
Abstract
Background:
Hallux valgus (HV) is a common cause of pain and deformity of the forefoot. Minimally invasive chevron Akin (MICA) bunionectomy is a method for HV correction associated with less pain and swelling, with early return to weightbearing in a regular shoe. The purpose of this study was to determine how the MICA procedure affects forefoot width.
Methods:
Twenty-eight patients (26 female, 2 male; 9 left, 19 right) at a single institution who underwent primary MICA for HV correction by 3 treating surgeons were retrospectively reviewed. Pre- and postoperative hallux valgus angle (HVA), intermetatarsal angle (IMA), distal metatarsal articular angle (DMAA), bony forefoot width, and soft tissue forefoot width were measured by 2 independent observers. Radiographic measurements were calibrated using fifth metatarsal length. Wilcoxon signed rank test compared changes in HVA, IMA, DMAA, and forefoot widths. Pearson correlation coefficient evaluated association between HVA, IMA, DMAA, and changes in forefoot width.
Results:
At mean follow-up of 5.4 (range 3-13.7) months, bony forefoot width decreased significantly by 3.7 mm (4%, P < .001) and soft tissue forefoot width decreased by 2.5 mm (2%, P < .01). Decrease in HVA was moderately correlated with change in bony forefoot width (r = .38, P < .05) and change in soft tissue forefoot width (r = .45, P < .05). Decrease in IMA was moderately correlated with change in bony forefoot width (r = .45, P < .05) and change in soft tissue forefoot width (r = .44, P < .05).
Conclusion:
The MICA procedure resulted in modest, yet significant, decrease in both bony and soft tissue forefoot width. Decrease in HVA and IMA demonstrated moderate correlation with changes in forefoot width. Patients can be counseled on these changes leading up to, and after, MICA bunionectomy surgery.
Level of Evidence:
Level III, retrospective comparative series.
Introduction
Hallux valgus (HV) adversely affects patients’ quality of life by causing difficulty with pain, cosmesis, and shoe wear. Minimally invasive surgical (MIS) techniques for correction of HV deformity, specifically the minimally invasive chevron Akin (MICA) bunionectomy, have recently fallen into favor by providing adequate bony and soft tissue correction through small percutaneous incisions with minimal soft tissue and periosteal disruption.2,14,15,24 The limited surgical dissection imposed during MIS procedures results in less soft tissue swelling, lower pain scores, and less stiffness following surgery.1,9
Patient satisfaction following HV correction surgery is related to foot appearance and shoe wear capabilities, among other variables. 7 Recently, 5 studies have investigated how forefoot width is affected by bunionectomy for HV correction. Conti et al 3 used weightbearing computed tomography (CT) scan to show that both bony and soft tissue foot width decreased significantly following the modified Lapidus procedure for bunionectomy. Vaida et al 23 expanded on this to measure foot width following triplanar tarsometatarsal arthrodesis for HV correction. Tenenbaum et al 22 showed that overall foot width decreased by only 2% following scarf osteotomy. Jung et al 12 found that bony forefoot width decreased on average by 16% following distal soft tissue procedure, proximal first metatarsal osteotomy with medial eminence resection and Akin osteotomy of the proximal phalanx. Lastly, Panchbhavi et al 17 demonstrated a difference in bony forefoot width of 8.7 mm following distal chevron Akin bunionectomy. All 4 of these studies used open surgical techniques for their HV correction.
Foot width is an important part of the patients’ ability to fit into certain types of shoes with varying toe box designs. Between 34% and 60% of patients undergoing HV correction attribute ill-fitting shoe wear to their condition.4,5 Establishing evidence on forefoot width following MIS bunion surgery will allow surgeons to better manage perioperative patient expectations when offering them a MICA for HV correction. The literature surrounding MIS HV correction is rapidly growing, but few studies have evaluated foot width following MICA surgery. For example, Neufeld et al 16 found that bony width significantly decreased on average by 5.2 mm and soft tissue foot width decreased on average by 4.0 mm in 94 patients following MICA surgery. However, unlike the current study, their surgical technique implemented medial eminence resection with a combination of side cutting Shannon burr and a rasp. The purpose of this study was to radiographically quantify how forefoot width changes following MICA bunionectomy. The authors hypothesized that forefoot width would significantly decrease following MICA bunionectomy. Furthermore, we hypothesize that changes in angular parameters, hallux valgus angle (HVA), intermetatarsal angle (IMA), and distal metatarsal articular angle (DMAA), all would be correlated with changes in forefoot width.
Materials and Methods
A retrospective chart review of 40 patients (40 operative feet) who underwent MICA bunionectomy for symptomatic HV by 3 fellowship-trained orthopaedic foot and ankle surgeons at a single academic institution between March of 2020 and January of 2022 was performed. Approval for the study was obtained from our institutional review board committee. Included subjects had adequate preoperative and postoperative anteroposterior weightbearing foot radiographs, were at least 18 years of age, and had a minimum of 3-month clinical follow-up. Patients were excluded from analysis if they underwent concomitant procedures that could affect forefoot width (such as fifth metatarsal osteotomy) or demonstrated loss of reduction of their osteotomy site during follow-up. Twelve patients were excluded from analysis based on these criteria: 1 patient who underwent concomitant fifth metatarsal osteotomy and 11 patients who were lost to follow-up prior to 3 months. Twenty-eight patients (28 operative feet) were included for final analysis.
Operative Technique
The MICA technique used (Figure 1) is a third-generation modification of the percutaneous description popularized by Vernois and Redfern, 24 and has been well described in several previous studies.2,13,16,21 Under miniature C-arm image intensification, a 2 × 20-mm Shannon burr (Wright Medical Group, Memphis, TN, USA) was used to create an extracapsular chevron osteotomy of the distal first metatarsal. When performing the osteotomy, 2 of the 3 treating surgeons aimed the trajectory of the burr orthogonal to the axis of the second metatarsal shaft, while the third treating surgeon aimed the burr slightly distal toward the second metatarsal head. The metatarsal head was then translated laterally to narrow the intermetatarsal angular deformity and was fixed with a 4.0- and 3.0-mm MICA (Wright Medical Group) chamfered screw. Any remaining prominent proximal medial metatarsal shaft was resected with a side-cutting-wedge burr in a medial to lateral direction. Following the first metatarsal osteotomy, a percutaneous Akin osteotomy was performed in a similar fashion and fixed with a 3.0-mm MICA (Wright Medical Group) chamfered screw. When indicated, a beaver blade was used to perform a percutaneous release of the lateral metatarsophalangeal joint capsule and adductor hallucis tendon.

Example preoperative (left) and postoperative (right) anteroposterior weightbearing foot radiographs demonstrating minimally invasive chevron/Akin bunionectomy.
Patients were allowed to heel weightbear in a postoperative sandal for the first 4 weeks following surgery. Full weightbearing to tolerance in a postoperative sandal during weeks 4-6 was enforced before allowing patients to weightbear in a regular shoe at 6 weeks. All patients were transitioned to accommodative athletic shoe wear with stiff soles at the 6-week postoperative visit if swelling allowed.
Radiographic Analysis
Radiographic measurements were performed independently by 2 masked orthopaedic surgeons who were not involved with the surgical procedures. Measurements were performed on preoperative weightbearing anteroposterior radiographs and most recent follow-up postoperative weightbearing anteroposterior radiograph. Images were analyzed using our institution’s picture archiving and communication system (PACS, 20/20 imaging; OpalRad, Crystal Lake, IL).
Angular measurements of HV deformity included HVA, IMA, and DMAA. In accordance with the American Orthopaedic Foot & Ankle Society ad hoc committee on angular measurements, all radiographic measurements were conducted using standard first and second metatarsal reference points. 6 Forefoot width was assessed by measuring both the bony width and soft tissue width (Figure 2) in a similar fashion to previously published literature on forefoot width following scarf and Lapidus procedures.3,22
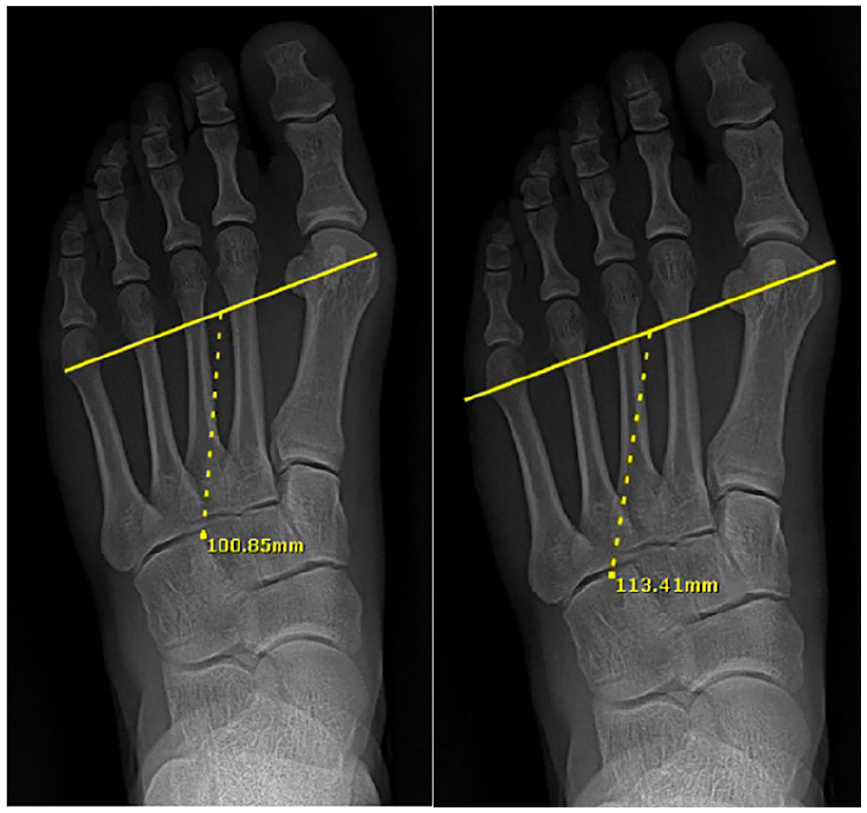
Example bony width (left) measurement and soft tissue width (right) measurements.
To account for possible variation in image magnification between preoperative and postoperative radiographs, a calibration factor was calculated by measuring the length of the fifth metatarsal from the most distal point of the articular head to the most proximal point on the base of the tuberosity. As similarly described in radiographic studies by Tenenbaum et al 22 (who used second metatarsal length) and Foran et al 8 (who used fifth metatarsal length), by calculating the ratio of fifth metatarsal length between the pre- and postoperative radiographs, we were able to compensate for small discrepancies in width caused by differing angles and magnification at which the radiographs may have been taken.
Statistical Analysis
Intraclass correlation coefficients (ICCs) were calculated to measure agreement between the 2 independent observers. For all radiographic parameters, an average between the 2 observers was calculated. Because of the small sample size, nonparametric statistical tests were implemented. Wilcoxon signed rank test was used to compare differences between pre- and postoperative HVA, IMA, DMAA, bony width, and soft tissue width. Pearson correlation coefficient was calculated to determine if HVA, IMA, and DMAA were at all associated with bony and soft tissue widths. Significance was set at .05. SPSS version 28.0.1.1 (SPSS, Inc, an IBM Company, Chicago IL) was used to perform all statistical calculations and analyses.
Results
Demographic data are displayed in Table 1. There were twenty-eight patients (26 female, 2 male; 9 left, 19 right), with an average follow-up of 5.4 ± 2.7 (range 3-14) months. The mean age of the patients was 46.6 ± 15.5 (range 18-78) years. All patients received both the minimally invasive chevron and Akin osteotomies as described above.
Patient Demographic Data.

Abbreviation: BMI, body mass index.
ICCs demonstrated at least good (>0.5) interobserver reliability for all measured radiographic variables. All pre- and postoperative foot width radiographic parameters demonstrated at least excellent (>0.9) interobserver reliability (Table 2).
Average Measure Intraclass Coefficients for Foot Width Measurements and Angular Parameters.
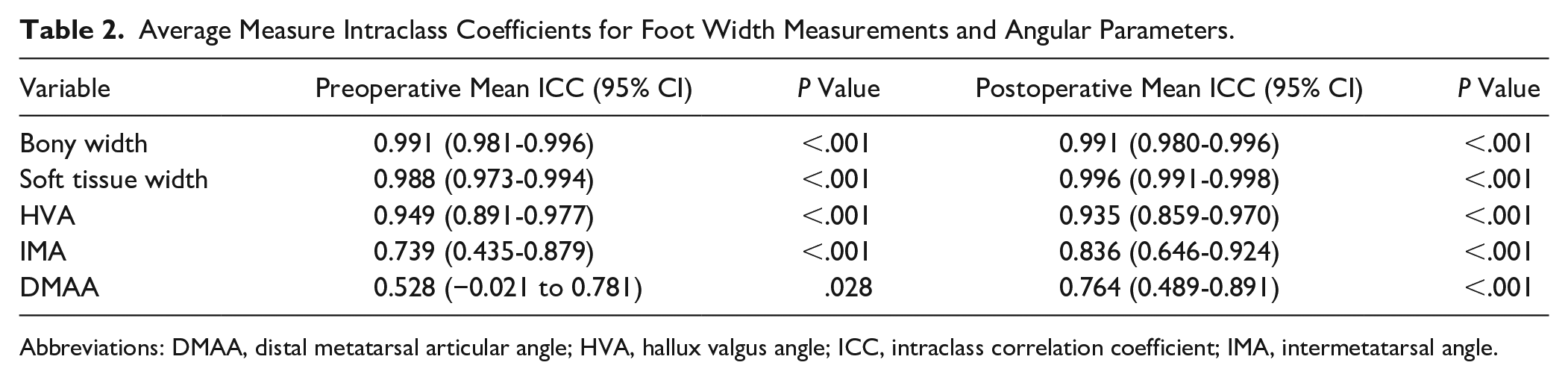
Abbreviations: DMAA, distal metatarsal articular angle; HVA, hallux valgus angle; ICC, intraclass correlation coefficient; IMA, intermetatarsal angle.
Pre- and postoperative angular parameters of HV deformity are shown in (Table 3). The average preoperative and postoperative HVA were 26.3 ± 7.2 degrees and 10.3 ± 8.1 degrees, respectively (P < .001). The average DMAA was 9.1 ± 6.20 degrees preoperatively and decreased to 2.1 ± 8.4 degrees postoperatively (P < .001). IMA averaged 11.7 ± 2.1 degrees preoperatively, which decreased to 4.3 ± 2.9 degrees postoperatively (P < .001).
Radiographic Angular Parameters of Hallux Valgus.

Abbreviations: DMAA, distal metatarsal articular angle; HVA, hallux valgus angle; IMA, intermetatarsal angle.
Bony width decreased in 25/28 patients (89%), from an average of 99.8 ± 9.4 mm (range 87.2-121.8) preoperatively to an average of 96.1 ± 9.6 mm (range 79.1-118.4, P < .001) postoperatively (Table 4). This represents a mean 3.7-mm (4%) decrease in bony forefoot width. Soft tissue width decreased in 22 of 28 patients (79%), from an average of 111.7 ± 10.1 mm (range 97.5-134.5) preoperatively to an average of 109.2 ± 10.1 mm (range 89.9-129.8) postoperatively (P < .01) (Table 4). This change represents a mean 2.5-mm (2%) decrease in soft tissue forefoot width.
Correlations Between Angular Parameters and Forefoot Width.

Abbreviations: HVA, hallux valgus angle; IMA, intermetatarsal angle.
P < .05. **P < .001.
Preoperative HVA was correlated with both preoperative bony width (r = 0.558, P = .002) and preoperative soft tissue width (r = 0.585, P = .001), whereas postoperative HVA was positively correlated with both postoperative bony width (r = 0.574, P = .001) and postoperative soft tissue width (r = 0.608, P < .001). Change in HVA was correlated with change in bony width (r = 0.379, P = .047) and change in soft tissue width (r = 0.453, P = .015). Change in IMA correlated with change in bony width (r = 0.448, P = .017) and soft tissue width (r = 0.437, P = .02). DMAA was not correlated with pre- or postoperative foot widths, nor was change in DMAA correlated with changes in foot widths (Table 5).
Average Forefoot Width Measurements Following MICA Bunionectomy.

Abbreviation: MICA, minimally invasive chevron Akin.
Discussion
The study found that bony and soft tissue radiographic forefoot width decreased by 4% and 2%, respectively, following MICA bunionectomy, thus confirming the study hypothesis. As the literature surrounding MIS techniques continues to grow, these study findings are an important validation of early transition into shoe wear following MICA bunionectomy. The angular parameters HVA and IMA were correlated with changes in foot width whereas DMAA was not. This information will allow surgeons to hold informed discussion when counseling patients on outcomes and expectations following the MICA procedure.
Forefoot width is an important radiographic factor before and after HV corrective surgery as it plays a role in both foot aesthetics and shoe wear capabilities.7,19,20 Prior studies have shown that between 93% and 100% of patients following MICA bunionectomy rated their outcome as excellent or good.10,16
Similar to the work by Conti et al 3 on CT foot width following the modified Lapidus procedure, our results demonstrate that both HVA and IMA play an important role in contributing to forefoot width. Change in HVA was moderately correlated with change in bony width (r = 0.379) and change in soft tissue width (r = 0.453). Change in IMA also moderately correlated with change in bony width (r = 0.448) and soft tissue width (r = 0.437). Our study went on to examine the effect of DMAA on forefoot width, which did not yield a correlation. DMAA is a measure of distal first metatarsal head orientation with respect to the first metatarsal axis, it comes as no surprise that it does not play a role in driving forefoot width. A narrowing of the IMA and decrease in HVA is achieved during the MICA procedure as lateral translation of the distal chevron osteotomy occurs. This effectively alters the mechanical axis of the first metatarsal shaft by shifting it laterally, more parallel to that of the second metatarsal axis.
Bony and soft tissue width changed by 3.7and 2.5 mm, respectively, in the current study. When taking into account that women’s shoe width size differs by about 10 mm between sizes and men’s shoe width size differs by about 5 mm, 11 the study findings do not suggest MICA procedure for hallux valgus creates enough change to alter shoe size. Moreover, the changes reported in this investigation are lower than what is reported by prior studies investigating foot width following hallux valgus correction (Table 6). With regard to foot width changes following various types of proximal first metatarsal procedures published in the literature (ie, Lapidus procedure, proximal chevron osteotomy), the results of the current study do not appear to be as powerful in decreasing width. Conti et al 3 demonstrated that bony foot width decreased after Lapidus procedure with Modified McBride and Akin osteotomy by 8.9 mm on radiographs and 7.9 mm on weightbearing CT scans in 31 feet. This is comparable to Vaida et al 23 who showed a reduction in bony forefoot width by 10.4 mm and reduction in soft tissue width by 7.3 mm following Lapidus procedure with Modified McBride soft tissue release. Jung et al 12 analyzed 118 feet that underwent proximal reverse chevron osteotomy and Akin osteotomy through a single medial incision and demonstrated that mean bony width decreased by 16 mm at final follow-up.
Change of width describe in the literature with different techniques.

Abbreviations: XR, radiography; WBCT, weightbearing computed tomography; MICA, minimally invasive chevron/Akin.
With regard to foot width changes following distal first metatarsal osteotomies (scarf, open chevron/Akin, and MICA), the outcomes of the current study and what is published in the literature vary in their comparisons. Tenenbaum et al 22 examined 71 feet treated with scarf osteotomy and found that bony foot width decreased on average by 5% and soft tissue foot width decreased by 2%. This is comparable to the mean 4% bony width decrease and 2% soft tissue width decrease observed in the current study. More notably, the Tenenbaum et al 22 study found that nearly one-fifth (18.3%) of their study subjects experienced an increase in foot width following scarf osteotomy. Panchbhavi et al 17 studied 52 patients who underwent open distal chevron/Akin osteotomy and found reduced radiographic bony forefoot width by an average of 8.7 mm. A recent study by Neufeld et al 16 reported on foot width following third-generation MICA technique in 94 feet. Their findings indicate a bony width decrease of 5.3 mm and soft tissue width decrease of 4.0 mm. Unlike the current study, their surgical technique implemented medial eminence resection with a combination of side-cutting Shannon burr and a rasp.
In addition to the Neufeld et al 16 study, the current study is the second investigation to our knowledge that has studied forefoot width following MIS hallux valgus correction. There are several differences worth noting between the 2 studies. The current investigation used 2 masked reviewers, neither of whom were any of the 3 treating surgeons, whereas the Neufeld et al 16 study did not specify how many reviewers and came from a single surgeon patient cohort. Additionally, the Neufeld et al 16 study group was a much larger sample (94 feet vs 28 feet) and carried a longer mean follow-up time (11.4 months vs 5.4 months). Despite this, our cohort demonstrated similar changes in bony width (5.5 mm vs 3.7 mm) and soft tissue width (4.0 mm vs 2.7 mm). These minor differences can potentially be explained by the additional medial eminence resection performed in their study and the longer follow-up period allowing for additional soft tissue swelling subsidence. Lastly, the current investigation used radiographic calibration to account for slight variation in image magnification between preoperative and postoperative radiographs.
The current study defined the measurement points for bony forefoot width as the most distal/medial point on the first metatarsal head and the most lateral point on the condyle of the fifth metatarsal head (Figure 2). This is similar to how forefoot width has been historically measured. 18 Tenenbaum et al, 22 Vaida et al, 23 Jung et al, 12 and Panchbhavi et al 17 used the same reference points as the current study to measure bony width; however, other prior studies have used varying bony landmarks, such as the base of the proximal phalanx or the medial aspect of the proximal metatarsal shaft.3,16 The decision was made to keep the same 2 reference points for each study subject in the interest of consistency and reproducibility. Additionally, if the foot width measurement reference points on the distal first metatarsal and distal fifth metatarsal head vary by shifting distally or proximally between subjects, then falsely elevated or falsely lowered width measurements could be obtained.
The authors propose a few explanations for why foot width did not decrease as substantially in the current study when compared to prior literature. First, most of the previously described techniques for Lapidus, open distal chevron/Akin, and proximal reverse chevron osteotomy involve some variation of resection of the medial eminence. The MICA technique described by Neufeld et al 16 utilizes a 2 × 20-mm Shannon burr to remove any prominence off the distal metatarsal head. This is a step that our technique does not routinely perform, out of fear for weakening the medial capsule, and relies solely on the lateral translation of the distal first metatarsal head to alter the metrics of the forefoot span. Lastly, postoperative soft tissue width is understandably correlated with the amount of postoperative swelling present. In some instances, foot swelling may persist up to a year following elective foot and ankle surgery. 14 Thus, the relatively short mean follow-up time of 5.4 months may have falsely elevated the postoperative soft tissue width measurements and as a result decreased the amount by which the soft tissue width narrowed following the MICA procedure.
The current study has several limitations. The first is the loss of follow-up of 11 of the 40 eligible patients. The small sample size and retrospective nature of the investigation come with their built-in drawbacks and pose a block to study generalizability. However, 3 treating surgeons who are at various stages of their MIS learning curves and who have small differences in their surgical technique, operative indications, and postoperative protocols does make the conclusions more generalizable. As mentioned above, the short-term follow-up does not provide enough time for foot swelling to completely resolve. However, the authors do feel that drawing conclusions based on minimum 3 months of follow-up is noteworthy as this is around the time frame that most HV patients would expect to return to regular shoe wear. Our inability to compare radiographic foot width changes with CT scans as well as correlate the changes with patient outcome scores is something that future work may be dedicated toward.
Conclusion
Foot width following MICA bunionectomy significantly decreases, but to a lesser extent than what is reported from other open HV corrective techniques. Decrease in HVA and IMA demonstrated moderate correlation with changes in forefoot width. Change in DMAA did not demonstrate any correlation with changes in forefoot width. Patients may be counseled on these expected changes leading up to, and after, MICA bunionectomy surgery.
Footnotes
Ethical Approval
Ethical approval for this investigation was obtained from the Rush University Institutional Review Board (protocol no. 22012701).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.