
Abstract
Keywords
Introduction
Although the most prevalent cause of degenerative changes in the hips is osteoarthritis, other etiologies that can affect both hips include rheumatoid arthritis, developmental dysplasia of the hip, slipped capital femoral epiphysis, and avascular necrosis. Among the most popular orthopedic operations, total hip arthroplasty (THA) is a very successful treatment for degenerative joint conditions.1,2 However, literature has shown that up to 42% of patients report having bilateral symptoms. Of patients with bilateral symptoms who undergo unilateral THA, as many as 97% of them will ultimately require a contralateral THA in their lifetime.3–5 Interestingly, in individuals with bilateral hip disease, functionality remains decreased until both hips have been replaced, even with one already repaired. 6
Simultaneous bilateral total hip arthroplasty (sbTHA) has been demonstrated to be an excellent option for patients with bilateral hip disease who are fit medically. 4 Previous studies have shown a higher risk of transfusion, but no increased risk for reoperation, revision, or complications.4,7,8 As well, sbTHA has been reported to decrease the inpatient cost of hospitalization between an estimated 15% to 27%.4,9 The direct lateral (DL), or Modified Hardinge, approach has been the most common approach across much of Canada for years. More recently, the direct anterior (DA) approach has become popular while claiming a faster recovery, positioning that facilitates the use of intraoperative fluoroscopy, and a more seamless transition from one hip to the other if performing sbTHA.10,11 To our knowledge, no previous studies have compared differences in patient-reported outcome measures (PROM) and costs of sbTHA performed via the DA or DL approaches.
The purpose of this study was to compare functional recovery and costs when performing sbTHA via DA or DL approach. Previous data from our center have demonstrated improved costs with unilateral THA via the DA approach as compared to the DL approach; 12 therefore, we predict improved function and lower costs for those undergoing simultaneous bilateral THA via the DA approach.
Methods
Study design
This single-center study was conducted at a tertiary care center. We performed a retrospective cohort analysis using our institution's arthroplasty database to identify all patients who underwent sbTHA between 2006 and 2020. We included patients who underwent sbTHA with either a DA or DL approach and had a clinical follow-up of at least 1 year. A matched cohort of patients who underwent sbTHA was established based on age and sex. The study was conducted in accordance with the Declaration of Helsinki and was approved by our institution's Research Ethics Committee (IRB 00000940) on February 8th, 2024.
Clinical outcomes were assessed using the Harris Hip Score (HHS), Veterans RAND 12-Item Health Survey (VR-12), and the Western Ontario MacMaster Arthritis Index (WOMAC) scores preoperatively and at 1 year postoperatively. Of note, we used the reversed WOMAC option, where 0 represents the worst and 100 the best status. Radiographic outcomes were assessed on the first available standing postoperative pelvic radiograph to determine limb length and combined offset discrepancy. Limb length discrepancy was measured using the inferior aspect of the ischial tuberosities to the most prominent medial point on the lesser trochanter. The combined offset discrepancy was measured using the distance from the axis of Köhler's teardrop to the axis of the femoral shaft (Figure 1).
Patient care
Inclusion criteria at our institution for sbTHA were patients with bilateral hip osteoarthritis that have failed conservative treatment. There were otherwise no specific age or comorbidities criteria, and the decision to proceed with sbTHA was at the discretion of the surgeon. All cases were performed by one of six dedicated arthroplasty surgeons at our center. The DA approach is used exclusively by two of the surgeons, whereas the other four surgeons use exclusively the DL. All patients received preoperative medical clearance. Patients in the DA group were positioned supine on a Hana table. Both hips were prepared and draped simultaneously. The most symptomatic hip was operated on first, with a sterile drape covering the contralateral hip. Between hips, fluoroscopy was moved to the other side of the operating room (OR), but no changes in positioning or preparation were necessary. Patients in the lateral group were positioned lateral decubitus on a regular operative table with hip bolsters. The most symptomatic hip was operated on first. After wound closure and dressing application, the patient was flipped to allow access to the contralateral hip and was prepared and draped again. The same instruments were used on each side for both the DA and DL procedures. All patients in both cohorts were given 1 g of tranexamic acid intravenously at the start of the first procedure. The type of anesthetic for the procedure was administered at the discretion of the anesthesiologist. Analgesia was managed by our institution's acute pain service. Postoperatively, patients were admitted to the orthopedic unit for at least one night. Blood transfusion criteria at our institution for all surgeons were hemoglobin below 70 g/L. Venous thromboembolism (VTE) prophylaxis was administered for 6 weeks postoperatively. Our institution's regimen consisted of 325 mg of aspirin taken daily unless the patient was considered high risk by our internal medicine colleagues. In such instances, stronger VTE prophylaxis was at the suggestion of the internal medicine team. All patients received the same standardized, unblinded physiotherapy by our institution's hip arthroplasty discharge pathway. After working with the physical therapist, a recommendation was made for discharge to home or a rehabilitation facility. All patients were seen at follow-up evaluations in the clinic for routine examination and radiographs. All patients were followed up for at least one year after surgery.
Cost analysis
The total cost for each patient was the sum of all in-hospital costs associated with their length of stay (LOS) and resource use. We recorded the length of time spent in the OR, during the procedure, in the post-anesthetic care unit (PACU), and in the inpatient orthopedic ward. Our institution's case costing department provided us with OR, PACU, and inpatient cost per minute.
The OR time was defined as the documented time that the patients entered the room to the time they left the room to recover in the PACU. The procedure time was defined as the documented time that the skin was cut to when it was closed. The Ontario Ministry of Health's schedule of benefits was used to obtain the costs associated with the billing surgeon and anesthetist. 13 Also, operative data, such as the number of people scrubbed, implants, gloves, drapes, dressings, sutures, tubing, and cautery, were recorded from patients’ charts and our institution's Inventory Control Clerk provided the unit costs for implants and OR supplies.
The DA approach has some unique elements, such as intraoperative fluoroscopy, radiologist reads, traction tables, and lead aprons. The costs associated with intraoperative fluoroscopy were determined on a per-minute basis, including the costs of the technician and use of the fluoroscopic machine. The Ontario Ministry of Health's schedule of benefits provided the cost of the radiologist reading the film postoperatively. 13 To protect against fluoroscopic radiation, lead aprons were needed for every DA procedure. The cost of each lead apron was distributed on a per-case basis using 1 year as the longevity of the item and similarly, the Hana fracture table was also included in the total cost based on a 10-year lifespan.
The length of each PACU admission was determined from the time of leaving the OR to the time of admission to the inpatient ward. This information was gathered from an electronic chart review.
We retrospectively reviewed the patient's medical records to obtain all resource use associated with their hospital stay, including medications, dressings, and urinary tract catheterizations. Unit costs were obtained from our institution's pharmaceutical and costing department.
Costs were acquired prospectively using a micro-costing method reported in 2022 Canadian dollars. 14 Micro-costing is a method of cost estimation that produces accurate estimates of economic costs by using unit cost data and comprehensive resource utilization. Costs were adjusted for inflation before analysis. The cost analysis was from the perspective of a public health care payer in Ontario.
Data analyses
All outcomes are described with appropriate summary statistics, means and standard deviations, or frequencies and proportions. We conducted between-group comparisons using independent t-tests for continuous variables and a Chi-Square test for categorical data. For non-normally distributed data, we used a Mann–Whitney U nonparametric test. Statistical significance was set at p < 0.05. Statistical analyses were performed using SPSS software version 22.0 (IBM, Armonk, NY, USA).
Results
We identified 95 patients who underwent simultaneous bilateral THA from the DA approach and 20 from the DL approach. A 2:1 match for age ± 5 years and sex was used and selected 34 and 17 subjects for analysis for the DA and DL approaches, respectively. Diagnoses were similar among groups, with a predominance of osteoarthritis in both. The DA group had a significantly lower body mass index (BMI) when compared to the DL group (26.99 ± 3.39 vs. 32.61 ± 5.79, p = 0.0009) (Table 1).
Demographic information for direct anterior and direct lateral groups.
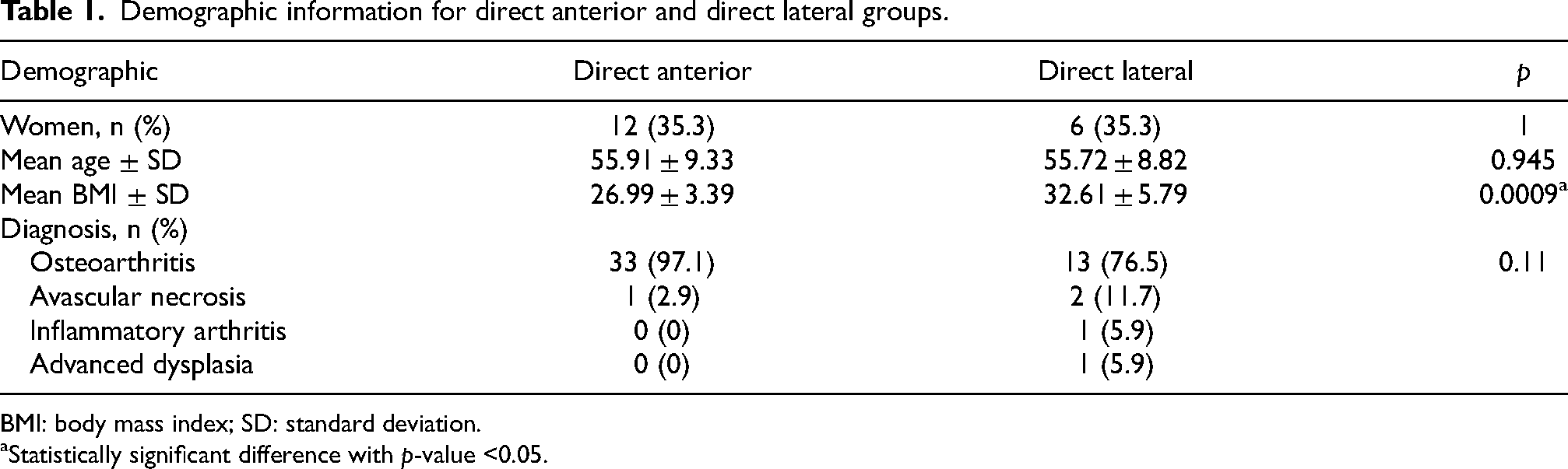
BMI: body mass index; SD: standard deviation.
Statistically significant difference with p-value <0.05.
We found that, at 1-year post-operation, HHS scores were higher for the DA group (97.65 vs. 86.21, p = 0.001). However, preoperative scores also identified a significant difference with the DA group being greater than the DL (50.3 vs. 36.8, p < 0.001). Preoperative WOMAC scores were also found to be higher for the DA group (37.3 vs. 24.0, p = 0.027); however, no differences were found when comparing it postoperatively (89.7 vs. 77.1, p = 0.123). Preoperative and postoperative VR-12 mental (pre: 55.9 vs. 52.4, p = 0.33, post: 57.0 vs. 55.5, p = 0.54) and physical scores (pre: 30.3 vs. 26.7, p = 0.18, post: 50.9 vs. 43.4, p = 0.058) demonstrated no statistically significant difference between the DA and DL groups (Table 2).
Preoperative and 1-year postoperative patient-reported outcome measures.
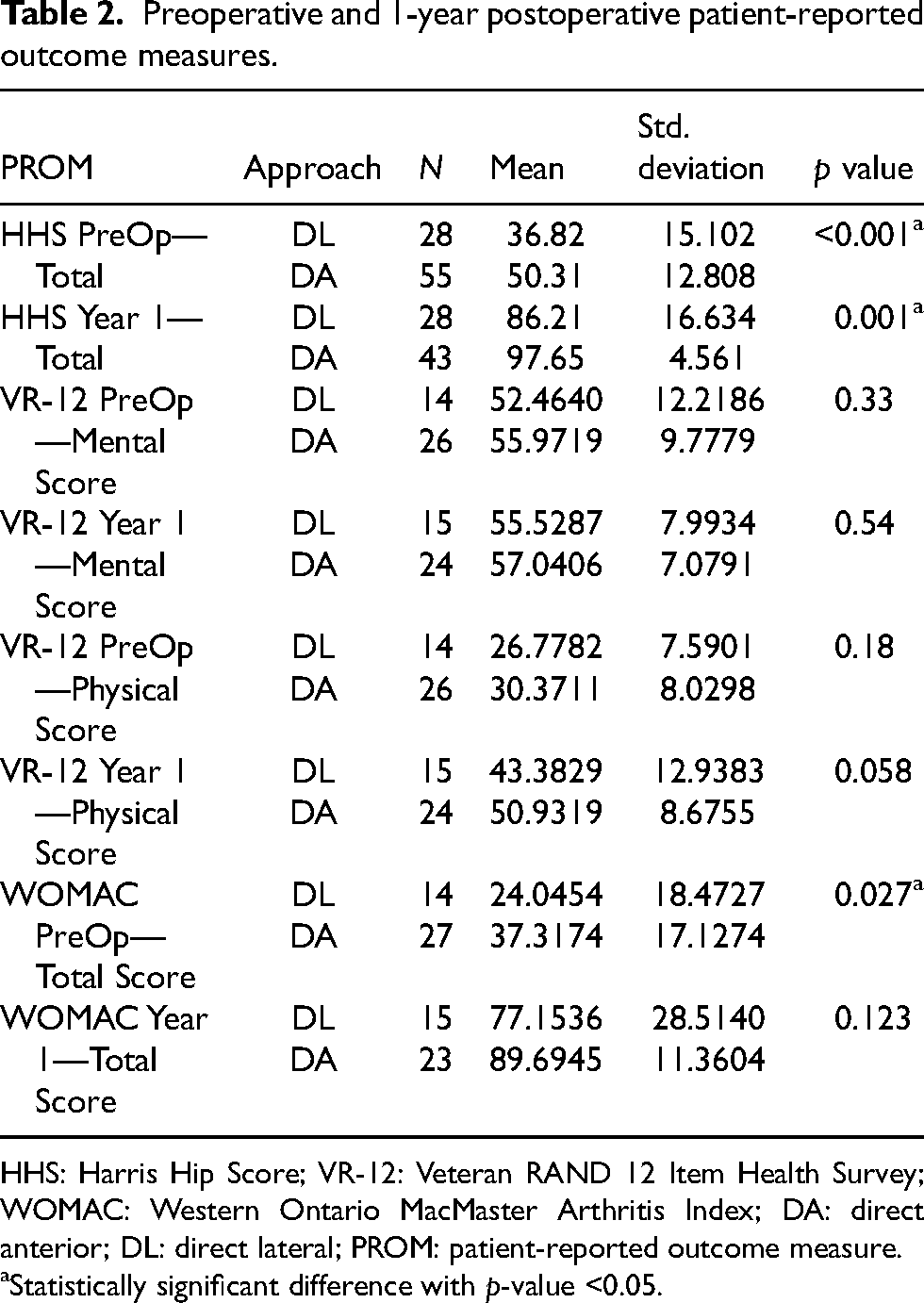
HHS: Harris Hip Score; VR-12: Veteran RAND 12 Item Health Survey; WOMAC: Western Ontario MacMaster Arthritis Index; DA: direct anterior; DL: direct lateral; PROM: patient-reported outcome measure.
Statistically significant difference with p-value <0.05.
Furthermore, evaluation of the change in HHS or WOMAC scores identified no significant difference between approaches (HHS: 46.4 vs. 49.8, p = 0.375, WOMAC: 51.6 vs. 62.8, p = 0.06) (Table 3).
Preoperative and 1-year postoperative change in HHS and WOMAC between approaches.
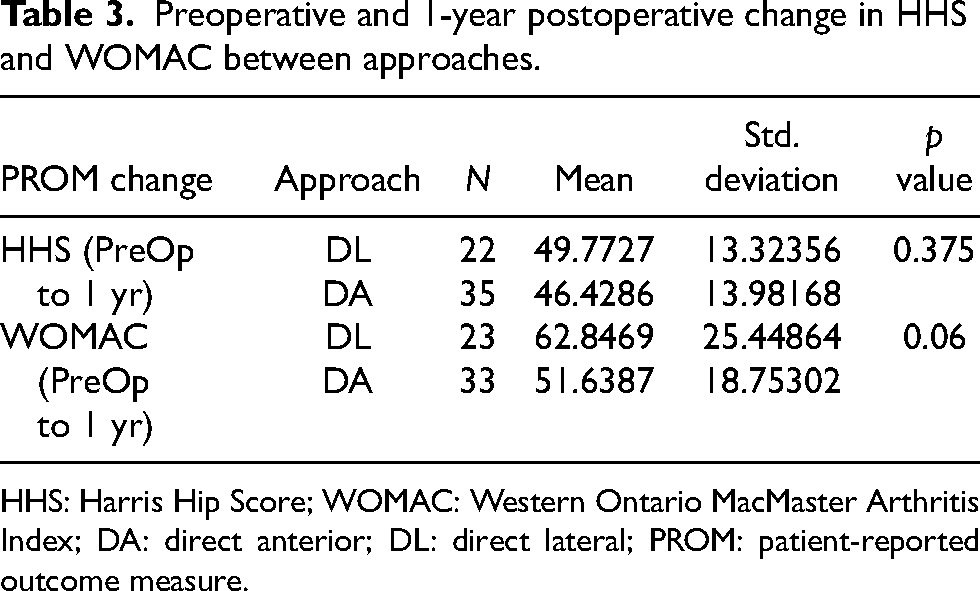
HHS: Harris Hip Score; WOMAC: Western Ontario MacMaster Arthritis Index; DA: direct anterior; DL: direct lateral; PROM: patient-reported outcome measure.
We did note a statistically significant difference in reported limp between groups, with 46.2% of the DL group and only 8.3% of the DA group demonstrating a limp at one year (p = 0.013) (Table 4).
Subjective limp at 1 year postoperative.
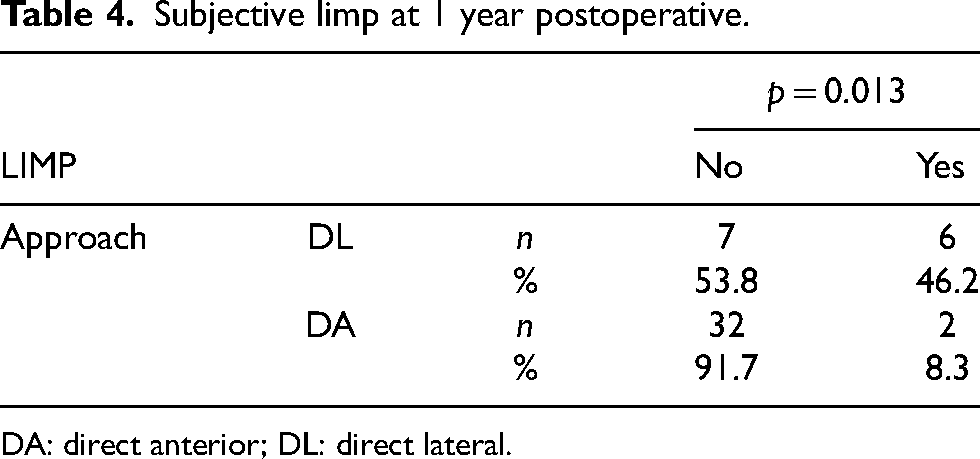
DA: direct anterior; DL: direct lateral.
Additionally, no statistically significant difference was seen in all-cause revision, which included periprosthetic joint infection, aseptic loosening, periprosthetic fracture, instability, and adverse tissue reaction (4 [11.8%] vs. 2 [2.9%], p = 0.094). When reviewing the first available standing postoperative pelvic radiograph, no differences were found between leg length (3.09 vs. 2.59 mm, p = 0.54) and combined offset discrepancies (3.97 vs. 3.29 mm, p = 0.50) (Table 5).
Limb length and combined offset discrepancy based on first postoperative radiograph.
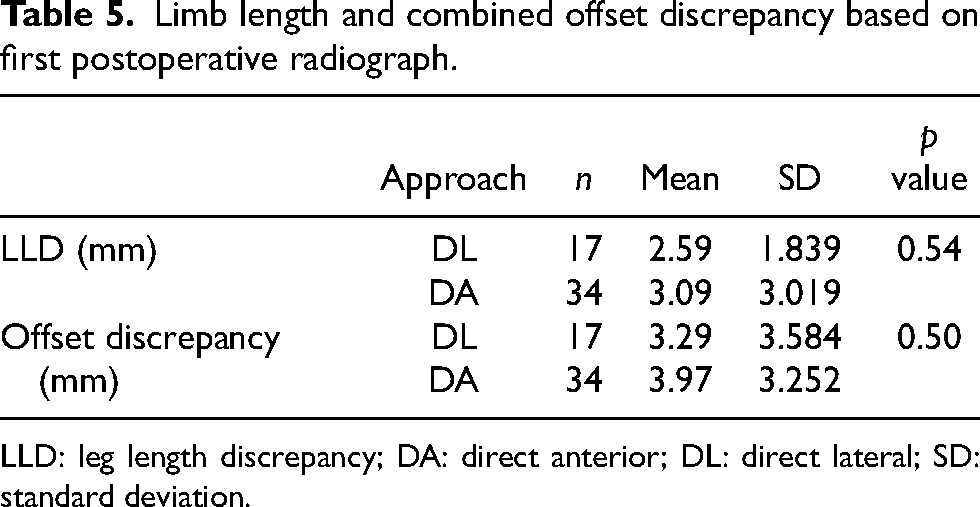
LLD: leg length discrepancy; DA: direct anterior; DL: direct lateral; SD: standard deviation.
The DA group demonstrated significantly lower procedure time (125.74 vs. 156.41 min, p < 0.001), total time in the OR (165.68 vs. 194.59 min, p = 0.005), LOS (1.97 vs. 6.65 days, p < 0.001), and rehab discharge (11.8% vs. 47.1%, p = 0.012). There was no significant difference in the number of hospital staff scrubbed in and units of blood transfused between groups (1 vs. 3, p = 0.51).
Total perioperative costs were significantly less for the DA (CAD 13,265.79) compared to the DL group (CAD 18,116.02) with a mean difference of CAD 4850.22 (95% CI: 3410.54–6289.90) (p < 0.001) (Table 6).
Perioperative cost analysis between approaches for sbTHA.
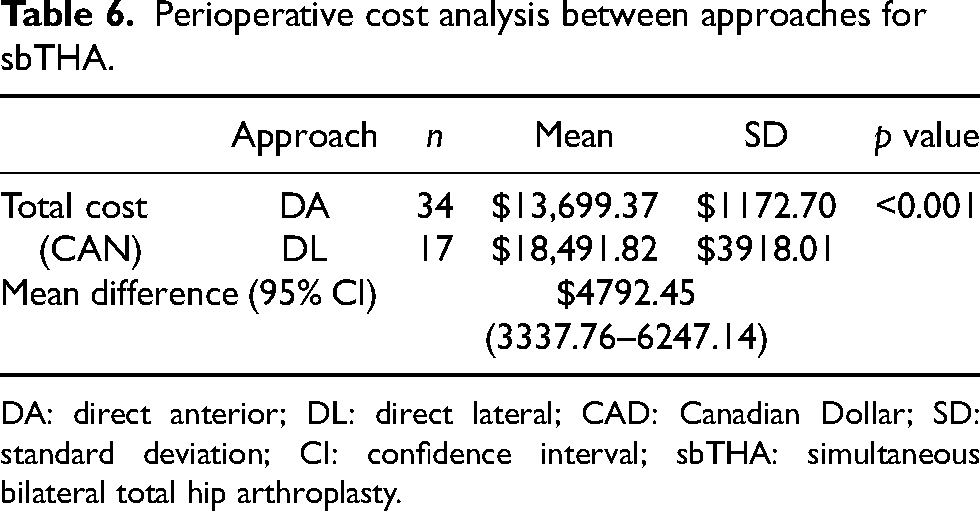
DA: direct anterior; DL: direct lateral; CAD: Canadian Dollar; SD: standard deviation; CI: confidence interval; sbTHA: simultaneous bilateral total hip arthroplasty.
Electronic PACU documentation did not exist at our institution before 2017, therefore, 15 patients from the DA cohort and 9 from the DL cohort lacked PACU admission length. Therefore, we used our average PACU admission length for all patients (175.56 min) to evaluate their PACU costs.
Discussion
It has been reported that up to 20% of THA patients require a contralateral arthroplasty within 5 years after their first surgery, putting into question whether simultaneous bilateral THA should be considered more often. 15 However, the safety of the procedure has been questioned. The potential benefits of a single surgery must be weighed against the slightly increased risk for systemic complications.16,17 Recent innovations in perioperative management have been shown to minimize complications,7,18 but it is unclear whether the surgical approach affects perioperative outcomes.
Despite a statistically significant difference in subjective limp in the DL group, no difference was seen in WOMAC/HHS/VR-12 scores. A study done at our institution in 2018 looked at gait analyses among the approaches in unilateral THAs. We found that the DL cohort demonstrated a decreased external rotation moment, higher ipsilateral trunk lean, and increased pelvic tilt at 12 weeks post-THA. 19 To our knowledge, no study has shown the effects of sbTHA via the DL approach on these gait elements. Further research is warranted in the gait analysis of patients who underwent sbTHA via the DL approach to understand their recovery.
Some of the purported disadvantages of the DA approach are the added costs associated with using a specialized OR table, such as the Hana fracture table in this study, as well as the costs of using intraoperative fluoroscopy. 12 Interestingly, recent literature has demonstrated that the anterior approach can be performed safely without the use of a specialized table and intraoperative fluoroscopy. 20 The other major cited disadvantage of the DA approach is increased OR time when comparing the anterior approach to other surgical approaches in unilateral THA.21,22 However, our study demonstrated the opposite, whereas the sbTHA DA had a significantly lower procedure time when compared to the DL. This difference is likely attributed to the ability to prepare and drape both sides before sbTHA DA surgery and thereby keep the interruption between hips to a minimum. These findings put into question some of the biggest arguments against the DA approach, especially in the setting of sbTHA.
Previous studies from our institution have demonstrated that the DA approach for unilateral THA has led to significantly decreased perioperative costs when compared to posterior or lateral approaches. 12 Most of this difference can likely be attributed to a decreased LOS in the hospital after a DA THA versus a posterior or lateral THA. Our previous study showed that DA patients stayed on average 34 h in the hospital compared to 64 h for a posterior or lateral. 12 Several other studies have found similar results showing that having a THA performed through an anterior approach results in a significant reduction in days spent in the hospital.21–23 We have demonstrated that these findings also seem to hold in the setting of sbTHA, with an LOS almost 5 days shorter in the DA group. The decrease in LOS is likely a strong contributor to the fact that total perioperative costs were significantly less for the DA group when compared to the DL for sbTHA.
This study should be interpreted considering important limitations. Our data were examined retrospectively. Thus, there may be unaccounted-for differences between our DA and DL sbTHA groups; in particular, the fact the DL had lower functional scores preoperatively than the DA group. This difference may have led to more difficulties in early postoperative function for DL patients, in turn, increasing hospital LOS. Also, the DA and DL approaches were used by different surgeons with differing experiences, techniques, and preferences, all of which could have affected outcomes. Notably, a difference in surgeon workflow introduces performance bias, which impacts not only procedure time but also the overall cost of the procedure. Furthermore, seeing as our data are collected between 2006 and 2020, temporal changes in practice, by the surgeons and administration, may further affect some of the cost parameters. Also, PACU times were lacking for part of our cohort, causing us to use an average which could have led to missing data bias. The generalizability of the data can also be questioned. The cost data are taken from a single academic institution within a publicly funded healthcare system, which would undoubtedly vary from one hospital to another and one healthcare model to another. Additionally, our sample was relatively small since simultaneous bilateral THAs are performed relatively infrequently at our institution. Moreover, our DL group had a significantly higher BMI than the DA group. This has some potential implications to confound the results as obesity has been linked to an increase in postoperative complications following THA such as infection or need for revision. 24 Interestingly though, literature has shown that obesity is not linked to a significant increase in hospital cost post-THA, 25 putting into question how much of a confounding variable BMI is in this study.
Conclusion
Simultaneous bilateral total hip arthroplasty is progressively increasing in popularity for the treatment of bilateral hip arthritis. To our knowledge, this is the first study of its kind comparing the DA and DL approaches concerning sbTHA. Despite PROMs showing no differences between approaches, patients undergoing simultaneous bilateral THA via the DL approach were significantly more likely to have a limp at one year compared to the DA approach. Also, the significantly reduced LOS and lower surgical time result in lower costs of a sbTHA performed through an anterior approach. Thus, the DA approach may lead to a better gait and lower costs for those undergoing sbTHA.
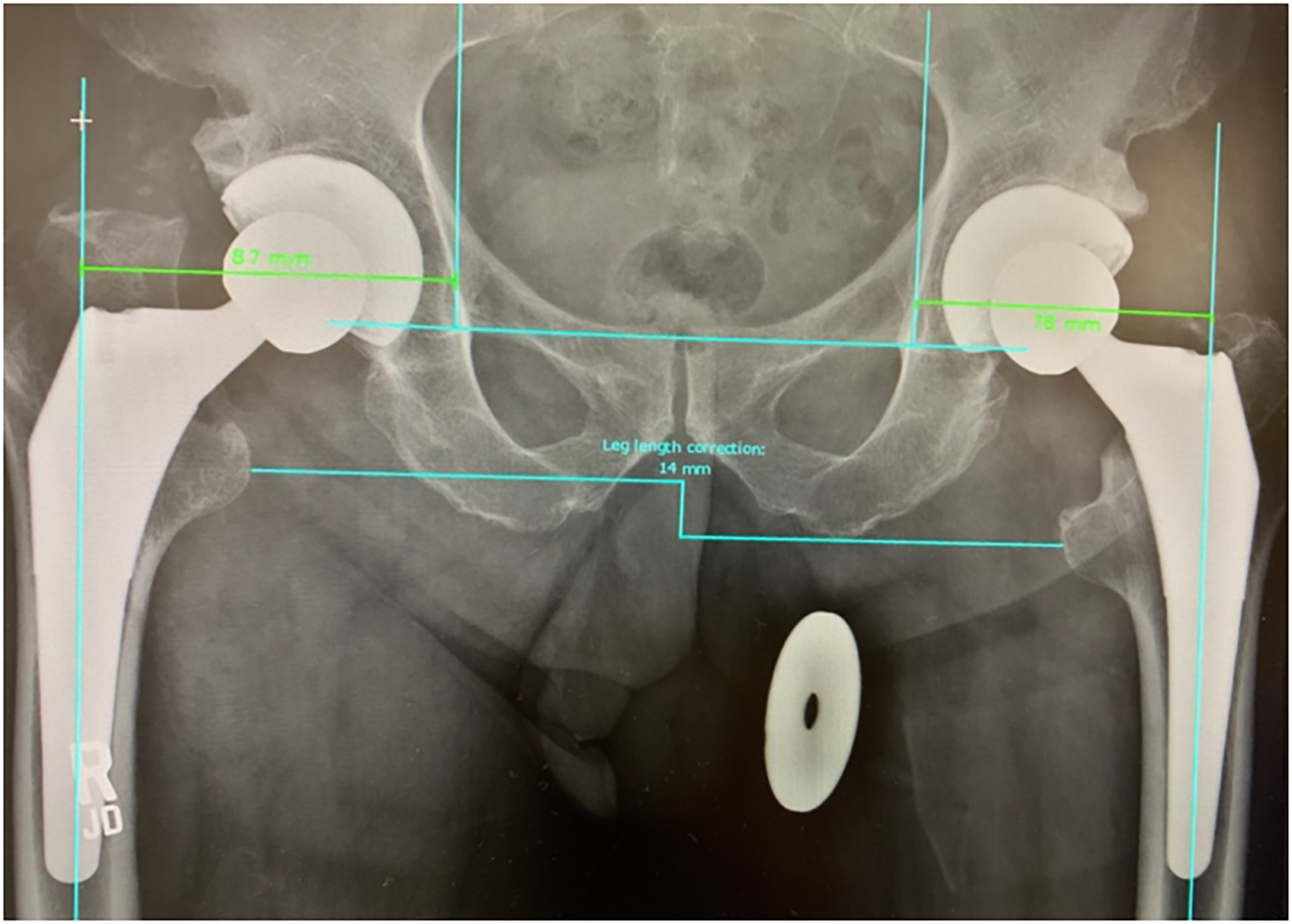
Postoperative AP low pelvis radiograph depicting radiographic assessment for limb length and combined offset discrepancy.
Footnotes
Acknowledgements
The authors would like to acknowledge Maharshi Nagda for his contributions to the data collection and analysis on this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.