
Abstract
Background
Hallux valgus is a common yet complex foot deformity involving the first ray. Characterised by medial deviation of the first metatarsal, lateral deviation and pronation of the great toe. 1 Moderate to severe cases often require surgical intervention to correct the deformity and restore proper alignment and function of the first ray. 1 The underlying aetiology is multifactorial, being a culmination of intrinsic and extrinsic factors. The first ray is dependent on both static and dynamic stabilisers to maintain acceptable alignments. 2 An imbalance in these stabilisers, the intrinsic, extrinsic foot muscles and the ligamentous structure will lead to such deformities. 3 Intrinsic factors range from patients with genetic predisposition, 4 ligamentous laxity, or natural anatomical variance that results in such malalignments involving, for example, the distal metaphyseal articular angle (DMAA), and hypermobility of the first ray. Poorly fitted foot wear, especially those with a narrower toe box may also play a role.1,2
One review estimated that the global prevalence was up to 23% between the ages of 18 and 65, and up to 35% above the age of 65. 3 Within the Asian population, the prevalence was quoted to be 21.96%, and a higher prevalence was found in women and among those above the age of 60. 5 A study based on the oriental Chinese population in Hong Kong published in 2017, indicated that hallux valgus deformities would gradually progress over time, emphasising the importance of shortening waiting times for timely surgical intervention. 6 Hallux valgus is a significant concern within the Chinese population, with a notable prevalence and tendency for progression if not addressed early.
In mild cases, patients may opt for nonsurgical intervention. Although some studies have shown good results in reduction of foot pain via the use of foot orthoses, night splints, and physiotherapy, the evidence for deformity correction and prevention of progression is less promising. 7 As the condition tends to worsen with time, in active, symptomatic patients that are fit for surgery: a surgical intervention may be the more effective option.
Currently there is an abundance of ways to go about surgically correcting a hallux valgus deformity, ranging from soft tissue procedures to bone procedures such as osteotomies, resection arthroplasties, to arthrodesis. 8
Two commonly performed procedures at our centre are the Modified McBride's procedure with Ludloff osteotomy and the minimally invasive Chevron Akin (MICA) osteotomy.9,10 The Ludloff osteotomy involves a linear oblique osteotomy of the first metatarsal shaft with lateral rotation and translation of the distal fragment. 11 This realigns the first metatarsal and first metatarsal–phalangeal joint, correcting the hallux valgus deformity. The Ludloff osteotomy is usually indicated for moderate to severe cases of deformities, especially when associated with greater intermetatarsal angles (IMA). 11 The MICA osteotomy is a minimally invasive technique that combines a percutaneous Chevron osteotomy of the first metatarsal with an Akin closing wedge osteotomy of the proximal phalanx by Isham burr.9,10 This dual osteotomy approach also aims to correct the deformity through realignment of the first ray.
While studies have reported that the Ludloff procedure leads to good results both radiographically and clinically (e.g. American Orthopaedic Foot and Ankle Society Score (AOFAS)), 11 comparative studies have shown mixed results. The MICA procedure, while providing patients with a smaller wound, have also been shown to significantly improve clinical outcomes while being associated with lower rates of complications and recurrence. 12 It has also been reported that the conversion rate to an open surgery was as low as 2%. 13 This minimally invasive procedure has also demonstrated to yield comparable results in a prospective cohort study comparing the MICA technique to the open Chevron osteotomy. 14
Both the Ludloff and MICA procedure have shown good clinical and radiological results in the surgical management of hallux valgus, 15 but there is limited high-quality comparative data on their relative efficacy. Understanding the comparative outcomes between these two techniques is important to help guide surgical decision-making for patients with moderate to severe hallux valgus.
Objectives
The primary objective of this retrospective study was to compare the radiographic and clinical outcomes of patients who has underwent either modified McBride's procedure with Ludloff osteotomy or the MICA osteotomy for the correction of moderate to severe hallux valgus angle (HVA > 35˚) deformity. Secondary objectives included reviewing complications, and time of osteotomy union between the two surgical techniques.
We hypothesise that the MICA osteotomy will yield a non-inferior outcome when compared to the Ludloff procedure, while being able to provide patient's with a smaller wound and a relatively better cosmesis with a smaller scar.
Methods
Study design
This was a single-centre, retrospective study. The medical records of patients who underwent either a Modified McBride's procedure with Ludloff osteotomy or a MICA osteotomy for the treatment of moderate to severe hallux valgus deformity between September 2010 and May 2023 were reviewed. Inclusion and exclusion criteria are as shown below (Table 1). Case matching was done to identify two groups of patients that had comparable demographics and preoperative deformity (Figure 2).
Inclusion and exclusion criteria.
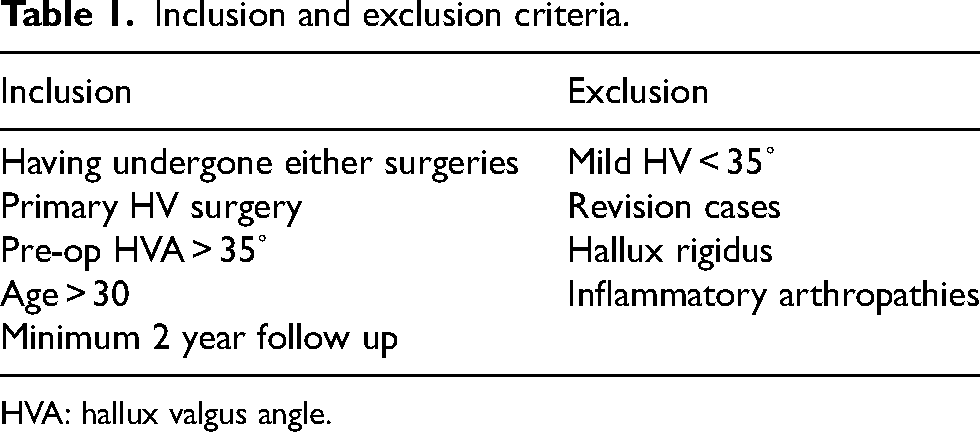
HVA: hallux valgus angle.
Surgical technique
Ludloff osteotomy with modified McBride's procedure
The procedure is done with the patient either under general anaesthesia or spinal anaesthesia. Upper thigh tourniquet is applied. Soft tissue modified McBride's procedure involving release of the adductor hallux tendon, metatarsosesamoid complex, and intermetatarsal ligaments are done via a dorsal incision over the first webspace. The Ludloff osteotomy is done using a reciprocating power saw through an incision over the medial aspect along the first metatarsal shaft. The dorsal and plantar medial cutaneous nerves, and the extensor hallucis longus tendon are identified and protected.11,15 A reverse L-shaped capsulectomy is carried out prior to performing bone cut. The bone cut is carried out in a proximal dorsal to distal plantar fashion at about 10° to the long axis. 2.7 mm cortical screws are placed proximally as a pivot to guide axis of rotation, a second and third 2.0 mm-screw is placed after adequate correction has been achieved with confirmation under an image intensifier (Figure 1). Bunionectomy is done, and plication of the capsule is then carried out through bone tunnels and anchored by vicryl 1 sutures prior to skin closure with non-absorbable sutures.

Ludloff procedure; pre- and post-op.

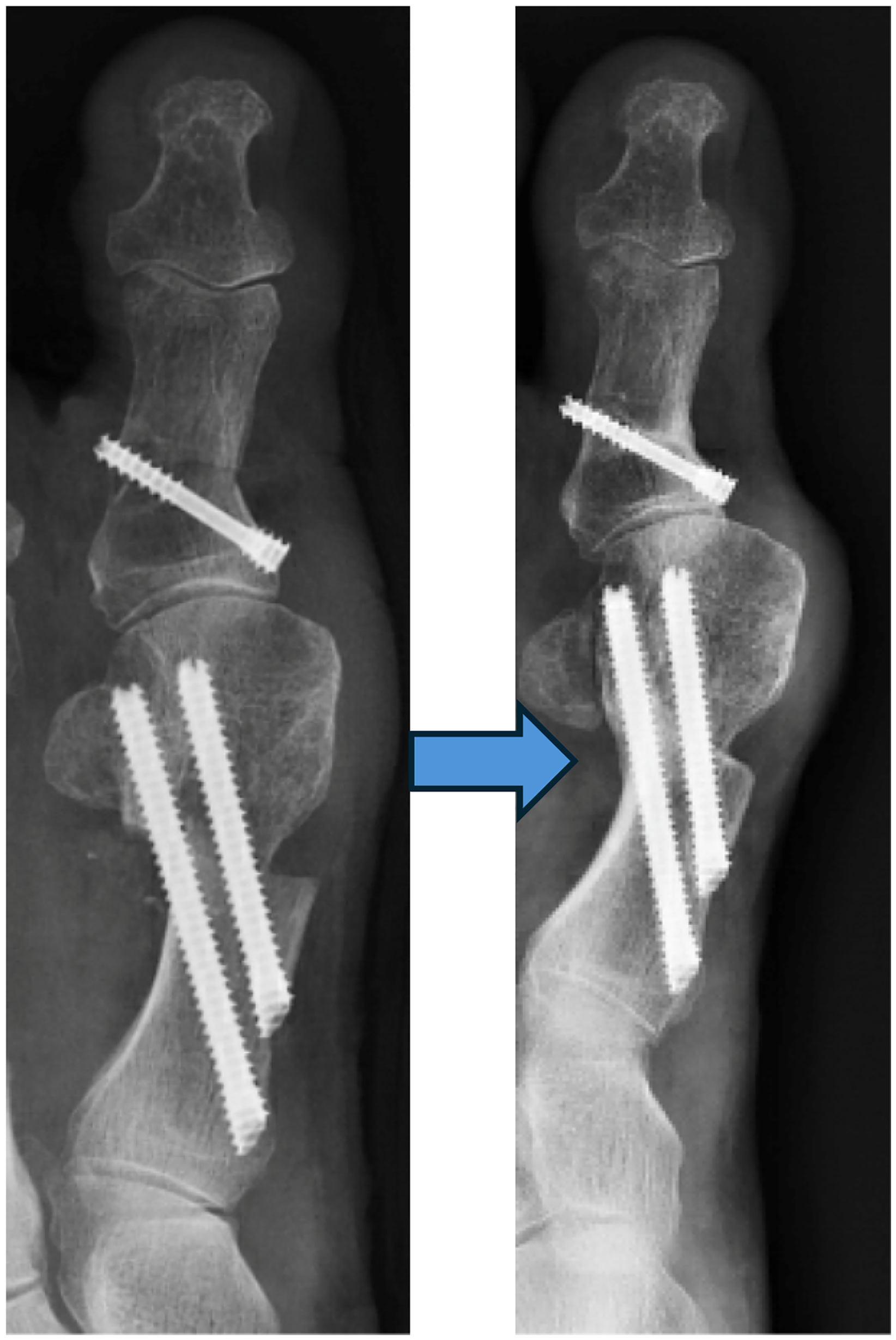
Pre- and post-op X-ray and clinical photo following MICA.
MICA osteotomy
The procedure is done with the patient under general or spinal anaesthesia. Through small stab incision over the direct medial aspect of the first metatarsal shaft, the metatarsal neck cut is done. Osteotomy is done using an Isham burr under intra-operative mini c-arm guidance. The distal metatarsal head fragment is shifted laterally, and temporarily fixed with two K wires placed antegrade through the proximal metatarsal fragment. The more proximal one of the two K wires will be engaging both medial and lateral cortices of the proximal metatarsal fragment. Alignment and position is confirmed under mini c-arm prior to insertion of two 3.5–4.0 mm minimally invasive screws (MIS) with bevelled head for MICA procedure. Percutaneous Akin is then done through an incision over the medial aspect at the base of the proximal phalanx using an Isham burr under mini c-arm guidance. The closing wedge akin osteotomy is then fixed in place with a 3.0 mm headless screw. Lesser toe reconstructions, if indicated, are carried out in the same manner for both groups regardless of the procedure done for the hallux valgus.
Post-operative care and rehabilitation
In both groups, patient go through the same rehabilitation regime on non-weight bear walking. Patients with Ludloff Osteotomy and Modified McBride's Procedure will have big toe creping for 6 weeks. Post-operatively, patients are sized and trained for full weight bearing heel walking in forefoot off-loading insoles with or without crutches/frame. Patients are allowed for walking exercise with physiotherapist on post-operative day 1, and are discharged on day 1 if their mobility is adequate. Patient's wounds are covered and dressings are kept intact until one week after the operation for wound inspection. Stitches are removed at the clinic two weeks after surgery. Patients are kept on the forefoot off-loading insole and are to continue heel walking for eight weeks total after surgery. If any lesser toe reconstructions procedures are done in the same operative session and are temporarily immobilised by axial K wires, they are removed at 6 weeks (Figure 3).

Measurement of HVA.
Outcomes parameters
The radiographic outcomes measured included the: HVA, first and second IMA, DMAA, tibial sesamoid position based on Hardy and Clapham's system, 16 and time to osteotomy union. X-rays were measured once pre-operatively, then routinely on follow ups at 3, 6, 12, and 24 months post-operatively. Clinical outcomes assessed, included the AOFAS Hallux Metatarsophalangeal-Interphalangeal Scale score, complications and recurrence.
The HVA, was measured as the angle between the midshaft longitudinal axes of the first metatarsal and the proximal phalanx. The IMA was measured as the angle between the midshaft longitudinal axis of the first and the second metatarsals. The DMAA was measured by adopting the same method as O’Brian, measuring the angle between a line perpendicular to the longitudinal axis of the first metatarsal and a line parallel to the distal articular surface; the articular surface was identified via the sagittal groove medially, and the lateral extent identified using the width of the proximal phalanx's articular surface as a guide. 17 In post-operative X-rays, we adopted a similar measurement method as Kaufmann, the longitudinal axis of the first metatarsal is taken as a line drawn from the centre of the metatarsal head to the centre of the metatarsal base. 10 Time of osteotomy union was determined based on the presence of any crossing of trabecular lines or blurring of the osteotomy sites on X-ray in the dorsoposterior projection (Figure 4).
Time to osteotomy union.
The above x-ray measurements were done by an orthopaedic higher trainee and an orthopaedic resident specialist in separate occasions.
Data analysis
We conducted t-test, Chi-square test, and Mann–Whitney test to ensure comparable demographics and disease severity between the two groups, with regard to gender, age, pre-operative clinical scores, and pre-operative radiographic measurements.
Mann–Whitney test was used to compare the mean of the outcomes between the two operations post-operatively, in regards to the HVA, IMA, DMAA, tibial sesamoid position, and post-operative AOFAS score. The Wilcoxon Signed Rank test, Friedman test and Dunn-Bonferroni post-hoc test was conducted for each operational group separately, comparing the pre-operative and post-operative AOFAS scores and radiological measurements. Chi-square test and Pearson correlation was used for analysis of recurrence. For all cases, a p-value of <.05 was considered statistically significant.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (No. 2024.728) on 12 February 2025, with the need for written informed consent waived.
Results
A total of 62 feet in 56 patients were included in the analysis, after having fit the inclusion and exclusion criteria and case matched for comparable demographics. Thirty-five underwent Ludloff osteotomy with modified McBride procedure, and 27 underwent the MICA osteotomy. The demographics are as listed below (Table 2). Age, gender, pre-operative severities were comparable between the two cohorts.
Patient demographics.
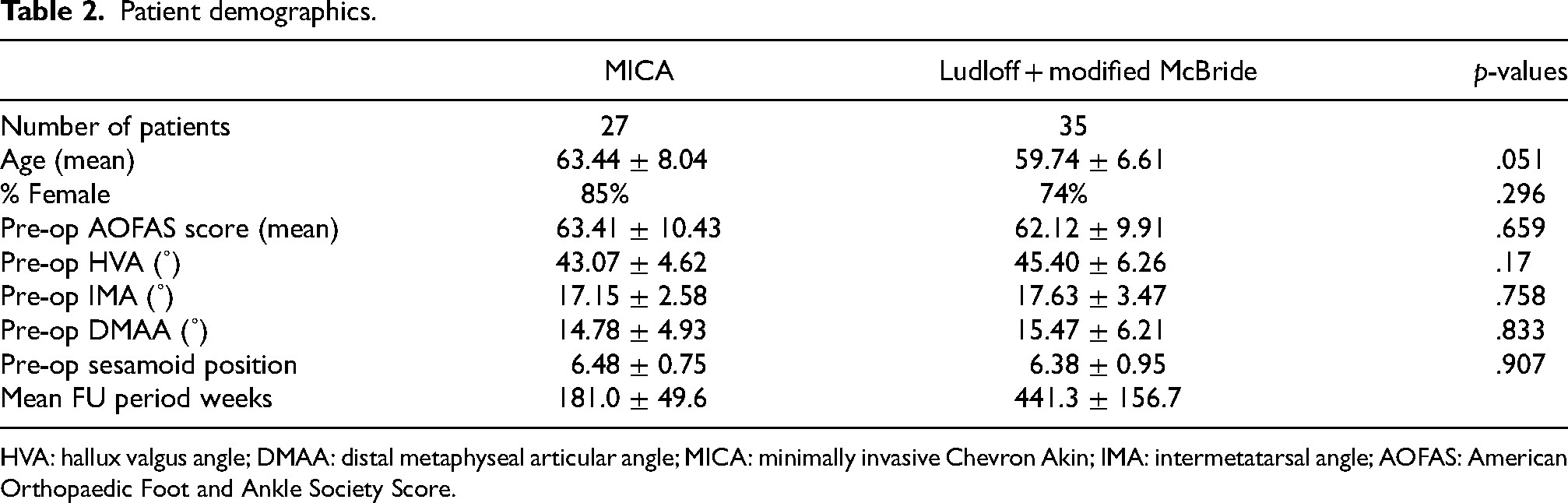
HVA: hallux valgus angle; DMAA: distal metaphyseal articular angle; MICA: minimally invasive Chevron Akin; IMA: intermetatarsal angle; AOFAS: American Orthopaedic Foot and Ankle Society Score.
Radiological outcomes
At final follow-up, the mean HVA was reduced to 16.77 ± 10.62 in the Ludloff group and 15.63 ± 7.68 in the MICA group, representing a significant improvement in both groups (p < .001) with no statistically significant difference between the two groups (p = .722) (Table 3, Chart 1).
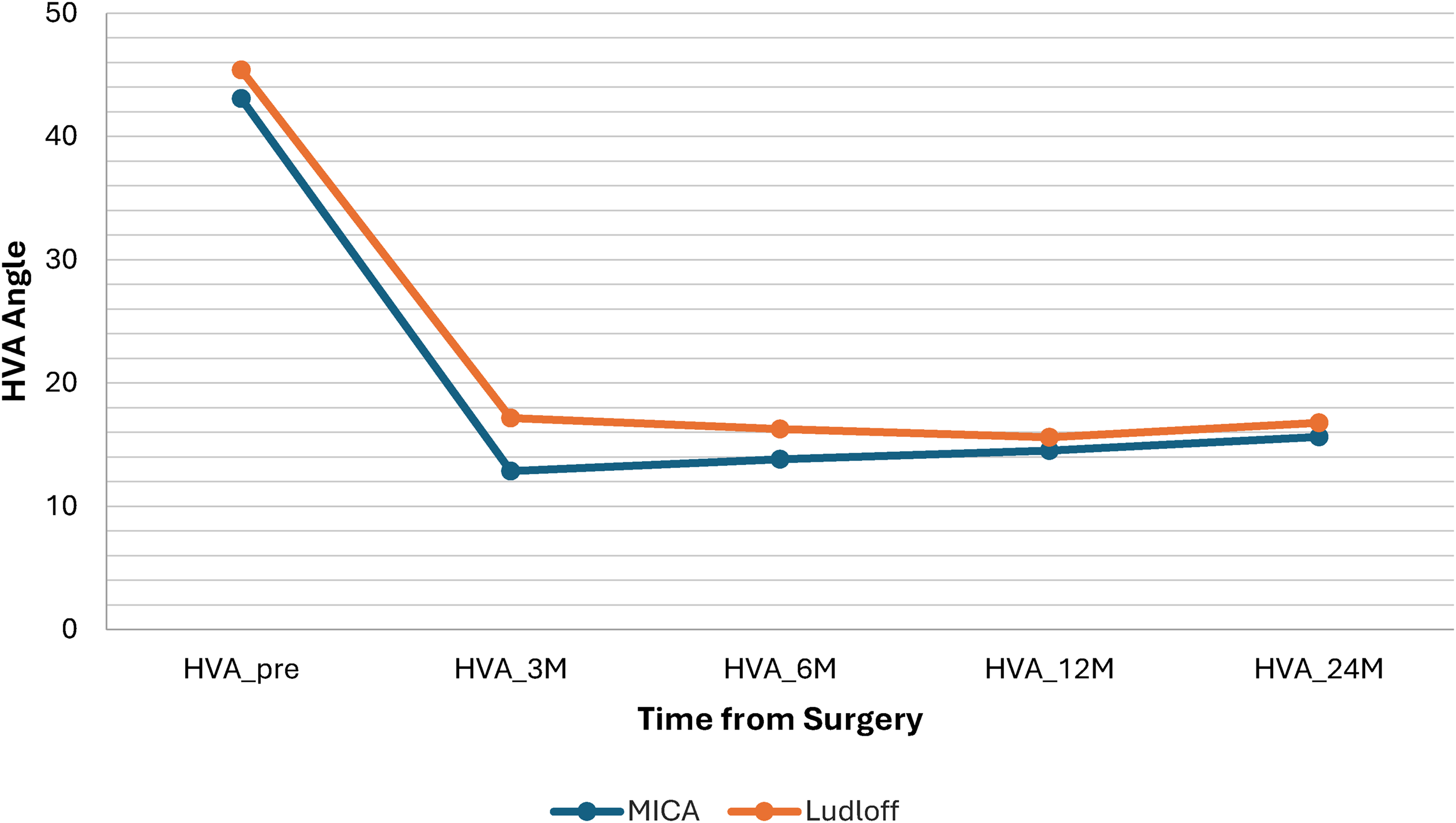
HVA.
Post-operative HVA.
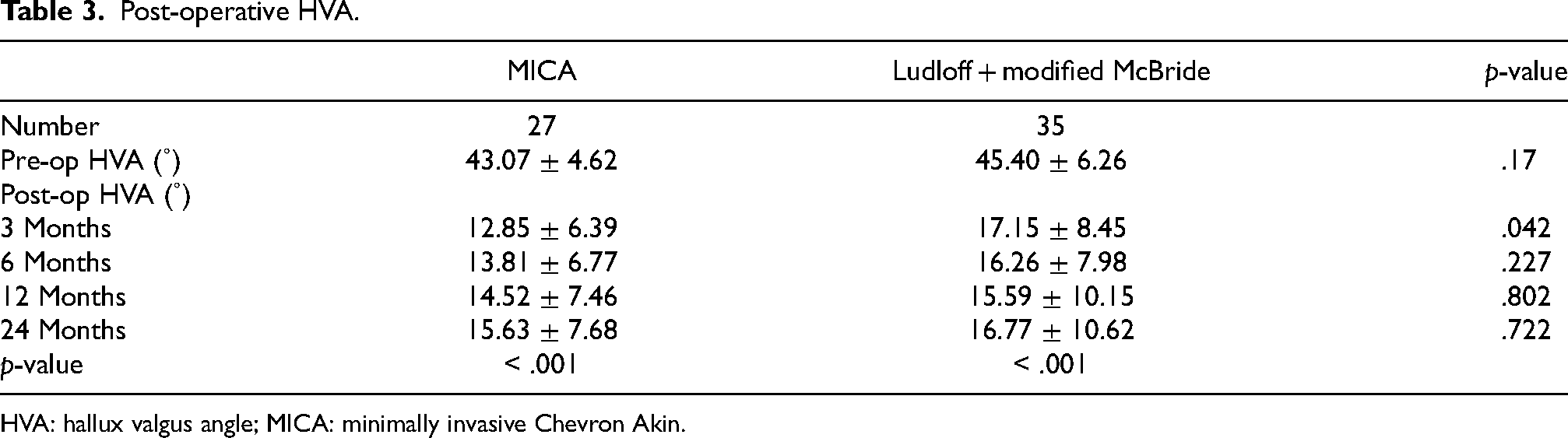
HVA: hallux valgus angle; MICA: minimally invasive Chevron Akin.
The mean IMA was reduced to 10.14 ± 4.28 in the Ludloff group, and 9.56 ± 3.43 in the MICA group, with statistically significant improvement within each group separately (p < .001), and no statistically significant differences between the two groups at final follow up (p = .754) (Table 4, Chart 2).
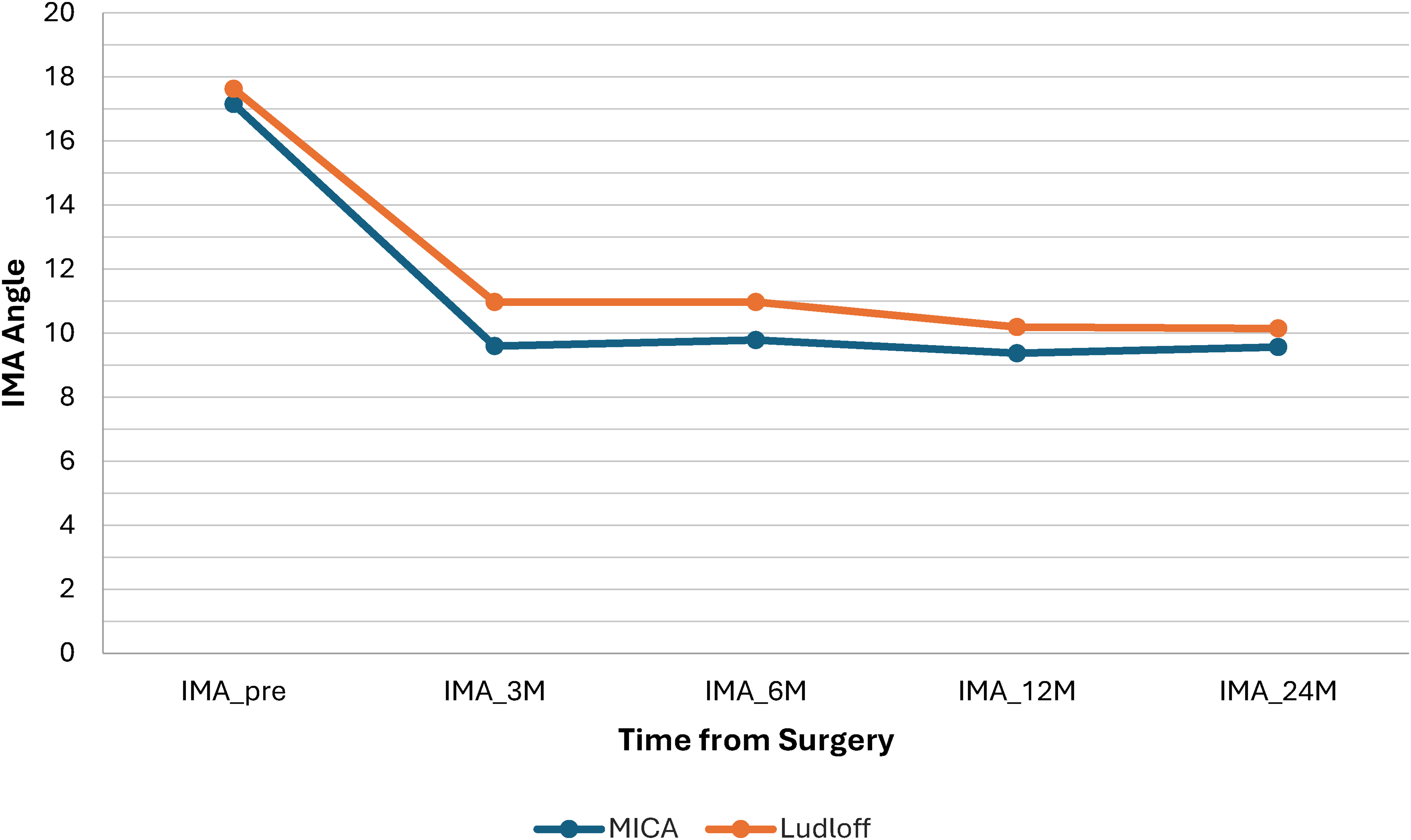
IMA.
Post-operative IMA.
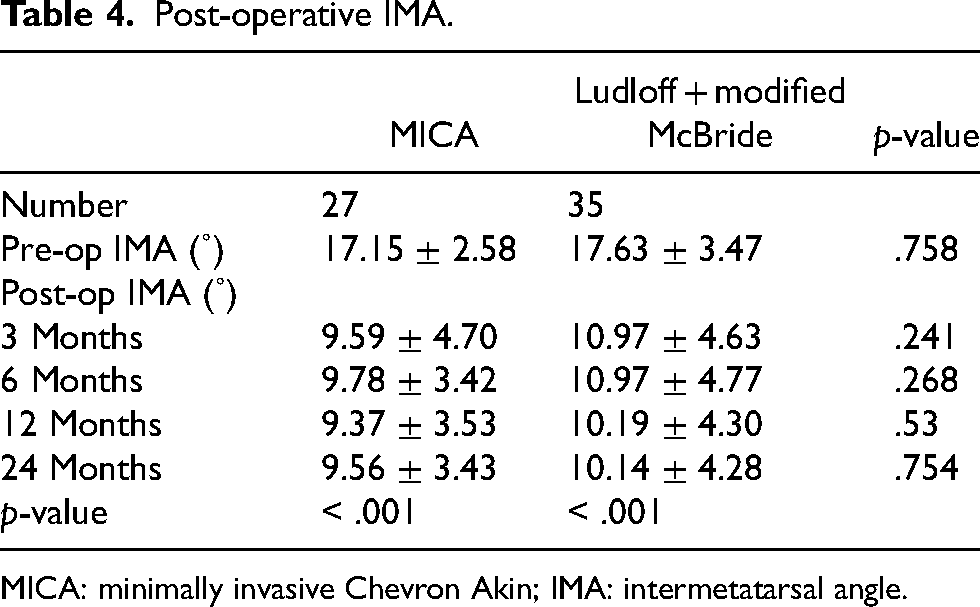
MICA: minimally invasive Chevron Akin; IMA: intermetatarsal angle.
For distal metatarsal articular angle, the pre-operative results were comparable with no statistical significance (p = .833). Both procedures also demonstrated statistically significant (p < .001) improvement between their pre-operative and post-operative mean DMAA individually. However, at three months, six months and 24 months post-operatively, there was a statistically significant difference in the mean distal metatarsal articular angle between the two groups, favouring the MICA group (p = .03, p = .012, p = .024, respectively) (Table 5, Chart 3).
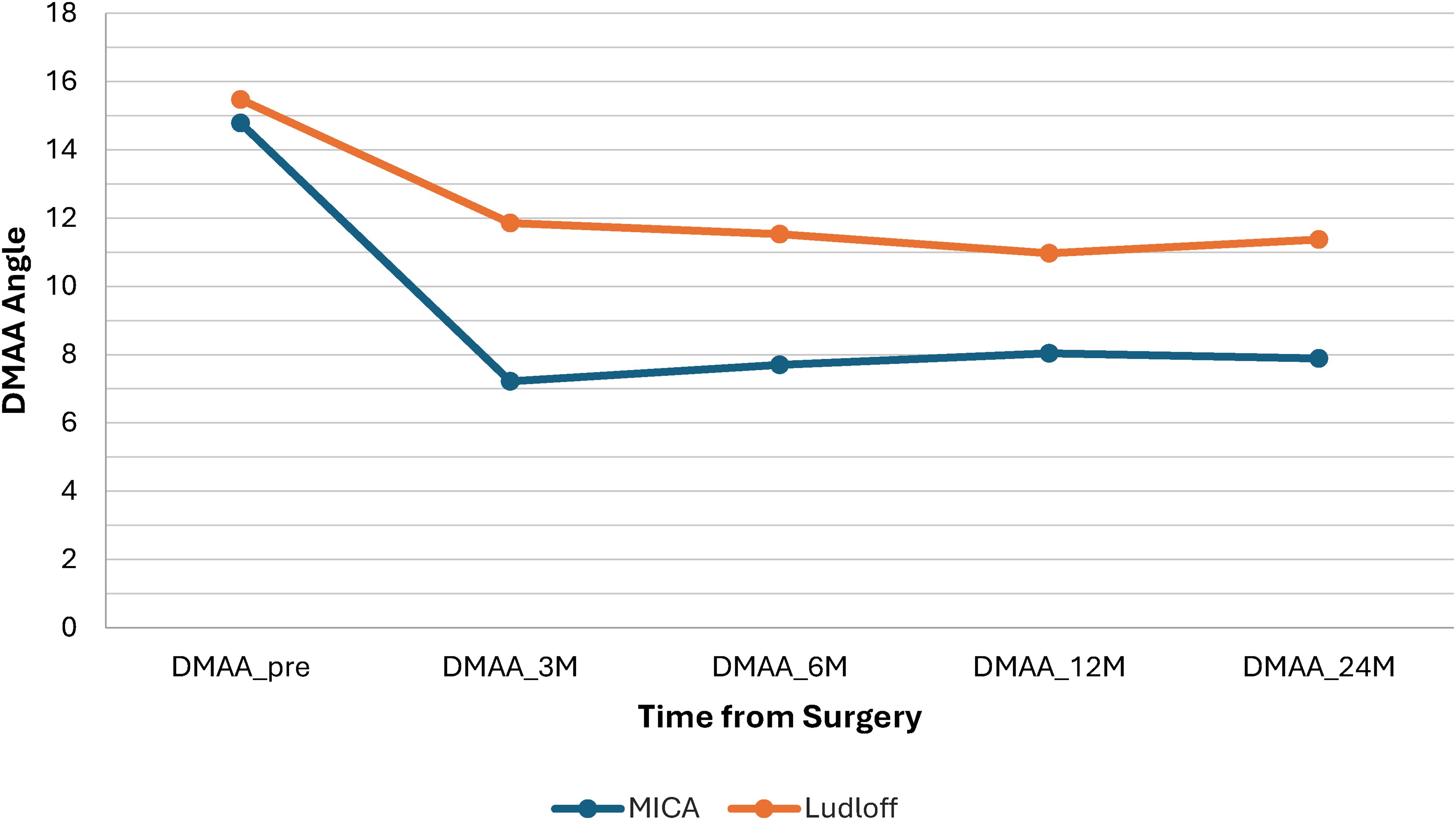
DMAA.
Post-operative DMAA.
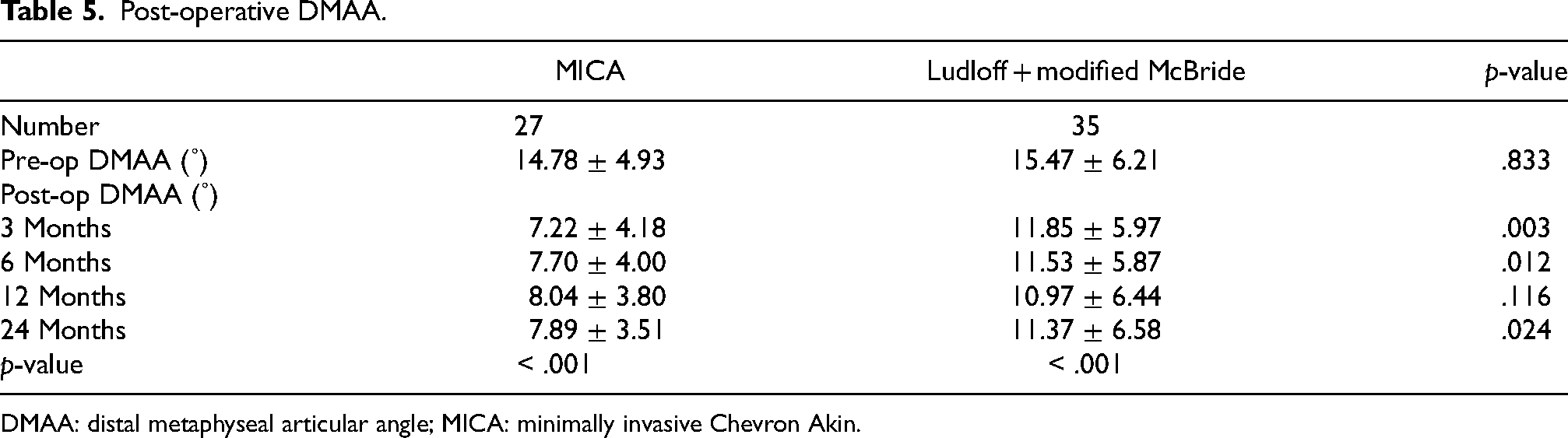
DMAA: distal metaphyseal articular angle; MICA: minimally invasive Chevron Akin.
For sesamoid position, the pre-operative results were comparable with 6.38 ± 0.95 for Ludloff group, and 6.48 ± 0.75 for MICA group (p = .907). Both procedures also demonstrated statistically significant (p < .001) improvement between their pre-operative and post-operative mean tibial sesamoid position individually. However, it was observed that at three months, six months, 12 months, and 24 months post-operatively, there was a statistically significant difference in sesamoid position between the two groups, favouring the Ludloff group (Table 6, Chart 4).
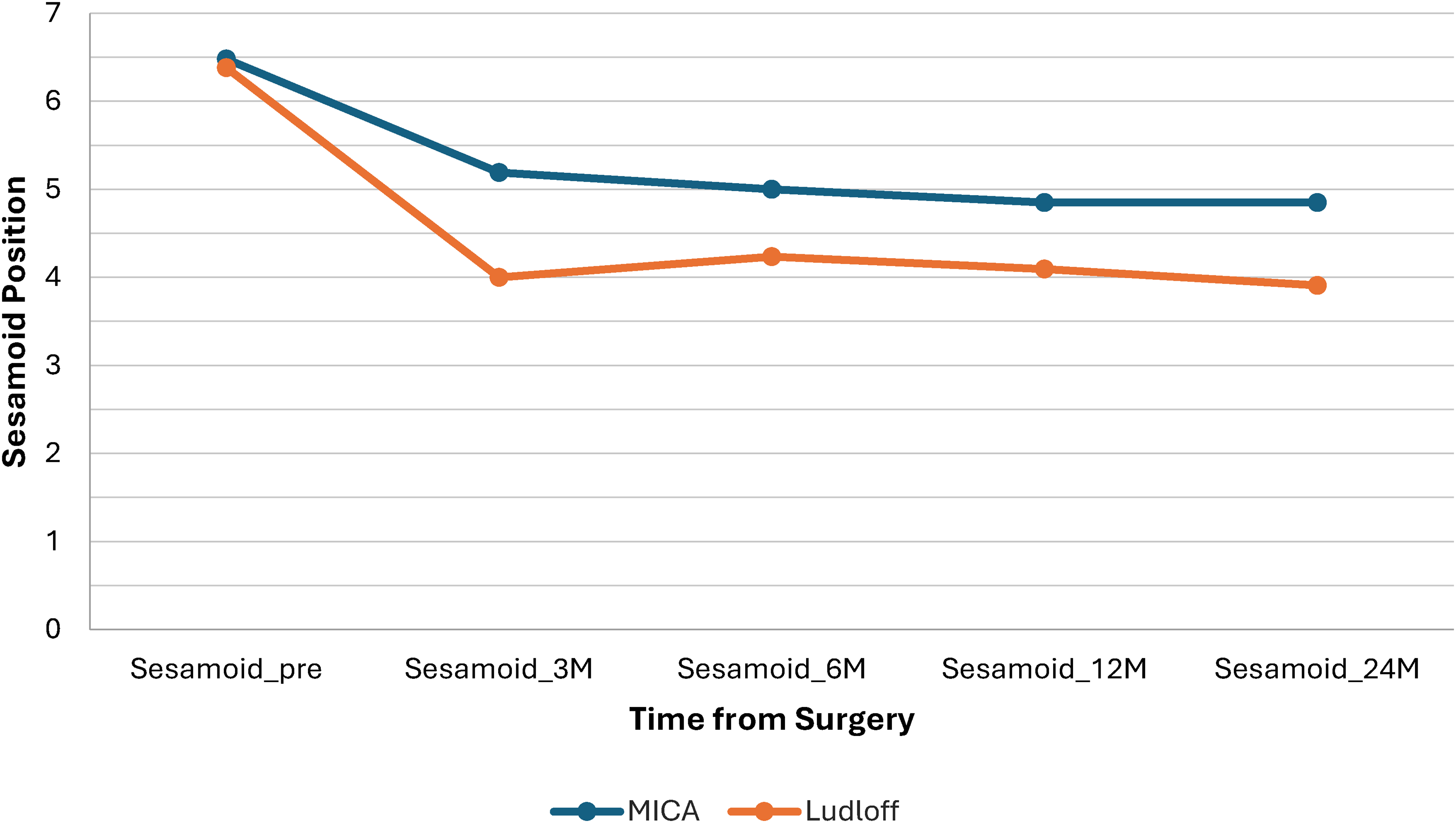
Sesamoid.
Post-operative sesamoid position.
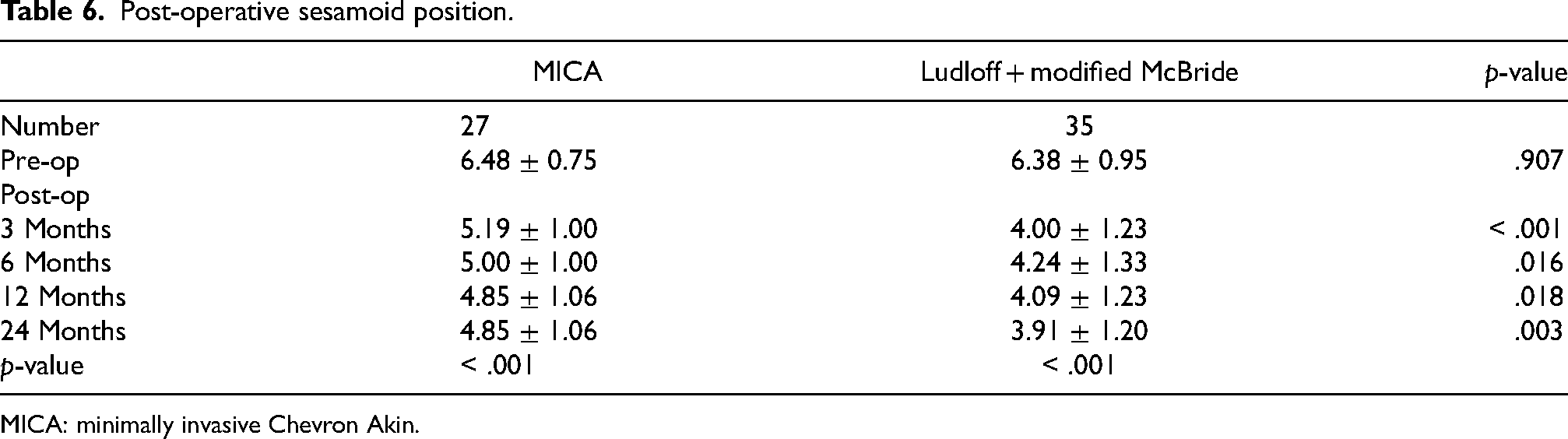
MICA: minimally invasive Chevron Akin.
Time to union was also similar between the two groups (p = 0.517). In the Ludloff group, the average time to union was 10.41 ± 2.66 weeks; in the MICA group, it was 9.93 ± 2.02 weeks (p = .52). Neither group had patients who experienced non-unions (Table 7).
Time to union.

MICA: minimally invasive Chevron Akin.
Clinical outcomes
The AOFAS scores showed statistically significant improvement, from a mean of 62.12 ± 9.91 preoperatively to a mean of 85.31 ± 9.27 postoperatively in the Ludloff group (p < .001), and from 63.41 ± 10.43 to 86.85 ± 6.86 in the MICA group (p < .001), with no significant difference between groups (p = .693) (Table 8).
Post-operative AOFAS.

AOFAS: American Orthopaedic Foot and Ankle Society Score; MICA: minimally invasive Chevron Akin.
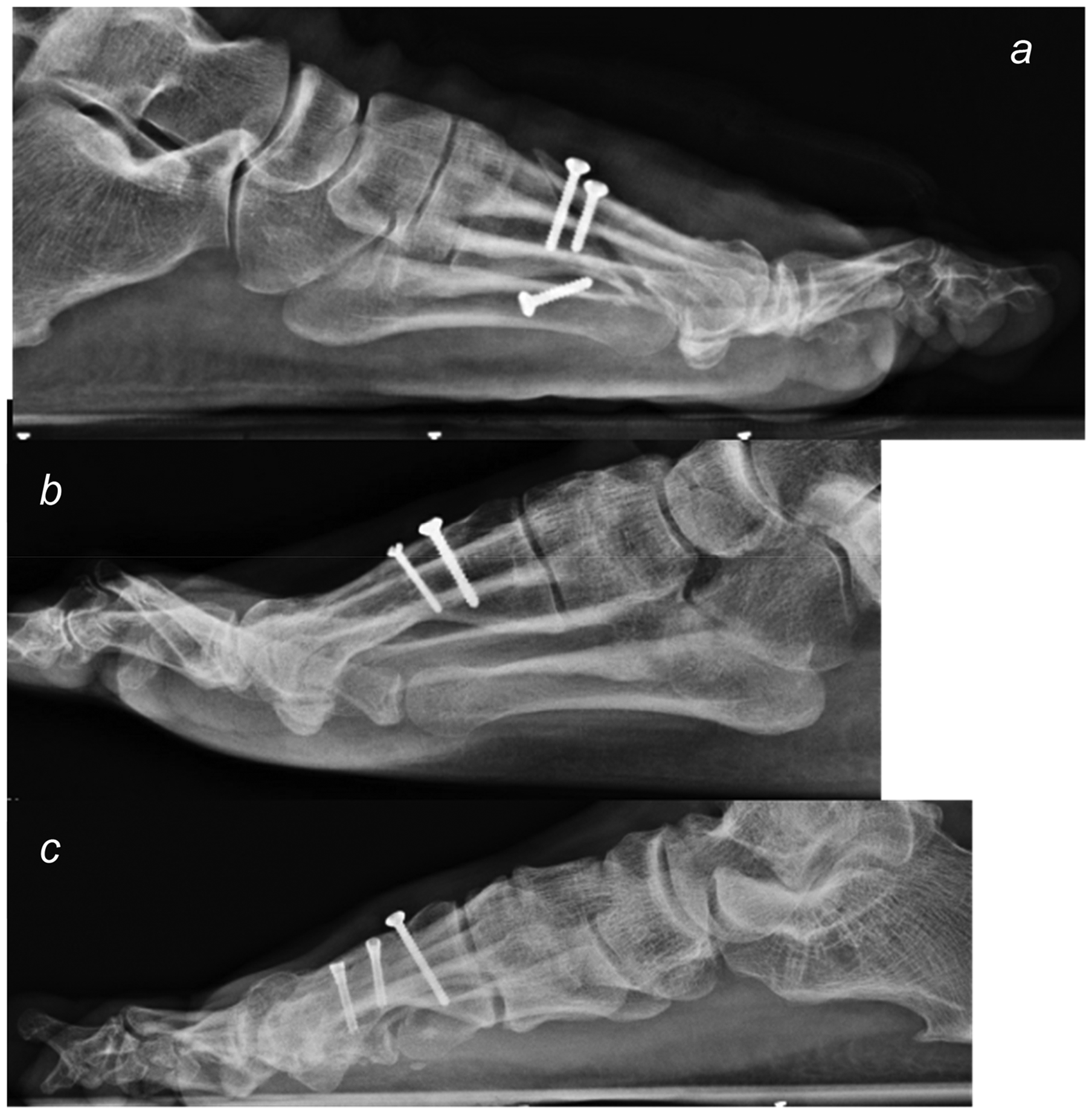
Both groups had three patients that experienced complications. In the MICA group: one case had a 4.0 mm MIS cut-out over the plantar aspect, requiring removal after the osteotomy site has healed; one case of akin screw backout leading to skin impingement, this occurred at approximately two years after the operation, which required removal; and one case of hallux varus of around 4˚, but the patient had no symptoms and opted for observation only. In the Ludloff group, there was one case of screw loosening requiring revision on post-operative day 13, and two cases experienced skin impingement by the screws requiring removal after the osteotomy sites have healed (Figures 5 and 6).

Examples of complications in MICA: (a) MIS cut-out, (b) akin screw backout, (c) hallux varus.
Examples of complications in Ludloff: (a) screw loosening, (b, c) skin impingement by screw.
A recurrence, in our study, was determined when both of the following occurs: (a) an HVA of ≥ 15˚ on latest follow up, and (b) a rebound in HVA of ≥ 10˚ when compared to the immediate post-operative HVA (e.g. (most recent HVA) – (Immediate post-op HVA) ≥ 10˚). There are two cases in the Ludloff group, with most recent HVAs measured to be 15˚ and 29˚ and three cases in the MICA group, with most recent HVAs measured to be 20˚, 24˚, and 16˚. Incidence of recurrence in both groups showed no statistically significant difference (p = .229) (Table 9). However, all cases were satisfied with their results and opted to continue conservative observation only.
Recurrence.
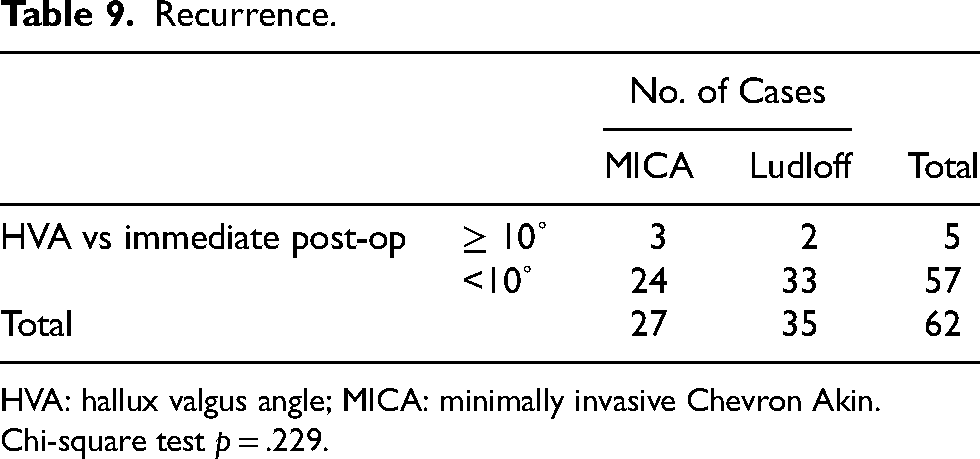
HVA: hallux valgus angle; MICA: minimally invasive Chevron Akin.
Chi-square test p = .229.
Within the MICA group, cases with a more severe pre-op HVA was noted to have a statistically significant moderate correlation (correlation coefficient (r) = 0.524 (p = .005)) (Table 10) with a greater degree of rebound in the latest follow up. However, no such correlation was noted with the Ludloff group within our study (p = .172).
Correlation with pre-op severity.
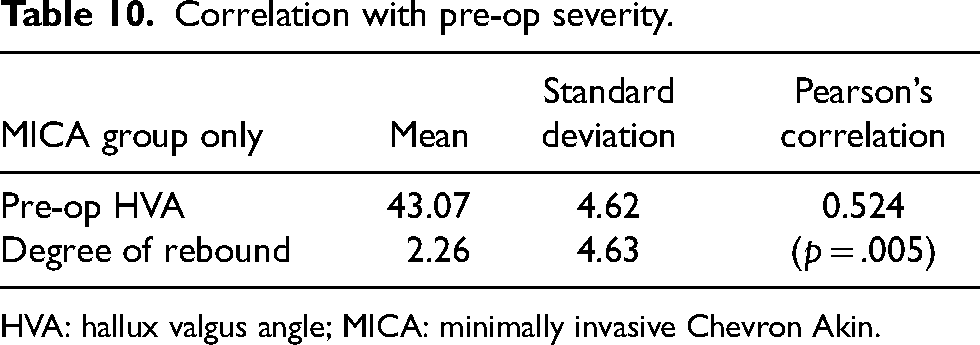
HVA: hallux valgus angle; MICA: minimally invasive Chevron Akin.
Discussion
In this study, both procedures were capable of significantly correcting moderate to severe hallux valgus deformity of > 35˚ to an acceptable alignment with comparable satisfactory AOFAS scores, and low incidence of complications and recurrence. While the MICA procedure showed better correction for the distal metatarsal articular angle, the Ludloff procedure showed better correction of the tibial sesamoid position. However, the overall clinical results based on the AOFAS scores were comparable with no statistically significant difference.
The post-operative tibial sesamoid position showed results that were favoured the Ludloff group. We suspect that this may be due to the addition of the Modified McBride procedure, as this step was not included in the MICA osteotomy group. Modified McBride procedure has been shown to improve sesamoid position even if done in isolation. 18 The incomplete reduction of sesamoid position has been reported to be a risk factor for the recurrence of hallux valgus after surgical collection. 19 However, this was not observed in our study as the incidence of recurrence were comparable with no statistically significant difference between the two groups.
As for the post-operative DMAA, our results favoured the MICA group. It has been shown in one study, focused on cases with high pre-operative DMAA, that an inadequate correction of DMAA had a moderate to strong correlation with HVA recurrence. 20 Again, this was not observed in our study in terms of incidence of recurrence. We suspect that while both procedures improved DMAA to a statistically significant extent, the MICA procedure involved only a translational component in its deformity correction, while the Ludloff procedure involved a rotation component: whereby the distal articular surface is rotated further lateral. So although the longitudinal axis of the first metatarsal is re-aligned during the Ludloff osteotomy procedure, reducing the IMA, the improvement in DMAA may be mitigated by the rotational component in its deformity correction.
The learning curve of MICA has been regarded to be more advanced and technically demanding when compared to other percutaneous procedures of the foot, and is generally believed to have a relatively steep learning curve, with some studies quoting around 30–40 cases before a reduction in operation time and fluoroscopic exposure is achieved.21–23 Complication rates and recurrence was also not reported to be significantly different as a surgeon becomes more proficient in the technique.
Limitations
After case matching, the available sample size only had limited occurrences of recurrence and complications. Although the data yielded no statistically significance differences, the limited incidence will limit the power of this conclusion. Stronger correlations in regards to recurrence and complications cannot be commented on with the available data as the minimal follow up duration is two years.
As this was a retrospective report, there was no blinding or randomisation of intervention. Patient's and operating surgeon were both actively involved in the decision making of the surgery that the patient will undergo, possible confounders and placebo may exists in terms of the clinical outcome. However, the radiographical outcome may not be largely affected by the lack of randomisation, as pre-operative radiographic measurements were statistically comparable.
Radiographic measurements were also done by two separate investigators, an orthopaedic trainee and an orthopaedic specialist. Although the methods of measurement and points of references used were the same as that mentioned in earlier parts of this study, interobserver differences may still be present. Both investigators shared measurements of X-rays in both the Ludloff group and MICA groups.
Further research
Besides addressing the limitations above, further investigation into possible qualitative clinical outcomes may provide additional valuable information regarding both procedures. This study so far has demonstrated that the MICA procedure can yield a non-inferior outcome when compared with the Ludloff with Modified McBride. We would further postulate that as MICA is a minimally invasive procedure, the post-operative wound pain and wound complications would be less, thus in future studies, documentation of pain score, for example via a visual analogue scale may shed light on this possibility. Length of stay could also be documented and compared, however with our post-operative rehab protocol, most of our patients could be safely discharged on post-operative day 1 on full weight bearing heel walking in a forefoot offloading sandal regardless of intervention.
Conclusions
Both the modified McBride's procedure with Ludloff osteotomy and the MICA osteotomy demonstrated excellent radiographic and clinical outcomes for the correction of moderate to severe hallux valgus deformity, with significant differences in two aspects between the two techniques, favouring Ludloff in terms of sesamoid position, and favouring MICA in terms of distal metatarsal articular angle.
These results suggest that both the Ludloff osteotomy and the MICA osteotomy are safe and equally effective options for surgical management of moderate to severe hallux valgus deformity. The choice between the two procedures may depend on surgeon preference and experience, as well as patient-specific factors such as activity level, and desire for a minimally invasive approach with smaller wound incision. Further prospective, randomised studies are warranted to provide additional high-quality comparative data on these two hallux valgus correction techniques.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Joint Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee (No. 2024.728) on 12 February 2025, with the need for written informed consent waived.