
Abstract
Study Design
Systematic Review.
Objectives
To detail every historical classification system of the sacrum and pelvis and their resultant integration into the encompassing AO Spine Sacral Injury Classification System.
Methods
A systematic review of MEDLINE, EMBASE and Cochrane Databases was performed in keeping with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines.
Results
49 studies were included in the systematic review. Historical systems fail to provide clinicians with a rational method of determining whether operative or non-operative management is appropriate. Fracture morphologies are presented in a non-hierarchical manner without considering crucial treatment changing factors such as degree of neurological injury or associated anterior pelvic injury. The AO Spine Sacral Injury Classification System introduces sacrum and pelvic fractures in a clinically meaningful manner ranging from the usually stable type A bony injures of the lower sacrococcygeal region, to the type B posterior pelvic injuries potentially involving the sacral foramina, and finally the type C unstable spino-pelvic injuries.
Conclusions
The sacrum and pelvis are biomechanically related structures and should be evaluated as a unified entity rather than separately as has been historically suggested. The AO Spine Sacral Injury Classification System achieves this by considering the integrity of the spino-pelvic bony as well as supporting ligamentous structures, whilst simultaneously providing a graded framework to guide whether surgical or non-surgical management is most appropriate.
Introduction
The sacrum and pelvis have traditionally been considered as distinct entities with their own separate historical classification systems. As our biomechanical understanding has increased, it has been increasingly evident that both the kyphotic keystone of the spine and its communication with the femurs should not be considered in isolation when evaluating traumatic injury. Historical rudimentary systems fail to provide clinicians with a sense of the stability and necessity for operative fixation when these injuries are observed. Furthermore, the neurological status and even weight-bearing status of patients is not conveyed in a clinically meaningful integrated manner. We performed a systematic review to reconcile these pre-existing systems and identify defining features which could strengthen a hierarchical modern universal classification.
Integration Between AO Spine Sacral and Pelvic Classification System and Existing Classification Systems
Methods
Search and Eligibility Criteria
The authors conducted a systematic electronic search of the Medline, EMBASE and Cochrane Database of Systematic Reviews from their date of inception to August 2024 was conducted in keeping with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Databases were queried with the proceeding terms combined with various Boolean operators: ‘sacr*’, ‘pelvi*’, ‘classification’, ‘system’ and ‘fracture’. Only studies examining human subjects in the language English or with available English translations were included. No registered review protocol exists for this study.
Inclusion and Exclusion Criteria
Eligible abstracts checked by two authors (B.T.S.K and J.W.T), before appropriate articles for full-text examination were scrutinized. Bibliographies of included studies were also interrogated for further eligible articles. Discrepancies were discussed until consensus attained. Inclusion criteria were defined as: (1) Any form of article, whether randomised or non-randomised controlled trials, cohort study, case series, case report or review article which proposed a new classification system defined as a method of grading fractures upon a rational basis with two or more categories (2) Any article which added a new category to an established classification system (3) Human Subjects.
Study Selection and Data Extraction
Extraction of data into a preformatted spreadsheet was performed independently by one author (B.T.S.K) and cross-checked by another (J.W.T) in accordance with the Cochrane Handbook for Systematic Reviews. 40 No authors were contacted for further unpublished data.
Appraisal and Synthesis of Results
The Risk Of Bias In Non-Randomized Studies of Interventions (ROBINS-I) tool and Murad et al instrument was applied for included non-randomized studies and case studies or case reports respectively.41,42 Study quality was independently assessed by two authors (B.T.S.K and J.W.T) with consensus attained following discussion. The ‘Robvis’ tool was utilised to generate the traffic light plot in accordance with Cochrane recommendation. 43
Results
Study Selection
The primary search retrieved 1059 articles which was filtered to 334 after duplicates were removed (Supplemental Figure 1). One-hundred-seven warranted full-text assessment for eligibility after screening was concluded. Forty-nine studies were eventually included in the systematic review. The most common for exclusion of articles after screening was failure to offer a new classification system.
Study Quality
Assessment of risk of bias of included studies was generally low as assessed by the Risk of Bias In Non-Randomised Studies (ROBINS-I) tool (Supplemental Figure 2).
Classification Systems
Forty nine articles described sacral and pelvic classification systems which we observed often were assessing injuries specifically related to either aforementinoed structure despite both being important to the symbiotic relationship between the spine and lower limbs (Table 1).
Discussion
Sacrum and Pelvis
Sacral and pelvic fractures have long been considered separately with discrete classification systems despite their inexorable link. We note 23 pelvic and 17 sacral existing classification systems have been historically described with each interrogating a particular nuance of fracture morphology. A logical means of classifying injuries to guide operative or non-operative management recognizing both the neurological status of the patient as well as biomechanical stability of the fracture itself is required. A fundamental validated classification will facilitate efficient communication between clinicians and provide the framework upon which a scoring system can be developed to guide management.
The sacrum is a wedge-shaped kyphotic structure at the base of the spine which transfers weight between spinal column and pelvis. Panjabi and White identified the sacrum as the keystone of the pelvis. 44 The incidence of sacral fractures demonstrates a bimodal peak usually occurring either in the very elderly in the setting of low energy trauma insufficiency fractures, or in the young as a consequence of high energy kinetic forces.45–49 The dynamic relationship between the sacrum to the lumbar spine as well as the pelvis has complicated biomechanical testing. 50 Stability of the sacrum and its major joints, including the sacro-iliac joint, is the product of a vast array of ligamentous structures. 51
Indeed, the sacroiliac joint is a synovial joint but Vleeming et al noted that it is both a synarthrosis and a diarthrosis given the joint is surrounded by a complex capsule and lined with cartilage.51,52 In comparison, the sacrum and ilia have a posterior articulation.51,52 The movement of the this joint is minimal and reported to be 2-3 degrees of rotation and 1-2 mm of translation. 51 Dontigny et al noted its primary function is merely to absorbed and transmit forces to the posterior pelvis. 53 An example of the variability of this is during pregnancy when hormonal changes deliberately relax the ligamentous complex to increase intra-pelvic movement for the purposes of facilitating childbirth. 51 On average, Rothkotter et al found that the ligamentous structure of the sacroiliac joint ligamentous complex could tolerate up to 3,368N with transverse loading. 54 Vukicevic et al identified the interosseous ligaments as the most crucial. 55 Harrison et al specifically commented that the movement of the sacroiliac joint was actually simultaneous rotation and translation in three dimensions.56,57 Axes of motion for SI joint are not straightforward and largely dependent upon the surface topography of joints. 58
In addition to this, stability of the sacroiliac joint is not solely dependent on ligaments. 59 Dijkstra et al studied the sacroiliac joint surfaces finding large variations but also roughened bony surface texture of the articular surfaces which themselves assist in generating friction forces to resist translation. 60 This was supported by Snijders et al who found a considerable friction coefficient of 0.4 when investigating the sacroiliac joint surfaces. 61 More than this, the sacral auricular surface is lined by hyaline cartilage that is three times as thick as the fibrocartilage that lines the iliac surface. Stability is owed as well to the thoracolumbar fascia acting as a self-bracing system and contributing to the overall stability of this region. 62 In particular, the erector spinae and multifidus muscles are the pivotal muscle groups that extendbetween the spine and the pelvis. 63 The three layers of this fascia from posterior to anterior attach respectively to the spinous processes, transverse processes and also cover the quadratus lumborum to reach the ilium and iliolumbar ligament. 64 Notably, there is no single muscle which crosses the sacroiliac joint with the purpose of muscles being to brace the joint rather than create motion. 51
An improving understanding of spine biomechanics underpins our research developing a novel spine trauma classification system for sacral and pelvic fractures. 65 We have shown that historically there have been a large number of proposed classification systems. 65 Indeed, 23 pelvic and 17 sacral grading schemes have been identified to date. However, these have all been either too detailed or too broad for daily clinical use. 65 The AO Spine Sacral Injury Classification System reflects our increasing biomechanical understanding. 65 The cadaveric research by Quan et al who loaded 10 fresh pelvic specimens in either the static or dynamic state found that low energy impact loads at 0.02-0.07 m/s2 resulted in ilium, acetabular or crista iliaca fractures similar to the Type A injuries proposed in the AO Spine Classification System. 66 Conversely, high energy impact loads at 1 m/s2 resulted in the three types of Denis fracture characterized by the B type subcategory described below. 66
AO Spine Classification
Despite the prevalence and importance of sacral and pelvic injuries, there is a notable absence of a universally accepted and validated classification system. The AO Spine Sacral Injury Classification System introduces injuries in a gradated manner across 3 main categories, each in turn subdivided into readily identifiable fracture morphology patterns. 65 It has since been validated internally and externally, and now forms the cornerstone for developing a treatment algorithm similar to the AO Spine treatment algorithms in the cervical spine and thoracolumbar spine. This sacral and pelvic classification is pioneering and unique in five novel ways.
Firstly, this AO System not only takes into consideration the morphological injury pattern itself but also the neurological status.65,67,68 Previous classification systems such as that by Medelman et al or Bonnin et al were concerned only with the radiograph that depicted the result of an impact force.25,26 Conversely, there existed injury classifications which focussed solely on the post-traumatic neurological status of the patient such as that proposed by Gibbons et al.
34
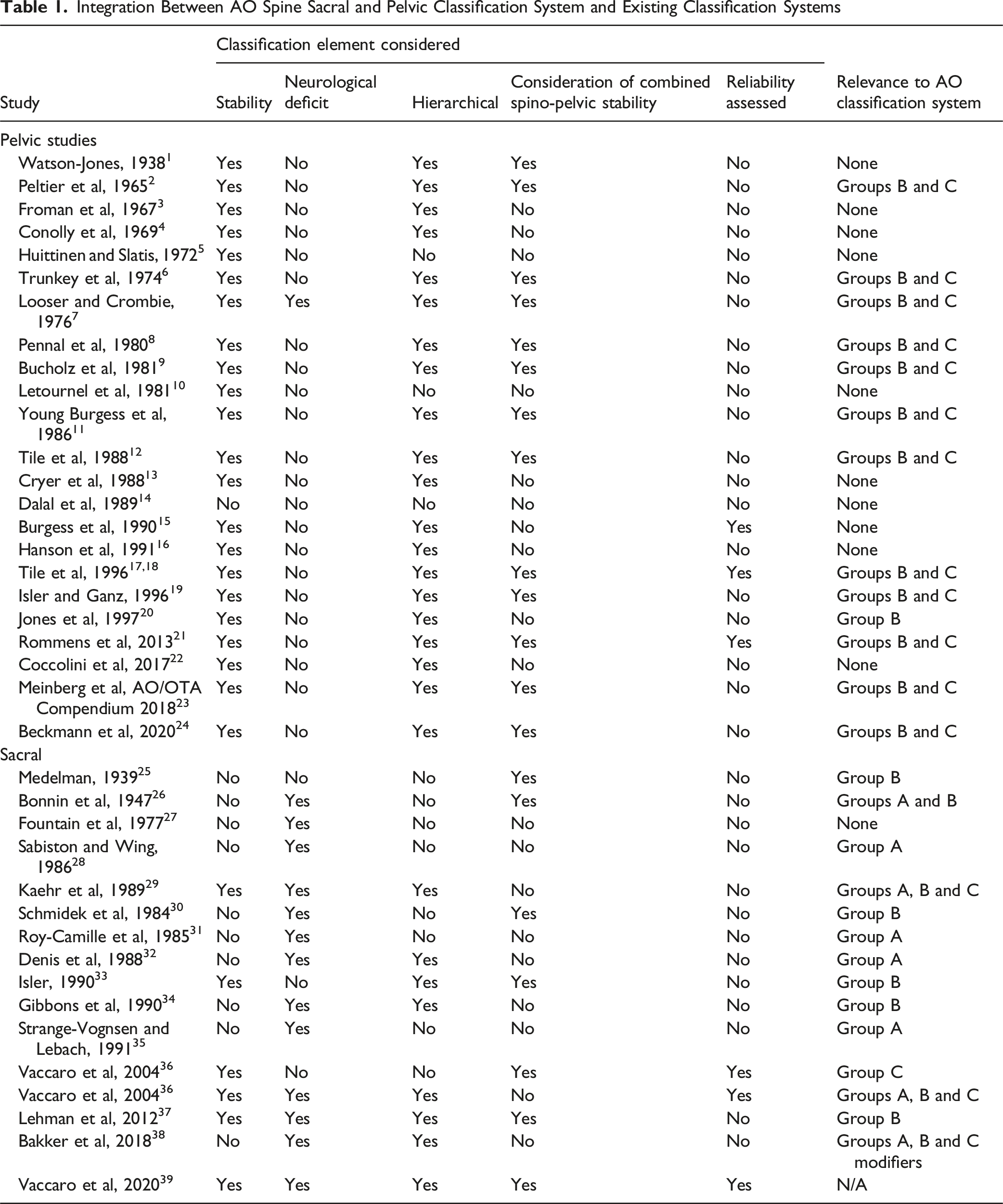
A more comprehensive and holistic system was required. The first category in the AO Spine System is Type A injuries of the lower sacrococcygeal region which in general are stable injuries given there is no impact on the stability of the spine or pelvis (Figure 1).
65
A1 injuries are defined as coccygeal compression or ligamentous avulsion injuries (Figure 1). Vukicevic et al removed the sacrotuberous and sacrospinous ligaments in 12 fresh human pelvis and demonstrated there was no influence on pelvic behaviour under physiologic loadings (50-200 N).
55
On closer inspection though, Dujardin et al proved there was some increase in micromotion of the sacroiliac joint after severing the sacrospinous and sacrotuberous ligaments even with this least unstable injury.
69
A2 and A3 injuries are non-displaced and displaced transverse sacral fractures below the sacroiliac joint respectively (Figure 1). Type A Sacral and Pelvic Injuries with the Most Benign Being A1 Subtypes Fractures Constituting Coccygeal Compression or Ligamentous Avulsion Injurie Whilst A2 Represent Non-Displaced Transverse Fractures Below the Sacroiliac Joint. The A3 Morphology Demonstrates Displaced Transverse Fractures Below the Sacroiliac Joint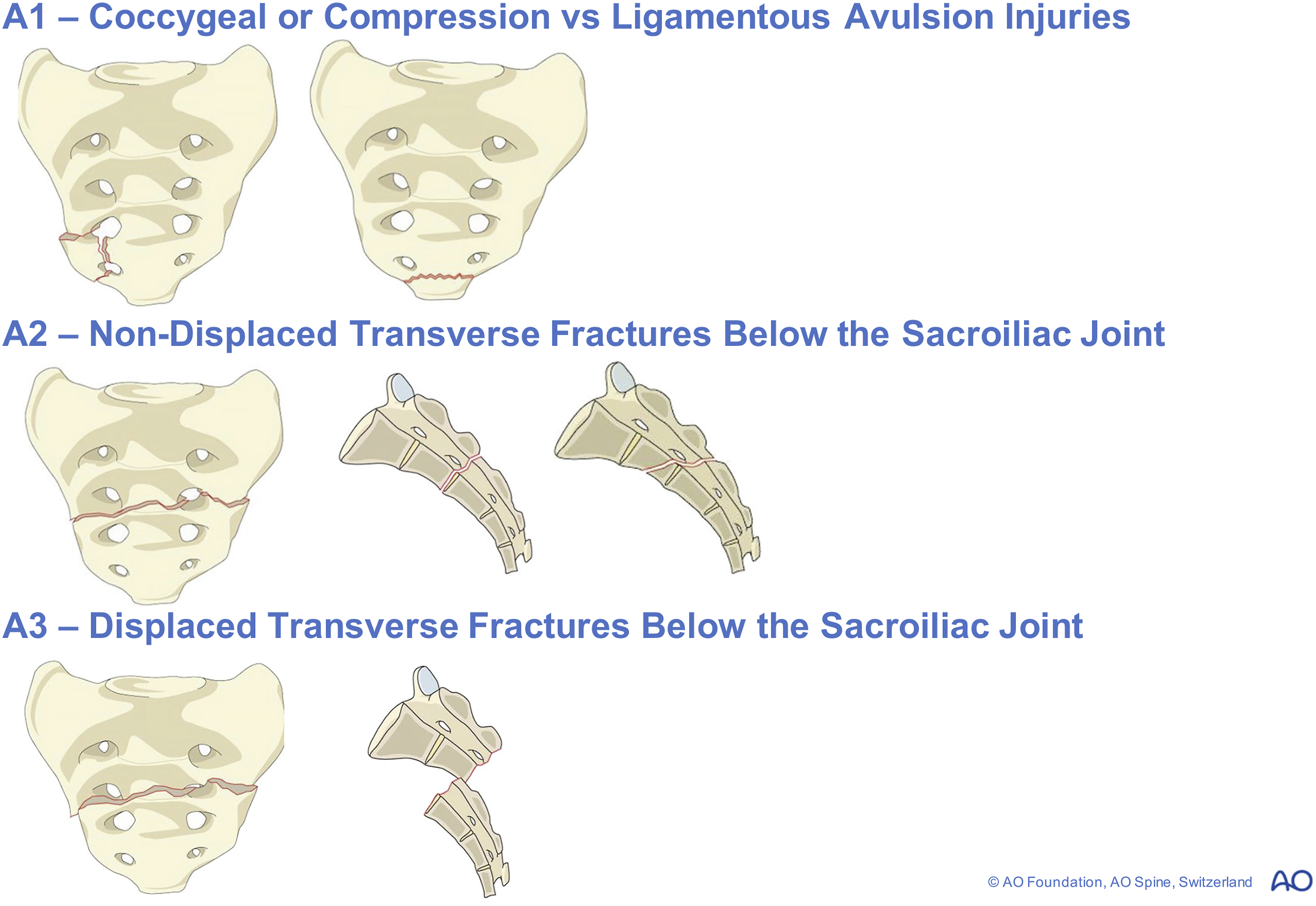
The next category in the hierarchy are the Type B injuries which disrupt the posterior pelvic complex without affecting spinopelvic stability (Figure 2). The hierarchy in this category is radical and contradicts traditional beliefs.
65
Originally, Denis et al defined three zones of the sacrum consisting of increasing rates of neurological deficit. This included the alar zone I (5.9%), foraminal zone II (34%) and central zone III (16%).
32
Our system challenges this traditional hierarchy by nominating the least severe B1 injury as actually the zone III injuries given the proposition that these are the most mechanically stable. This is followed by B2 transalar fractures which were previously Denis zone I, and finally the B3 injuries through the foraminal zone are rated as most severe. Indeed, De Peretti et al astutely identified that there were 2 sites of fixation of the nerve rootlets within the dura mater.
70
The first is the neck of the dural sheath which requires 6 kg of traction to disrupt, and the second point of fixation is as the nerve root expands passing from spinal nerve to the outer periphery of the foramen.
70
As such, transforaminal injuries which result in dislocation of bone have the potential to damage the nerve root contained within.32,70 The rationale behind this is that zone III injuries may include an entire range of injuries including undisplaced vertical fractures to the extremely ‘unstable’ U type variant which constitutes a Type C injury according to the new AO Classification.36,39,65 Type B1 Central Fractures Involve the Spinal Canal, B2 Trans-Alar Fractures Which Spare the Sacral Foramina and B3 Transforaminal Injuries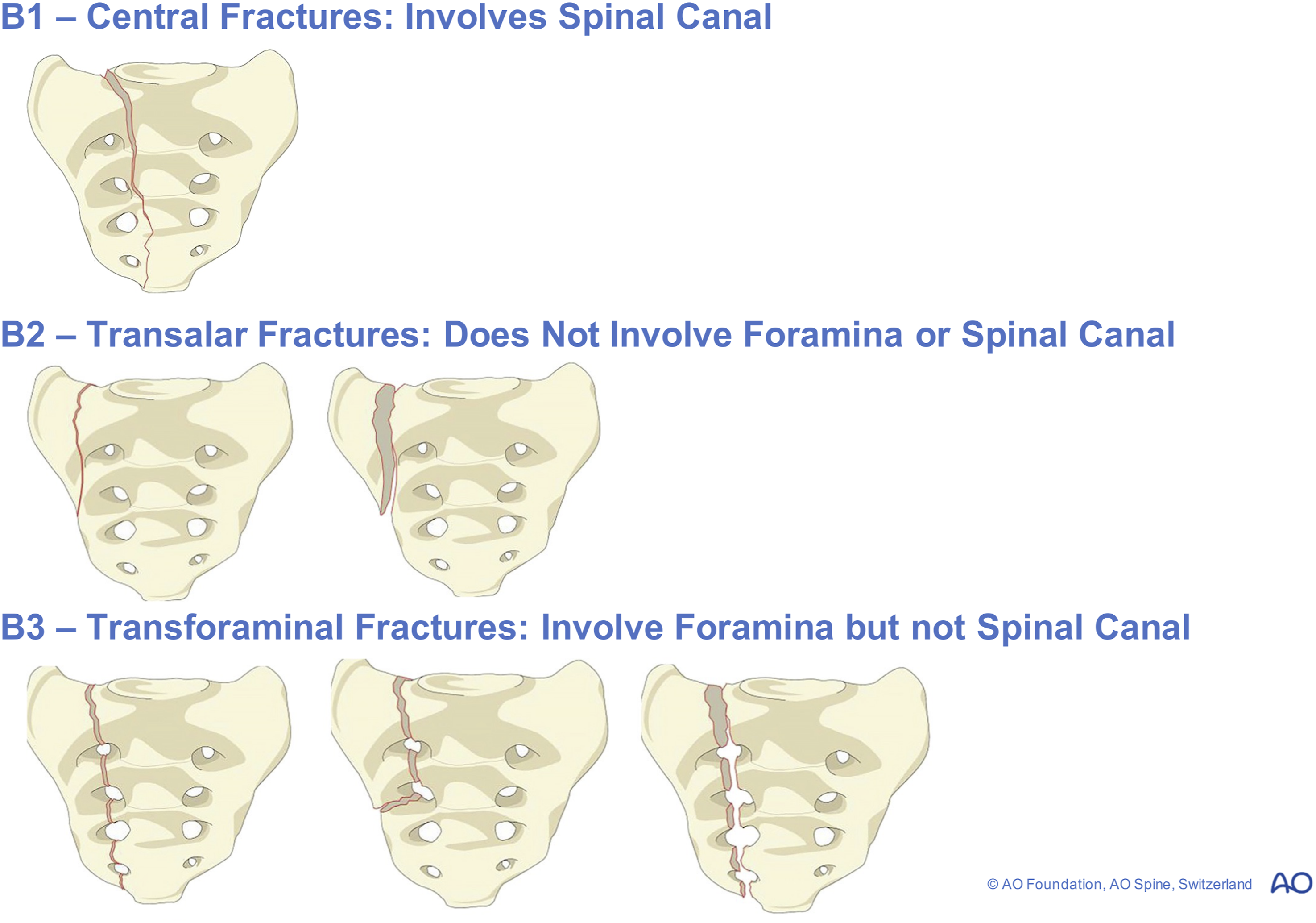
Indeed, our biomechanical understanding of this region is in keeping with rotational injuries being the most severe. Berber et al noted that pelvic reconstruction with a plate and screws improved stability with 100N loading, but still failed when rotational forces around a mediolateral axis were applied. 71 Indeed, even though this construct consists of a triangular osteosynthesis (iliosacral screws and trans-iliac bar) to distribute load, it still has a maximal displacement of 2.1 degrees around the mediolateral axis at a load of 500N. 71 Kuklo et al emphasised that achieving stability of the lumbosacral joint anterior to the rotational axis is crucial to construct rigidity. 72 This was supported by Lebwohl et al who found adding a second fixation point distal to S1 screws decreases strain.73–79 Furthermore, McCord et al examined 66 bovine spinal segments to compare different lumbosacral instrumentation techniques. 80 These authors concluded that S2 pedicle screw fixation or extending constructs to the ilium logically increases stability, and Sutterlin et al agreed with this sentiment.80–82
Type C injuries affecting spinopelvic stability occupy the most severe injury category in the AO Spine hierarchy (Figure 3).
65
Gunterberg et al showed this by vertically loading the first sacral vertebra with a force twice the physiological load in both intact and then disrupted specimens.
83
Failure occurred in the ala of the sacrum in both specimen groups consistent with the ala fracturing first in type A injuries.65,83 Importantly, resection of the sacrum at the level of S1 resulted in 50% of load-bearing capacity whereas resection between S1 and S3 resulted in 30% of loss. What this confirms is that higher sacral injuries result in greater loss of stability, which is entirely consistent with the ordering of the Type B injuries being below the level of the sacroiliac joint and the Type C injuries consisting of those above this.65,83 Type C0 Non-Displaced Sacral U Type Variant Fractures are Contrasted to the C1 Displaced Injuries. Bilateral Type B Injuries Without a Transverse Component are Exemplified by the C2 Subtype, and Finally the Most Unstable C3 Fracture Demonstrates a Displaced U Type Injury
For example, Griffin et al reported a series of 62 patients with type C vertically unstable pelvic fractures who underwent closed reduction and percutaneous iliosacral screw fixation. 84 Despite this, fixation failed in 4 patients with vertical sacral fractures, and this vertical morphology pattern was significantly associated with failure (P = 0.04). 84 Kiapour et al also noted that the flat shape of the sacroiliac joint transfers flexion/extension and compression loads more easily than shear loads, consistent with Type C injuries. 85
For this reason, the C1 subtype injury is one in which the fracture line is medial to the ipsilateral S1 facet. The C2 subtype injury is bilateral vertical fracture lines without a transverse component, whilst a C3 subtype injury adds the transverse component to form the ‘U-type’ fracture coined by Vaccaro et al39,65 Sacral injuries are often neglected given their co-occurrence with major traumatic injuries to other organ systems which cause haemodynamic compromise. However, clues to a sacral fracture should be noted. Morimoto et al observed that an L5 transverse process fracture was significantly associated with sacral injuries, and it must be recalled that the strong iliolumbar ligament attaches here. 86 It is also associated with more vertically unstable steering injuries. 87 Pool-Goudzward et al dissected 17 human cadavers and divided the sacroiliac part of the iliolumbar ligament to confirm its importance to stability, and the fact that its fibre orientation, usually in the coronal plane perpendicular to the sacroiliac joint assists in opposing rotational forces. 88
To biomechanically confirm the hierarchical nature of the AO Spine classification which is highly clinically applicable (Figure 4), Simonian et al tested 7 intact pelvic specimens and progressively disrupted them by sectioning the pubic symphysis, anterior and interosseous sacroiliac ligaments and capsule then the sacrospinous and sacrotuberous ligaments.
89
Interestingly, the iliac wings flared out under loading but the sacroiliac joint position remained unchanged.
89
However, the femurs were fixed which may have confounded these results. This is especially important given Miller et al applied pelvic loads to and measured translating motion with one leg vs both legs fixed.
90
As expected, displacements of the sacroiliac joints were small with both ilia fixed, whilst the greatest range of motion was with shear and torsional forces consistent with those which produce type B and C injuries.65,90 Vrahas et al expanded upon this by allowing the femurs to move on rollers and found that either the anterior or posterior sacroiliac ligaments must remain for stability.
91
Pure movement flexibility testing has also been performed by Flesicher et al in 6 cadaveric specimens, and it was determined that S1 screw strains were greatest in the pedicle screw group and reduced by 38% when augmented by anterior lumbar interbody fusion.92,93 AO Spine Classification Distilled into a Flowchart But Note is Made That the Degree of Neurological Injury is also Taken into Consideration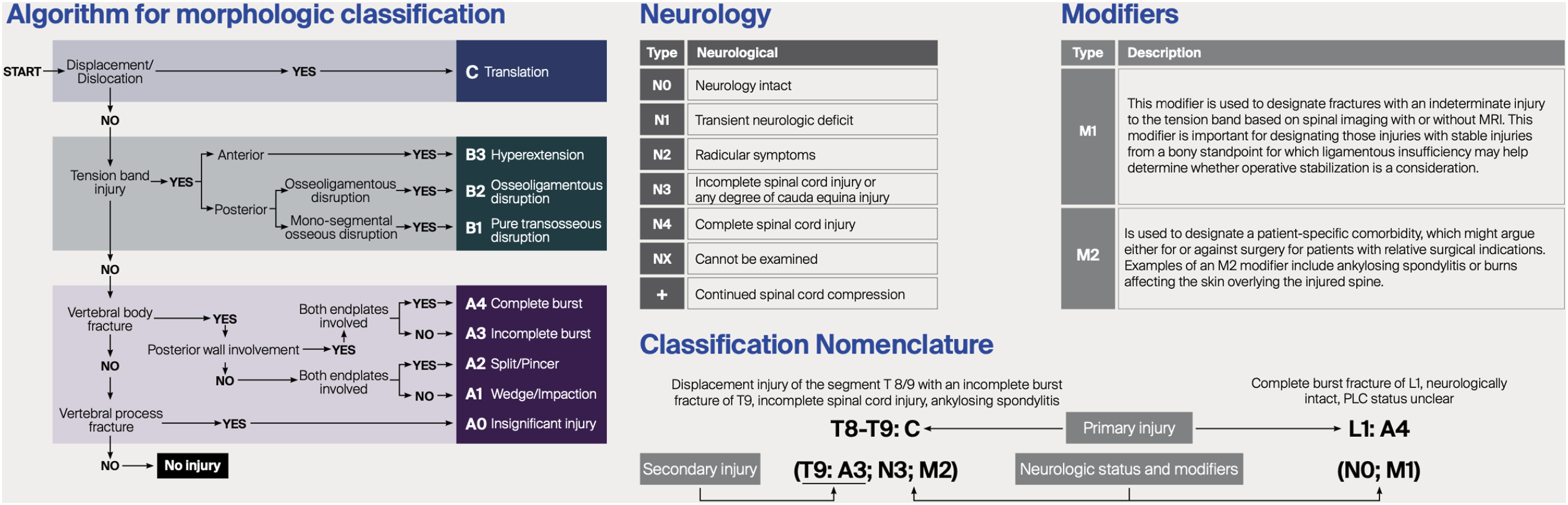
This is entirely consistent with the anterior and posterior sacroiliac ligaments being essential for stability. 92 This finding is consistent with type A1 avulsion ligamentous injuries to the sacrospinous and sacrotuberous ligaments causing micromotion of the sacroiliac joint, but any further ligamentous disruption likely resulting in clinically significant instability. What can be concluded from this is that pubic symphysis diastasis less than 25 mm means that one can infer there is likely no disruption of the sacroiliac joint. 89 If there has been disruption, then Fradet et al concurred that adding sacroiliac screws rather than sacral fixation alone resists forces of failure by 2.75 times. 94 Insufficiency fractures of the sacrum represent a unique subset. The AO System allocates them in the C0 subgroup since most of them show bilateral sacral fractures and even horizontal fractures, thereby being most in keeping with C-type injuries. In contrast to sacral fractures due to high energy trauma insufficiency fractures are less unstable but may show secondary displacement with neurological deficit. Patients with C0 injuries ultimately have a broad range of management options ranging from conservative or sacroplasty for low energy osteoporotic fractures, to trans-iliac trans-sacral fixation in the setting of high energy trauma resulting in an acute neurological deficit. 95
Clinical Applicability
The hierarchical validated of the AO Spine Sacral Injury Classification System facilitates its inherent ability to guide clinical decision making in the management of these complex patients. Indeed, Lee et al have assigned points in order to generate a quantifiable scoring system in order to recommend non-operative or operative management. 96 In this system, it is possible to integrate the type A fractures recognised historically by Denis et al and Roy-Camille et al into a group of usually stable injuries.31,32 This is proceeded by B type injuries resembling the morphologies highlighted by Medelman and Isler et al previously, with the final more unstable U type injuries of the type C categories emphasised by Vaccaro et al25,33 Each of these historical systems is not only integrated into the final synthesis of the AO Spine system, but arranged in order of biomechanical stability. Moreover, the system takes into consideration neurological status and other relevant modifiers such as specifically the presence of anterior pelvic ring injury or sacroiliac joint injury. 96
Beyond this though, the AO Spine system challenges existing ideology in many ways. For example, traditional tenets would suggest that the greatest rate of neurological injury is highest in Denis zone 3 injuries (56.7%) compared to zone 2 (28.4%) or zone 1 (5.9%) fractures. 32 This is a rational conclusion given this rate of neurological deficit correlates with greater proximity to the central canal. 97 The AO Spine is contrary to this and progresses understanding by noting whilst this may be the case that the zone 3 injuries may include unstable ‘U type’ variant injuries as Vaccaro noted and therefore be skewed. 39 As such, the transforaminal or zone 2 injuries are actually assigned the most severe category of B3 rather than central canal or B1 injuries consistent with evolving understanding of the literature. 39 Additionally, the system also is pioneering in noting that the most severe injuries of type C are true spino-pelvic injuries, and if bilateral in nature require fixation regardless of neurological status. 96
Strengths and Limitations
The novel AO Spine Sacral Injury Classification System is the culmination and progression of existing historical classification system. This is readily applicalble hierarchy and a logical means of clinicians communicating the severity of fractures with its attendant likelihood of requiring operative intervention. Future iterations of this classification should focus on guiding clinicians on specific surgical strategies, such as whether a short or long construction of fixation is indicated. However, it is reasonable to deduce that type B injuries usually require repair of the often vertically orientated sacral fracture line, whilst type C injuries usually require spino-pelvic support. Future research should focus on developing an objective validated scoring system.
Conclusions
The AO Spine Sacral Injury Classification System is a validated means of synthesizing and recognizing that injuries in this complex anatomical region should be considered as intertwined rather than separate entities. The logical 3 categories of type A, type B and type C are further subdivided in a fashion of escalating severity for ease of timely recognition by clinicians to guide treatment decisions. Trans-foraminal injuries or Denis zone 2 injuries are acknowledged as the most severe injury being designated type B3 which is contrary to traditional tenets of belief. Furthermore, the unstable ‘U’ type variant is discretely acknowledged as a type C injury rather than being potentially misclassified as a type B Denis zone 3 injury.
Supplemental Material
Supplemental Material - Sacral and Pelvic Fractures: Historical Systems and Advancements with the AO Spine Classification
Supplemental Material for Sacral and Pelvic Fractures: Historical Systems and Advancements with the AO Spine Classification by Barry Ting Sheen Kweh, MBBS (Honours), Alexander R. Vaccaro, MD, PhD, MBA, Gregory Schroeder, MD, Jose A. Canseco, MD, PhD, Maximilian Reinhold, MD, Mohamed Aly, MD, PhD, MRCS, Sebastian Bigdon, Mohammad El-Skarkawi, MD, PhD, Richard J. Bransford, MD, Andrei Fernandes Joaquim, MD, PhD, Harvinder Singh Chhabra, MBBS, MS (ORTHO), Emiliano Vialle, MD, Rishi M. Kanna, MS, MRCS, FNB, Charlotte Dandurand, MD, MSc, FRCSC, Cumhur Öner, and Jin Wee Tee, BMedSci, MBBS, MD, FRACS in Global Spine Journal
Footnotes
Acknowledgements
This study was organized and funded by AO Spine through the AO Spine Knowledge Forum Trauma, a focused group of international Trauma experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Study support was provided directly through AO Network Clinical Research.
ORCID iDs
Ethical Considerations
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AO Spine, AO Network Clinical Research through the AO Spine Knowledge Forum Trauma.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.