
Abstract
We assessed the efficiency of point-of-care (POC) tests in the emergency department (ED) by comparing them with the international standard. We recorded the turnaround times (TATs) for processing laboratory biomarkers to assess laboratory efficiency from 17 EDs in national/regional hospitals. We also compared patient components between national and regional hospitals. Although the 17 enrolled hospitals expanded their EDs, they contained only five POC machines among them. The P50 (P25, P75) of the TATs for POC tests was 47 min (39, 55.5 min) for cardiac troponin T, which was much longer than the international standard (30 min). The TATs of other cardiac biomarkers were also longer than 30 min. The low efficiency of TATs for POC tests was a common feature in both regional and national hospitals (p > 0.05). Myocardial infarction was diagnosed in 61% of investigated ED patients who visited national hospitals, which is more frequently than those diagnosed at regional hospitals (46%, p < 0.05). Chronic heart failure was less frequent at national hospitals (28%) than at regional hospitals (41%, p < 0.05). The patient distribution in this study indicates that patients have the tendency to choose hospitals when they are affected with chest pain. However, the POC panel is rarely used in the ED, which delayed the TAT level and affected laboratory efficiency. This finding indicates a severe problem in the administrative management of EDs. This issue should be addressed in the next version of the medical reform policy.
Keywords
Introduction
The health care system in China is largely influenced by financial support and economic prosperity. Chinese economic development offers a high-quality and wide breadth of coverage that is not found in any other country. However, the Chinese health care system has not improved at the same pace as the economy. Because of rapid urbanization and the aging population, the Chinese health care system faces the challenge of increased urban populations and overcrowding during patient visits,1 –3 which is also a worldwide problem. Therefore, a call for Chinese health care reform was inevitable, and the Chinese government launched a reform plan in 2009, which included spending approximately US$125 billion to fund a public health provision. 4 With this funding for primary public health care, equipment at medical facilities, infrastructure development, and training sessions have been innovated. The Chinese medical environment is expected to gradually improve 5 and reach the international level. Unfortunately, no solid data- or multicenter evidence-based research has been reported on the quality or clinical effectiveness of public health services since the reform was implemented, 1 and this is due to the lack of a database on clinical efficiency pre-reform.
Based on the lack of such a database, we designed a questionnaire to investigate the medical situation of emergency departments (EDs). Newly expanded and newly equipped EDs with independent laboratories at 17 public hospitals in Shanghai were included in the study. We described the emergency mode and assessed the laboratory efficiency. We hypothesized that some routine values of laboratory efficiency matching the international standard would indicate that the reform is successful in approaching the international level. We recorded the infrastructure construction of the 17 EDs and analyzed the turnaround times (TATs) of cardiac biomarker measurements from patients who were suffering from chest pain, which are routinely used to exclude acute myocardial infarction (AMI) and acute coronary syndrome (ACS). 6 ACS, one of the most common clinical and serious cardiovascular diseases, is a main cause of death in most countries. In addition, AMI is the first reason for death in China, with the increase in its incidence and mortality. By assessing the laboratory efficiency of cardiac biomarker measurements in the ED, we expected to learn the situation of emergency medical care from this observation and descriptive study and to get a global impression of the present health care reform for future improvement.
Materials and Methods
Setting and Study Design
The study was designed to evaluate the medical environment of ongoing health care reform. The medical infrastructure building and training sessions are close to completion. Based on the principle of “large samples and multiple center study,” we selected all tier III hospitals in 10 districts of Shanghai and 1 representative tier II hospital in the district. In total, there were 7 tier III hospitals and 10 tier II hospitals in the group. The 17 EDs that were recruited for our study have been functioning in the newly expanded infrastructure for more than 1 year in Shanghai, which is the largest city in China with more than 24 million residents.
All of the enrolled hospitals constructed laboratories in their EDs, which were defined as sectional laboratories for ED routine tests. Emergency physicians recruited chest pain patients for the study when cardiac biomarkers were required for a diagnosis. A short training session was presented to the enrolled emergency physicians and laboratory personnel after the study was initiated in January 2011. The study lasted 8 months, spanning from April 2011 to December 2011.
Selection of Participants and Data Collection and Processing
The TAT was defined as the time point when the cardiac biomarker tests were ordered until the time point when the ED physicians were available to analyze the test results. On a questionnaire, the emergency physicians recorded the time at which they received the laboratory reports from the computer-based system of the hospital. Then they completed the rest of questionnaire according the electronic medical records of each patient after they had finished the task at hand. The cardiac biomarkers tested included serum cardiac troponin T (c-TNT), creatine kinase MB (CK-MB) and myoglobin. In addition, supplementary tests, such as N-terminal pro-brain natriuretic peptide (Nt-proBNP) and D-dimer, were recorded. All of the laboratories we selected used the same machine (immunoassay system from Beckman, Brea, CA, and Sysmex Corporation, Kobe Japan) and kits (Cat. No. 331869, 560166, and 28165215) to detect the cardiac marker in the study. Different methods increase the possibility of the variation of this study, but the expected TAT value suggested by the international guideline should be less than 30 seconds independent of methods and kits. By completing detailed questionnaires, the emergency physicians provided the following information regarding the tests: (1) the TAT values of cardiac biomarkers that were obtained in the ED using conventional or point-of-care (POC) instruments and (2) the types of instruments that were used to obtain the biomarker values.
Primary Data Analysis
The study was designed as a retrospective and multicenter analysis. The 17 enrolled hospitals included 7 regional hospitals (tier II) and 10 national hospitals (tier III). This observational investigation was aimed at detecting improvements in health care after the reconstruction of basic infrastructure, which was initiated by the health care reform policy. This study focused on fast clinical decisions regarding acute chest pain in patients with a high risk of AMI or ACS.
We evaluated the frequencies of these conditions and the TATs of the laboratories. We used the Wilcoxon rank-sum test and Kruskal-Wallis tests to assess the differences between tier II and tier III hospitals and between central and ED laboratories if the results of the study failed to satisfy normal distributions (SAS procedures PROC UNIVARIATE and PROC NPAR1WAY). We considered a 2-sided p value of 0.05 or less statistically significant. From the aggregate data, we determined the TATs for the c-TNT, CK-MB, myoglobin, Nt-proBNP, and D-dimer tests. All of the discrete data, including the TATs for cardiac biomarkers, including c-TNT, CK-MB, myoglobin, Nt-proBNP, and D-dimer, are presented as the median (quartiles). The categorical data, the number of AMI patients, and the number of patients with a high or low level of Nt-proBNP are presented as the total counts and percentages. All of the analyses were conducted using SAS software version 8.2 (SAS Institute Inc., Cary, NC).
Role of the Funding Source
The sponsor of this study had no role in the study design, data collection, data analysis, data interpretation, or the writing of the report. The corresponding author had full access to all of the data in the study and made the final decision to submit the manuscript for publication. All the funding sources were used for the data collection, the statistical analysis, and service fees.
Results
Description of the Reconstruction of ED Equipment due to Health Care Reform
In China, tier I hospitals are designed to supply primary health services without emergency health care. Tier II hospitals are designed as regional public hospitals with medical facilities for patients from nearby districts. Their EDs are equipped with 24 h intensive care units and a fast path for resuscitation. Tier III hospitals are typically teaching hospitals with state-of-the-art medical equipment and nationally or internationally known specialists. The level of medical care at tier III hospitals is aimed at meeting national requirements.
Before initiating the study, we demonstrated the ED equipment of Shanghai hospitals. According to the Chinese health care system reform, the EDs enhanced the primary health care facilities by improving the equipment in resuscitation rooms, enlarging the fast passage areas, and providing more rapid service from the fast passage area to the resuscitation room. Every ED we interviewed shared a similar structure and similar working models (see Fig. 1 ), including a triage area, a general medical ED with one to six clinics (depends on the scale of hospitals, one to two in tier II and two to six in tier III), a surgical ED with one to four clinics, a resuscitation hall that has its own entrance and 2 to 16 monitored beds for acute critical care support (2–4 monitored beds in tier II and with 4–20 monitored beds in tier III), one intensive care unit with 4 to 18 beds, one intravenous therapy room with at least 20 to 120 seats without limitation, one observation unit that can be extended to 20 to 78 beds and function as a temporary transitional inpatient ward for those who cannot be admitted to the in-hospital ward immediately because of the scarcity of bed resources, and a pharmacy that provides the medications necessary for the ED department and all the other departments in the hospital after daily working hours.
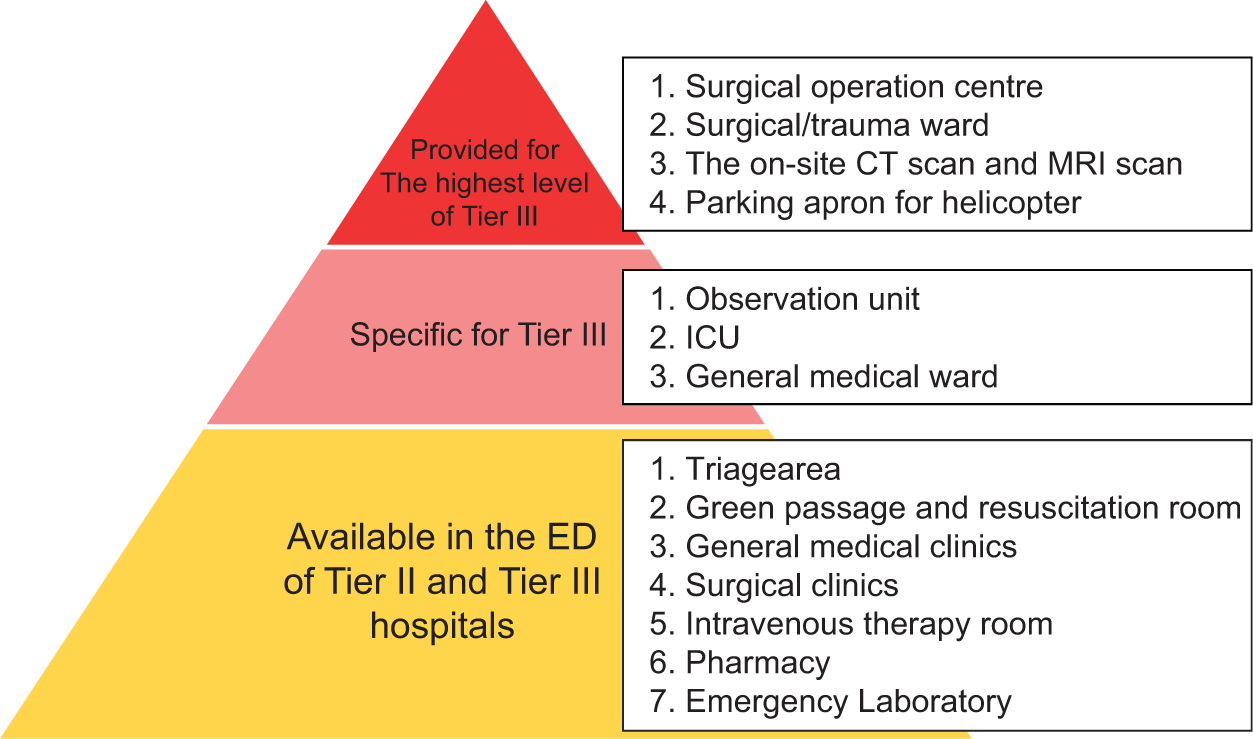
The structure and working models of the emergency department (ED) in national (tier III) and regional (tier II) Shanghai hospitals. The orange pyramid indicates infrastructures available for both hospitals. The pink pyramid indicates medical wards available only in the ED of tier III hospitals, and the red pyramid indicates medical supplies provided in the highest level of tier III.
The highest level of ED in tier III hospitals is among the 20 largest EDs in China. The EDs in the hospitals can extend their observation unit from 10 to nearly 100 beds and function as a temporary transitional inpatient ward for those who cannot be admitted to the in-hospital ward immediately because of the scarcity of bed resources. These EDs also include one surgical/trauma ward with nearly 30 beds. One of the largest EDs enrolled in this study is among the three largest EDs in China, which is well known for its scale and equipment among EDs in Chinese hospitals. The hospital has more than 100 years of history and has 1800 beds with an average occupancy rate of 105.24% from 2009 to 2011. Under the reform program, the hospital has recently built a helicopter parking apron for the transfer of critically ill patients, and this is charged by the ED department. The equipment of the ED in this hospital includes an on-site computed tomography scanner, a digital subtraction coronary angiography and a surgical operation room that is separated and available for two operations at the same time, and one surgical/trauma ward with 36 beds, besides the above equipment.
Our investigation indicates that the Chinese health care system has made significant progress in the construction of infrastructure and medical facilities, especially in tier III hospitals; thus, the equipment of their ED is among the first in the world.
The Situation of Implicating the POC Panel
Unfortunately, the EDs equipped with such novel equipment process very few POC panels, which are widely used in the United States and Europe to improve laboratory efficiency. There were only five POC machines in the 17 enrolled hospitals, including four panels in tier III hospitals and one panel in a tier II hospital. Only 6.7% of total samples were assayed by POC panels.
POC Test TAT Values Were Severely Prolonged Compared with the International Level
The P50 (P25, P75) of the TATs for POC machines (POC tests) was 47 min (39, 55.5 min) for c-TNT, 53.5 min (40, 60 min) for CK-MB, 57 min (43, 60 min) for myoglobin, 45.5 min (36, 59 min) for Nt-pro-BNP, and 52 min (30, 58 min) for D-dimer (see Table 1 ). The TATs for POC machines approached the TAT values from laboratory reports (60 min), which is far from the proposed international standard (30 min). The P50 (P25, P75) of the TATs for the laboratory report was 64 min (47, 83 min) for c-TNT, 64 min (48, 83 min) for CK-MB, 65 min (47, 84 min) for myoglobin, 60 min (46, 82 min) for Nt-pro-BNP, and 62 min (41, 88 min) for D-dimer (p < 0.05; see Table 1 ). They are nearly approaching the international standard (60 min) with the extension of 2–5 min.
Characteristics of Survey Respondents.
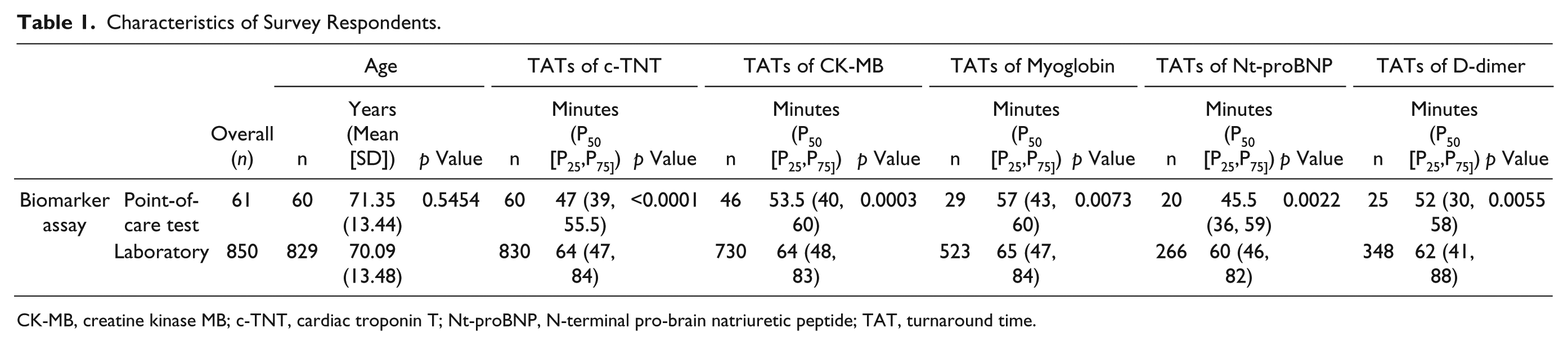
CK-MB, creatine kinase MB; c-TNT, cardiac troponin T; Nt-proBNP, N-terminal pro-brain natriuretic peptide; TAT, turnaround time.
We could not find the reason at the beginning why the TAT of POC tests was prolonged. The prolonged TAT from laboratory reports (see Table 1 ), which were 2 to 5 min longer than the proposed time (60 min), could be due to the delay in delivery, centrifuge time, or insufficient operator skills.7 –11 We wondered how the TAT of POC tests prolonged to an extent even more severe than the prolonged TAT of laboratory reports. We then did a deep investigation of the emergency management and found that the 5 POC machines were placed in the laboratories instead of at the bedside because of the limitations of hospital conditions, which prohibited two of the most important advantages of POC panels: avoiding long delivery times and decreasing reporting times. 12 This finding indicates an important problem in the administrative management of the ED. Moreover, this defect occurred regardless of the hospital tier and suggests that administrative staff lack basic clinical training. Therefore, communication between clinicians and administrative staff should be improved, and reform of ED management and administration should be advocated.
Assessment of TATs of POC Tests at Tier II and Tier III EDs according to the TATs
We assessed the TATs between tier II and tier III hospitals. Our results demonstrate that the TATs of POC tests for c-TNT between tier II and tier III hospitals were very similar (p > 0.05; see Fig. 2a ). The P50 (P25, P75) TAT for c-TNT was 47 min (40-55 min) in the tier II hospital versus 45.5 min (36.5–57.5 min) in tier III hospitals. The TATs for CK-MB and myoglobin were also close in tier II and tier III hospitals (p > 0.05; see Fig. 2b , c ). The P50 (P25, P75) TAT for CK-MB was 52 min (40–64 min) in the tier II hospital versus 54 min (42–58 min) in the tier III hospitals, and the P50 (P25, P75) TAT for myoglobin was 57.5 min (41.5–85 min) versus 54 min (49–60 min), respectively. Moreover, The P50 (P25, P75) TAT for Nt-proBNP was 42.5 min (36–58.5 min) versus 53.5 min (36–59 min). The P50 (P25, P75) TAT for D-dimer was 53 min (30–57 min) versus 39 min (29–61.5 min) (p > 0.05; see Fig. 2d , e ). This finding indicates that the prolonged TAT of POC tests exists in both the regional and national hospitals; thus, it is a common feature of the Chinese ED.
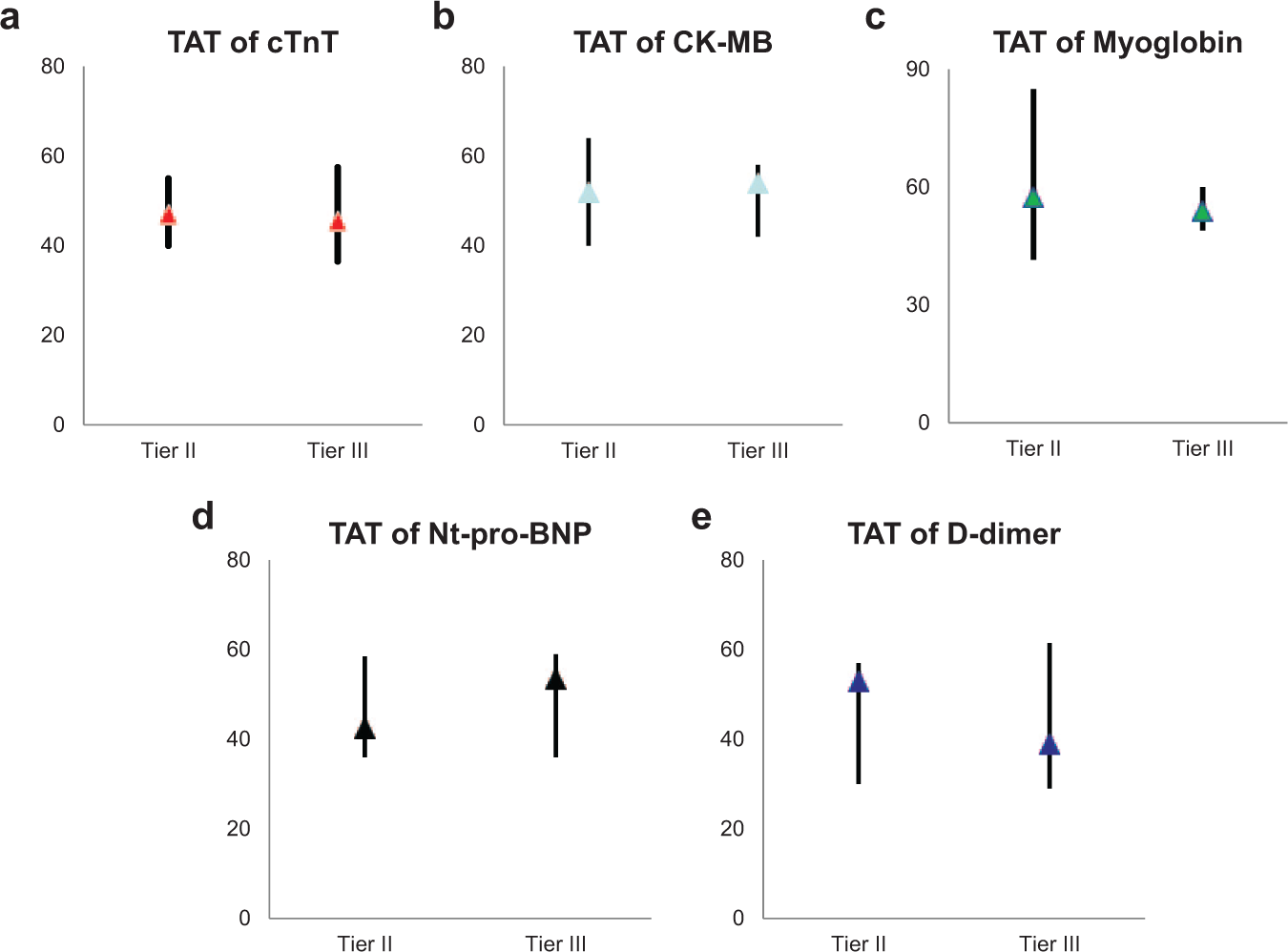
Analysis of turnaround time P50 (P25, P75) of point-of-care tests for cardiac troponin T (
Assessment of Patient Visits to Tier II and Tier III Hospitals
We investigated whether patients tended to visit tier II hospitals and determined which type of patients visited these hospitals after the health care reform policy was implemented. We analyzed disease severity and found that 61% (306) of the patients who complained of chest pain were AMI patients at tier III hospitals, whereas 46% (187) of the patients at tier II hospitals were AMI patients (see Fig. 3a ). Other diagnoses included angina pectoris, cardiac arrhythmias, pneumothorax, and pulmonary embolism (data not shown). This finding indicates that patients with severe and urgent chest pain prefer tier III hospitals, which may be due to security reasons. Similar to these results, we found that only 28% of tier III patients were chronic heart failure patients (Nt-proBNP ≥900 pg/mL) among those who underwent Nt-proBNP testing, whereas 41% of tier II patients were chronic heart failure patients (see Fig. 3b ), which suggests that patients who received previous medical treatment prefer regional hospitals that are nearby possibly because these hospitals are familiar with their cases. However, patients with acute severe symptoms or unknown discomfort visit tier III hospitals, which indicates that patients may still have doubts about the medical quality of tier II hospitals.
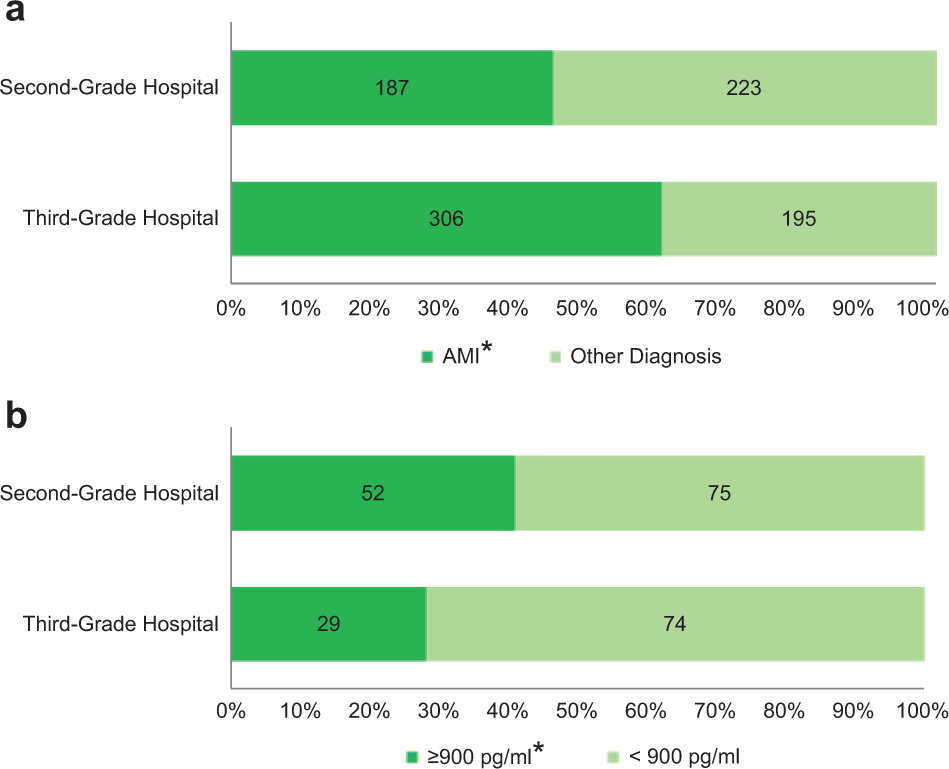
The analysis of disease characteristics of chest pain patients from tier II and tier III hospitals. (
Discussion
China has been experiencing a health care reform since 2009, and the Chinese medical environment is expected to gradually improve. 4 We investigated how the EDs at Shanghai hospitals were affected by the development of basic infrastructure and primary medical facilities, which has been attributed to the reform strategy. However, there are few statistical reports on the medical quality of Chinese hospitals and clinical effectiveness after public health reform.
Therefore, we designed an observational investigation that described the medical situation of the EDs. Although the data we collected are not standard markers for evaluating clinical efficiency, they are the first to describe the situation of EDs in Shanghai after national health care reform. These observations indirectly showed the inspiration of the reform and reveal peculiar phenomena that we did not expect.
Retardation of TATs due to the Incorrect Use of POC Panels
In this article, we investigated and analyzed the TATs of tests that are routinely used to exclude AMI and ACS 6 in independent laboratories at 17 public hospitals in Shanghai. The TATs for cardiac biomarkers were used to assess laboratory efficiency and administrative management in the EDs, as acute chest pain occurs in approximately half of the patients who are treated by internal medicine specialists in the ED, 2 and the early reporting of laboratory examinations is crucial for decisions regarding ACS treatment.13,14
We found that the TATs from POC tests are nearly 10 to 15 min (50%) longer (see Table 1 ) than guideline recommendations (30 min). It is worth focusing on the solutions to resolve the delay in POC testing. Extremely prolonged POC testing suggests that laboratory efficiency is low, and this could be a factor that directly leads to a delay of emergency diagnosis and a missed opportunity for intervention therapy. Thus, launching a standard application of POC tests, as well as spreading the use of POC machines, is a possible solution for improving the laboratory efficiency in our EDs.
These results suggest that in addition to financial support, evaluation and the close monitoring of the health care system are important to ensure medical quality.
Assessment of TATs Indicates That Laboratory Efficiency Was Similar in Tier II and Tier III Hospitals
The close TATs of POC tests in tier II and tier III hospitals suggest not only that the routine laboratory efficiency in both grades of hospitals is similar but also that incorrect usage of POC tests is a common problem in Chinese hospitals, which is independent of hospital level and infrastructure. All of these hospitals encountered defects of administrative management in the EDs. Thus, we highly advocate a next version of medical reform policy, which should be based on additional scientific studies and evaluations. These improvements will increase the clinical efficiency and cost-effectiveness of EDs and will enhance Chinese medical reform after the reconstruction of a basic infrastructure.
Our Investigation Indicates a Tendency of Patient Flow in Regional and National Hospitals
Chinese health services have been considered difficult to access with variable levels of quality. No shift in patient flow from high-level institutions to primary health care community institutions has been recorded after the health care reform policy was enacted; therefore, our results present the first report of this shift.
We discovered in this research that patients have a tendency to choose hospitals when they are affected with chest pain. The patients tended to visit tier II hospitals; however, they expressed doubt when choosing tier II hospitals for the treatment of severe diseases. Because there are numerous reasons why patients select hospitals, our results alone are not sufficient to analyze the patient flow in a general way. Moreover, the base number of tier II hospitals is two to three times larger than tier III hospitals in Shanghai, whereas the hospitals we selected for this study did not represent this difference. Thus, our data reflect only part of the phenomenon of patient flow. Thus, it is worth designing a questionnaire based on a multicenter and large sample collection of patient opinion, and we will benefit from the information by understanding why and how to improve patients’ recognition of tier II hospitals. Solutions could be found to relieve emergency overcrowding and rationalize medical service distribution.
Overall, these results suggest that in addition to financial support, evaluation and close monitoring of the health care system are important to ensure medical quality. The Chinese health care system has made significant progress in the construction of infrastructure and medical facilities and should now focus on reorganizing medical administrative affairs to improve clinical efficiency.
The POC test findings reveal several defects in ED management that cannot be corrected with increases in medical supplies or the construction of basic facilities. This finding indicates that the construction of infrastructure has been the primary focus of reform, and the administrative staff at Chinese hospitals lack medical knowledge and communicate with clinical doctors insufficiently. All of these issues should be addressed in the next version of the medical reform policy.
Footnotes
Author Contributions
Y.L., J.Y., and D.Z. studied concept and design. W.L., J.J., C.W., B.W., Y.Y., P.Y., J.T., and L.C. gathered the data. J.Y. and W.L. performed the statistical analysis and drafted the manuscript. J.Y. critically revised the manuscript for important intellectual content. J.Y. and Y.L. obtained funding. Y.L. and J.Y. supervised the whole study. Y.L. takes responsibility for the article as a whole.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant No. 81000875, 81171846, 81270433, 81372099), the Shanghai Foundation for Basic Research of Science and Technology, China (grant No. 13JC1404001), the Foundation for Committee of Science and Technology in Shanghai (grant No. 11ZR1422100), the Foundation for City Star of Science and Technology in Shanghai (grant No. 11QA1404400), and National Clinical Key Subject, China. All of these funding sources were used for data collection, statistical analysis, and service fees. No pharmaceutical company or other agency has paid us to write this article. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.