
Abstract
Background
Fragility fractures of the posterior pelvic ring are associated with osteoporosis and are becoming more common with demographic change. Known limitations of conservative therapy include a significant loss of autonomy and high mortality. Surgical stabilisation using percutaneous sacroiliac (SI) or trans-iliac trans-sacral (TITS) screws, has been established to increase mobility, but long-term results have not yet been studied.
Materials and Methods
138 patients with percutaneous SI and TITS screw fixation of the posterior pelvic ring in osteoporotic fragility fractures were followed up for more than a year postoperatively in this retrospective study. Thereby, all patients were operated in the conventional supine position in a hybrid operating room consisting of a fixed, robot-assisted 3D flat-panel detector and a navigation system.
Results
34 patients were male and 104 female. The mean age was 77.6 ± 9 years. 26 patients were ASA 1 + 2, 93 patients ASA 3 and 19 patients ASA 4. 80 fractures were classified as FFP 2, 23 FFP 3 and 35 FFP 4. Time to surgery was 127.5 ± 113.2 hours. Hospitalisation lasted an average of 15.7 ± 8.5 days. At the time of discharge, 68.8% of the patients had regained their original mobility, while 31.2% remained limited. The home situation remained unchanged in 73.9% of the patients, worsened in 26.1% and improved in 2.8%. 90.6% of the screw fixations showed no signs of loosening. In 9.4%, loosening could not be ruled out radiologically, but a surgical revision was not necessary. The 1-year mortality rate was 10.1%.
Conclusion
Percutaneous navigated screw fixation of the posterior pelvic ring in fragility fractures is a simple, safe, minimally invasive and precise method with good clinical results in terms of rapid recovery with early mobilization of patients to maintain autonomy and reduce mortality. Further clinical studies with controlled cohorts and a large number of patients with long follow-up periods should be carried out to compare the procedure with other methods. In particular, the question of an additional standardized treatment of the anterior pelvic ring in unstable dislocated fragility fractures should be investigated.
Keywords
Introduction
About 7% of all osteoporotic fractures in patients over 50 affect the pelvic ring and the incidence is 25-92/100000 with an upward trend. 1 Thereby the number of pelvic procedures has increased significantly in recent years. 2 Conservative treatment results in a major loss of autonomy compared to the level of activity before the fracture, with a doubling of the daily support required and a mortality rate of around 20%. 3 A considerable deterioration in mobility must be expected not only temporarily but permanently, with up to 40% of patients not fully recovering. 4 Patients with fragility fractures of the pelvis, regardless of age and gender, report long-lasting pain that severely impairs their everyday life, so that they cannot return to their normal state before the injury. 5 Osteoporosis is the most common cause of sacral insufficiency fractures. The clinical symptoms are very unspecific, so that diagnosis and treatment are often delayed and conventional X-ray diagnostics are not sufficient. Computed tomography (CT) is the gold standard for pelvic fractures, but magnetic resonance imaging (MRI) and dual energy / spectral CT are significantly more sensitive for fragility fractures.6-10 A fracture classification frequently used in everyday surgical practice is fragility fractures of the pelvic ring (FFP), which also provides suggestions for conservative (FFP 1 a + b) and surgical treatment (FFP 3 and 4 a-c). FFP 2 a-c fractures can be treated conservatively or surgically depending on the patient’s symptoms and ability to mobilise.11-13 Another classification system is the osteoporotic fractures of the pelvis (OF-pelvis), which also uses CT and MRI images to differentiate between five fracture groups and thus derive corresponding treatment recommendations. 14 If surgery is necessary, various treatment alternatives are possible. In sarcoplasty, cement is inserted into the fracture zones via cannulas,15,16 but a potential leakage of cement into the fracture gaps (27%), into venous vessels (6%), into the neuroforamina and into the intervertebral disc space L5/S1 (2%) has been reported. 17 Conventional screws or plates as well as open transiliac bridge plate osteosynthesis are also used less frequently due to their considerable invasiveness. 18 In addition, the posterior pelvic ring can be stabilised with a transiliac internal fixator (TIFI) based on the surgical treatment of fractures of the spine with a screw rod system.19,20 A widely used extension of this method is spinopelvic fixation, in which the internal fixator extends from the ilium to the lumbar spine. 21 With decreasing invasiveness, lumbopelvic fixation as well as stabilisation with sacral bars or long transiliac transsacral screws (TITS) are most commonly used today.22,23 In the current literature, these three methods and their common modifications continue to be the subject of lively debate. There is still some disagreement regarding a treatment recommendation as the gold standard, primarily due to a lack of clinical data. 12 In the meantime, percutaneous cannulated screw osteosynthesis has developed into a simple, low-risk and reliable method that is also very minimally invasive and very precise.18,24-27 Depending on the fracture and sacral morphology, sacroiliac (SI) screws are used unilaterally or bilaterally as well as transiliac-transacral (TITS) screws at several sacral heights, because surgical fixation should obtain adequate stability, yet be as less invasive as possible. 18 But if possible, TITS should be used in preference to SI screws to increase stability.23,28 The main problem with SI / TITS screw implantation is the potential for malpositioning with possible damage to the neurovascular structures and fixation in the osteoporotic bone. A malpositioning rate of 2 to 15% has been reported29-31 with an incidence of neurological damage between 0.5%–7.7%. 31 In this context, it has been shown that the implantation of cannulated screws using image-guided 3D computer navigation is significantly more precise than under conventional X-ray control.29,32-36 In order to achieve the best possible fixation in the osteoporotic bone, the screws are selected as long as possible with a large diameter and continuous thread.37,38 If necessary, additional cement augmentation can be performed. Depending on the fracture morphology, ventral stabilisation with a fixator, additive screws or plates can also be applied.12,39-41 The stability of SI and TITS screws for osteosynthesis in osteoporotic bone has now been well investigated biomechanically. 23 However, the in vivo outcome has so far mainly been investigated under inhomogeneous conditions, in smaller patient groups and over a short follow-up period.18,24-27 So the aim of this retrospective study was to investigate the demographic, clinical and radiological long-term results of a larger group of patients with fragility fractures of the posterior pelvic ring and surgical stabilisation with SI and TITS screws.
Materials and Methods
The approval of the ethics committee for the use of the data was obtained. Between January 2018 and December 2020, 138 patients with osteoporotic fractures of the pelvis were treated using percutaneous SI or TITS screws and included in the study. Inclusion criteria were a low energy trauma or no adequate / ascertainable trauma with a proven fragility fracture of the pelvic ring and inpatient treatment with surgical therapy. Completely conservatively treated fractures were excluded from the study. All fractures were categorised according to the FFP classification. 11 Patients with FFP1 fractures were treated conservatively, patients with FFP3 and FFP4 fractures were treated surgically. Patients with FFP2 fractures were initially treated conservatively with painkillers and physiotherapeutic mobilisation under thrombosis prophylaxis. If adequate mobilisation could not be achieved over 5-7 days, the indication for surgical stabilisation was made together with the patient. In principle, the treatment strategy was selected according to the FFP classification recommendation, but was adapted individually for each patient on the basis of their physical condition, the existing sacral and fracture morphology and any instabilities. Percutaneous SI and TITS screws were used solo or in combination at the level of the first and/or second sacral vertebra (S1/S2), if necessary together with additive ventral column screws, an external fixator or a symphyseal plate. In our hybrid operating room, which consists of a fixed robot-assisted 3D flat-panel detector image converter (Artis zeego, Siemens Healthineers, Germany) combined with a carbon operating table (Trumpf, Germany) and a navigation system (BrainLab Curve, BrainLab, Germany), the patients were operated on in the supine position. At the beginning of the operation, a reference was attached to the iliac crest, then an intraoperative 3D scan was performed and the data sent to the navigation system. A 3.2 mm Kirschner wire (K-wire) was then inserted according to the planned trajectory using a navigated drill guide. The exact wire placement was checked with a second 3D scan and after confirming the correct position, the 7.3 mm cannulated screw was inserted with a washer. Depending on the fracture and sacral morphology, the screws were inserted unilaterally or bilaterally at S1 and/or S2 height. Over the course of the study period, the authors implanted an increasing number of fully threaded TITS screws depending on the possible corridor in the sacrum due to higher primary stability. Postoperative mobilisation was always permitted with free functional mobility and full weight bearing. For the retrospective analysis, clinical records, including patient files, laboratory results and X-rays, were reviewed. Patient-related data such as age, gender, BMI (body mass index) and ASA (american society of anaesthesiologists) classification were collected. In addition, preoperative CT images were analysed for FFP fracture classification. Clinical and radiological follow-up examinations were standardised at 6 weeks, 3 months and one year postoperatively. In these follow-up examinations, the X-rays were analysed for secondary dislocation, screw loosening and implant fracture as well as pseudarthrosis. The patient’s mobility and place of residence before the accident and after surgical treatment were assessed, as well as any differences between the two. Surgical (injury to nerves, vessels, muscles and organs as well as haemorrhage, haematoma, wound healing disorder and infection) and non-surgical complications (cardiovascular, respiratory and organ-specific as well as general damage and disorders) were investigated. The time from hospitalisation to surgical treatment was counted as time to surgery in hours and the days until discharge were defined as the length of the hospital stay. One-year mortality was analysed using the German civil register.
Statistical analysis: The data was analysed using IBM SPSS Statistics (V21.0) and Microsoft Excel (V16.3). Due the explorative study type no power analysis was performed. All patients in the described timeline were included resulting in a large cohort compared to current literature. Demographic characteristics were described as mean and standard deviation. A total of four outcome measures were analysed using logistic regression for various variables. The primary endpoints were 1-year mortality and length of hospital stay, and the secondary endpoints were differences in mobility and living at home. Tested Variables for the primary and secondary outcomes were patient age, gender, ASA, FFP, non-surgical complications and time to surgery.
Results
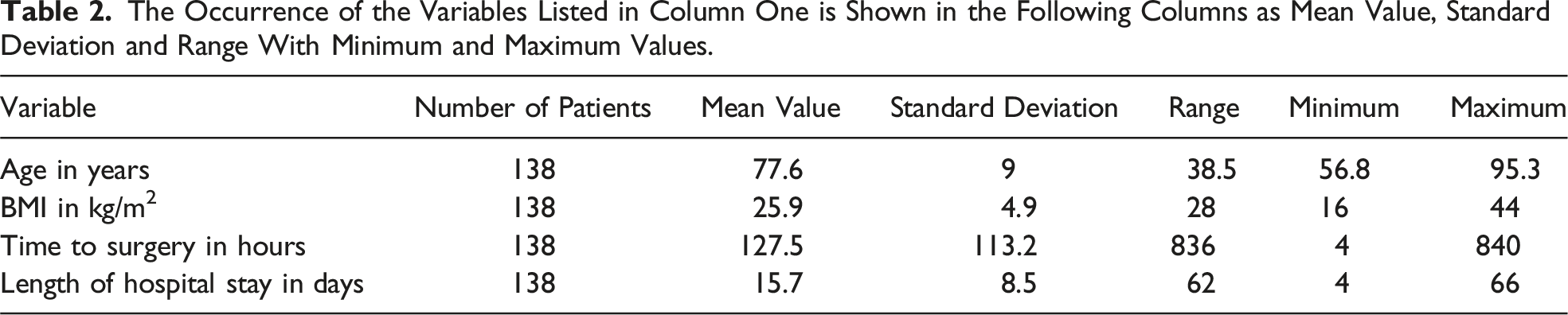
A total of 138 patients were included in the retrospective study. Of these, 34 (24.6%) were male and 104 (75.4%) female. The mean patient age was 77.6 ± 9 years. The youngest patient was 56.8 years old, the oldest 95.3 years old. The patients had a mean BMI of 25.9 ± 4.9 kg/m2 in the range between 16 and 44 kg/m2. The distribution of ASA classification showed 26 patients (18.8%) with ASA 1 + 2, 93 patients (67.4%) with ASA 3 and 19 patients (13.8%) with ASA 4.
As only patients who had undergone surgery were included in this study, conservatively treated pelvic fractures of type FFP 1 and in some cases 2 were not included in the analysis. The distribution of fracture classification according to FFP thus showed 80 patients (58%) in group 2, 23 (16.6%) in group 3 and 35 (25.4%) in group 4.
On average, the time from patient arrival in our emergency department to the start of surgery was 127.5 ± 113.2 hours. The shortest time to surgery was 4 hours, the longest 840 hours. Patients stayed in hospital for an average of 15.7 ± 8.5 days, ranging from a minimum of 4 to a maximum of 66 days, depending on their condition and the general environment.
Before the injury, 136 patients (98.6%) were able to walk with full weight bearing, one patient with partial weight bearing and one patient in a wheelchair. In addition, 125 patients (90.6%) lived at home before the injury, 13 came to the hospital from a nursing home. At discharge, 94 patients (68.1%) were still mobile with full weight-bearing ( on their own, with crutches, a rollator or a walking frame), 42 patients (30.4%) could only partially weight-bear or had to relieve their weight, and two patients (1.4%) were dependent on a wheelchair. At the end of inpatient stay, 94 patients (68.1%) could be discharged back home, 44 patients (31.9%) had to be sent to a nursing home. Due to the pelvic injury with surgery and inpatient stay, there was a difference in condition between before and after for the variables mobilisation and place of residence. 95 patients (68.8%) regained their original mobilisation by the time of discharge, 43 patients (31.2%) remained less mobile. On discharge from inpatient stay to home or nursing home, the situation remained unchanged for 102 patients (73.9%), worsened for 36 patients (26.1%) and improved for 5 patients (2.8%).
General non-surgical complications occurred in a total of 28 patients (20.3%), while 110 patients (79.7%) had no complications during their stay.
X-Ray examinations showed no signs of screw loosening in 125 cases (90.6%) up to one year postoperatively, while 13 patients (9.4%) had a radiological suspicion.
The 1-year mortality rate was 10.1% (14 patients) according to the records and the German civil register.
The Occurrence of the Individual, Mostly Demographic, Variables in Column One is Categorised in Column Two and Listed in Column 3 and 4 in Frequency and Percentages.

The Occurrence of the Variables Listed in Column One is Shown in the Following Columns as Mean Value, Standard Deviation and Range With Minimum and Maximum Values.
The distribution of the 138 cases among the FFP classifications is shown in Figure 1, with 58% FFP 2, 16.6% FFP 3 and 25.4% FFP 4. The different FFP groups divide the pie chart into percentages. FFP 2a 10.9% blue, 2b 26.1% orange, 2c 21% grey, 3a 1.4% yellow, 3b 2.9% light blue, 3c 12.3% green, 4a 3.7% dark blue, 4b 15.9% brown and 4c 5.8% dark grey.
In order to analyse the relationship between fracture morphology and 1-year mortality, a comparative group analysis was carried out using the chi-square test shown in Figure 2. No significant differences were found between the FFP 2, 3 and 4 groups in mortality over 365 days after surgery. Kaplan-Meier diagram with the 3 curves FFP 2 blue, FFP 3 red and FFP 4 green. The Y-axis shows the cumulative survival (from 1.0 = 100% to 0.4 = 40% of the total = 138 cases) and the X-axis shows the time after surgery (in 0 to 2000 days).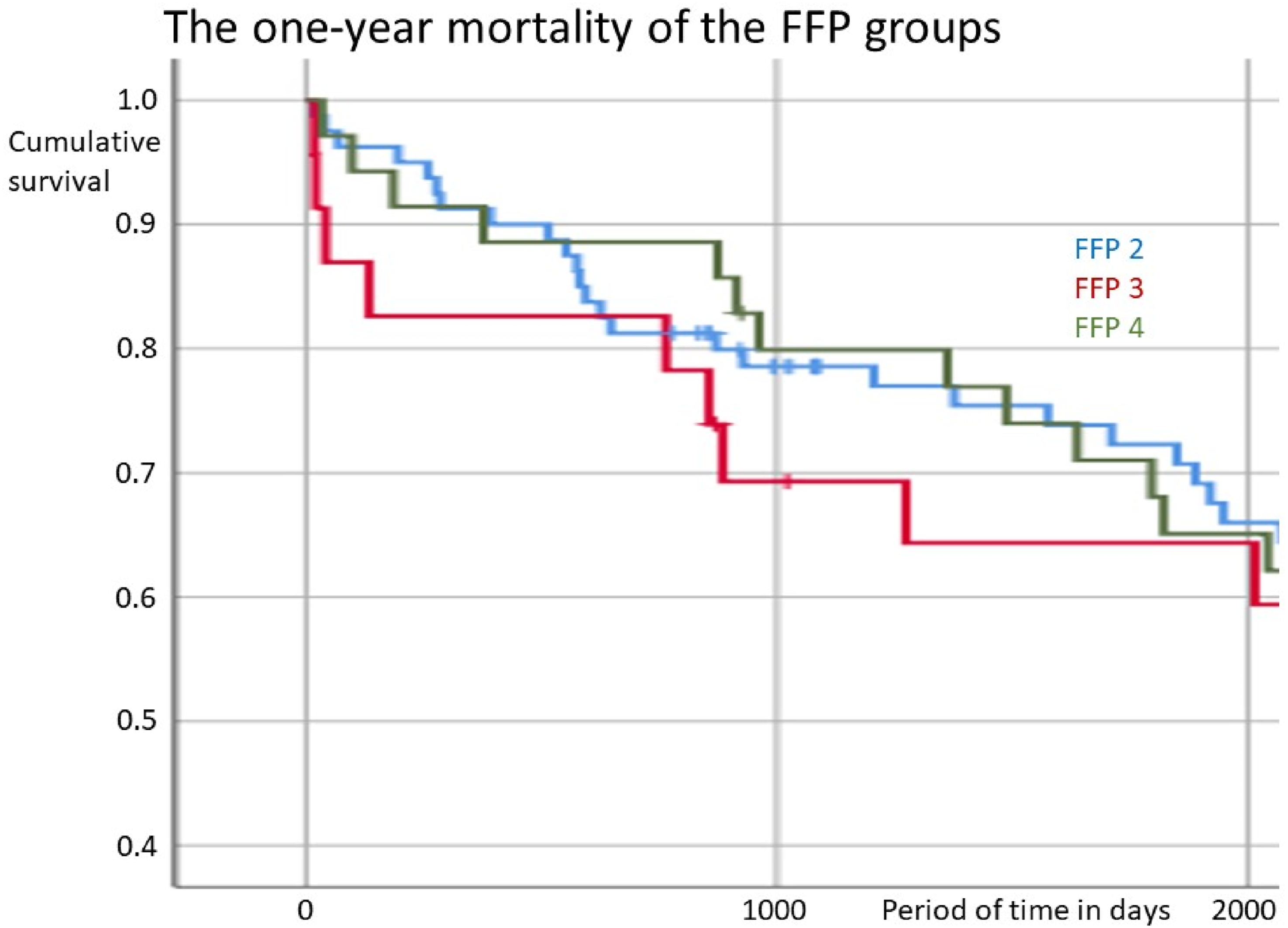
Calculations of Logistic Regression
The logistic regression for 1-year mortality was carried out with the variables screw loosening, non-surgical complications, FFP fracture classification and ASA classification. No significant effects were found.
The logistic regression for the length of the hospital stay was carried out with the variables time to surgery, non-surgical complications, ASA and FFP. The hospital stay increased significantly by 0.03 days with each hour of increase in time to surgery. Non-surgical complications significantly increased the hospital stay by 5.51 days. ASA 4 significantly prolonged the hospital stay by 4.88 days, compared with ASA 1 and 2. However, the calculations with FFP 3 (prolonged the length of hospital stay by 0.41 days) and FFP 4 (shortens it by 0.35 days) compared to FFP 2 were not significant.
Logistic regression for mobility was performed with the variables patient age, gender, ASA, FFP and time to surgery. The risk of being unable to walk with full weight bearing after surgery was significantly increased in younger patients (1.1-fold), in women (3.5-fold), in ASA 4 (8.5-fold) and in FFP 4 (3.4-fold). By contrast, no significant effect was found for the variable time to surgery.
Logistic regression for living at home was performed with ASA, FFP and time to surgery. The risk of not living at home after surgery was only significantly positive for ASA 4 patients (8.5-fold).
Discussion
The aim of this retrospective study was to investigate long-term outcomes and mortality after surgical SI / TITS stabilisation for immobilising fragility fractures of the posterior pelvic ring, as there are currently only a few clinical studies and data available on this, mostly with a small number of patients and short follow-up.18,24-27 In this regard, 138 patients who had undergone surgical treatment at our Level 1 Trauma and Geriatric Centre between 2018 and 2020 were included in the study. The complete data on 1-year mortality could be collected using the German civil register.
Due to a steadily increasing number of patients, driven by demographic change, and at the same time high demands of each individual, the health system and hospitals are facing major challenges. 2 The average age of our patients was 77.6 ± 9 years, 75.4% were female, thus showing a correlation of osteoporosis and fragility fractures in accordance with the literature, which further complicates surgical care. 1
Several studies report a poor outcome in elderly patients undergoing conservative therapy with a significant and lasting loss of autonomy. 3 In our collective, 67.4% of patients had ASA 3 and 13.8% had ASA 4, showing that they were seriously ill with corresponding borderline compensation at home. The result is a doubling of the daily support required due to a permanent restriction of mobility, 4 so that a return to domesticity is no longer achieved. 5 The BMI of 25.9 ± 4.9 kg/m2, which at first seems balanced, ranges from 16 to 44 kg/m2, from cachectic malnutrition to obese overweight.
It is crucially important for the diagnosis and treatment planning to perform a suitable cross-sectional diagnosis, preferably using dual energy / spectral CT or MRT.6-10 In our patient collective, this resulted in an FFP distribution of 58% group 2, 16.6% group 3 and 25.4% group 4, which is generally in line with the literature.11-13
With regard to the majority of FFP 2 fractures, patients were initially treated conservatively in line with the recommendations in the literature and only if pain-related immobilisation persisted surgery was indicated. Therefore, time to surgery was 127.5 ± 113.2 hours with a wide range from 4 to 840 hours. 12 The length of inpatient stay, with an average of 15.7 ± 8.5 days and range from 4 to 66 days, can also be explained by this, among other things. Regarding the choice of surgical procedure, the authors of this study decided to stabilise the posterior pelvic ring with percutaneously navigated 7.3 mm cannulated SI / TITS screws with a continuous thread, depending on the fracture type and sacral morphology.12,23
The procedure for SI / TITS screws is minimally invasive and easy to perform.18,24-27 Non-surgical complications can be reduced through a reliable postoperative improvement in complaints and rapid mobilisation. Among the 138 patients in our study, a total of 28 patients (20.3%) suffered from general complications such as pneumonia, catheter-associated infections, renal failure or cardiopulmonary problems, while 110 patients (79.7%) did not suffer from any complications during their hospital stay, despite most having severe pre-existing diseases.
The general surgical intraoperative risk, such as a possible screw malpositioning with neurovascular damage, is reported to be between 2 and 15%,29-31 as well as a symptomatic occurrence of neurological damage due to this between 0.5 and 7.7%. 31 According to the literature, screw implantation in the sacrum and ilium under fluoroscopic control is currently reported to have a risk of 31.3% for general complications and 15.6% for surgical complications, with a operative revision rate between 4.4% and 13%. 40 With regard to the comparison of percutaneous and open procedures, the current literature shows significantly better results for the more minimally invasive procedure in terms operation-related complications (19.2% vs 43.9%) and surgical revisions (13.1% vs 29.3%). 18 However, in line with the current literature, we did not see any serious malpositioning with neurological deficits or necessary surgical revision when using image-guided 3D computer navigation consistently in this study.29,32-36 The procedure of navigated SI / TITS screw insertion can therefore be considered precise and safe.
Good biomechanical data are available regarding the reliability and stability of SI / TITS screws in osteoporotic bone.23,37,38 The few clinical studies on this were mostly carried out on inhomogeneous small groups or with short follow-up periods.18,24-27 With this study of 138 patients and a follow-up period of more than a year, we support the view that the SI / TITS screw stabilisation is reliable and stable. In 125 cases (90.6%), we found no evidence of screw loosening or fracture dislocation on X-rays up to one year after surgery, while in only 13 patients (9.4%) a radiological suspicion could not be ruled out. But none of the findings were so serious that a surgical revision was necessary.
Our hypothesis in this study was that the clinical outcome of patients with fragility fractures of the posterior pelvic ring after surgical stabilisation is likely to be better than with conservative therapy:
With regard to mobility, a significant deterioration must be expected after conservative treatment, not only temporarily but permanently, with up to 40% of patients not fully recovering. 4 In our surgically treated collective, 68.8% of patients had already regained their original mobility by the time of discharge, whereas 31.2% were discharged with poorer mobility than before trauma. The risk of restricted mobility after surgery appears to be higher for younger patients, women, ASA 4 and FFP 4. However, no significant correlation could be seen for the variable time to surgery, so initial conservative treatment with analgesia and physiotherapy mobilisation seems justified for FFP2 fractures.
With a view to length of hospital stay, the authors were not surprised by the positive correlation with the variables non-surgical complications and ASA 4. However, a significant correlation with time to surgery shows that surgical stabilisation can lead to faster recovery. Regarding the comparison with surgical stabilisation, the current literature shows a high complication rate, especially with open procedures, which is why a minimally invasive procedure is recommended (significant difference in the surgical revision rate from open 29.3% to percutaneous 13.1%). 18 In our study, no surgical revision was necessary; only 20.3% showed general non-surgical complications.
It has been reported that conservative treatment can lead to a significant loss of autonomy with reduced activity levels and an increased need for support at home. 3 Long-lasting pain, regardless of age and gender, impairs mobility and is thus a cause of restrictions in everyday life. 5 In the studies mentioned, 83% of patients were living at home and 77% were independent before the fracture; after the fracture, under conservative therapy, 56% were living at home and only 33% were independent. With regard to further care, 68.1% of patients were able to live at home again after surgical stabilisation in our study. The home situation remained unchanged for as many as 73.9% of patients. The risk of no longer being able to be discharged home postoperatively was significantly increased for only ASA 4 patients. Overall, surgical stabilisation was found to be advantageous for further treatment after trauma. We also see a better postoperative result here than previously described in the literature. 18
According to the literature, the 1-year mortality rate with conservative treatment is 20%. 3 In contrast, a retrospective study of a mixed group of patients who had undergone surgery showed a 1-year mortality rate of only 9.7%, with no correlation to FFP classification or the surgical procedure used. 18 After surgical stabilisation, this rate was also only 10.1% in our study. And this is not dependent on fracture severity, screw loosening, non-surgical complications or ASA categorisation.
On the basis of this study, we support the treatment recommendations on the minimally invasive surgical stabilisation of fragility fractures of the posterior pelvic ring.11,41 Furthermore, fracture progression can possibly be prevented this way. 13
Limitations
A power analysis was not performed and the study was not designed as a controlled cohort study. Therefore, there is no internal control group. Potential confounding factors such as individual concomitant diseases, nutritional status and pre-existing mobility were not taken into account. These could have an influence on recovery and mortality rates.
Conclusion
Percutaneous navigated screw fixation of the posterior pelvic ring in fragility fractures is a simple, safe, minimally invasive and precise method with good clinical results in terms of rapid recovery with early mobilization of patients to maintain autonomy and reduce mortality.
Further clinical studies with controlled cohorts and a large number of patients with long follow-up periods should be carried out to compare the procedure with other methods. In particular, the question of an additional standardized treatment of the anterior pelvic ring in unstable dislocated fragility fractures should be investigated.
Footnotes
Acknowledgements
I would like to thank my family for their support and encouragement, day in, day out. I would like to thank Professor Gebhard, Medical Director of the Department of Trauma, Hand, Plastic and Reconstructive Surgery, Plastic Surgery Section, Ulm University, for his trust and support in my clinical and scientific work. I would like to thank Professor Schütze for our close daily collaboration and for his guidance in science and research. I would like to thank all my colleagues in my department and the staff in the operating room, on the ward, in the outpatient clinic and in the emergency room, as well as the physiotherapy team, for their work in providing the best possible care for our patients.
Ethical Statement
Consent for publication
With regard to the retrospective study design, patient consent was also not required for the publication of the anonymously processed and analysed data.
Authors’ contributions
Authors’ contributions (in accordance with the ICMJE recommendations based on the CRediT principle): Alexander Böhringer (corresponding author) – 1, 2, 3, 5, 6, 7, 8, 11, 12, 13, 14 Florian Gebhard – 8, 10, 11 Alexander Eickhoff – 2, 5, 7 Raffael Cintean – 2, 5, 7 Tobias Gruber – 2, 5, 12 Konrad Schütze – 1, 2, 3, 5, 6, 7, 10, 11, 12 Carlos Pankratz - 1, 2, 3, 5, 6, 7, 8, 11, 12, 13, 14.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All authors have decided that the data and material in this publication may be deposited in a public repository.