care. In these settings, mostly acute and episodic syndromic care, relying on symptomatology and, if present, simple diagnostic testing, is provided. However, in the evolving health landscape, the fundamental health systems approach will need to evolve to meet the chronic disease burden. This is in large part due to the change in the initial asymptomatic nature of many chronic noncommunicable diseases, their shared risk factors, and their chronic and incurable nature, as well as frequent comorbidities. The goal for chronic disease care is not to attain a cure but rather to prevent or delay onset of disease or symptoms, monitor disease progression, and maintain an appropriate quality of life. This requires continued monitoring, adherence, education, and care. 10
Guidance for successful management of chronic disease includes the World Health Organization (WHO) Innovative Care for Chronic Conditions model. This model includes integrated and continuous care for individuals through a platform of care that can provide immediate and follow-up diagnostic and treatment information, support for adherence and retention on medications, multidisciplinary teams, task shifting of care to appropriate health providers, and community-based care. 11 Examples of successful implementation of such care are HIV programs that have aimed to provide “diagonal” care. 12 POC diagnostics in chronic disease management allows for continuous and sustained engagement of a patient, allowing for opportunities for prevention, promoting appropriate use of medications and services, and facilitating a healthy lifestyle.
Characteristics of Diagnostic Testing in the Developing World
Depending on the degree of functionality and state command and control of the public health care system of a given country, the use of diagnostics is more or less systematic and driven by health priorities. In general, in poorer countries, there is a large gap between the need for diagnostic testing and the degree that the health care system can provide it. There are two main ways in which countries typically attempt to fill this gap in light of hyperconstrained resources: (1) substandard diagnosis relying largely on clinical presentation and low-cost, but marginally effective, diagnostic testing methods and (2) donor-funded, internationally managed, high-quality vertical screening and treatment campaigns that usually center on a single disease such as AIDS (e.g., the U.S. President’s Emergency Plan for AIDS Relief program 13 ), malaria (e.g., President’s Malaria Initiative 14 ), or tuberculosis (e.g., the Stop TB Partnership 15 ). This leaves many diseases largely undiagnosed and untreated, especially neglected tropical diseases and chronic conditions.
Diagnostics Bring an Information-Based Approach to Health Care
Diagnostic testing is generally a very cost-effective strategy to improve the quality and efficiency of a health care system. Diagnostics comprise 3% to 5% of health care spending but influence 60% to 70% of health care decisions. 16 The main roles of diagnostic testing are as follows:
To improve an individual patient’s health: diagnostics determine the cause or status of a disease by measuring the presence, absence, or level of a biochemical in a patient to guide treatment.
To inform epidemiology: diagnostics screen segments of a population to determine current health status or the presence of pathogens or toxins, generally to influence public health policy.
To perform case finding and follow-up during elimination campaigns.
To monitor and evaluate: diagnostics test a study population to determine the consequences of an intervention (e.g., monitoring populations before/after vaccination or nutrition campaigns).
As part of integrated health care projects: prevention, diagnosis, treatment, and monitoring ( Fig. 1 ).
Without reliable diagnostic testing, global health care is essentially flying blind (A. Merieux, personal communication, 2010). A common example of diagnosis based on clinical presentation (i.e., syndromic diagnosis), typically augmented by local provider knowledge, is the presumptive provision of malaria medication to patients presenting with fever in malaria-endemic areas. Even though a significant minority of the cases will not be caused by malaria but rather other infections such as dengue, typhoid fever, measles, influenza, and many others, 17 antimalarials are prescribed (or simply purchased by the patients) regardless. This happens primarily because the treatment is inexpensive and has few side effects, and no good treatment for viral causes of febrile illnesses is readily available in any case. What is usually not considered by either patients or physicians are the public health consequences of overprescriptions of antimalarials or antibiotics that can lead to drug resistance.
Some diagnostic methods and tests have recently become more widely available. Vertical programs were initiated by various donors precisely because in-country programs were unable to deal with the severe health crises caused by diseases such as AIDS, tuberculosis, and malaria. However, this has led to several major problems. The programs are costly and largely unsustainable without external donor funding, and they tend to view the diseases in an insular way. In many cases, the vertical programs have established a parallel health care, screening, and diagnostic infrastructure that deals only with particular syndromes. This streamlines the process for the providers and may improve availability, quality, and accountability, but it has made life more difficult for the patients and has pushed other diseases further underground.
How POC Diagnostics Can Be Transformative in Chronic Disease Management
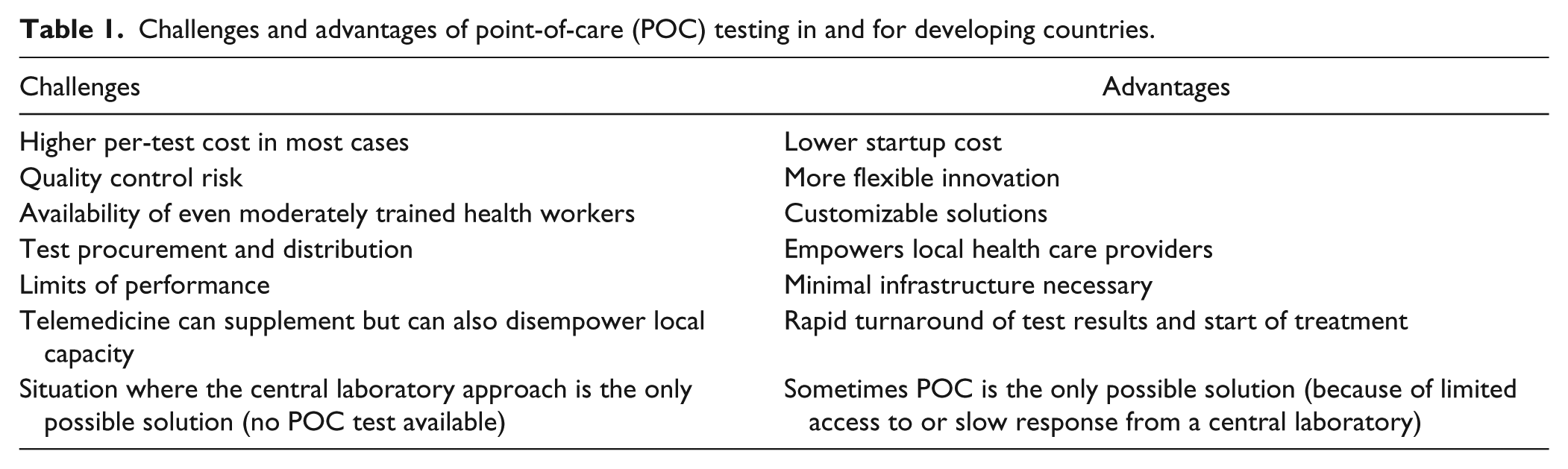
With a goal of establishing a focus on sustainable, systematic, rational, and long-term improvements of the overall health care systems in low-resource settings, integrated diagnostic capabilities that systematically address the most critical diseases and conditions should be established and prioritized by importance to individual and public health and cost-effectiveness of the interventions. The current crop of improved POC diagnostics products compatible with low-resource settings (e.g., POC nucleic acid amplification test assays 18 and higher quality lateral flow strip tests 19 ) may be the catalytic event that will cause the creation of a long-term sustainable, modest, but effective health care system for all in developing countries through improved primary care. A list of challenges and advantages with POC tests is shown in Table 1 .
Challenges and advantages of point-of-care (POC) testing in and for developing countries.
For POC diagnostics, there is thus a transformational opportunity in developing countries: the development of a POC diagnostic tool kit for primary care. This tool kit would
be low-cost, simple, sustainable, preferably produced in a low-resource setting, and provide reliable, locally actionable diagnostic results;
contain tests for all critical, locally important infectious and noncommunicable diseases, including chronic conditions; and
be synergistic regarding instruments used, reagents required, and training needed.
The “Primary Care Diagnostic Tool Box”: Broadening the Scope of POC Diagnostics in Low-Resource Settings to Include Both Chronic and Communicable Diseases
In 2010, WHO developed a package of essential noncommunicable (PEN) disease interventions for primary health care in low-resource settings. 20 The list of interventions, designed to be a prioritized set of cost-effective interventions that can be delivered to an acceptable quality of care, even in resource-poor settings, focuses primarily on chronic diseases. According to the report, it should not be considered as yet another package of basic services but rather an important first step for integration of noncommunicable diseases into primary health care and for reforms that need to cut across the established boundaries of the building blocks of national health systems. WHO’s PEN is meant to be the minimum standard for noncommunicable diseases to strengthen national capacity to integrate and scale up care of heart disease, stroke, cardiovascular risk, diabetes, cancer, asthma, and chronic obstructive pulmonary disease in primary health care in low-resource settings.
The WHO PEN includes prevention programs such as smoking cessation, drugs such as blood thinners and statins, and a list of devices ( Table 2 ).
Essential technologies and tools for implementing essential noncommunicable disease interventions in primary care.
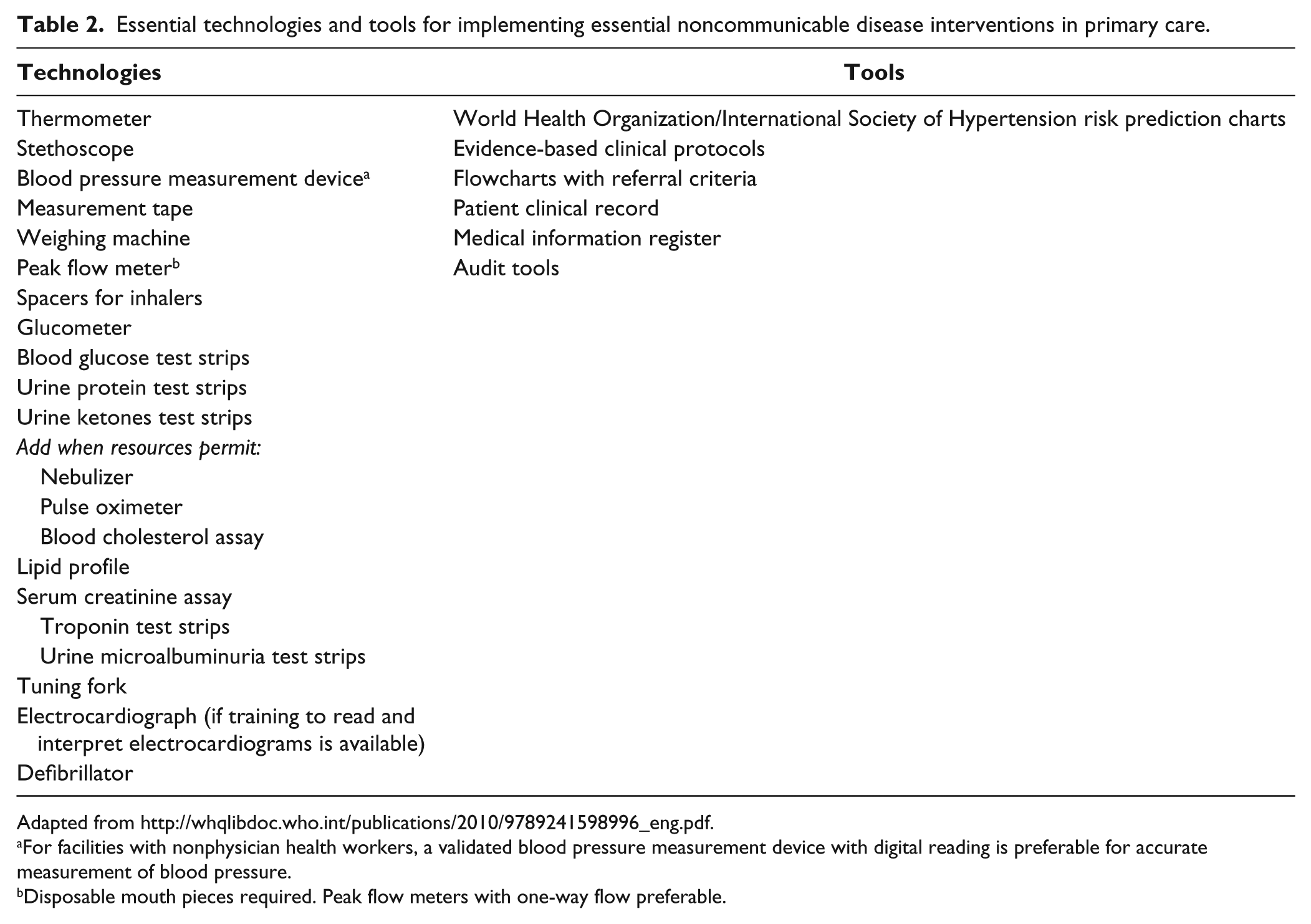
For facilities with nonphysician health workers, a validated blood pressure measurement device with digital reading is preferable for accurate measurement of blood pressure.
Disposable mouth pieces required. Peak flow meters with one-way flow preferable.
Table 2 does list a number of POC assay technologies. However, it is clear that this list of interventions is aspirational rather than descriptive. Most primary health care settings in low-resource settings do not currently have routine access to diabetes assays, for example.
Despite the WHO PEN report, developing-country health care for the general public is still synonymous with fighting infectious diseases. Donor funding priorities largely reflect this view. While chronic diseases now comprise more than 60% of morbidity and mortality in low-resource settings, they receive only 2% of the total research and development funding. 21 This is partially based on the long history of havoc that infectious diseases have inflicted on developing countries and the more recent emergence of urbanization, globalization, lifestyle and environmental changes, and an aging population.22,23 However, communicable diseases may also be more at the forefront because they appear more threatening to the developed world by their potential to cause pandemics and economic and political instabilities worldwide, including in the developed world. However, there is growing awareness that chronic diseases such as diabetes and associated syndromes need to be tackled lest they impede the growth of the emerging economies in low- and middle-income countries.
There are many more existing commercial diagnostic tests for chronic diseases already in use in developed countries than tests for infectious diseases simply because chronic diseases contribute disproportionally to morbidity and mortality in developed countries. While most of these tests were designed for high-throughput central laboratory use, versions of many are designed for smaller laboratories or even POC use. They can, with moderate expense and effort, be converted to low-cost products suitable for low-resource settings. A basic suite of chronic disease diagnostics, as outlined in the WHO PEN report, could form a relatively inexpensive core to which the basic infectious disease diagnostics could then be added, which would need to be adapted from country to country based on local epidemiology. However, most kits would include tests for sexually transmitted infections, HIV, strep, and hepatitis, supplemented with malaria and neglected tropical disease rapid diagnostic tests where these diseases are endemic. Furthermore, in high-endemicity HIV areas, CD4 assays and likely POC tuberculosis assays could eventually be added to settings that have the necessary patient throughput.
Breaking the Disease Silos Will Enable POC Diagnostics Developers to Create Better Products
Beyond the issues already identified with vertical programs above, another one is particularly relevant to POC assay developers—many new diagnostic technologies are platform technologies. That is, the same device, disposable, or technique can be used, with minimal adaptations, for a variety of different diagnostic assays. This would allow, in principle, installation in settings that do not have the necessary patient load for any single disease to justify their use, but the patient load would be sufficient if the same platform is used for multiple diagnostic assays. Primary care settings have a high but diverse patient load that would benefit from a platform diagnostic with multiple assay capability.
Even for diagnostics that do not require an instrument, such as rapid diagnostic strip tests, synergies can be found when the same platform is used. Standardization of sample input, operation, and signal output, such as is typical for rapid diagnostic tests, simplifies training, reduces the potential for errors, and allows systematic archiving and sharing of results and data.
Vertical programs usually only have use for a single analyte test or a small suite of related diagnostic tests. That is what they procure, reimburse, manage, train, review, sometimes approve, and simply know and care about. To cater to vertical programs, POC diagnostics manufacturers have to deal with each vertical program separately, even though their products would work for multiple analytes. This adds excessive costs to product development.
A “horizontal” program that integrates care across the disease spectrum on the health care setting rather than a specific disease could be transformational to how care is provided in low-resource settings. There are some attempts to tackle platform technologies for low-resource settings through research and development funding (such as the Bill & Melinda Gates Foundation’s Grand Challenges Diagnostics program 24 or several requests for applications issued by the U.S. National Institutes of Health and the Indian Department of Biotechnology 25 ). The U.S. Agency for International Development now does fund integrated health care projects but does not significantly fund new tools such as diagnostics. What is needed to really attract a broad-based investment in platform diagnostics is a care setting–based funding program that focuses on demonstration and scale-up of integrated health care and interventions at the primary care level.
How POC Diagnostics Can Strengthen Primary Care in Developing Countries
POC diagnostics may strengthen primary care by providing key and potentially comprehensive diagnostic information that can facilitate appropriate care. Primary care providers include all front-line providers, including community health workers, nurses, physicians, and other allied professionals that engage with individuals. Given that primary care has been recognized as an efficient and cost-effective way to design a health system and provide care with better outcomes and satisfaction, with the appropriate tools, skills, and knowledge, primary care providers have the potential of providing effective care. 26
In many countries, primary care outreach is done by first-line providers such as community health care workers (CHWs). CHWs, sometimes called “village health workers,” are selected by their community members to provide basic health and medical care locally ( Figure 2 ). CHWs are given a limited amount of training to provide essential, safe, and highly effective primary health care services to the population. Programs involving CHWs (e.g., in China, Brazil, and Iran 27 ) have demonstrated that using such workers can help improve health outcomes for large populations in underserved regions. “Task shifting” of primary care functions from professional health workers to CHWs is considered a means to improving the health of millions at a reasonable cost. In general, it has been shown that CHWs are most effective if they receive some form of payment. Volunteerism cannot usually be sustained for long periods, and, as a rule, CHWs are poor and thus expect and require an income. 28
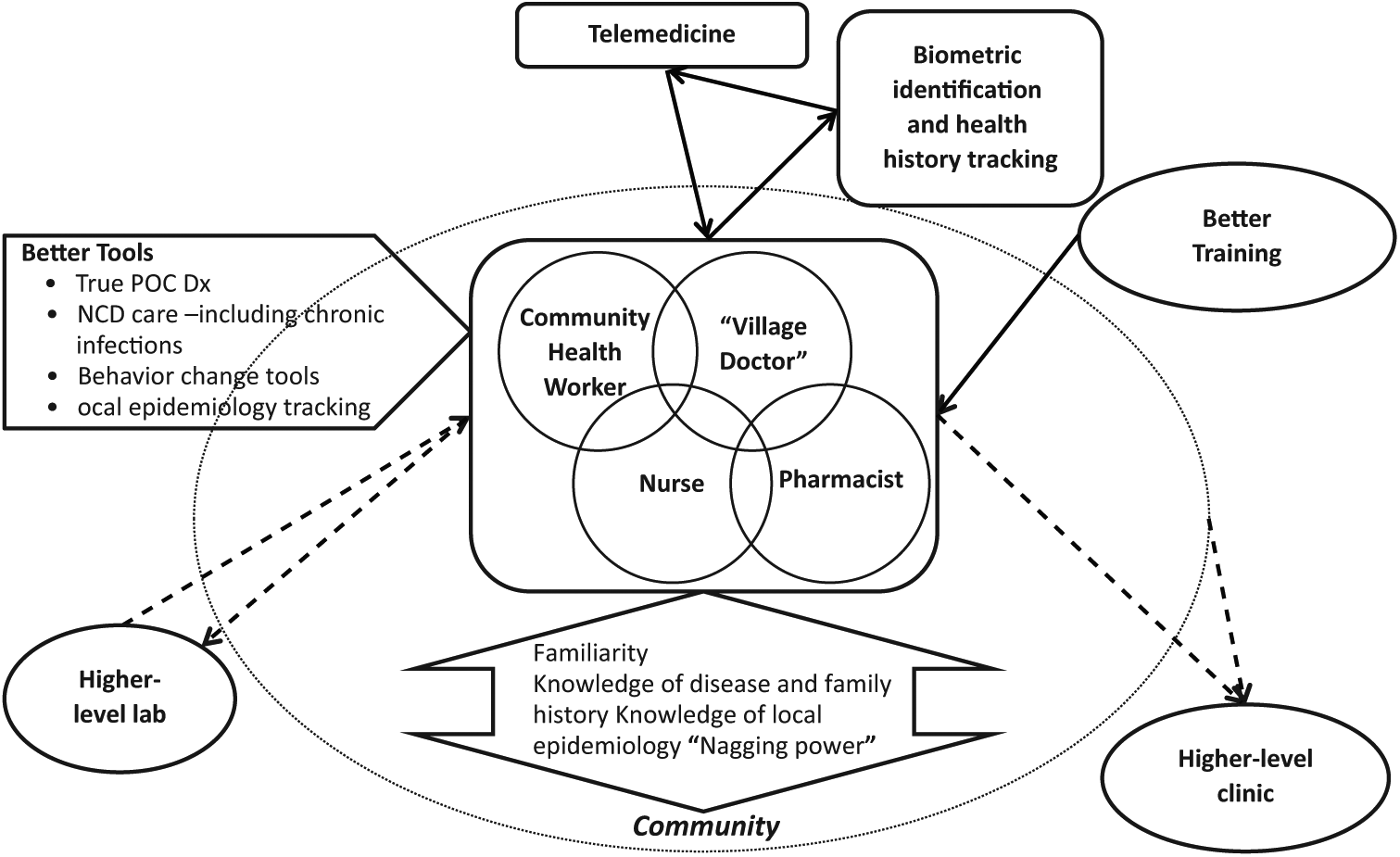
The elements of “empowered” primary health care: increasing the impact of marginally trained community health care providers with better tools (including point-of-care [POC] diagnostics) and training. Dx, diagnosis; NCD, noncommunicable diseases.
CHW programs have been successfully providing medical services to underserved populations, even though their impact has been hampered by lack of training and equipment. One of the main advantages of a strong CHW system is that they can build on an essentially “free” asset—CHWs’ intimate knowledge of the community, individuals’ health histories, and local epidemiology. In addition, their continuous presence allows them to interact with the community and reinforce health behaviors. As chronic diseases become more prevalent, this will be ever more important. CHW care is usually limited to giving health advice (especially in the area of maternal and child and reproductive health), performing simple procedures, and, in some cases, handing out drugs. However, if the WHO PEN disease interventions for primary health care in low-resource settings (see Table 2 ) were accessible to CHWs, together with better training, telemedicine support, and additional tools to tackle some infectious disease diagnostics and care, CHWs could have a much bigger impact.
Beyond access to care issues, CHW-based care offers another distinctive advantage: clinics in developing countries have an especially high risk of nosocomial infections. 29 Many are crowded, understaffed, and lined with patients with multiple and severe infections. By their nature, CHWs provide care in settings with a lower patient throughput with typically lower disease severity, and any transmission will have mostly local consequences.
Business Models and Funding to Enable POC Diagnostics and Support for Local Primary Health Care
For primary care to be empowered through better tools, including POC diagnostics and better training, business models will be needed to facilitate its provision. A primary research question will be the cost-effectiveness of strengthened primary health care. There are essentially two main funding approaches to primary health care, with many hybrid versions coexisting in most countries. For primarily government-controlled primary care models, extra costs incurred through primary care strengthening would have to be borne though public health care expenditures and ideally offset through cost savings in other secondary and tertiary care settings (because fewer patients would need to access secondary care).
An alternative model is microcredit-financed primary health care,30,31 which has been the topic of several demonstration projects. These include the HealthStore Foundation’s child and family wellness (CFW) model, a network of micropharmacies and clinics whose mission is to provide access to essential medicines to marginalized populations in the developing world; CFW Shops, 32 a clinic and pharmacy franchise in East Africa; MicroClinic International, 33 a primary clinic franchise operating in Ghana; E-Health Point, 34 a chain of primary health clinics using telemedicine to connect patients to doctors in rural areas; and Saude 10, 35 a low-cost chain of primary health clinics in Brazil that started up in 2010. Beyond the out-of-pocket payment model that the franchises listed above use, there are also models that combine existing health care centers with microinsurance. 36
While the business models listed above will provide some market opportunities for diagnostics developers in the coming years, they are unlikely to incentivize the development and introduction of all diagnostics that will eventually be needed to strengthen capacity in primary care settings. New funding and purchase guarantee schemes may yet emerge that make the development of primary care diagnostics more attractive for developers.
Research and development grant funding is available for a variety of programs focusing on POC diagnostics for low-resource settings such as the Gates Foundation’s Grand Challenges Diagnostics program 37 and the Grand Challenges Canada program, the program issued by the National Institute of Biomedical Imaging and Bioengineering (NIBIB) on “Development and Translation of Medical Technologies That Reduce Health Disparities,” 38 or the PATH Center for POC Diagnostics for Global Health (GHDx Center), 39 also funded by the NIBIB (note that the original funding for the GHDx Center has ended as of June 2013, but the essential functions of the GHDx Center have been incorporated into the PATH Diagnostics group and are ongoing). Grant funding does reduce developing costs for diagnostics developers and can incentivize them to focus their efforts and dollars on diagnostics for low-resource settings rather than other opportunities in the diagnostics field. For example, the GHDx Center currently works with 17 different organizations that develop diagnostics, both for profit and nonprofit, to help them create versions of their assays for low-resource settings. 40 The GHDx Center has been focusing on four core activities:
Clinical needs assessments: Understanding the opportunities and barriers to deployment of effective, appropriate POC diagnostic technologies in low-resource settings is a critical step in informing the selection of technologies for consideration as exploratory projects or for clinical evaluation. The GHDx Center draws on PATH’s considerable institutional knowledge and conducts in-depth clinical needs analyses to help target the most pressing global health challenges and increase the likelihood of success. These clinical needs analyses help technology developers navigate potential pitfalls that can derail successful commercialization and uptake of POC diagnostic technologies. As an example, the GHDx Center has studied the need and opportunity for multiplexed febrile illness diagnostics. 41
Supporting exploratory technology projects: The GHDx Center provides financial and technical support to developers of promising technologies to tackle solutions to these identified needs. Through competitive solicitation processes, the GHDx Center identifies, selects, and supports innovative and promising technologies that could have a significant positive impact on public health outcomes. Candidate technologies are assessed for anticipated health impact, relevance to the needs and realities of low-resource settings, and market-related issues that could affect the eventual products’ commercialization prospects. Examples of current supported technologies include sample preparation, nucleic acid amplification, and detection components that will be needed to develop POC molecular tests.
Clinical testing of prototype POC diagnostics: The GHDx Center has adopted a very cost-effective three-step evaluation process (due diligence, laboratory, and field) of prototype diagnostic devices targeted for low-resource settings. The evaluation takes place in close collaboration with the assay developers and is designed to assist them in identifying design and performance flaws very early. Uniquely, the results of early evaluations are usually not published. This allows for a greater openness between developers and evaluators about problems and potential solutions.
Training on the clinical realities of designing POC products for low-resource settings: This unit of the GHDx Center offers a four-tier progressive training program to engage individuals with varied experience and backgrounds from the fields of assay and device development, clinical laboratories, and disease specialties. The GHDx Center courses create a networked group of POC test developers and POC test users for training in state-of-the-art technology and challenges for global health in low-resource settings. Networking and collaboration among individuals with this unique skill set has already resulted in the development new diagnostics for low-resource settings.
In addition to (and beyond) research and development funding, other mechanisms also exist that can, but not always do, incentivize development and introduction of POC-compatible diagnostics for low-resource settings. These include the following:
Diagnostic technology “trickle down” from central to primary care: Primary care markets, while large, also present some of the greatest problems for diagnostics developers.
Diagnostic technology “trickle down” from developed to developing countries: Some diagnostics, such as POC hemoglobin 42 and glucose 43 meters, first developed for developed-country POC settings, are being used fairly widely now in low-resource settings.
Diagnostic technology “trickle down” from biodefense products: Starting in the mid-1990s, much effort has been put into developing bioterrorism pathogen detection devices for environmental and diagnostic samples. 44
Diagnostic technology development and manufacturing in developing and emerging countries: One of the most promising developments in the landscape of diagnostics for low-resource settings is the rapidly increasing capability of current and former developing countries to engage in very cost-effective development and manufacturing of POC diagnostics specifically for the markets in which they are situated. For example, PATH has a long track record of transferring rapid diagnostic strip test technologies to manufacturers in Southeast Asia. 45 The GHDx Center is also working with parastatal organizations such as the Kenya Medical Research Institute in Kenya and Fiocruz in Brazil to transfer and manufacture both immunoassays and molecular assays and assay components. Locally produced diagnostics frequently have an advantage in market acceptance and in access to regulatory bodies.
In conclusion, there are many pieces to the puzzle of improving access to needed diagnostic tests and primary care services for patients with chronic diseases in developing countries. New technologies and approaches promise to transform primary health care. Existing research and development funding and other sources of innovation help create building blocks for new primary care systems for low-resource settings such as better POC diagnostics, improved supply chains for heat-sensitive drugs and reagents, task shifting to lower levels of the health care system, and improved mobile phone–based training and adherence tools. A significant challenge will be scale-up and integration of these new tools into existing primary care delivery platforms that will require large-scale donor commitments focused on improving primary and NCD care in low-resource settings at a similar scale as existing vertical disease programs for TB, HIV, and malaria.
Footnotes
Acknowledgements
We thank Dr. Kenneth Hawkins of PATH for valuable insights and manuscript editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was provided by the National Institute of Biomedical Imaging and Bioengineering under the Point-of-Care Technologies Research Network, grant number 1U54EB007949, and the institutional National Service Research Award to the Department of Family Medicine at University of Washington. At the time of this work, Dr. Neogi was supported by a NRSA Ruth L. Kirchstein T32 Primary Care Research Fellowship at the University of Washington.