
Abstract
Introduction
Restoring pelvic ring stability is essential in definitive pelvic fracture management. Posterior pelvic ring provides 60–70% of the stability, anatomical reduction, and restoration of the mechanical stability are crucial.1,2 Percutaneous sacroiliac screws are commonly used for posterior ring fixation. For more comminuted posterior pelvic ring injury, sacral bar technique previously advocated in Cheng et al. 3 but was gradually replaced by percutaneous sacroiliac screws as possible in recent years given its high complication rate. Along with the great improvement in imaging devices and orthopedics surgical technique, navigation-guided sacroiliac screws becomes a popular technique for posterior pelvic ring fracture fixation.4–6 They are less invasive, require shorter operation time while providing adequate stability.7–10 For sacral fracture or sacroiliac joint diastasis, sacroiliac screws are gaining popularity11 and its fixation strength has shown to be comparable. However, navigation guided SI screws back-out was not uncommonly observed especially in geriatric patient or cases with fracture comminution. In view of this, iliac–sacral–iliac (ISI) fixation technique has been proposed. It was first introduced by Vanderschot et al. in 199912 and became widely used in past two decades with incorporation of navigation system. Study has shown superior biomechanical property of ISI screw over conventional sacroiliac screw.13 In our center, we have started using ISI screw in selected cases since 2019. It inserts horizontally from one side of posterior ilium to the opposite side of posterior ilium, through the whole sacral vertebra, providing additional screw purchase from multiple cortices and theoretically reducing the risk of screw back-out which could result in impingement symptom and loss of fixation. This article aims at reviewing the application of 3D-navigation guided percutaneous ISI screw. Case selection, technical execution and outcomes will be discussed.
Patients and methods
Patients with traumatic pelvic fracture admitted from 2019 to June 2023 were retrospectively reviewed. Those with sacral fracture or sacroiliac joint diastasis were included in our study. Three-dimensional navigation minimal invasive surgery (MIS) ISI screws insertion were chosen for appropriate cases. Indications include bilateral sacral fracture with subjective radiological osteopenia, sacral comminution involving both sacral alar, ipsilateral or bilateral sacral fracture with contralateral or bilateral sacroiliac joint diastasis. Feasibility of MIS ISI screw insertion in the selected cases was further assessed by preoperative planning navigation system used in pelvic computer tomography. The patient demographics, injury severity score (ISS), operative parameters, postoperative complications and radiological measurements were documented by the author.
Fracture reduction and preoperative planning
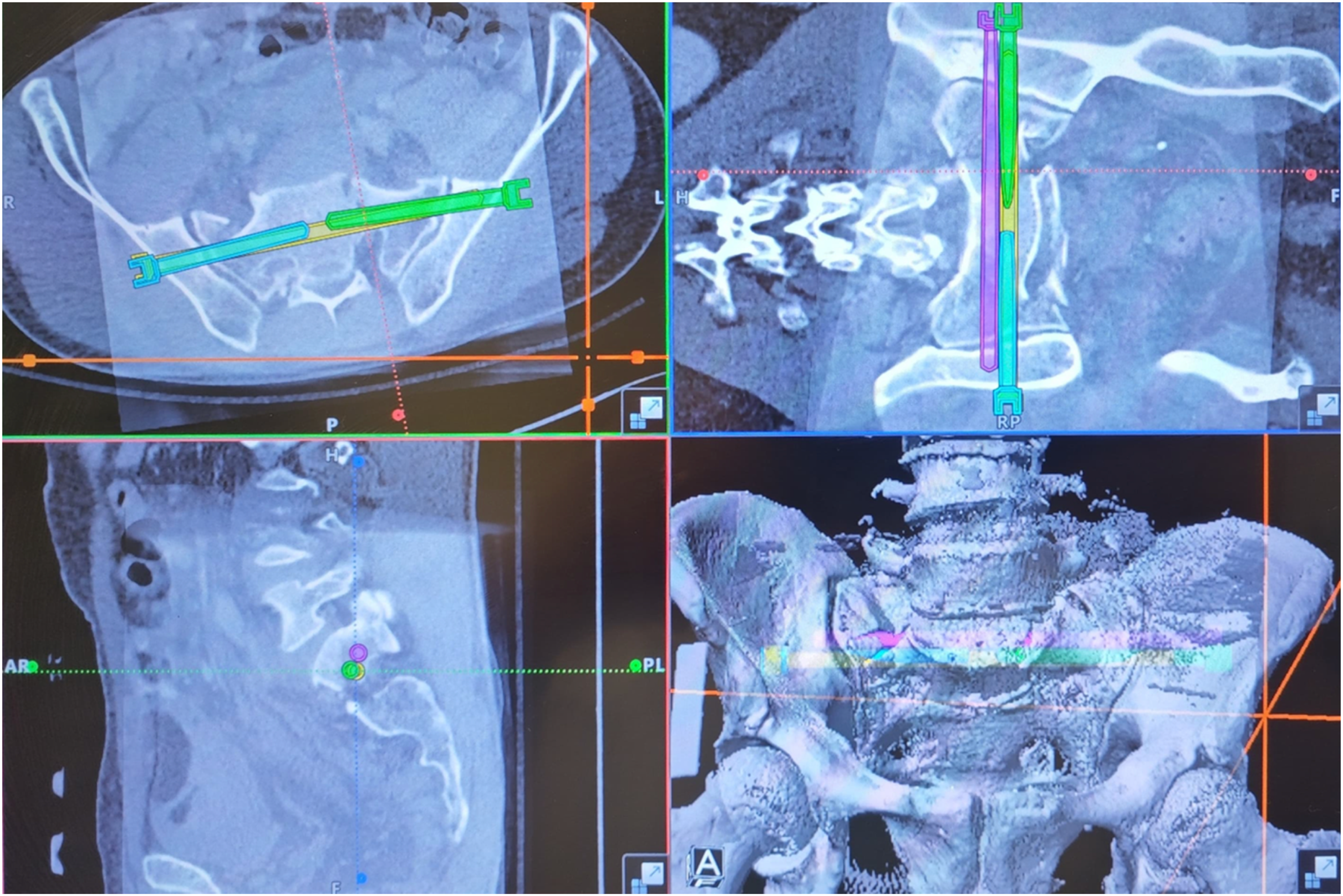
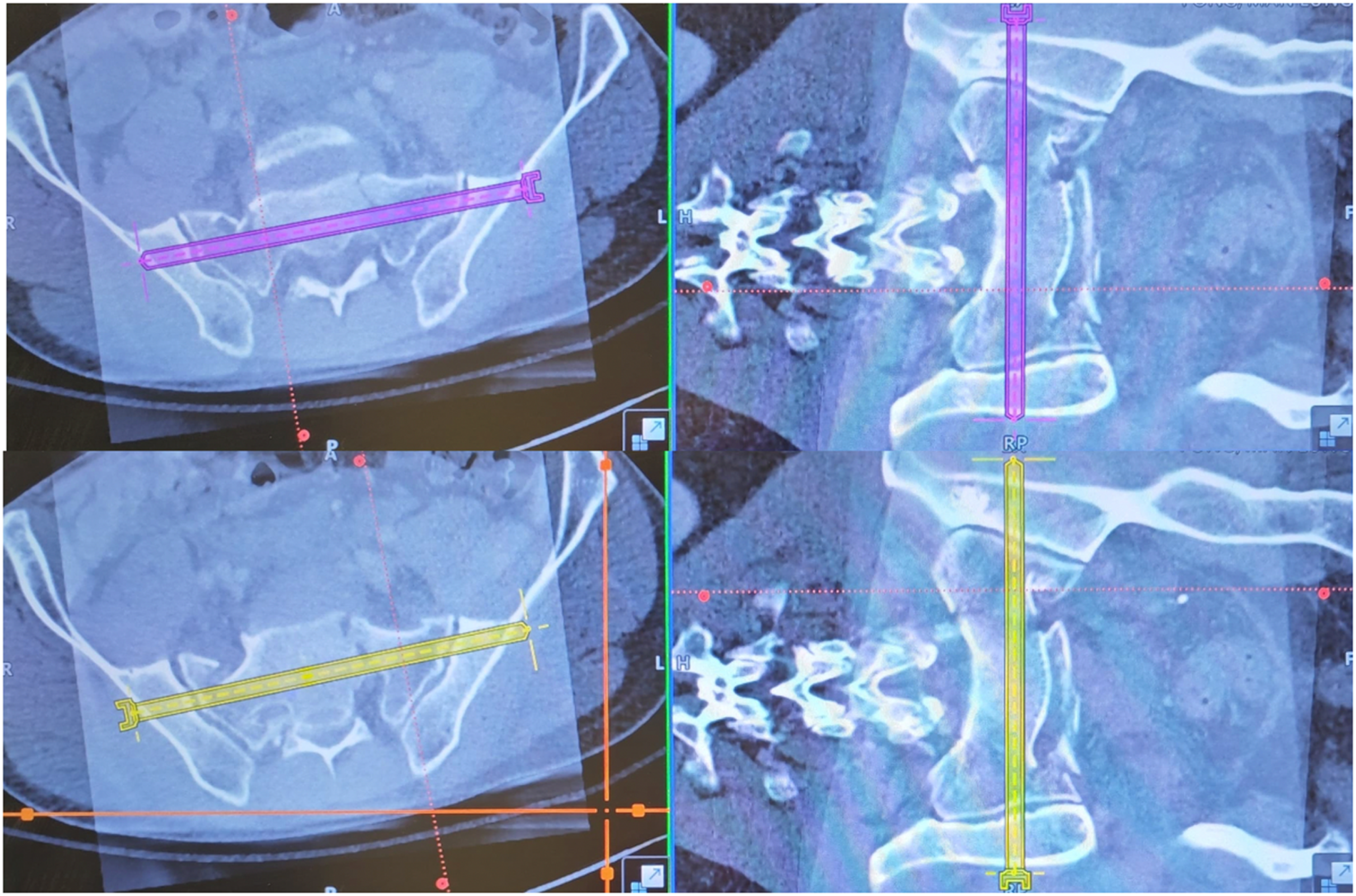
Nondisplaced or displaced but reducible fracture is one of the prerequisites for MIS fixation of pelvic fracture. Reduction, if necessary, was performed via joytstick manipulation of ilium using external fixator ± limb traction. Once satisfactory reduction is achieved, the fracture alignment will be maintained by the pelvic external fixator. After patient's hemodynamic status has been stabilized, pelvic computer tomography will be arranged before MIS surgery. The scan aims to further delineate the fracture pattern as well as the feasibility to execute navigation-guided MIS. We could plan the optimal entry and trajectory of screws insertion preoperatively, taking into account the feasibility and practicability of navigation execution (as shown in Figure 1). ISI screw will be shooting from one side of ilium, through the entire S1 ± S2, to contralateral ilium, anteriorly to avoid anterior sacral alar (where L5 nerve root locates), posteriorly to avoid spinal canal, superiorly and inferiorly to keep away from superior and inferior endplate,14,15 involving 5–6 cortices. The longest screw length available in our center was 150 mm (as shown in Figure 2). For cases with stable vital signs and simple fracture pattern, one stage close reduction + intraoperative 3D imaging of pelvis + navigation MIS could be performed.
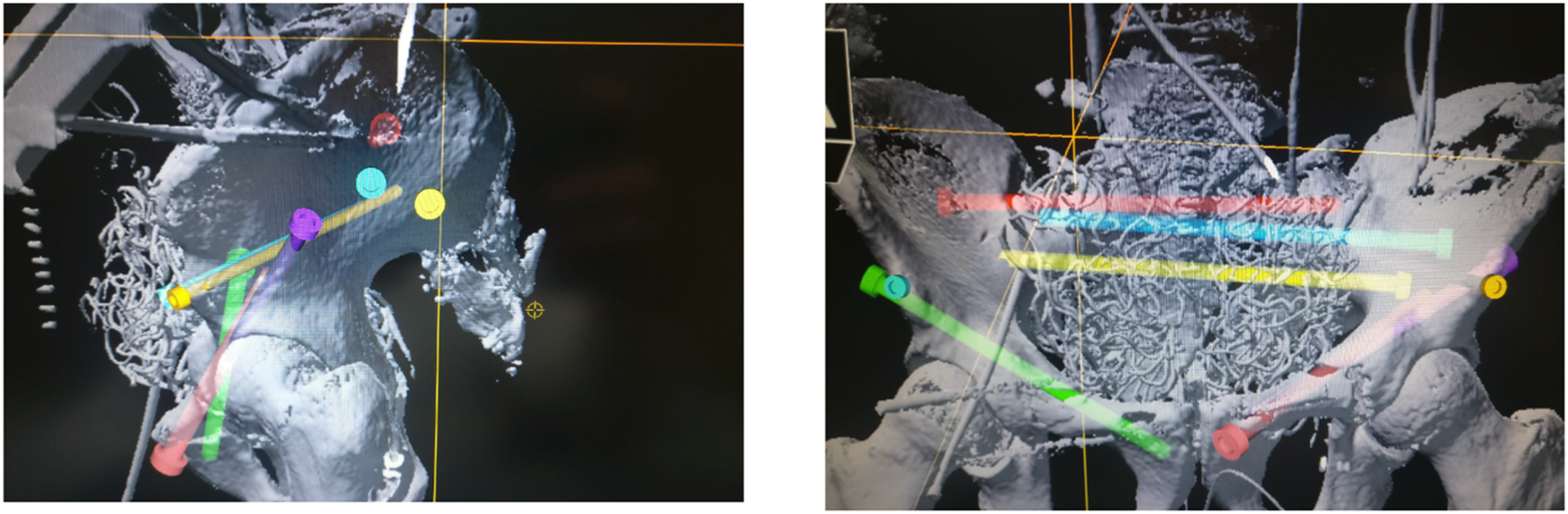
Patient's 3D surface image with transparent screw. Red, blue, and yellow screws are ISI screws.
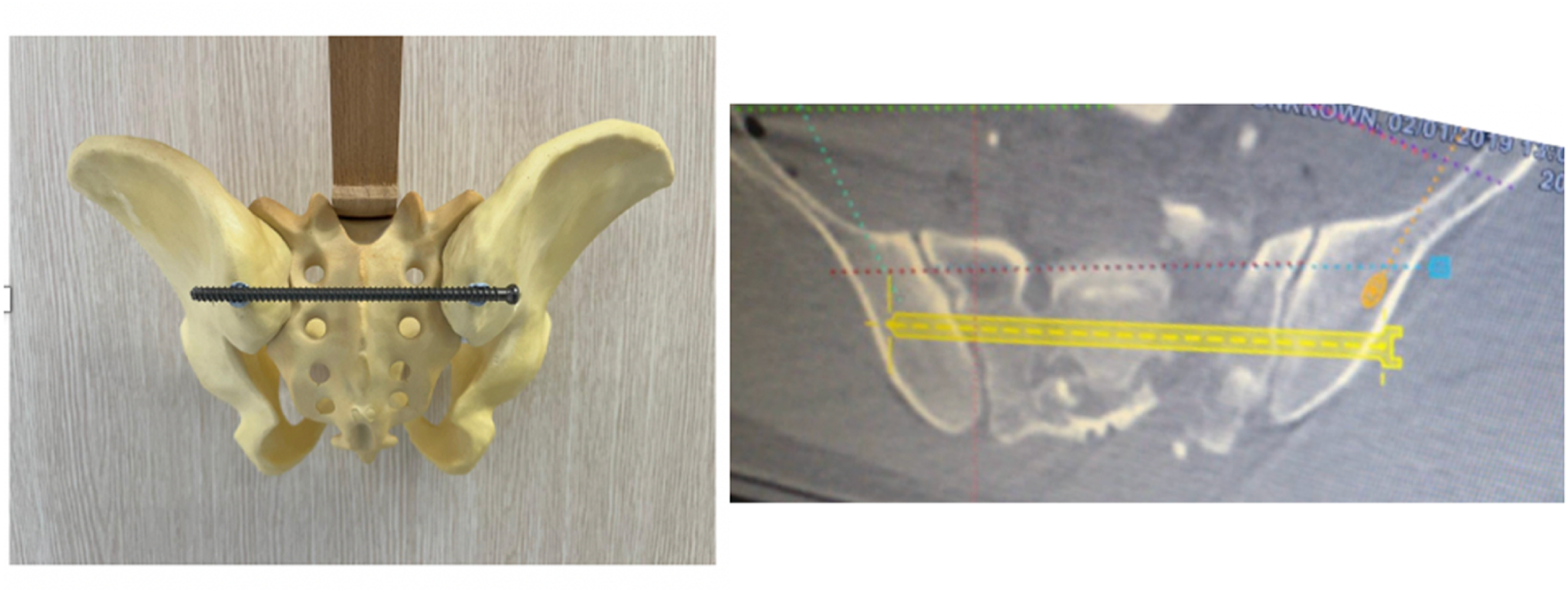
A 150 mm length and 8.0 mm diameter screw of pelvic bone model and planned trajectory in preoperative CT planning.
Operative setup and execution
Patient is given general anesthesia and positioned supine on the OSI radiolucent table. This allows intraoperative 3D screening and pelvic radiological assessment.
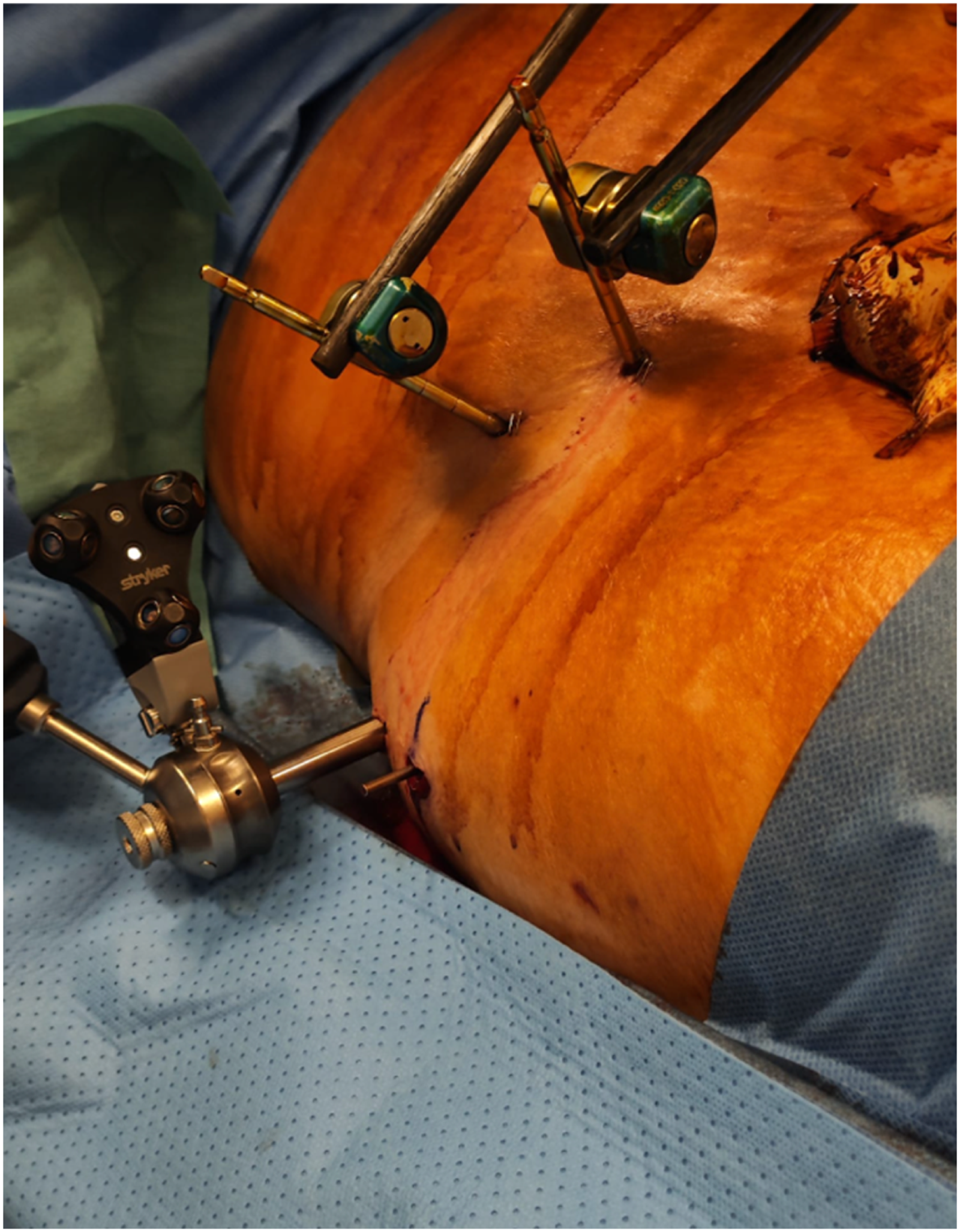
No sacral support is needed in all cases even in skinny patient as author finds this less risk of displacing sacral fracture. Stryker NAV3i navigation is connected to Ziehm Vision RFD 3D Flat Panel, C-arm is positioned to contralateral side of ISI screw insertion. In cases requiring bilateral ISI screws, C-arm will be placed at the side with less fracture complexity. Lower abdomen and entire pelvic region are sterilized and draped. A navigation-coupled patient tracker is installed on either external fixator or either side of iliac crest via a slab incision (as shown in Figure 3). Three-dimensional screening of the fracture region is performed and the resultant image is merged with preoperative CT scan.

The operative set up for intraoperative 3D screening.
If two images can be merged, we will execute as preoperative planning (as shown in Figure 4).
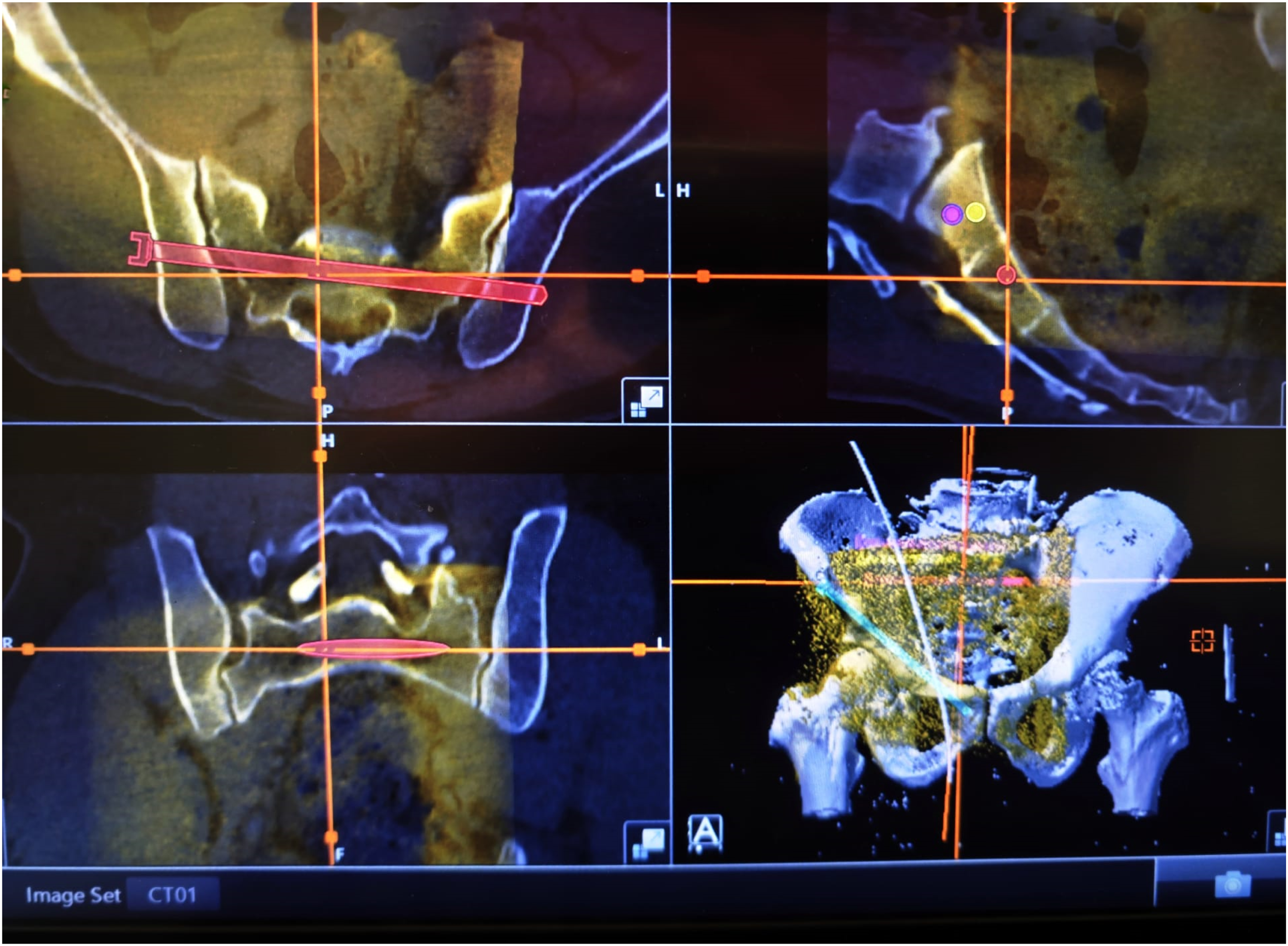
The merging of preoperative CT scan with intraoperative 3D screening image.
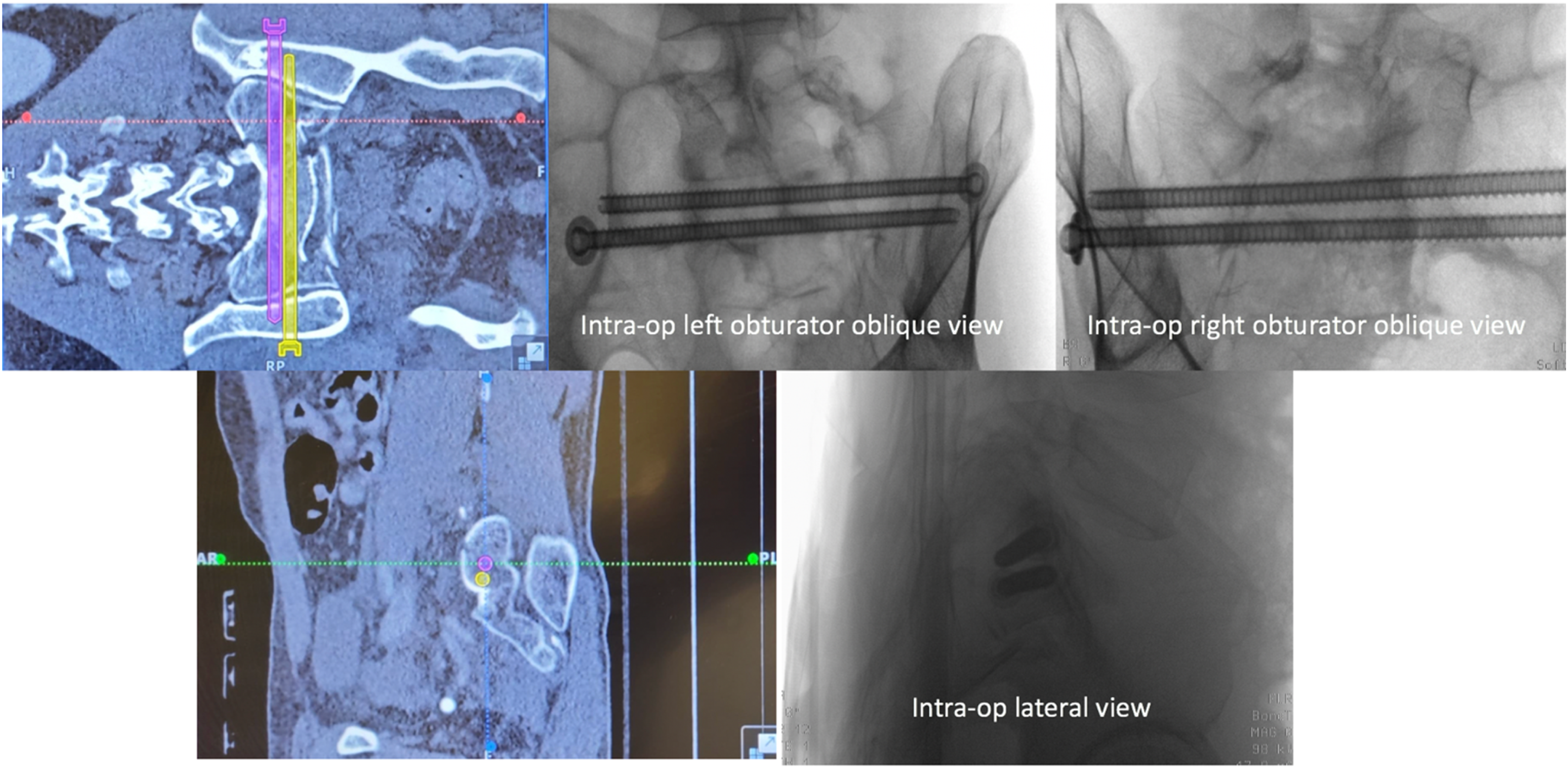
If there is any difficulty in merging two images like fracture displacement, intraoperative planning would be performed before execution. Skin incision and soft tissue dissection tract are guided by the exact screw trajectory under navigation guidance to minimize skin incision and unnecessary soft tissue trauma. Guide pins are inserted under navigation guidance (as shown in Figure 5), external fixator will then be loosened for manual compression of both ilium toward midline during insertion and tightening of cannulated screws if required. Fully threaded cannulated screws are used in these groups of patients in order to maximize screw purchase. Position of the guide pin must be confirmed with intraoperative fluoroscopy before screw insertion.
The guide pin insertion from right side of the ilium.
Immediate full weight bear walking exercise is allowed in all cases except for those with concomitant comminuted acetabular or lower limb periarticular fracture.
Postoperative radiological measurement
Relative ISI screws positions at immediate post-op and at least six months after operation on standard obturator oblique and outlet view were recorded (as shown in Figure 6).
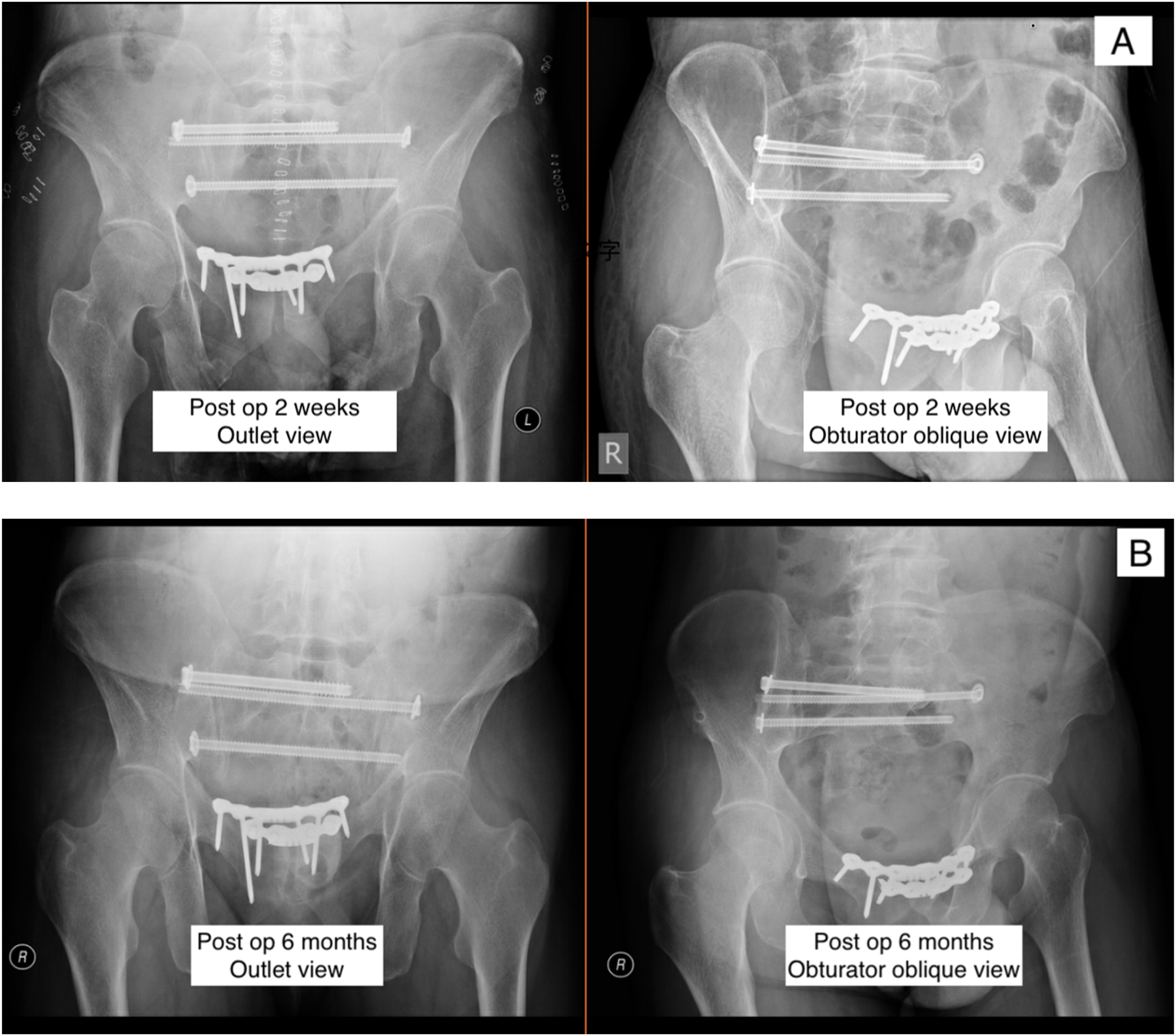
The standard outlet view and obturator oblique view of patient #5, a 51-year-old man who received navigation-guided ISI screws insertion, taken on postoperative two weeks (a) and six months (b) respectively.
The screw back-out distance is defined as the distance from the center of screw head to the outer cortex of posterior ilium at least six months after operation, compared with that immediately after fixation. All radiological measurements were done by the author.
Results
We have reviewed the cases of posterior pelvic fracture in from 2019 to June 2023. There were 18 consecutive patients with traumatic posterior pelvic ring fracture undergoing 3D-navigation-guided MIS for ISI screw fixation while another 18 patients received conventional SI screw fixation. There were 50% of the cases are amenable for ISI fixation as recruited in our study.
The following table showed the patient demographics, intraoperative and postoperative parameters (Table 1).
Patient demographics, intra-operative and post-operative parameters.
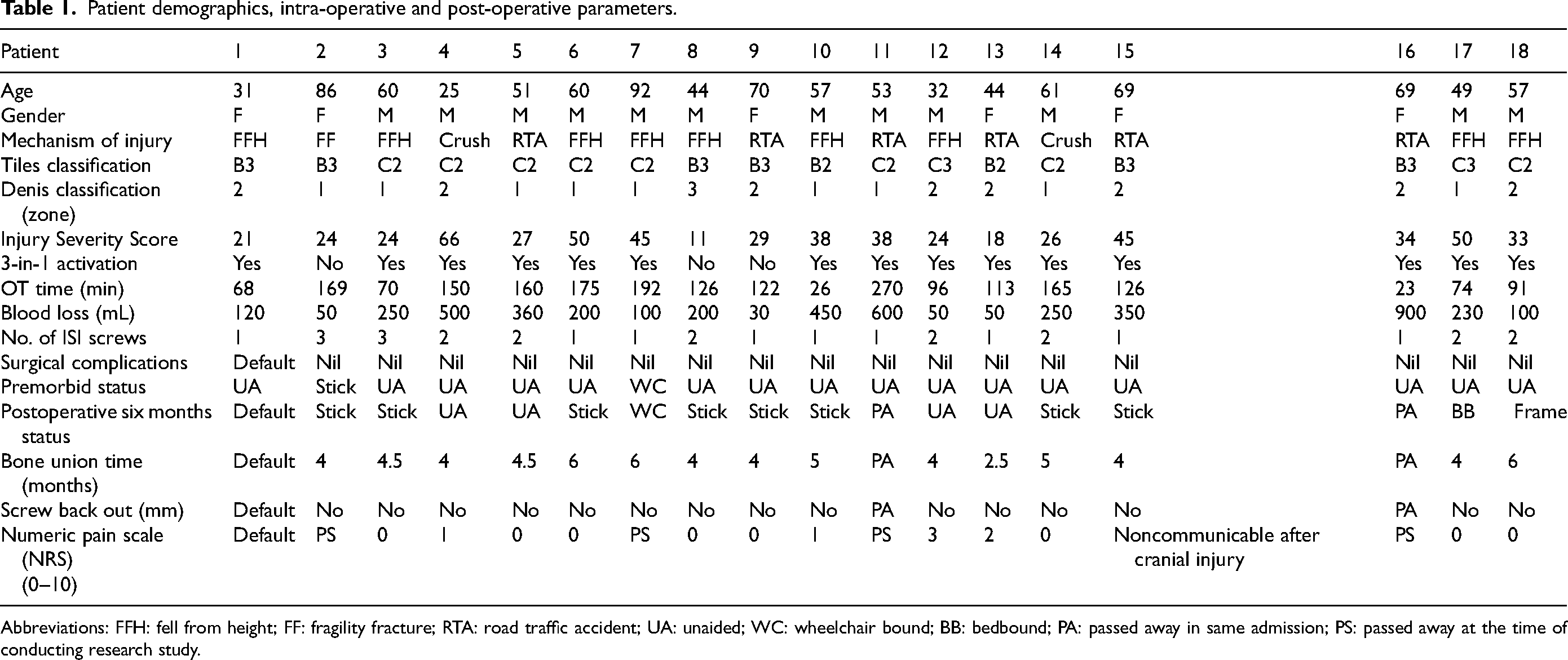
Abbreviations: FFH: fell from height; FF: fragility fracture; RTA: road traffic accident; UA: unaided; WC: wheelchair bound; BB: bedbound; PA: passed away in same admission; PS: passed away at the time of conducting research study.
The mean age was 56 (25–92) years old. Seventeen patients (95%) had multidisciplinary trauma activation at the Accident and Emergency Department upon arrival. The average ISS was 33.5 (11–66). Fifteen patients (83.3%) presented with unstable hemodynamics upon arrival, underwent our three-in-one exsanguinating pelvic fracture damage control protocol3,4,5 for emergency pelvic hemostasis including pelvic external fixation, laparotomy with retroperitoneal packing, followed by angiogram with or without embolization. Mean duration from injury to definite MIS fixation was 6.2 (1–14) days. Twelve cases (66.6%) received one-stage closed reduction, intraoperative 3D pelvis, intraoperative planning and 3D navigation-guided ISI screw insertion. The remaining six cases (33.3%) required separate operative sessions for close reduction and definitive fixation in order to prioritize management of other life-threatening concomitant injuries. Total 29 ISI screws were inserted and all of them were fully threaded, 80% of ISI screws were 6.5 mm in diameter while the remaining 20% were 8.0 mm in diameter. The average total operative time per navigated screw was 30 min (11–63 min). Average intraoperative blood loss was 266 mL, 15 cases (83.3%) had concomitant procedure performed including major limb fixation, navigation-guided screw fixation in other part of pelvis and open reduction with internal fixation of pelvic fracture which also accounted for the intraoperative blood loss.
There was no immediate, early, or major surgical complications regarding ISI screws insertion. Patient #1 was transferred to hospital in Taiwan after operation and defaulted in our follow-up. There were another two patients who passed away in the same admission after operation due to hospital-acquired pneumonia. The remaining 15 patients (83.3%) were followed up in our outpatient clinic for at least six months with X-ray. The average bone union time was 4.5 months. Among the selected cases, no cases had shown screw backout in follow up X-ray after fracture union was attained.
Nine of our cases (50%) had postoperative pelvic CT scan available and there was no cortical perforation into the sacral foramen of all screws. Among the 18 cases, nine of the cases (50%) navigation-guided ISI screw execution was performed by orthopedics trainee under supervision.
Case illustration
Patient #8 was selected for case illustration. 44/M, premorbid walks unaided who suffered from fell from height injury with comminuted bilateral sacroiliac fracture (as shown in Figure 7) and right foot multiple fractures.
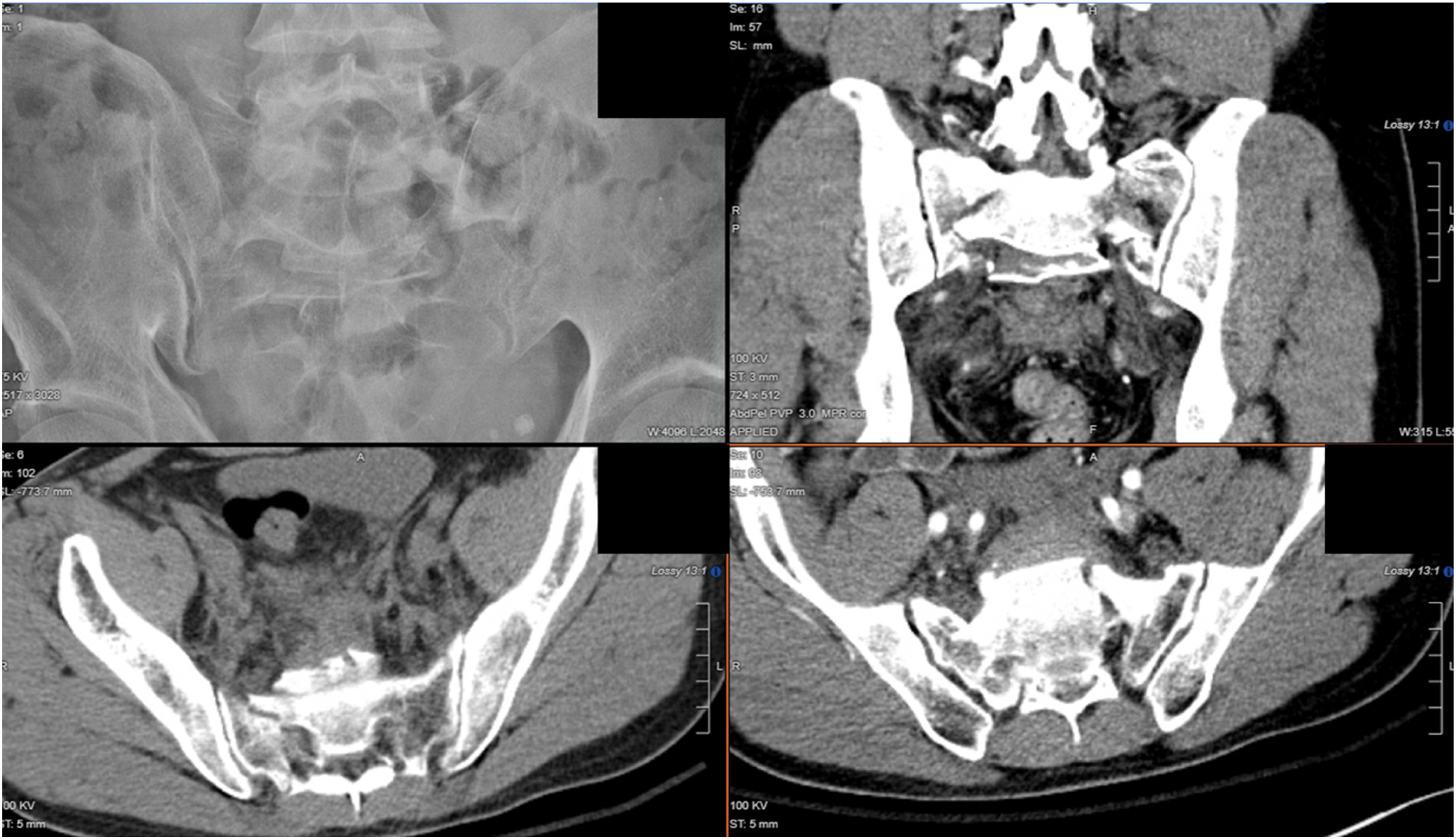
The preoperative imaging findings. XR and CT pelvis showed comminuted bilateral sacroiliac fracture.
Preoperative CT scan performed with screws insertion trajectory planned (as shown in Figure 8).
Our previous practice for comminuted bilateral sacral fracture by inserting two sacroiliac screws (blue and green) versus our current practice with ISI screws (purple and yellow).
As ISI screw's maximal screw length available in our center is 150 mm, sometimes in cases with large body build or wide pelvis, the optimal cortical purchase is limited (as shown in Figure 9).
The planned trajectory of two 150 mm ISI screws in our selected case.
In order to maximize fracture fixation, two ISI screws were inserted in this case. Intraoperative XR were taken to confirm the correct position of the screws (as shown in Figure 10).
The planned trajectory of the two ISI screws and intraoperative screw position under fluoroscopy.
Patient was discharged 11 days after the index operation. Subsequent follow-up XR showed bone union at four months after operation (as shown in Figure 11), and patient could walk with stick upon eight months follow-up.
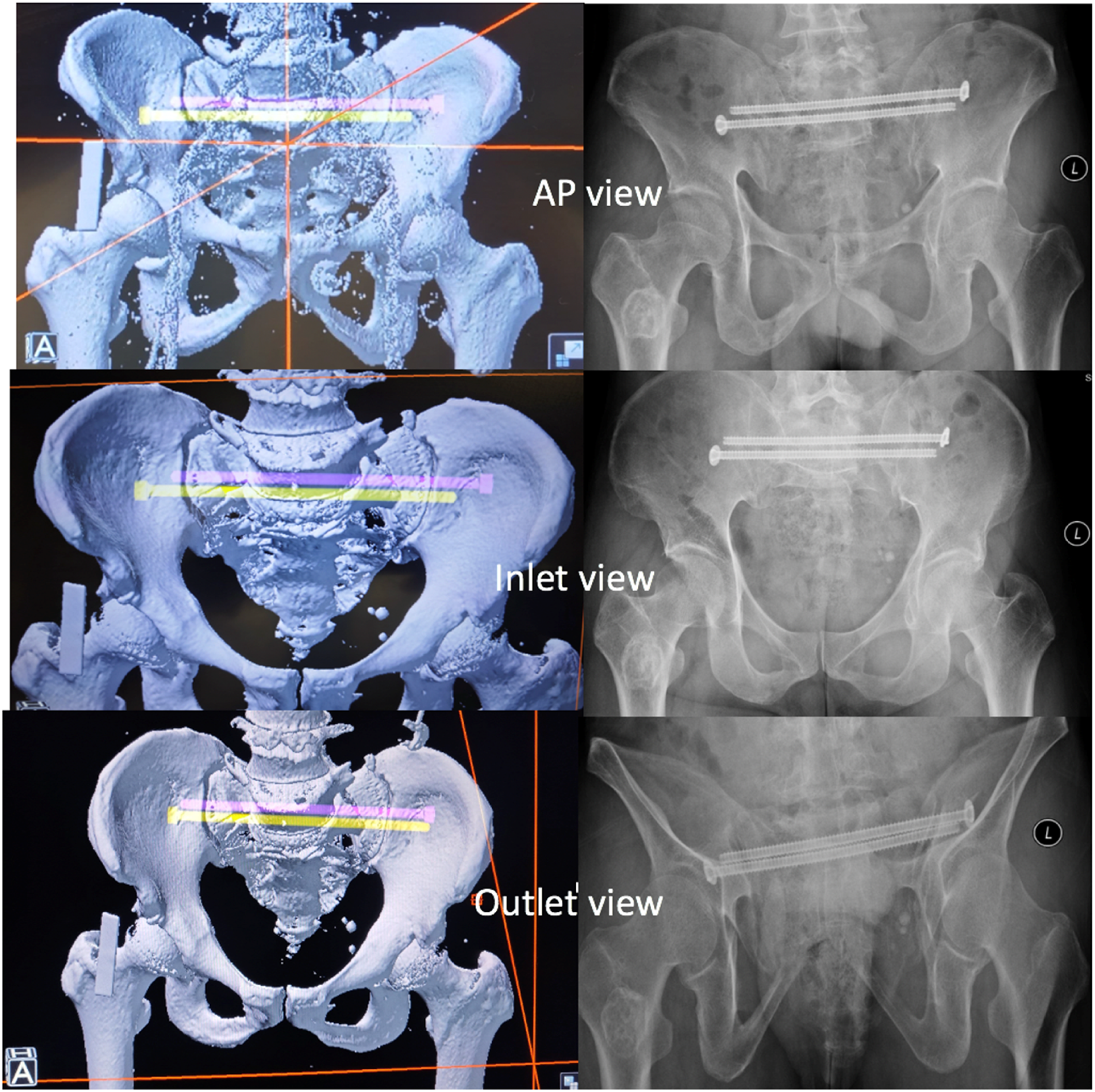
The planned screw trajectory in CT scan and postoperative 1 year XR in both AP, inlet and outlet view.
Discussion
Traditional sacral bar technique is associated with more difficulty in patient positioning, larger surgical wound, greater blood loss, higher chance of soft tissue complications, and longer operation time.16,17 Percutaneous screw under 3D navigation not only shows comparable biomechanical stability, it shortens the operation time with less blood loss and soft tissue jeopardy.18,19,20 It also allows patient to be operated in supine position which associated with less venous obstruction, pressure injury, and easier resuscitation if needed.21,22 However, sacroiliac screw fixation purchases are limited by short screw length owing to its trajectory, regional bone quality, fracture pattern, etc. Based on our previous review on 3D navigation MIS fixation for consecutive 38 pelvic-acetabular fracture cases23 we have noticed 12.7% of total screw backed out for an average of 5.3 mm. When focused on sacroiliac screws only in the same database, the average SI screws inserted was 73.7 mm and there was 16.4% of SI screw back out for an average of 4.45 mm. From our experience since 2015 to 2024, navigation guided SI screws back-out was consistently and commonly observed, especially in patients with suboptimal bone quality or sacral comminution. When focusing the group of patients received conventional SI screw fixation in the same period, there was 4.8% screw back-out with an average distance of 18 mm. Screw backout may lead to severe consequences including impingement, risk of surrounding neurovascular structure and even loss of fixation (as shown in Figure 12).
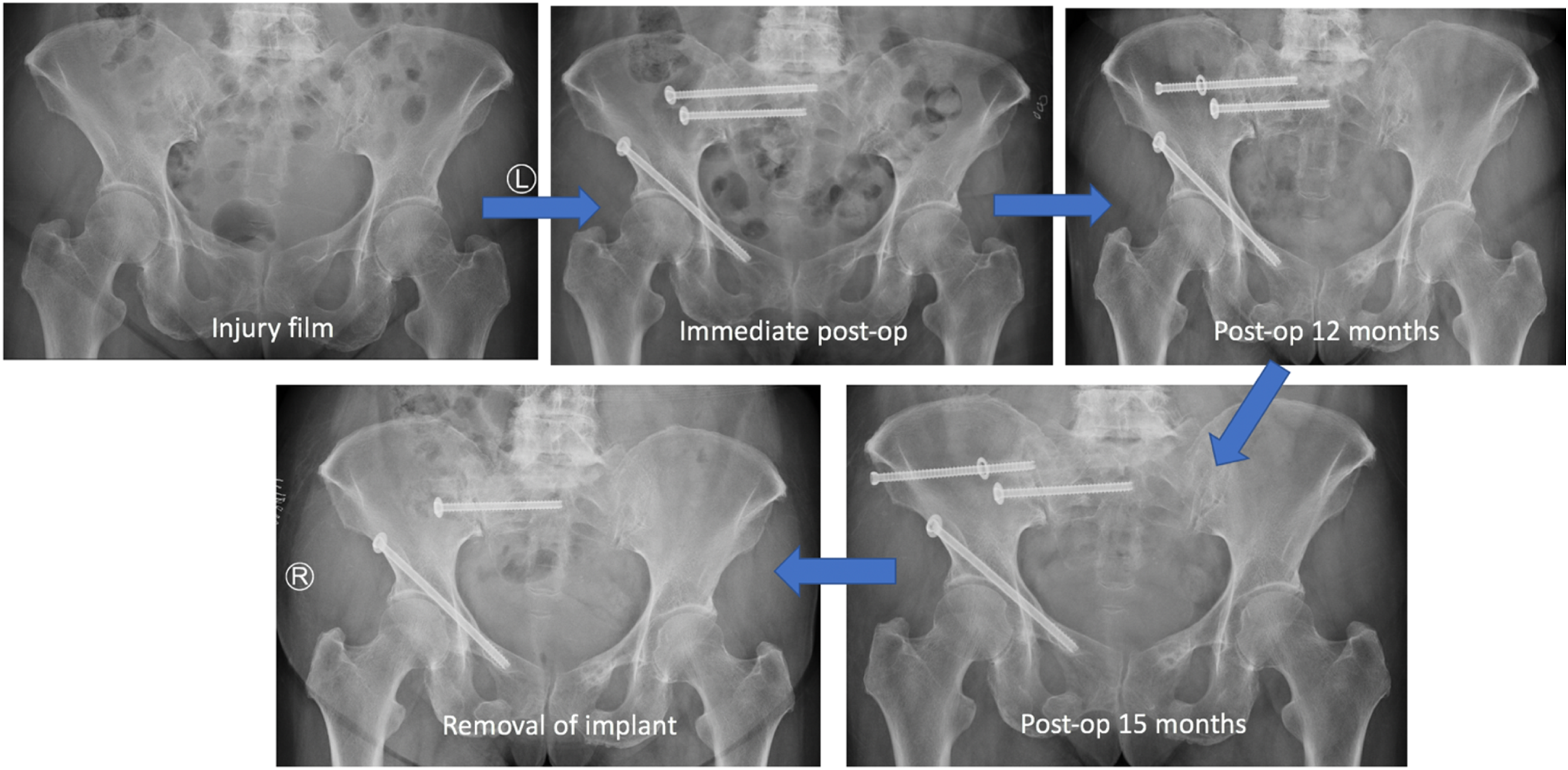
Case of an 82/F with fragility pelvic fracture, received navigation-guided SI screw fixation. Subsequent follow-up showed progressive back out of the screw with impingement symptom, requiring removal of implant eventually.
When compared to traditional SI screw, ISI screw not only has longer screw length (longest screw available in our center is 150 mm), it could also anchor into bilateral iliac cortical bone and achieve better mechanical stability, and theoretically also better maintain sacral alignment and sacral width especially in sacral comminution because the long positional screw can span bilateral SIJ cortices with screw threads (as shown in Figure 13). Reuther et al.24 reported 14% of iliosacral screw back out upon the total 85 screws inserted, while in our study none of the ISI screws showed back out.

Patient #2, a case of an 86/F with pelvic fracture received MIS-guided ISI screws + right retrograde acetabulum screw + left antegrade ISI screw insertion. Subsequent XR showed back-out of right acetabulum screw while ISI screws all remained in-situ. It demonstrated that in advanced age patients with suboptimal bone quality who are more prone to have screw back out, ISI screws with more cortical purchase could maintain better mechanical stability and less back-out.
Practically, unlike cases requiring bilateral SI screw which the contralateral SI screw may be physically blocked by the C-arm, ISI screw could accommodate more flexible C-arm positioning. Moreover, traditional SI screws are usually inserted via S1 vertebra which is larger in size, but more inclined in anatomy due to limited visualization of sacral anatomy in X-ray. Thanks to the maturation of navigation technique, with comprehensive and careful preoperative planning, insertion of screw through difficult anatomical region such as S2 in this review becomes feasible.25 S2 usually provides a long and straight corridor which can accommodate a 6.5–8.0 mm screw (as shown in Figure 14). Anatomically, S2 vertebra has flatter surface, reducing the chance of drill guide slipping away when it is placed on the outer table of posterior ilium. Unwanted slip of drill guide is not uncommon during drilling, inadvertent slippage into greater sciatic notch may result in neurovascular injury.26,27 Author sometimes found it is even easier to plan and execute S2 screw insertion than S1. Most of our patients could achieve good walking status except patient #17 and patient #18, who both suffered from multiple level of spinal fracture with neurological damage at the time of injury.
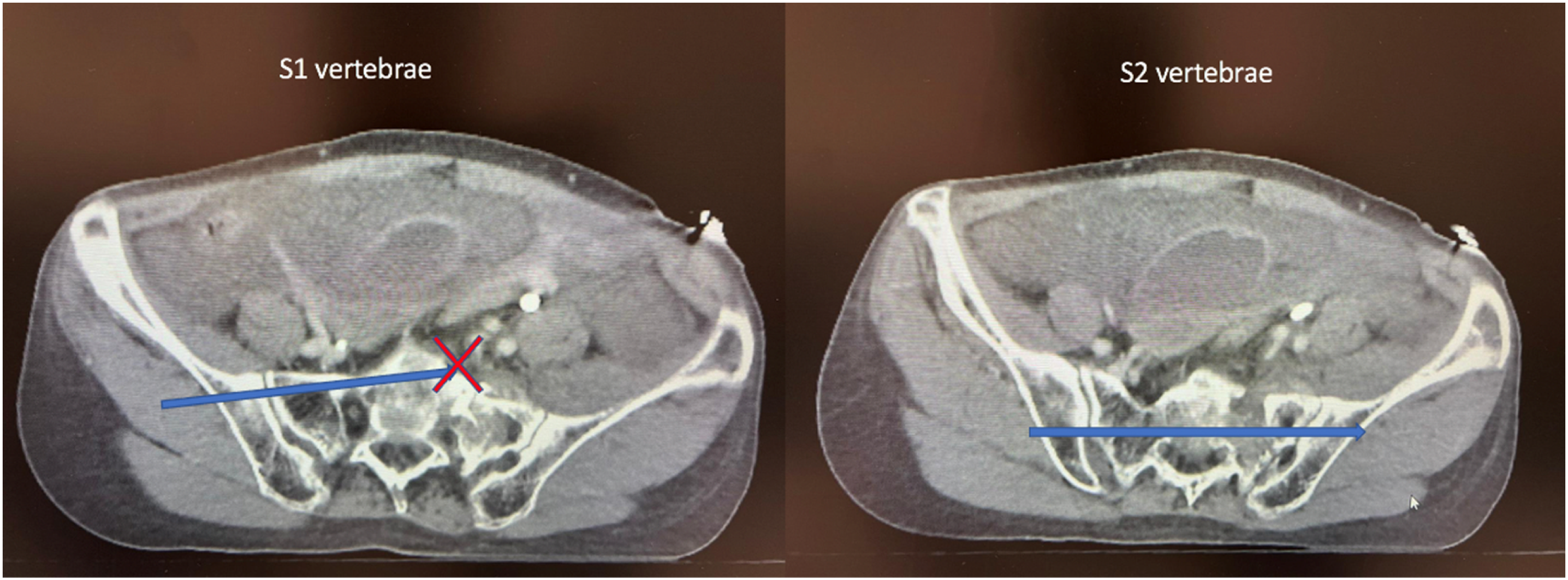
The planned trajectory of ISI screw (blue arrow) in S1 and S2 vertebrae in the same patient. The left photo showed despite S1 vertebrae is larger in size, its relatively inclined anatomy sometimes may not accommodate the ISI screw. The right photo showed more straight bony corridor in S2 vertebrae allowing the passage of the ISI screw.
The learning curve of navigation-guided ISI screw insertion is not steep and the results are reproducible. In our reviews, 50% of cases were performed by orthopedics trainee under supervision.
However, there are several contraindications of ISI screw insertion including unacceptable sacroiliac joint or sacral alar reduction, impossible trajectory due to significant fracture displacement, posterior ilium comminution at where screw entry is planned and inadequate sacral bony corridor in accommodating the screw.18,28 In this review, parameters including intraoperative blood loss, radiation time, transfusion rate, and postoperative rehabilitation status could not be individually measured for ISI screw insertion alone as most of our patients were suffered from polytrauma. The authors find that the blood loss for ISI insertion alone was minimal following navigation-guided skin incision and gluteal muscle dissection along screw trajectory (as shown in Figure 5) where only trace amount of blood stained on the operation drape after insertion of the guidepin and screw.
Although navigation itself is accurate, surgeon still need to verify the trajectory and position of screw very carefully with the intraoperative XR. Technical error including failure of calibration or human error like accidental displacement of patient tracker should actively be aware of throughout the procedure.28,29,30 During execution, it is essential to ensure guidepin is in coaxial position before screw insertion, otherwise the drill bit may break at intraosseous corridor while drilling. Single-use guide pin is also advised.
In our selected cases, only 50% cases had follow-up pelvic CT performed due to concomitant intra-abdominal trauma in the primary injury. Nevertheless, X-ray in most cases can confirm union and screw position in good quality inlet, outlet, and obturator oblique view. Three-dimensional navigation-guided ISI screw fixation had relatively short operation time with minimal blood loss. It had no significant procedure-related complication, bone union could be achieved in a reasonable time with no obvious screw back-out observed.
Limitations of this study include its relatively small patient sample, its inherent retrospective design and the lack of objective functional score. Furthermore, the heterogeneity in patient's demographics and injury patterns may complicate the analysis.
Conclusion
Three-dimensional navigation-guided percutaneous ISI screw provides rapid and stable restoration of pelvic anatomy. It is a safe and promising fixation alternative to ORIF or percutaneous sacroiliac screw in case of comminuted sacral fracture or bilateral sacroiliac joint injuries, not only does it shorten operation time, it also minimizes soft tissue dissection. It is especially important in cases of polytrauma patient who have multi-organ disturbance and concomitant local soft tissue injuries. When compared to traditional sacroiliac screw, ISI can achieve more cortical purchase with better mechanical stability, reducing the chance of screw back out and loss of fixation especially in patient with suboptimal bone quality. The result of this surgical technique is also reproducible with reasonable learning curve. With the rapid advancements in modern technology, artificial intelligence is widely integrated into multiple aspect of medical care. We believe that it will also play an important role in advancing navigation-guided surgery in the future, including planning safe corridor in anatomically difficult cases like sacral dysmorphism, improving accuracy in screw insertion and improving surgical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our study has been approved by the Hong Kong Hospital Authority Central Institutional Review Board (Central IRB).