
Abstract
Objective
The purpose of this study is to present a surgical technique that simultaneously reduces and fixates the transverse parts of U-shaped sacral fractures.
Methods
The sacral fracture was exposed through a posterior median approach. In a flexion injury, the rotation of the lower sacral segment is reduced by distraction along a pre-curved rod. Then, lordotic restoration is performed with a Weber clamp placed at the lower sacral segment through dragging. In an extension injury, longitudinal distraction is performed along the spinopelvic rod to reduce the vertical displacement. Next, the transverse displacement is reduced by a dissector placed between the upper and lower sacral segments through levering. The sagittal reduction on the lateral pelvic view was judged by PI. A regression analysis of Oswestry disability index (ODI) with Z-scores of PI, lumbar lordosis (LL), sacral slope (SS), and pelvic tilt (PT) was performed.
Results
At the 1-year follow-up, the average PI, LL, SS, and PT values were 51.6 (range: 43.1–76.0), 44.8 (34.6 – 60.1), 35.4 (18.1 – 48.0), and 16.7 (2.2–35.4) degrees, respectively. All patients were able to maintain an upright stance. The average ODI was 27.6% (2–72%). Surprisingly, the regression analysis demonstrated a significant linear relationship between ODI and LL (R2 = 0.367, p = .048) but not between ODI and PI (R2 = 0.227, p = .138).
Conclusions
Using PI as guidance, the surgical procedures were helpful to reduce the PI of transverse sacral fractures into the normal range. However, the relationship between PI and the prognosis remains to be evaluated by future researches.
Introduction
U-shaped sacral fractures usually occur because of high energy trauma. In these fractures, approximately 45% will traverse the sacrum. 1 Because the kyphosis or lordosis of transverse parts of U-shaped sacral fractures, lower motor deficits and bowel and bladder dysfunction are common complications. In the past, the patients with U-shaped sacral fractures were usually treated conservatively because of polytrauma, but recent research suggests that patients treated surgically have better spinopelvic stability and neurological status. 2
Even though surgical treatment benefits many patients with transverse sacral fracture, the management of this kind of fracture was controversial and the reduction was often poor. Fortunately, the development of surgical implantation systems has facilitated management of these fractures, and therefore, satisfying reduction, stable fixation, and early mobilization have been possible. However, the published reports offered few reduction techniques, which are the hardest part in the management of transverse sacral fractures.
A U-shaped sacral fracture involves bilateral vertical fractures in conjunction with a transverse fracture, resulting in separation of the spine from the pelvis. The distal sacral fragment (connected to pelvis) either rotates in extension or flexion relative to the upper sacral fragment (connected to spine) because of the injury mechanism (Figure 1(a) and (b)), and this rotation creates lumbosacral kyphosis or lordosis.3,4 Because the U-shaped sacral fracture pattern is often caused by axial compression and extension forces, published methods usually include flexion and distraction using bolsters and spinopelvic pedicle screws. However, the reduction of transverse sacral fracture is often unsatisfactory.
3
The mechanisms of flexion and extension injuries. In a flexion injury, the lower sacral fragment is rotate in flexion relative to the lumbar spine, which creates a kyphosis across the fracture site (a). In an extension injury, the lower sacral fragment is rotate in extension relative to the lumbar spine, which creates a lordosis across the fracture site and the displacement can be increased by the contractive forces of the psoas muscles (b).
The critical first step towards an optimal reduction method requires a clear and accurate definition of radiographic measurements. 5 Unfortunately, the specific radiographic measurements that aid the surgeon in reduction and prognosis assessment are rare. The traumatic spinopelvic dissociation leads to PI alternation, resulting in a sagittal imbalance of the spine. PI has been shown to be correlated with both the adequacy of surgical reduction and the risk of high-grade spondylolisthesis progression. 6 Using PI as an intraoperative guide, we intended to introduce a standard procedure to reduce and stabilize the fracture, allowing for earlier mobilization and to assess whether PI affects the prognosis of transverse sacral fractures.
Patients and methods
From June 2016 to October 2019, a total of 27 patients with U-shaped sacral fractures were diagnosed at our trauma centre. From these, patients, those with non-operative treatment (n = 2), modified Roy-Camille classification type I, which precludes transverse reduction (n = 1), spinal fractures that may affect the spinal posture (n = 9), insufficient duration of follow-up (n = 3) and those who have incomplete data documentation (n = 1) were excluded. Thus, 11 patients remained in the study. Written informed consent was obtained from all participants and was approved by the institutional review board of our institution.
Patient demographics and injury characteristics.
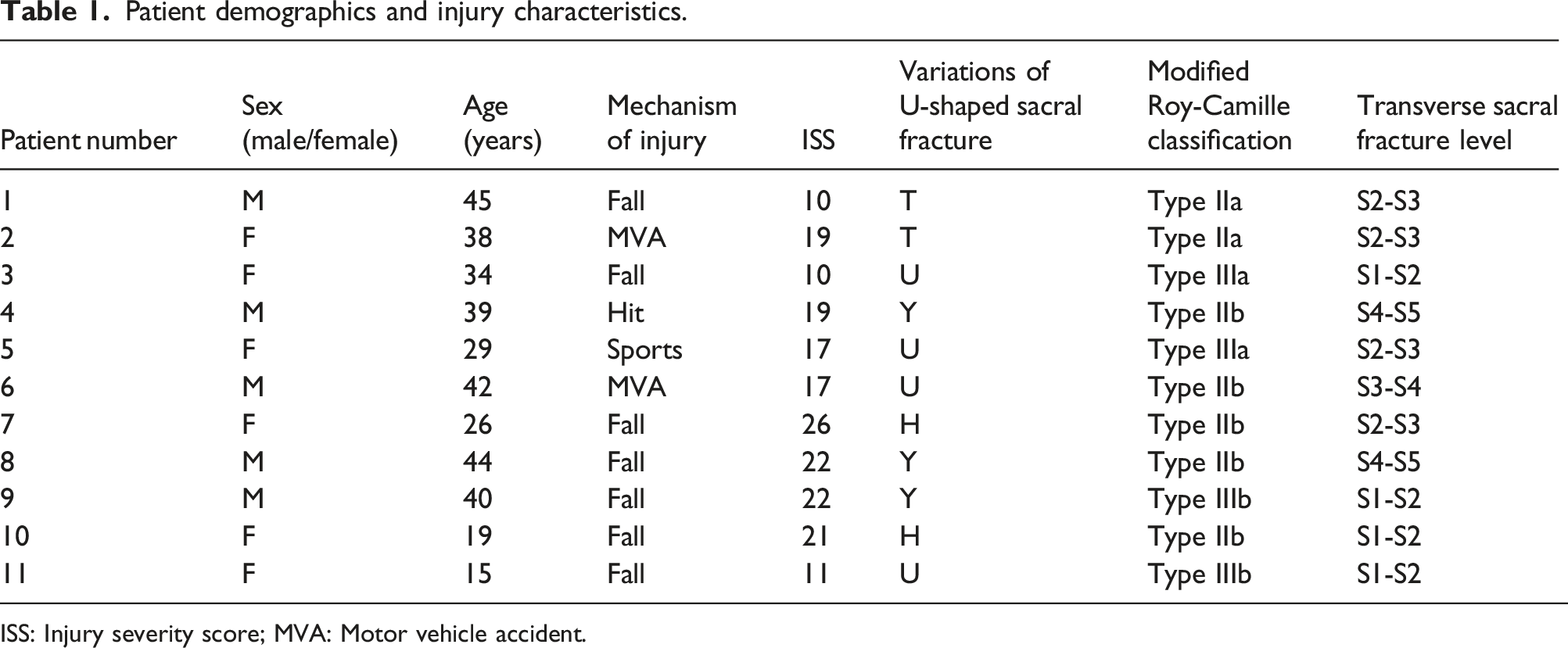
ISS: Injury severity score; MVA: Motor vehicle accident.
Surgical management
The patient is positioned on a radiolucent operating table permitting unobstructed fluoroscopic visualization for the AP, inlet, outlet and lateral radiographic projections. The key in reducing a transversely displaced sacrum is to first decompress the sacral plexus to ensure that the sacral nerve roots maintain a loose status during reduction. Then, the displacement is reduced according to the injury mechanism. PI was used as guidance of transverse parts reduction of U-shaped sacral fractures.
With the patient in the prone position, a median skin incision is performed from L4 to S3. The lumbodorsal fascia is dissected close to its origin at the medial sacral crest and the L4 and L5 spinal processes if necessary. The transverse fibres of the gluteus maximus are mobilized from medial to lateral. Then, the paraspinal muscle is dissected distally, allowing the paraspinal muscle mass to be superiorly reflected to expose the entire sacrum, including the sacral foramina and fracture line. The soft tissues must be kept moist during the remainder of the procedure. At this stage, sacral decompression was performed through a laminectomy and a clearance of fracture fragments, the nerve roots should be isolated and decompressed to their foraminal exit. In some cases, in order to sufficiently release the cauda equina and S1-S4 nerve roots, a sacral osteotomy of the kyphotic upper sacrum is carried out. Next, the reduction procedures are different in a flexion injury versus an extension injury.
In a flexion injury, pedicle screws (6.5 mm diameter and 40–45 mm in length) are implanted into the pedicle to the anterior third of the vertebral body of L4 and L5 on the lateral view. The pedicles of L5 and L4 are directed medially approximately 25 degrees or more, with the starting point lateral to the facet joint.
9
Then, two iliac screws (7 or 8 mm diameter and 70–90 mm in length) are inserted in the ilium from the posterior superior iliac spine (PSIS) to the anterior inferior iliac spine and parallel to the sacroiliac joint (Figure 2(a)). The entry point on PSIS for the iliac screw is incised by 1.5 cm*1.5 cm to avoid postoperative irritation of the subcutaneous tissues. The safe placement of iliac screws can be verified by a lateral pelvic view with a precise overlap of the sciatic notches, an obturator inlet view showing the inner and outer tables of the ilium, and the guidance of digital palpation.
10
Pre-curved longitudinal rods were placed into the L4 and L5 polyaxial pedicle screws and secured with tightened nuts. With the two screws in the ilium not yet tightened. Longitudinal reduction is performed by inserting two distraction forceps between the L5 pedicle screws and the closed multiaxial screw (CMAS) (WEGO, Inc, Shandong, China) (Supplementary File), thereby reducing the impaction between the upper and lower sacral segments (Figure 2(b)). Because the distraction is along the pre-curved longitudinal rods, this action can also reduce the rotation of the lower sacral segment through a hyper-extension manner. Then, lordotic restoration is performed with a Weber clamp placed at the lower sacral segment through dragging. In some cases, raising the lower extremities might benefit reduction of kyphotic displacement. If there is a sagittal gap in the sacrum, it can be closed by a reduction clamp between the locked CMAS and the iliac screw. After confirmation of the reduction on the AP and lateral pelvic view, the spinopelvic rod is locked with the CMAS and a connecting rod is applied (Figure 2(d)). The decompression, reduction, and fixation of a flexion injury. After sacral decompression, L4/5 pedicle and iliac screws were inserted (a). Longitudinal distraction along a pre-curved rod was performed between the locked L5 pedicle screws and the iliac screw (b). Then, the transverse displacement is reduced by a Weber clamp placed at the lower sacral segment through dragging, combined with lifting of the lower sacral segment if necessary (c). The reduction is completed, the spinopelvic rod is locked with the CMAS and a connecting rod is applied (d). The green tap indicates the rod is free to slide across the tap and the red tap indicates the opposite.
In an extension injury, two pedicle screws are implanted into the vertebral body of L4 since the pedicles of L5 are not accessible at this stage. After iliac screws are inserted and the spinopelvic rod is locked with the L4 screws, longitudinal distraction is performed along the spinopelvic rod, thereby reducing the vertical displacement between the upper and lower sacral segments (Figure 3(a)). This action can also partially reduce the rotation of the lower sacral segment and expose the L5 pedicles. Next, the L5 pedicle screws are placed and further longitudinal distraction is carried out (Figure 3(b)). Elevation of the joystick on the L5 pedicle screw can further reduce the posterior displacement of the hemipelvis. Then, the transverse displacement is reduced by a dissector placed between the upper and lower sacral segments through levering (Figure 2(c)). After confirmation of the reduction on the AP and lateral pelvic view, the spinopelvic rod is locked with the CMAS and a connecting rod is applied (Figure 3(d)). The decompression, reduction, and fixation of an extension injury. After sacral decompression, L4 pedicle and iliac screws were inserted. Longitudinal distraction was performed between the locked L4 pedicle screws and the iliac screws (a). Then, the L5 pedicle screws were inserted and longitudinal distraction was performed between the locked L5 pedicle screws and the iliac screws (b). Transverse displacement is reduced by a dissector placed between the upper and lower sacral segments through levering (c). The reduction is completed, the spinopelvic rod is locked with the CMAS and a connecting rod is applied (d). The green tap indicates the rod is free to slide across the tap and the red tap indicates the opposite.
Statistical analysis
GraphPad PRISM 5 (GraphPad Software, Inc., La Jolla, CA) was used for statistical analyses. Z-scores of PI, LL, SS, and PT were calculated using norm-based scores for the asymptomatic volunteers. 11 Correlation analysis between ODI and Z-scores of PI, LL, SS, and PT was performed. A p value of less than 0.05 was considered to indicate significance.
Results
Surgery details and main outcome measurements.

PI: Pelvic incidence; LL: Lumbar lordosis; SS: Sacral slope; PI: pelvic tilt; ODI: Oswestry disability index; ASIA: American spinal injury association; FU: 1-year follow-up; LPF: Lumbopelvic fixation; TOS: Triangular osteosynthesis.
Flexion injury case
A 19-year-old female fell from a six meters height. Preoperative three-dimensional CT reconstruction on three-view showed a modified Roy-Camille type IIb sacral fracture and an H-shaped pelvic fracture (Figure 4(a)–(c)). Before reduction, a sacral decompression was performed, and implants had been inserted (Figure 4(d)). Then, the transverse displacement was reduced by a Weber clamp placed at the lower sacral segment by dragging (Figure 4(e) and (f)). The postoperative radiographs showed that the deformity was reduced (Figure 4(g)–(i)). At the 1-year follow-up, the PI, LL, SS, and PT values were 43.4, 39.6, 28.2, and 15.2 degrees, respectively. Before surgery, the patient had paralysis of the lower extremities. At the 1-year follow-up, she was able to maintain an upright stance but depended on crutches when walking. A 19-year-old female fell from a particular height. Preoperative three-dimensional CT reconstruction on lateral (a), anterior (b), and posterior (c) view acquired at the time of injury showing a modified Roy-Camille type IIb sacral fracture and an H-shaped pelvic fracture. Before reduction, the sacralplexus was exposed through a sacral decompression (d). The transverse displacement is reduced by a Weber clamp placed at the lower sacral segment through dragging (e-f). The postoperative radiographs showed that the deformity was reduced (g–i).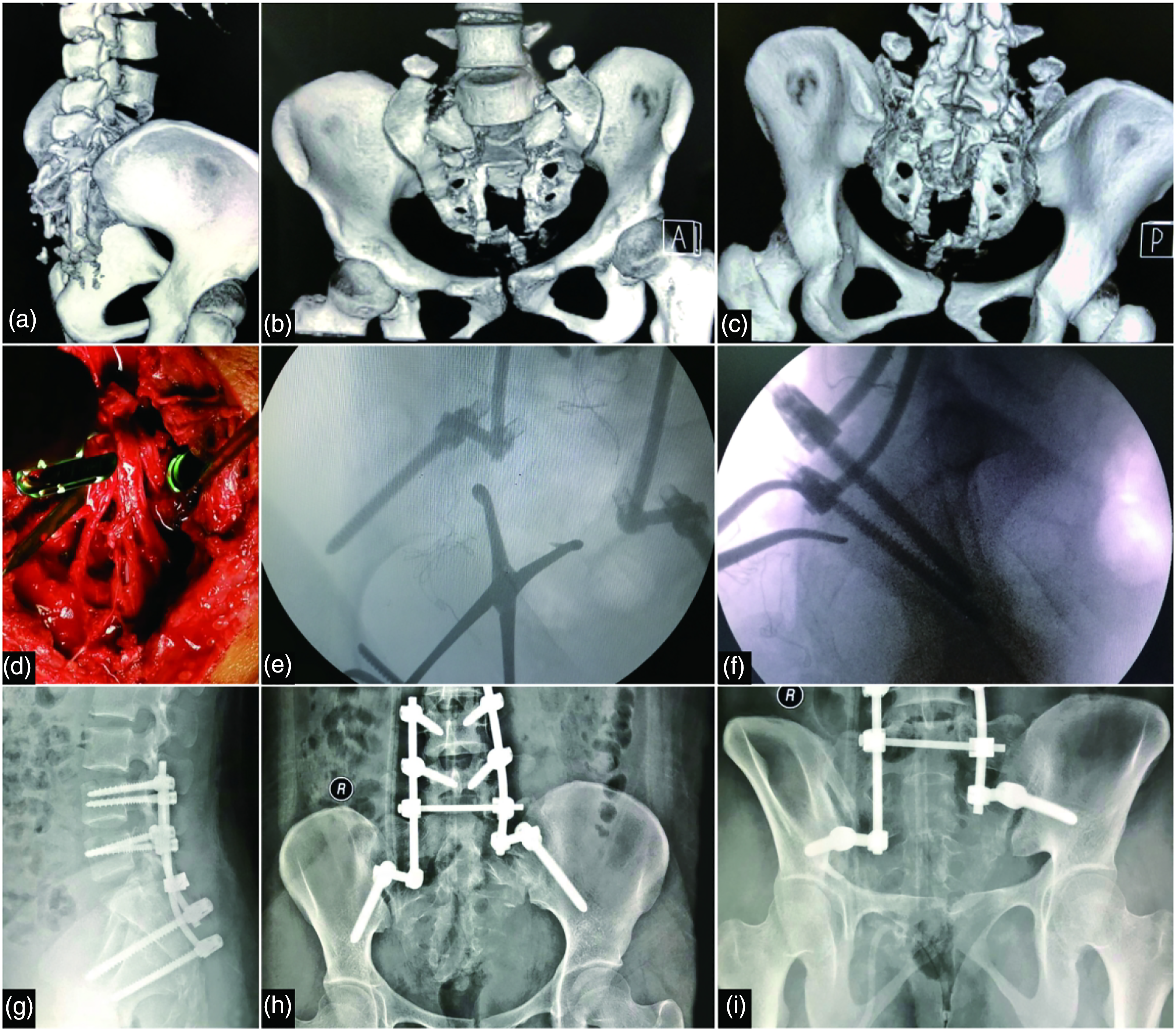
Extension injury case
A 40-year-old male fell from a particular height. Preoperative radiographs showed a modified Roy-Camille type IIIb sacral fracture and a U-shaped pelvic fracture (Figure 5(a)–(c)). The transverse displacement was reduced by a dissector placed between the upper and lower sacral segments through levering (Figure 5(d)). The postoperative radiographs showed that the displacement was reduced (Figure 5(e) and (f)). At the 1-year follow-up, the PI, LL, SS, and PT values were 45.9, 46.6, 29.9, and 16.0 degrees, respectively. The patient walked normally but was suffering from minor pain with persistent walking. He could manage the pain with oral celecoxib. A 40-year-old male fell from a particular height. Preoperative CT on the lateral view (a) showinga modified Roy-Camille type IIIb fracture. Preoperative three-dimensional reconstruction on anterior (b) and posterior (c) view showing a Y-shaped pelvic fracture. The transverse displacement is reduced by a dissector placed between the upper and lower sacral segments through levering (d). The postoperative radiographs showed that the displacement was reduced (e and f).
Discussion
Because a U-shaped sacral fracture is created by axial compression forces, published methods usually include flexion and distraction using bolsters and spinopelvic pedicle screws. However, the reduction is often unsatisfactory. 3 To date, the understanding of the displacement of transverse sacral fractures to a great extent has been limited to extension and flexion; however, the rotation of the lower segment of sacral fracture may be responsible for the unsatisfying reduction. In an extension injury, in addition to kyphosis across the fracture site, the lower sacral fragment is free to rotate in extension relative to the lumbar spine, which may be increased by the contractive forces of the psoas muscles. 6 In a flexion injury, in addition to lordosis across the fracture site, the lower sacral fragment is free to rotate in flexion relative to the lumbar spine. How to reverse the rotation of the sacral segments corresponding to the injury mechanism in the reduction process becomes critical. In our surgical procedures, the reverse rotation in flexion injury is provided by distraction along a pre-curved rod combined with a Weber clamp placed at the lower sacral segment through dragging, the reverse rotation in extension injury is reduced by longitudinal distraction combined with a dissector placed between the upper and lower sacral segments through levering.
Evaluating the rotation of the pelvis during the operation is another challenge. PI is a radiographic parameter of spinopelvic morphology and orientation; it controls the balance between the spine and pelvis and correlates with the adequacy of sagittal plane reduction. 6 Importantly, PI remains a constant value for each individual after adolescence. 12 The pathological process can change the shape of the sacrum and acetabulum, thereby altering the position of the acetabula within the pelvis. We used PI as intraoperative guidance for sagittal plane reduction. The referenced normative data for the PI is 55 ± 10.6 degree 11 Although there are many studies that have reported clinical and radiological outcomes in patients with U-shaped sacral fractures, the association of PI and the prognosis of transverse sacral fracture have not been reported. The authors hypothesize that a relatively ‘normal’ PI may benefit the patient regarding physiological activity and bodily pain. Surprisingly, the regression analysis did not demonstrate a significant linear relationship between ODI and PI. However, because of the limitations of this study, the relationship of PI and the patient outcome remains to be judged by a larger case series and longer period of follow-up data, which is the focus of our future research.
For transverse sacral fracture patients, operative reduction, and sacral decompression is beneficial for the recovery of the cauda equina injuries. 13 It seems that patients achieving better functional recovery are those who were treated surgically, and the sacral plexus was found to be compressed but largely intact. 2 Our intraoperative findings also confirmed the conclusion. The patients with sacral roots having been compressed but intact were found to have only mild dysfunction (ODI < 20%) at 1-year follow-up. In addition, it has been found that nearly one-half of the displaced transverse sacral fracture patients had delayed neurological abnormalities, despite that they had a normal initial examination. 14 Therefore, we recommend sacral decompression in patients with modified Roy-Camille classification type IIb, IIIb, and IV fractures or those who present neurological deficits. Routinely, a sacral decompression is performed to expose all involved sacral roots before manual reduction, to ensure that the sacral nerve roots maintain a loose status during reduction. Intraoperative SSEP (somatosensory evoked potential) monitoring provides useful assistance to avoid iatrogenic neural damage. 15
Patients with U-shaped sacral fractures are usually polytraumatized, concomitant injuries preclude early fracture surgery, and the hard callus, and soft tissue contracture is probably very strong to resist reduction. An operation that permits immediate weight-bearing may reduce mortality and improve the quality of life in these patients. 7 Therefore, an ideal surgical technique involving reduction is conducted through internal fixation, and the reduction is simultaneously supported by internal fixation. The key element in the surgical procedure is the presence of CMAS, which simultaneously offers the possibility of rotation around and slide along the spinopelvic rod, thereby omitting complex 3-dimensional rod contouring and facilitate the reduction and fixation procedure.
Limitations
U-shaped sacral fractures are rare. Besides, because of the retrospective design, the complete data of all patients could not be acquired, which leads to a relatively small number of cases. Therefore, selection bias may be influential. Another limitation is that the contribution of the reduction method to the radiographic parameters may be difficult to interpret because the acquisition of preoperative PI was not practical because of the pelvic fracture and associated injuries.
Conclusion
The key towards a satisfying reduction includes two aspects: one aspect is to ensure that the sacral nerve roots maintain a loose status during reduction, and the other aspect is the direction of reduction force should encounter the direction of initial injury force. Because the direction and rotation of the fracture segments on the sagittal plane are difficult to estimate intraoperatively, PI provides significant assistance to restore the proper sagittal alignment of the lumbosacral spine and the pelvis. Reducing the PI within or close to the normative range for these fractures demonstrates that the anatomic sagittal balance between the spine and pelvis has been restored. However, this study failed to demonstrate the benefits of PI-guided reduction, and the relationship between PI and the patient outcome remains to be judged by a larger case series and longer period of follow-up data.
Supplemental Material
Supplemental Material - Pelvic incidence-guided reduction in transverse parts of U-shaped sacral fractures: Technical recommendations
Supplemental Material for Pelvic incidence-guided reduction in transverse parts of U-shaped sacral fractures: Technical recommendations by Li He, Song Gong, Tianyu Li, Meiqi Gu, Zhe Xu, Hua Chen and Chengla Yi in Journal of Orthopaedic Surgery
Supplemental Material
Supplemental Material - Pelvic incidence-guided reduction in transverse parts of U-shaped sacral fractures: Technical recommendations
Supplemental Material for Pelvic incidence-guided reduction in transverse parts of U-shaped sacral fractures: Technical recommendations by Li He, Song Gong, Tianyu Li, Meiqi Gu, Zhe Xu, Hua Chen and Chengla Yi in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
The authors gratefully acknowledge WanRong Lu (Cancer Biology Research Center (Key Laboratory of the Ministry of Education), Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China for her assistance with statistical analysis.
Author contributions
LH, HC, and CY conceived of the study. LH, SG, TL, MG, and ZX participated in the study design and data collection. LH and TL performed data management. LH performed the statistical analysis. All authors drafted and revised the manuscript. All authors had read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The original study protocol was approved by the local Ethics Committee. Because of the retrospective and observational nature of the study, the local Ethics Committee agreed to exempt written informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.