
Abstract
Background:
Recognizing preoperative first-ray hypermobility is important to planning hallux valgus (HV) surgery. A recent study showed the minimally invasive chevron Akin (MICA) osteotomy increased varus displacement of the proximal fragment of the first metatarsal osteotomy. The present study aims to evaluate the ability of the radiographic first-ray squeeze test to predict the varus displacement of the proximal fragment of the first metatarsal osteotomy when performing the MICA procedure.
Methods:
A prospective case series of patients with moderate to severe HV who underwent MICA was performed. The HV deformity correction was analyzed by comparing the preoperative and 12-week postoperative hallux valgus angle (HVA) and the intermetatarsal angle between the first and second rays (1-2 IMA). The ability of the radiographic first-ray squeeze test to predict the varus displacement of the first metatarsal was done by comparing the preoperative 1-2 IMA measured in the AP radiographic first-ray squeeze test (IMA-ST) with the intermetatarsal angle between the second metatarsal and the axis of the first metatarsal osteotomy proximal fragment (IAPF) taken 12 weeks postoperatively.
Results:
Between July 2022 and May 2023, a total of 39 feet in 28 patients underwent MICA. The mean IMA improved from 13.8 (SD = 2.2) to 3.8 degrees (SD = 1.5) (P < .001), and the mean HVA improved from 27.8 (SD = 6.1) to 4.9 degrees (SD = 2.5) (P < .001). A linear regression analysis revealed that IMA-ST is highly associated with the 12 week assessed IAPF (P < .001).
Conclusion:
The preoperative radiographic first-ray squeeze test appears to predict with high fidelity the varus displacement of the proximal fragment of the first metatarsal that can occur after the MICA procedure.
Keywords
Introduction
Minimally invasive chevron Akin osteotomy (MICA) is a versatile procedure for treating hallux valgus (HV).2,14 The technique is a third-generation minimally invasive surgery indicated for symptomatic mild to severe HV.9,26 Deformity correction is achieved through lateral first metatarsal head displacement associated with a medialization of the proximal fragment of the first metatarsal with rigid fixation done by 2 screws and Akin osteotomy.19,20,27,28 The medialization of the proximal fragment is variable and depends on the degree of the first-ray hypermobility (FRH). 17
The MIS third-generation procedure has become popular and widely used to correct severe HV deformities.5,12,13,16 The literature on HV in patients undergoing MICA shows significant radiographic corrections and patient outcomes.12,13,16 Despite this, there needs to be more literature on the limits to the indications for MICA. The indication is based on measuring the first intermetatarsal space and the size of the metatarsal head.20,27 The technique is contraindicated if more than 100% head lateral displacement is required to correct the intermetatarsal angle between the first and second rays (1-2 IMA).20,27 This measurement was described in an anteroposterior (AP) weightbearing radiograph and did not consider the FRH.
The instability of the first-ray is an important topic related to HV that has been widely discussed.22,24,25 The FRH is a consequence of the instability of midfoot joints, such as the first metatarsal cuneiform joint and intercuneiform joints.1,10 Unrecognized transverse plane instability contributes to a failure of procedures involving first metatarsal osteotomies.7,31 Nunes et al 17 demonstrated hypermobility in the transverse plane with increased varus displacement of the proximal fragment of the osteotomy in all patients that underwent MICA, suggesting that the medialization of the proximal fragment is part of the reduction maneuver of the technique and increases the first-ray stability by fixing the proximal fragment of the first metatarsal as medial as possible. Some specific maneuvers can demonstrate hypermobility in the transversal plane preoperatively by showing an increased 1-2 IMA.15,27,30 Vernois and Redfern 27 called this maneuver a squeeze test. The test involves squeezing the first metatarsal interspace using 1 or 2 fingers, which leads to increasing the 1-2 IMA. 27
The authors of this study hypothesize that a radiographic first-ray squeeze test can predict the varus displacement of the first metatarsal that occurs in the proximal fragment during the MICA procedure, thus predicting the amount of head lateralization necessary to correct the deformity.
This would be useful in preoperative planning for the MICA procedure, indicating how much correction can be achieved and how much bone contact can be expected. Our study aims to evaluate the change in 1-2 IMA on the radiographic first-ray squeeze test and compare this to the varus displacement of the first metatarsal that occurs in the proximal fragment after the MICA procedure.
Methods
Study Design
It is a prospective case series of consecutive patients with HV who underwent surgical correction using the MICA technique. The inclusion criteria were patients aged >18 years with isolated HV deformity, defined by 1-2 IMA >9 degrees or a hallux valgus angle (HVA) >15 degrees. 21 Exclusion criteria were patients with a previous history of foot surgery, osteoarthritis or inflammatory arthritis of the first metatarsophalangeal joint or the first metatarsal-cuneiform joint, and associated hindfoot, midfoot, and forefoot deformities who required additional procedures.
This single-surgeon series was performed at the Brasília Cote clinic. The operating surgeon had more than 8 years of experience with MIS using the MICA technique. Local ethics committee approval was granted for the current study, and the protocol followed the Declaration of Helsinki and the Guidelines for Good Clinical Practice. This study was reported in line with STROBE guidelines for reporting observational studies. 29
Radiographic Analysis
The radiographic outcome parameters were measured using a standard weightbearing foot anteroposterior view (AP) taken preoperatively and postoperatively at 12 weeks after the surgery and a radiographic first-ray squeeze test taken preoperatively. The AP was done with the beam centered to the base of the third metatarsal and angled 15 degrees posteriorly.
The measurements were done in a protocolized manner using the mechanical axis of the metatarsals.16,23 The radiographic first-ray squeeze test is a nonweightbearing foot AP image (radiographic beam centered to the base of the third metatarsal and angled 15 degrees posteriorly) in which the examiner’s thumb and forefinger apply direct pressure between the first and second metatarsal heads to increase the 1-2 IMA (Figure 1).15,27

(A) Clinical demonstration of the Squeeze test. (B) Radiographic Squeeze test view.
The HV deformity correction was analyzed by comparing the pre- and postoperative HVA and 1-2 IMA measured in a weightbearing AP view. The varus displacement of the first ray was done by comparing the preoperative 1-2 IMA with the intermetatarsal angle between the first-ray osteotomy proximal fragment and the second metatarsal (IAPF). 17 The ability of the radiographic first-ray squeeze test to predict the varus displacement of the first metatarsal was analyzed by comparing the 1-2 IMA measured in the preoperative AP first-ray squeeze test (IMA-ST) with the IAPF. The IAPF was measured in the 12-week postoperative weightbearing AP view (Figure 2).
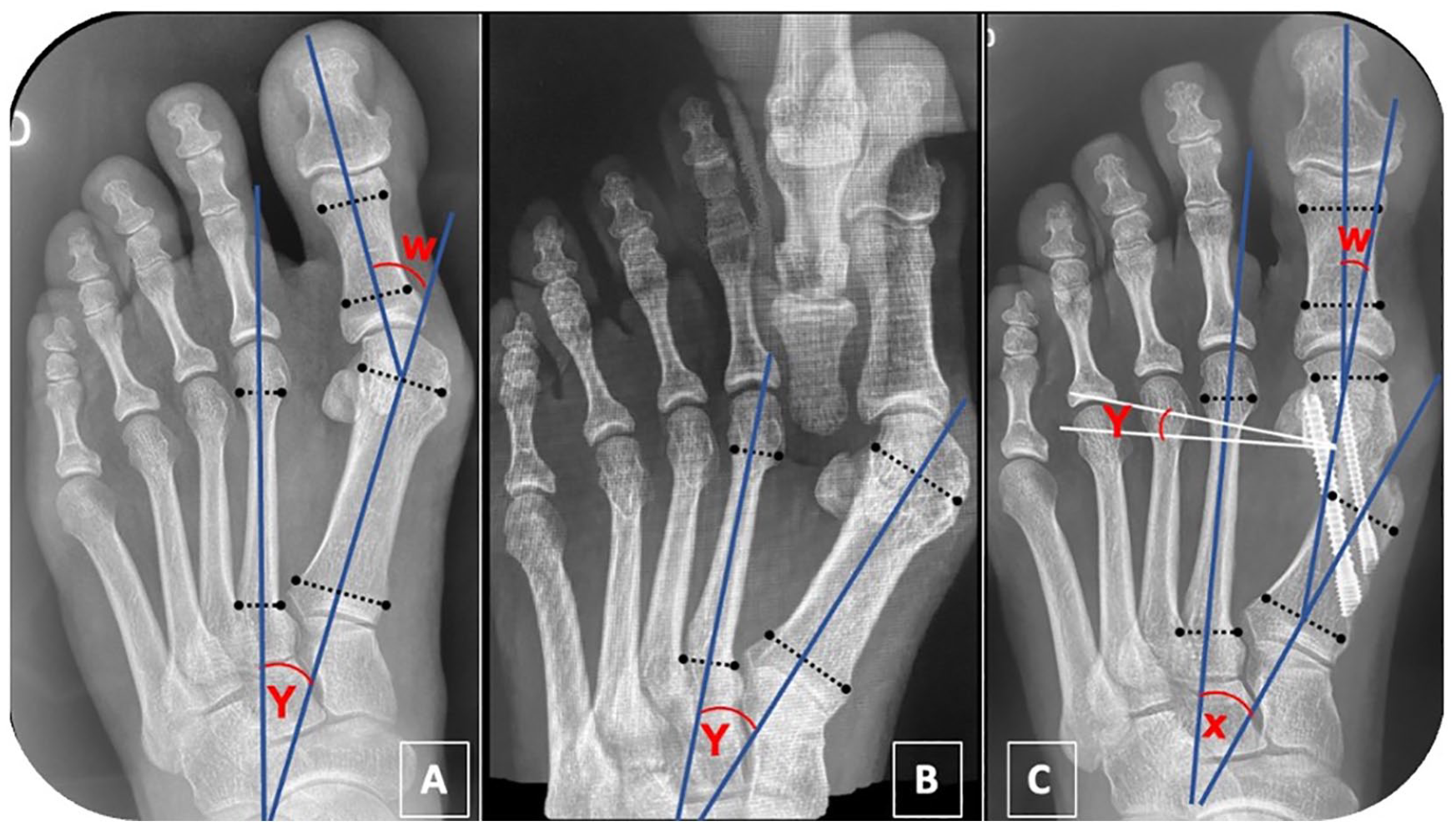
Radiographic parameters on the (A) preoperative weightbearing anteroposterior radiography, (B) preoperative radiographic Squeeze test, and (C) the 12-week postoperative weightbearing anteroposterior radiography. W, hallux valgus angle; Y, intermetatarsal angle between the first and second rays; X, intermetatarsal angle between the proximal fragment of the first metatarsal and the second ray.
The radiographic measurements were performed by 2 fellowship-trained surgeons not involved in the surgery using Carestream Vue Motion software according to the American Orthopaedic Foot & Ankle Society guidelines.4,21 Interrater reliabilities for continuous data were performed using interclass correlation coefficients.
Surgical Technique
The technique was performed as described by Redfern and Vernois.20,27 The equipment used was Beaver blade, periosteal elevator, rasps, 2 × 12 mm Shannon burr; 3.1 wedge, drill (dedicated, low-speed, high-torque, with handpiece), and C-arm fluoroscopy. The patients were positioned supine with both feet hanging from the end of the operating table by 6 inches, supported on the image intensifier detector. For the right-handed surgeon, the author prefers that the C-arm be positioned on the patient’s right side and the surgeon on the patient’s left side. 11
Using a beaver blade, an extracapsular portal at the distal metaphyseal-diaphyseal transition on the medial side of the first metatarsal was done. After that, a 2 × 12-mm Shannon burr was introduced at this point to perform the osteotomy. The osteotomy displacement plane was determined according to the orientation of the burr in the transverse and coronal planes. A chevron osteotomy was made in a “V” shape with an angle of approximately 130 degrees, with a dorsal cut parallel to the axis of the first metatarsal and a plantar cut in the proximal direction.
The next step was to place 2 guidewires for 4.0- and 3.0-mm cannulated chamfered screws. The guidewires were inserted, fixing only the proximal fragment. The proximal 4.0-mm guidewire passed through the medial and lateral cortex of the proximal fragment. The second guidewire was inserted in the same plane but slightly distal to the first screw.
Subsequently, a detacher was inserted in the medullary canal to lateralize the first metatarsal head and correct the deformity. After achieving the desired correction, the guidewires were progressed, fixing the metatarsal head, and 4.0-mm chamfered cannulated screws were inserted. The medial prominence of the proximal fragment of the metatarsal osteotomy was removed using a 2 × 12-mm Shannon burr through the proximal screw entry portal. 8
The release of lateral soft tissues (sesamoid-phalangeal ligament and lateral head of flexor hallucis brevis) was done in case of persistent incongruence of the metatarsophalangeal joint of the hallux or if the lateral sesamoid remained uncovered. It was evaluated intraoperatively with a simulated weightbearing fluoroscopic image.
Finally, the Akin osteotomy was performed using a 2 × 12 mm Shannon burr through medial access to the base of the proximal phalanx. The washing and removal of bone debris were performed with abundant saline irrigation.
Postoperative Protocol
Patients were allowed full weightbearing when discharged from the clinic using a rigid-sole orthopaedic shoe worn for 6 weeks. In the first 14 days after surgery, patients were instructed to keep their feet elevated above the level of the ipsilateral hip to minimize postoperative swelling. After the first week, the surgical dressing was replaced by Steri-Strips applied to the portals.
Thenceforth, the dressings were changed daily by the patients. Gentle exercises for the range of motion of hallux were introduced in the second week and intensified during the follow-up according to the patient’s progress. After the sixth week, the patients were allowed to wear conventional shoes with a wide toe box and a rigid sole.
Statistical Analysis
All statistical analysis was conducted using the R software’s Stats package. For categorical variables, we initially performed an analysis based on percentages, whereas continuous variables underwent assessments of minimum, maximum, median, mean, and SD. Additionally, we evaluated the distribution of continuous variables using the Shapiro test and employed the Wilcoxon signed-rank test for nonparametric distributions. We also performed a multivariate analysis using a linear regression model. Statistical significance was established at P <.05.
Results
Between July 2022 and May 2023, a total of 39 feet in 28 consecutive patients diagnosed with HV underwent primary MICA. All patients in this study were treated by a foot and ankle orthopaedic surgeon with >5 years of experience with MIS HV correction. There was no loss of any patient during follow-up. The sample included 28 patients, of which 11 were bilateral, totaling 39 feet. The mean age of the patients was 44.9 years; the majority were female (71.4%), and the left side (56.4%) was the most common. The radiographic results are represented in Table 1.
Results of Radiographic Evaluation.

Abbreviations: HVA, hallux valgus angle; IAPF, intermetatarsal angle of the proximal fragment; IMA, intermetatarsal angle.
IAPF – IMA.
Univariate Analysis
Preoperative 1-2 IMA × IAPF
A linear regression model analysis showed a statistically significant relationship (P < .001) between preoperative 1-2 IMA preoperative and IAPF. Additionally, the F statistic is significant (P < .001), supporting the overall significance of the model.
IMA-ST × IAPF
Univariate analysis revealed a significant and positive association between these 2 variables (P < .001). The overall fit of the model was significant, with an F statistic of 37.69 (P < .001) (Figure 3).

Linear regression analysis of the relationship between IMA-ST and radiographic measurements.
Multivariate Analysis
IMA-ST × IAPF
A linear regression analysis examined the relationship between IMA-ST and radiographic measurements (HVA preoperative, HVA postoperative, IMA preoperative, IMA postoperative, and IAPF) (Figure 4).
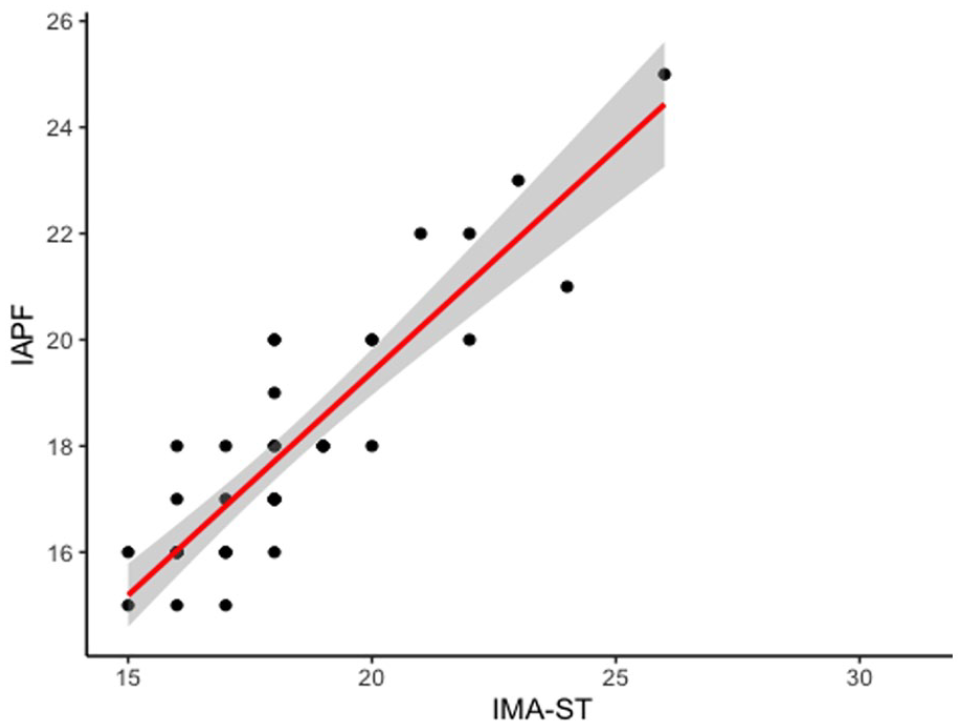
Univariate analysis between the preoperative intermetatarsal angle between the first and second rays measured in the radiographic first-ray Squeeze test (IMA- ST), with the intermetatarsal angle between the second ray and the axis of the first metatarsal osteotomy proximal fragment (IAPF) showing a significant and positive association between these 2 variables.
Discussion
The most important finding of this study was to demonstrate a statistically significant association between the IMA-ST and the IAPF. These findings suggest that the radiographic squeeze test appears to be reliable for predicting the varus displacement on the proximal fragment of the first metatarsal after the MICA procedure.
Univariate analysis revealed a significant and positive association between IMA-ST and IAPF. This implies that an increase in IMA-ST is strongly associated with a corresponding increase in IAPF. The F test revealed an extremely low value, indicating the robustness of this relationship and reinforcing the idea that IMA-ST is a significant and relevant predictor for IAPF. These results reflect a bidirectional relationship between the 2 variables, highlighting their interdependence. The univariate analysis between the preoperative 1-2 IMA and IAPF also demonstrated a significant and positive association. The estimated coefficient for the preoperative 1-2 MA suggests that for each unit increase in preoperative 1-2 IMA, there is an average increase of 0.6625 in IAPF. The R-squared value of 0.419 implies that approximately 41.9% of the variability in IAPF can be explained by the preoperative 1-2 IMA. A multivariate analysis examined the relationship between IMA-ST and radiographic measurements (HVA preoperative, HVA postoperative, 1-2 IMA preoperative, 1-2 IMA postoperative, and IAPF). Among these variables, only IAPF demonstrated a statistically significant association with IMA ST (P < .001). These findings underscore the significance of IMA ST as a predictive test for IAPF and emphasize the nuanced relationships within the examined variables. IMA-ST and postoperative HVA have not been found to have a relationship in this multivariate analysis. Therefore, we believe that a study with greater follow-up could reveal this association.
The FRH is an important factor related to HV deformity etiology, severity, and recurrence. Understanding the role of FRH in HV is critical to the successful surgical treatment of this deformity.10,25 The transversal plane was related to an increased 1-2 IMA, suggesting a connection between this hypermobility and metatarsus primus varus.7,15,29,30 Palladino 18 emphasized a preoperative assessment of the transversal plane of the first metatarsal-cuneiform joint. He settled that the gapping present between the metatarsal bases should be less than 2 mm.
Based on the concept that the varus displacement of the proximal fragment increases the IAPF when performing MICA, 17 the authors of this study used the preoperative radiographic first-ray squeeze test to analyze the 1-2 IMA and assess whether this test could predict the severity of instability of the first ray and if this reflected the final deformity correction.
MICA has become a widespread technique in recent years.12 -14 It is a versatile procedure correcting mild to severe deformities according to the amount of the first metatarsal head lateralization. 5 Several studies of patients with severe HV treated by this procedure have recently been published, demonstrating promising clinical and radiographic results with a similar recurrence rate to other techniques.12 -14 However, these studies have not established the potential limitations of this procedure concerning first-ray instability.
Lewis et al 13 described a series of 53 severe HV (HVA >40; IMA >20), with a mean of 3 years’ follow-up, that underwent percutaneous chevron akin osteotomy (PECA). They reported a higher mean deformity radiographic correction using the MIS technique than in the general literature, with a mean HVA and 1-2 IMA correction of 12.4 and 32.5 degrees, respectively. Nevertheless, 24.5% of patients had insufficient correction with a residual HV. 13 They attributed this rate of HV residual to an incomplete correction at the time of surgery due to the initial severity of the deformity. We believe the radiographic squeeze test can help surgeons better plan for the appropriate technique in preoperative large–1-2 IMA cases with excessive first-ray instability. A Lapidus arthrodesis may be the most suitable treatment for these cases.
Establishing the limits of any procedure is very important. According to the literature, this procedure may be contraindicated if 100% of head lateral displacement is insufficient to correct the 1-2 IMA.20,27 This evaluation considers the size of the metatarsal head and the 1-2 IMA. As this measurement was described in an anteroposterior (AP) weightbearing radiograph, it does not consider the FRH. Based on the findings of this study, we recommend using IMA-ST instead of IMA to redefine the limits of MICA. We suggest a Lapidus arthrodesis when the first metatarsal head size is smaller than the space between the first and second metatarsal in an IMA-ST radiographic incidence. It is necessary to conduct additional research to explore the significance of these findings in a clinical context.
Nunes et al 17 analyzed 50 cases of MICA, demonstrating some degree of hypermobility in the transverse plane with increased varus displacement of the proximal fragment of the osteotomy in all cases. They stated that this mechanism would lock the first ray in a maximum medial position, stabilizing the transverse plane and reducing the recurrence risk. We believe there is a limit to this mechanism because the degree of first-ray instability varies significantly and can be unpredictable without a preoperative assessment.
Cody et al 3 showed a comparative study between MICA and Lapidus. They observed some cases with a progressive medialization of the proximal fragment of the osteotomy with a recurrence of the deformity in the MICA group. 3 These controversies make it clear that we should work on a common standard regarding the indication of the technique and investigate the long-term effects of this increased varus displacement on the proximal fragment.
The ability of the radiographic first-ray squeeze test to anticipate how much shift will be achieved intraoperatively and the true potential 1-2 IMA may also be helpful for planning the MICA for those HV cases with a narrow 1-2 IMA. Performing MICA in mild deformities with a narrow 1-2 IMA can be challenging, as there is not enough space to put the proximal screw properly. Predicting this situation can be an advantage for the surgeon. These cases can require another procedure, such as a percutaneous intracapsular osteotomy 6 or an open chevron osteotomy. Another option is using specific jigs to assist the screw positioning in the MICA procedure.
To our knowledge, this is the first study in the literature focused on analyzing MICA’s limits and proper indications. This study proposed the radiographic first-ray squeeze test as a valuable tool for clarifying the MICA indications and planning the procedure. The ability of this test to predict the varus displacement of the first metatarsal is important to show the severity of the first-ray instability in the transverse plane in severe HV, clarifying the limits of the technique. Additionally, it assists the surgeons in planning the correction of mild HV with a narrow 1-2 IMA. Studies like this are essential to make the technique safer and more predictable.
This study has several limitations. First, the force performed in the first-ray squeeze test was not standardized, making this maneuver subjective. Additionally, each patient has a different degree of instability, so the force required to medialize the first metatarsal can differ. Despite that, the varus displacement of the proximal fragment was similar to what occurred during the squeeze test, and the radiographic test was done by the same author, reducing the risk of bias per examiner. Second, a longer follow-up would be necessary to reinforce the results of this research. Finally, no clinical evaluation of the patients was carried out.
Conclusion
The findings of this study confirm the authors’ hypothesis. The preoperative radiographic first-ray squeeze test appears to reliably predict the varus displacement of the proximal fragment of the first metatarsal that can occur with the MICA procedure.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241239331 – Supplemental material for Minimally Invasive Chevron Akin Osteotomy: Preoperative Planning Using the Radiographic First-Ray Squeeze Test
Supplemental material, sj-pdf-1-fao-10.1177_24730114241239331 for Minimally Invasive Chevron Akin Osteotomy: Preoperative Planning Using the Radiographic First-Ray Squeeze Test by Gustavo Araujo Nunes, Gabriel Ferraz Ferreira, Miguel Viana Pereira Filho, Kepler Alencar Mendes de Carvalho, Thomas Lorchan Lewis, Jorge Castellini, Robbie Ray and Joel Vernois in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Bioethics Committee of Medical Institution, CAAE (Ethics Evaluation Submission Certificate) number 16213319.8.0000.5122. Informed consent was obtained from all individual participants included in the study. The authors affirm that human research participants provided informed consent to publish the images in figures. The participant has consented to the submission of this case series to the journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.