
Abstract
Background:
There is limited literature available that provide information about fixation methods for minimally invasive hallux valgus osteotomies. Our objective was to evaluate the strength of different fixation methods for a percutaneous extracapsular transverse cervical metatarsal (PTCM) osteotomy in a sawbone model.
Methods:
Thirty solid foam sawbone foot models were used. Percutaneous extracapsular transverse cervical metatarsal osteotomies were performed and fixed in a standardized fashion in 6 different groups: (1) one 4.0-mm screw; (2) 2 (one 4.0-mm and one 3.0-mm) parallel screws; (3) 2 (one 4.0-mm and one 3.0-mm) divergent screws; (4) same as group 3, but with lateral metatarsal head cortex purchase with the 4.0-mm screw; (5) same as group 4, but with two 4.0-mm screws; (6) same as group 5, but with two 3.5-mm screws. Cyclic and load to failure testing were performed applying a plantar load to the metatarsal head. The measured variables were stiffness and force needed to create deformity using a Zwick Roell Universal Testing Machine.
Results:
Group 1 failed as a result of rotational instability in cyclic testing. In load to failure testing, group 3 did not achieve difference compared with group 2 (P = .09) (181 vs 131 N). Group 4 was stronger (P = .02) (250 N) than groups 1-3. Group 5 did not show differences relative to group 4 (P = .1) (223 N). Group 6 was stronger only than groups 1 and 2 (P = .01) (193 N).
Conclusion:
In this sawbones-based study, we found that the use of two 4.0-mm screws or use of a 3.0-mm screw and a 4.0-mm screw with lateral first metatarsal head cortical purchase was superior to other screw configurations.
Introduction
In the last decade, there has been a growing interest in percutaneous surgery in hallux valgus. Publications relating to minimally invasive surgery in hallux valgus have increased 150% in the past 10 years. 11 Many different techniques have been described with varying results.
Minimally invasive techniques have gained popularity in all surgical specialties essentially because of reduced soft tissue complications, better cosmesis, quicker return to work, and lower opioid use.6,10 In hallux valgus surgery, minimally invasive techniques have the potential added benefits for patients in whom wound healing is a problem.
First-generation percutaneous techniques for hallux valgus treatment involved bone osteotomies without any kind of fixation.4,13 Later, Bosch introduced the concept of a straight bony cut on the first metatarsal neck, which was fixed with an axial Kirschner-wire (second generation), providing coronal stability, but lacking sagittal and rotational stability. 3 Later, Redfern and Vernois12,16,17 proposed the MICA technique (minimally invasive chevron and Akin), including a chevron osteotomy at the metatarsal neck level, fixated with an internal fully threaded screw with bicortical support showing good clinical and radiologic results (third-generation technique).
Over the last decade, Lam et al 7 introduced the PECA technique (percutaneous chevron and Akin). In 2020, Robinson and Lam 14 modified the chevron osteotomy to an extracapsular cervical transverse osteotomy (Bosch like) as variation, and a more distal screw position provided theoretically a more stable construct. 14 This technique was later published as META (metaphyseal extraarticular transverse and Akin osteotomy). 8
To the best of the authors’ knowledge, there is no published evidence evaluating which one of the different screws and osteotomy configurations provide a more stable fixation construct in percutaneous hallux valgus techniques. Only a few biomechanical studies have evaluated different constructs for open techniques using cadaveric and sawbone models.1,2,5,15,18,19
The aim of this study was to compare the mechanical performance (stiffness and failure mode) of different screw configurations in a first metatarsal sawbone model where a cervical straight osteotomy was performed. The authors’ hypothesis is that divergent and bigger screws will lead to an increase in construct stiffness.
Materials and Methods
Thirty first ray foot solid foam sawbones models (A Pacific Research Company, Washington, DC) were used. All specimens were the same size and quality. All procedures were performed by foot and ankle fellowship–trained orthopaedic surgeons. One surgeon completed all transverse cervical osteotomies as described by Lam et al. 7 The osteotomies were performed using a 2.1 × 13-mm minimally invasive surgical burr. The power unit was set to 5000 rpm and 100% torque.
First, the meta-diaphyseal junction of the first metatarsal was identified. The burr was angled 15 degrees to the axis to minimize shortening of the first metatarsal. The transverse neck metatarsal osteotomies were then performed. The distal remnant was displaced by 75% of the metatarsal head width.
The 30 samples were divided into 6 groups (5 specimens each) (Figures 1 and 2). Using a polymethylmethacrylate (PMMA) first metatarsal osteotomy template, bone segments were fixed with a standardized displacement (75%) to avoid variations during the procedure (Figure 3). Using the template, standardized screw-positioning holes were used to fix the models in an identical fashion with the following variations:
For group 1, 1 guidewire was percutaneously placed at the proximal first metatarsal, traversing the medial and lateral metatarsal shaft cortices, ending into the metatarsal head fixing the cervical osteotomy. After this, the Kirschner-wire was replaced with one 4.0-mm fully threaded cannulated screw.
For group 2, 2 guidewires were percutaneously placed at the level of the proximal first metatarsal. The first wire was inserted into the metatarsal head as in group 1; the second wire was driven parallel and 1 cm distal to the first wire. This wire starts at the medial metatarsal cortex ending in the metatarsal head center, not penetrating the lateral metatarsal cortex. The proximal wire was replaced by a 4.0-mm and the distal wire by a 3.0-mm fully threaded cannulated screw.
For group 3, 2 screws were used similarly to group 2, but divergent in the axial plane.
For group 4, 2 screws were used similarly to group 3, but the proximal screw traversed the lateral head cortex.
For group 5, 2 screws were used similarly to group 4, but using two 4.0-mm fully threaded cannulated screws.
For group 6, 2 screws were used similarly to group 5, but using two 3.5-mm fully threaded cannulated screws. See Figures 1 and 2 for details.
All screws were constant-pitch, fully threaded cannulated cortical screws made of titanium. They were inserted aligned and parallel to the metatarsal shaft in the sagittal plane.

Groups diagram. Diagram showing the 6 study groups. A green line represents a 4.0-mm cannulated screw. A blue line represents a 3.0-mm cannulated screw. An orange line represents a 3.5-mm cannulated screw.

Groups example. Four first metatarsal-great toe sawbones models are shown. Specimens from groups 3, 4, 5 and 6 are shown from left to right.
Template. The polymethylmethacrylate (PMMA) first metatarsal osteotomy template is shown here, where bone segments were fixed with a standardized displacement (75%) to avoid variations during the procedure. Using the template, standardized screw-positioning holes were used in order to fix the models in an identical fashion.
Biomechanical Testing
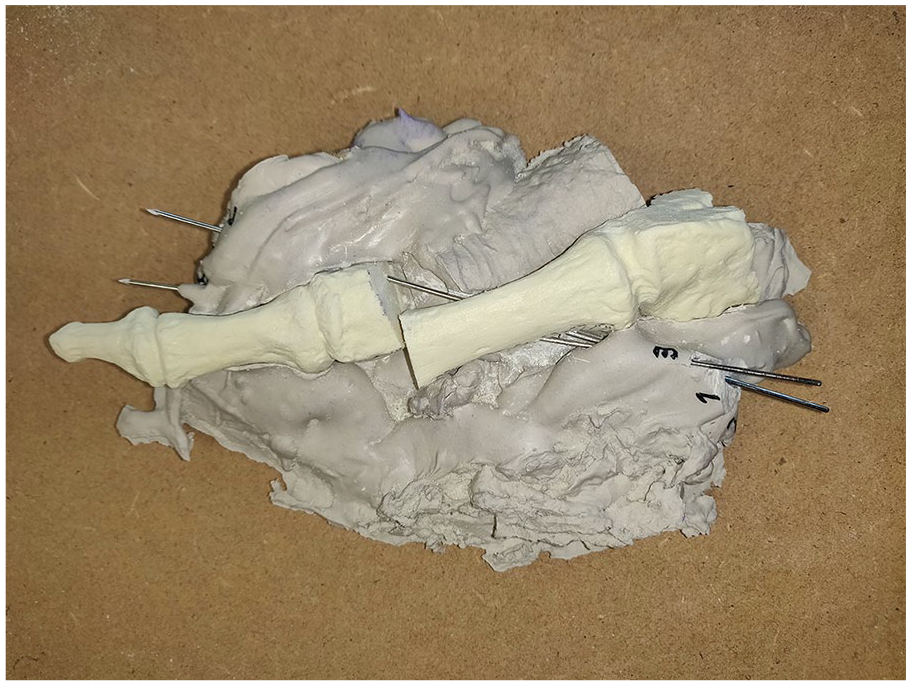
A hallux valgus model in a biomechanical cantilever configuration was used as described by Aiyer et al. 2 The first metatarsal base (embedded in PMMA) was fixed to a clamp to avoid dissipation of the force proximal to the osteotomy (Figure 4). Testing was performed on a Zwick-Roell universal testing machine. The compression post applied a preload of 10 N to stabilize the sample. A load to failure test was performed on 1 construct (pilot sawbone of group 2) to determine the cyclic load to be applied throughout the study.

Cantilever testing.
Variables were measured during the cyclic phase and the load to failure phase. Cyclic phase: in every construct, a cantilever test was applied at a rate of 1 mm/s using 100 N (50% of the failure load of the pilot test) for a total of 1000 cycles. Stiffness (newtons applied per millimeter of displacement) was measured for the cyclic testing. Load to failure phase: finally, a load to failure test was performed in cases that did not fail in the cyclic test measuring load to failure in newtons.
Specimen failure was defined as a dorsal displacement at the site of the osteotomy of 5 mm, >2 mm of metatarsal head rotation, fracture of the metatarsal, or implant breakage or loosening. The displacement and rotation were measured using a calibrated caliper taking consistent points on the models.
Statistical Analysis
Statistical analysis was performed with the SPSS software with the help of a statistician. Data distribution was evaluated, and analysis was performed using an analysis of variance. The statistical differences were considered with a P value <.05. The Bartlett test for equal variances was used to analyze the variability between specimens and group behavior.
Results
The Bartlett test showed that the variances were homogeneous (P = .002); thus, the groups were comparable. A post hoc power analysis was performed yielding a statistical power of 88%.
Under cyclic testing, group 1 failed because of rotational instability, therefore failing to complete the test. Groups 2 to 6 showed no failures in cyclic testing. Stiffness under cyclic load showed that group 1 was significantly weaker against all groups (P = .01). Group 2 was significantly weaker than groups 4 to 6 (P = .015). Using divergent screws (group 3 vs group 2) increased stiffness but did not achieve statistical significance (P = .08). Group 4 (lateral metatarsal head cortex purchase) showed a statistically significant increase in stiffness against group 3 (P = .03). Using two 4.0-mm screws (group 5) did not show differences against group 4 (P = .2). Finally, using two 3.5-mm screws (group 6) decreased the stiffness, making it only more resistant than group 2 (P = .01), but not significantly different from groups 3, 4, and 5 (P = .15) (see Table 1).
Biomechanical Resistance in Load to Failure Testing.

Groups 4 and 5 showed significant differences to all other groups in load to failure test, but not between them.
In the load to failure test, group 2 was significantly weaker than groups 4 to 6. Using divergent screws (group 3 vs group 2) increased the load to failure force but did not achieve statistical significance (P = .09) (181 N vs 131 N). Group 4 (lateral metatarsal head cortex purchase) showed a statistically significant increase in load to failure force against the previous groups (P = .02) (250 N). Using two 4.0-mm screws (group 5) did not show differences against group 4 (P = .1) (223 N). Finally, using two 3.5-mm screws (group 6) significantly decreased the load to failure force (193 N), making it only more resistant than group 2 (P = .01) but significantly weaker than groups 4 and 5 (P = .02) (see Table 1).
Regarding failures in the load to failure phase, in group 2, all specimens failed through implant loosening, ending in head rotation. In group 3, three of 5 specimens failed through implant loosening and 2 of 5 failed through proximal metatarsal breakage. In groups 4, 5, and 6, all specimens failed through proximal metatarsal fractures. See Table 2, Figures 5 and 6.
Failure Type per Group.

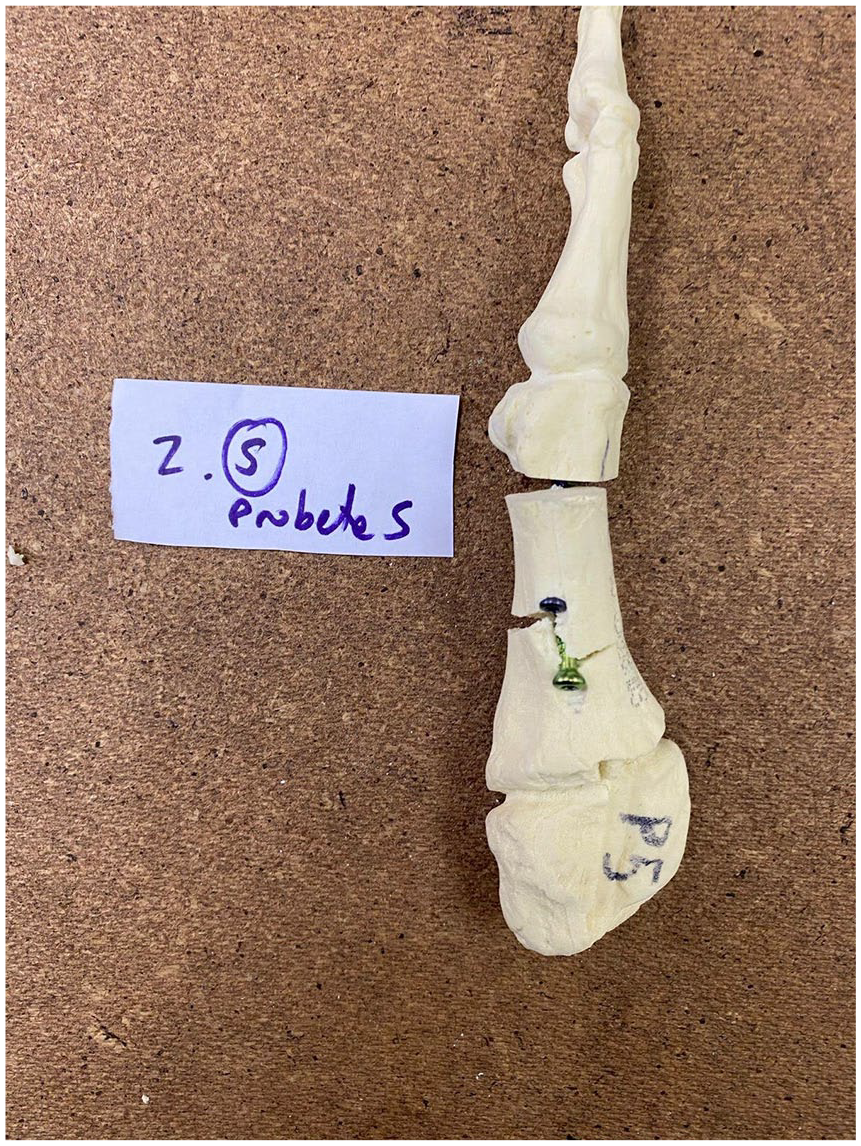
Metatarsal failure. A specimen failure is shown. Metatarsal fracture is evident at the proximal metatarsal.

Metatarsal failure. A specimen failure is shown. A fracture line is evident between both screws’ entrance.
Discussion
Minimally invasive surgical techniques have been used for many years, especially in Europe and Australia. It all started with minimally invasive surgical techniques that do not use fixation (eg, Reverdin-Isham), that progressively evolved to osteotomies (eg, Bosch) and using cannulated screws (eg, MICA).4,12,13,16,17 The current recommended fixation method is currently using 2 cannulated screws, but technical variations have not been evaluated and compared. Different screw sizes (eg, 3.0, 3.5, and 4 mm), screws number (1 or 2), and screw directions (parallel or divergent) have been used, but with no clear reason or evidence.
In this study, findings show that in this cantilever sawbone model, using 2 divergent screws, with the most lateral screw traversing the lateral metatarsal head cortex, is the most stable construct for first metatarsal cervical osteotomies.
The aim of this study was to compare the mechanical performance (stiffness and failure mode) of different screw configurations in a first metatarsal sawbone model where a cervical straight osteotomy was performed. This was evaluated in a cyclic and load to failure testing. This model tried to mimic the immediate weightbearing status frequently allowed for these techniques. It is interesting that divergent screws did not show a significant difference to parallel screws. Nevertheless, failures behaved differently between these groups. In group 2 (parallel screws), all failures occurred through implant loosening. In contrast, in group 3 (divergent screws), metatarsal breakage occurred in 2 of 5 specimens, which demonstrates a more rigid construct, but not achieving a statistically significant difference. This could be explained by the small working space available in the metatarsal, preventing a significant divergence between screws and not being enough to significantly increase stability. The other interesting finding is that there was no difference between two 4.0-mm screws and one 4.0- and one 3.0-mm screw. This could suggest that the proximal lateral screw is the one that yields mechanical stability and stiffness, and the distal medial screw mainly an antirotatory screw with less mechanical relevance. Finally, two 3.5-mm screws with lateral head purchase (group 6) are weaker than groups 4 and 5 (which use one 4.0-mm lateral screw), but are stronger that groups 2 and 3, which do not cross the metatarsal head cortex but use 4.0-mm screws. These findings suggest that screw diameter is less important than lateral head purchase. See Figure 7 for a clinical example for using a 4.0- and 3.0-mm screw with lateral first metatarsal head cortical purchase.

Radiographic example. An anteroposterior foot weightbearing radiograph showing a percutaneous extracapsular transverse cervical metatarsal osteotomy can be seen. Please note the following: lateral screw crosses the lateral head cortex; screws’ divergence; and different screw diameters (ie, 4.0- and 3.0-mm screws).
One of the limitations of this study is the use of sawbones, which do not hold similar physical properties to bone and lack soft tissues. Nevertheless, because what was being evaluated was only the mechanical performance of different screw configurations, the sawbone, being a constant variable, should not affect the study outcomes.
Having said this, given the difficulties to work with specimens with similar bone density, because the material used in this study was standardized, bone strength and quality can be ruled out as a confounding variable, and therefore only the screw configuration was tested and compared. In addition, direct patient extrapolation cannot be performed, and clinical trials are needed to evaluate its clinical significance. Finally, even though a reduced number of samples were used per group, the statistical analysis showed similar and reduced variances between groups, allowing safe comparison between them.
To the authors’ knowledge, this is the first published biomechanical study that assesses commonly employed implant constructs following percutaneous metatarsal cervical osteotomies for hallux valgus correction.
In this study, lateral head cortex purchase further optimized with a larger diameter on the lateral screw demonstrated improved performance. Although this finding has clear biomechanical reasoning, evidence is lacking. However, it is important to note that relevance for application may be dependent on patient anatomy and metatarsal diameter. Clinical studies are needed to apply these concepts in hallux valgus surgery and to evaluate the clinical impact of these findings.
Conclusions
The results of this study using foam-based surrogate first metatarsal bone models suggest the following: (1) 2 screws are required to maintain rotational stability of the construct; (2) relative screw orientation did not demonstrate an effect on construct stiffness; (3) lateral screw purchase of metatarsal head cortical bone is associated with a notable impact on construct stiffness; and (4) screw diameter increases stiffness.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241303768 – Supplemental material for Biomechanical Evaluation of Different Fixation Methods for Percutaneous Extracapsular Transverse Cervical Metatarsal Osteotomy in a Hallux Valgus Sawbone Model
Supplemental material, sj-pdf-1-fao-10.1177_24730114241303768 for Biomechanical Evaluation of Different Fixation Methods for Percutaneous Extracapsular Transverse Cervical Metatarsal Osteotomy in a Hallux Valgus Sawbone Model by Pablo Wagner, Emilio Wagner, Miguel Pinochet, David Salinas and Peter Lam in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval was not sought for the present study because it is a basic science study using sawbone models.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.