
Abstract
Purpose
A drug known as carbazochrome sodium sulfonate (CSS) can reduce blood loss. But, it is not known how it can prevent the development of hemostatic and inflammatory conditions in patients who undergo bilateral simultaneous total hip arthroplasty (SBTHA). This study will analyze the safety and effectiveness of combining this drug with SBTHA.
Methods
The study was conducted on 100 patients who underwent SBTHA with simultaneous total hip replacement. They were split into two groups: group B received TXA with CSS, group A received TXA with no CSS. The main observation of the study was the total blood loss, which is the most common indication of blood loss. Other secondary indicators of the study included hidden blood loss, postoperative blood transfusion rate, level of inflammatory reactants, hip function, pain score, venous thromboembolism (VTE) and the incidence of adverse events.
Results
Group B had significantly lower TBL and HBL compared to Group A. Group B showed significant improvement in inflammatory biomarker levels, blood transfusion rate when compared to Group A (p < .05). No thromboembolic complications occurred in either group. There were no significant differences between the two groups in terms of postoperative swelling rate, intraoperative blood loss, visual analog scale pain score, platelet count, discharge motion and average length of stay.
Conclusions
As a hemostatic agent, CSS combined with TXA can reduce postoperative blood loss in patients undergoing SBTHA, and is more effective than TXA alone in terms of blood loss and inflammation, and does not increase the incidence of thromboembolic complications.
Keywords
Introduction
Total hip arthroplasty (THA) is considered to be one of the most successful surgical interventions to relieve pain and improve function in patients with end-stage hip disease. 1 THA is in great demand in China and will grow by 25%-30% per year. 2 In fact, a significant proportion of patients experience bilateral hip lesions and eventually require bilateral THA. 3 For these patients, simultaneous bilateral total hip arthroplasty (SBTHA) may be an alternative because simultaneous surgery can be significantly more cost-effective by reducing overall anesthesia time, hospital stay, and recovery time, and it does not compromise functional outcome or increase the risk of revision, reoperation, or postoperative complications compared with staged surgery. 4
Bleeding during SBTHA surgeries can be significant, with approximately 90% of patients developing postoperative anemia. 5 The overall allogeneic transfusion rate after SBTHA can range from 49.3% to 72.7%. High transfusion rates lead to increased morbidity, transfusion-related complications, and economic burden for patients. Although the use of tranexamic acid can reduce blood loss in the perioperative period of SBTHA, some patients with SBTHA still receive blood transfusions during or after surgery, and transfusion rates after SBTHA vary widely between countries. TXA has been found to possess certain anti-inflammatory effects, although they may not be particularly strong. Coagulants like TXA, which reduce blood loss, can potentially increase the risk of thromboembolic events. However, evidence suggests that TXA does not significantly raise the risk of venous thromboembolism (VTE). Despite TXA’s effectiveness in reducing blood loss and transfusion requirements, it may not adequately address hidden blood loss (HBL) or the inflammatory response associated with SBTHA. Therefore, additional measures are necessary to further mitigate these issues.
CSS makes them valuable in the treatment of conditions involving bleeding. CSS is mentioned as being used in the treatment of hemorrhagic diseases affecting different body systems, including the urinary system, upper gastrointestinal tract, respiratory tract, and obstetrics and gynecology. CSS likely helps in reducing excessive bleeding in these conditions.6,7 Previous studies have indicated that TXA combined with CSS can significantly reduce the amount of blood loss after TKA without increasing the risk of asymptomatic DVT. 8 In addition to orthopedics, CSS can be used to treat other diseases.9–13 First, CSS can improve bleeding symptoms in patients with hereditary hemorrhagic telangiectasia. Second, CSS improves pain and post-urination symptoms in patients with refractory chronic prostatitis. Finally, the application of CSS may help eliminate the risk factors for severe hemorrhagic fever and shock. 14 However, CSS does not prevent plasma leakage or symptoms of shock in patients with dengue hemorrhagic fever/dengue shock syndrome. 10
On the premise of not increasing the risk of thromboembolic complications, reducing perioperative blood loss and excessive surgical stress immune response is the key to reduce the preoperative complications of THA and other major operations. Therefore, the objective of this randomized controlled trial was to evaluate the additional effects of CSS combined with TXA on hemostasis, thrombosis, and anti-inflammatory effects in patients undergoing simultaneous bilateral total hip replacement.
Materials and methods
Patient recruitment
The study was registered in the Chinese Clinical Trials Registry (ChiCTR1800015839) and approved by the Ethics Committee of our hospital. The whole experiment was carried out in the Department of joint Surgery of our hospital. Obtain written informed consent from all patients prior to surgery.
Inclusion and exclusion criteria
Patients with osteoarthritis of the hip or femoral head necrosis (Ficat stage IIIB or IV) between September 2017 and October 2023 who were scheduled to undergo SBTHA in our hospital were included in this study: (1) adult patients who received an initial SBTHA; (ii) American Society of Anesthesiologists (ASA) Medical Conditions I-III; (3) Age ≥18 years old. The exclusion criteria are as follows : (1) receiving other operations during hospitalization; (2) Severe anemia (hemoglobin <70 g/L); (3) Patients with a history of kidney transplantation, arterial thromboembolism (such as myocardial infarction or stroke), arterial stenting, DVT, pulmonary embolism, or knee surgery were excluded. (4) Patients who are allergic to TXA, CSS, and patients who refuse to accept blood products or patients with missing data. The demographic and preoperative characteristics of the patients were recorded before operation.
Research drug treatment options
Patients were randomly assigned to two groups using a computer-generated table of random numbers. A nurse not associated with the study prepared an experimental drug cocktail and a placebo (B vitamins) to ensure blindness. On the morning of surgery, the patient drew a random number from an opaque envelope sealed by Investigator 1. Investigator two recorded the groups in preparation for subsequent action; Post-operative outcome evaluators (LJC) and statistical analysts (QHL) were also unaware of this grouping. Both groups received 1000 mg of tranexamic acid intravenously before surgery. Group A received the same dose of placebo after surgery, and group B received 40 mg of intravenous CSS within 3 h after surgery.
Surgical technique and perioperative management
All patients underwent SBTHA surgery using DAA under general anaesthesia by the same senior surgeon. A Corail or Trilock handle and a pinnacle acetabular cup were used intraoperatively, and no drainage tube was used postoperatively. After the patient woke up in the recovery room, the patient was transferred back to the ward to begin muscle contraction exercises such as ankle pump and quadriceps. During hospitalization, he used a walker to walk with weight. Low molecular weight heparin was first administered 0.2 mL 12 h after surgery and then 0.4 mL every 24 h thereafter until discharge. Patients were discharged when pain was effectively controlled by oral analgesics. They can change positions independently, climb stairs, or walk at least 200 feet without assistance. After discharge, rivaroxaban was given 10 mg orally once a day for 2 weeks to prevent venous thromboembolism. Deep vein thrombosis was detected by Doppler ultrasound before operation and followed up 1 and 3 months after operation. If the patient has chest pain, hemoptysis, dyspnea, or other symptoms, a chest CT should be performed to determine if the patient has a pulmonary embolism. When the hemoglobin (Hb) concentration is below 70g /L or 70g /L < Hb < 100g /L, blood transfusion is required, but dizziness, fatigue, and other obvious symptoms of anemia are observed.
Results and follow-up
Baseline signs were collected for all patients at admission: age, sex, body mass index (BMI), surgical side, coagulation function, Hb levels, hematocrit (Hct), and inflammatory factors before surgery and 13 and 25 days after surgery. The primary outcome was TBL, calculated using formulas from previous studies. Secondary outcome measures included HBL, estimated intraoperative blood loss (IBL), blood transfusion rate, levels of inflammatory markers (C-reactive protein [CRP], interleukin-6, and erythrocyte sedimentation rate [ESR]), numerical scale pain score (NRS), hip movement at discharge, duration of surgery, and incidence of associated complications.
TBL was calculated based on the patient’s preoperative and postoperative Hb levels on the third day, and the formula was as follows: TBL = patient blood volume (PBV) × (hct pre-HCT post-HCT)/Hctave. PBV (ml) = [k1 × height (m) 3 + k2 × weight (kg) + k3] ×1000, in which male k1 = 0.3669, k2 = 0.03,219, k3 = 0.6041, Female k1 = 0.3561, k2 = 0.03,308, k3 = 0.1833. The amount of blood loss during the operation was the amount of fluid in the suction tank + the weight gain of surgical gauze. HBL is defined as TBL minus intraoperative blood loss.
Statistical analysis
SPSS 26.0 software was used for statistical analysis of all the data. To achieve a minimum clinically significant difference of 182 mL in the leading indicators between the two groups, we used a bilateral α level of 0.05 and a 90% response rate to calculate a minimum sample size of 27 patients. At least 30 patients were enrolled in each group to accommodate patient loss during follow-up or discontinuation. The continuous data of normal distribution is expressed as mean ± standard deviation, and the qualitative data is expressed as frequency and percentage. Univariate ANOVA was used to compare continuous variables, and Chi-square test or Fischer precision test was used to compare categorical variables. A p value <.05 was considered statistically significant.
Results
Patients
A total of 109 patients undergoing SBTHA in our hospital were evaluated, of whom five met the exclusion criteria and four did not wish to participate in this study. Thus, a total of 100 patients, 50 in each group, were enrolled in the study (Figure 1). There were no significant differences in preoperative baseline characteristics between the two groups (Table 1). Flow chart for patient selection and exclusion. Baseline characteristics of the patients. Notice:a Student’s t test. bPearson’s chi-squared test. cMann-Whitney U test.

Primary outcomes
The blood loss of group A was (1305.71 ± 352.23) ml, and that of group B was (1109.73 ± 263.14) ml, which was statistically significant (p = .002).
Secondary outcomes
The hidden blood loss was 1109.51 ± 348.46 mL in group A and 914.65 ± 261.28 mL in group B (p = .002) (Figure 2). Volume of blood loss.
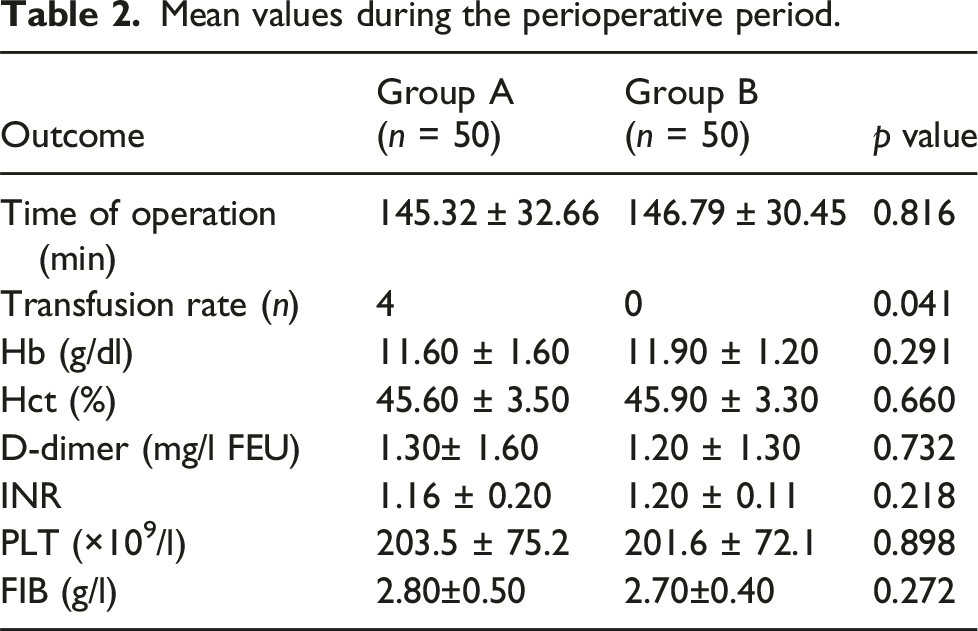
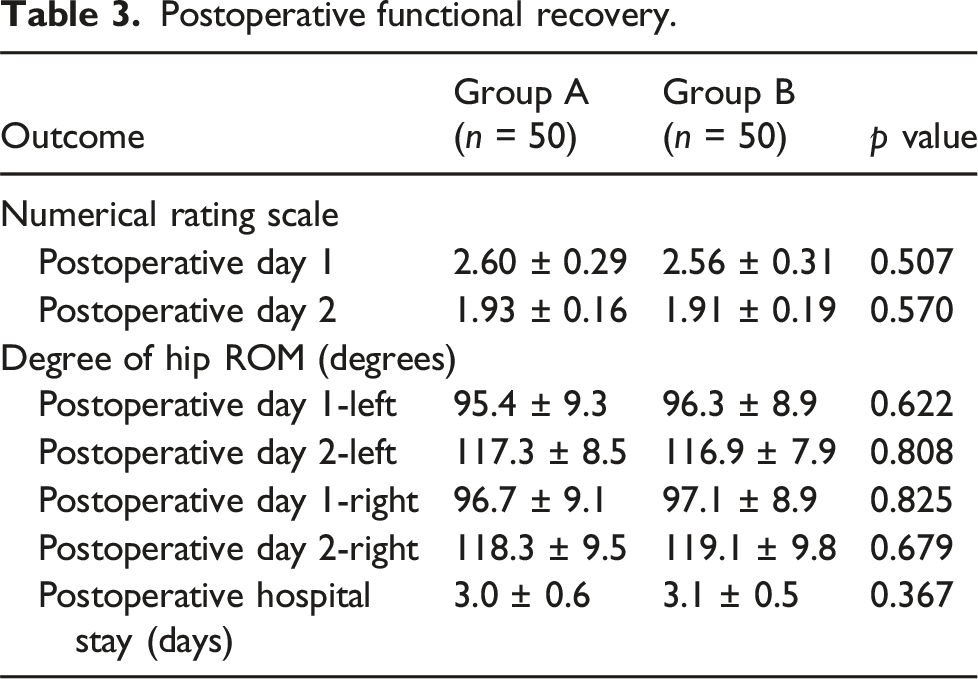
In Group B, the levels of inflammatory markers CRP (pre p = .438 pod1 and pod3 p < .05), IL-6 (pre p = .636 pod1 and pod3 p < .05), and ESR (pre p = .746 pod1 and pod3 p < .05) were significantly lower than those in Group A on postoperative days 1 and 3 (Figure 3). There were no anemia-related symptoms reported in either group. However, in Group A, four patients received blood transfusions due to an Hb concentration <70 g/L. The blood transfusion rate in Group B was significantly lower than that in Group A, suggesting that patients in Group B required fewer blood transfusions (p = .041). There were no significant differences between the two groups in terms of operation time (145.32 ± 32.66 vs 146.79 ± 30.45,p = .816) and IBL (196.20 ± 9.81 vs 195.08 ± 8.62,p = .546) between the two groups (Table 2). There were no significant differences between the two groups in pain scores and hip motion recovery from surgery to discharge (Table 3). During hospitalization, both groups experienced complications such as wound exudation or delayed healing, with 2 cases in Group A and 1 case in Group B. However, there was no significant difference in the incidence of wound complications between the two groups. Similarly, The incidence of nausea and vertigo was similar between the two groups. There were no reports of drug-induced urticaria, skin spots, muscle cramps, or other related thrombotic events during follow-up (Table 4). Expression Levels of the inflammatory factors ESR, CRP, and IL-6. Mean values during the perioperative period. Postoperative functional recovery. Postoperative complications.

Discussion
In this study, we investigated the safety and efficacy of carbazochrome sodium sulfonate in patients undergoing simultaneous bilateral total hip arthroplasty. We found that carbazochrome sodium sulfonate was effective in reducing total blood loss, hidden blood loss, transfusion rate, and inflammatory marker levels after simultaneous bilateral total hip arthroplasty compared with the blank group. And it does not affect the incidence of DVT and other complications.
With the development of minimally invasive surgery (MIS), SBTHA is safer and has better outcomes than two-stage in hip disease. This procedure can shorten the length of hospital stay, reduce blood loss, improve hip symptoms rapidly and is cost-effective. 15 Previous studies have proved that tranexamic acid has a certain role in reducing the total blood loss, hidden blood loss and transfusion rate in patients undergoing simultaneous bilateral total hip arthroplasty. 16 Studies have also shown that tranexamic acid combined with sodium caroside sulfonate can effectively reduce the total blood loss, hidden blood loss and blood transfusion rate in total knee arthroplasty and total hip arthroplasty. 17 However, the role of the combination of tranexamic acid and sodium caroxane sulfonate in SBTHA is unknown.
After operation, the Hb level of the body was positively proportional to the quality of life of the patients. Perioperative blood loss increases the risk of postoperative infection, slows recovery of joint function, prolongs hospital stay, and increases mortality. Total blood loss can be calculated using a number of formulas, allowing doctors to better assess blood loss and facilitate perioperative management of patients. We calculated the total blood loss of hematopoietic changes before and after surgery by Gross formula, and concluded that tranatemic acid combined with carotene sodium sulfonic acid can effectively reduce the amount of blood loss after SBTHA.
Acute response can play a role in fighting infection, reducing bleeding, and promoting the speed of wound healing. This systemic response plays a role in normal blood clotting and immune function. But when this inflammatory response is overdone, it can alter the course of the disease and cause more damage to the body. Inhibiting this persistent inflammatory response can promote the recovery of joint function and reduce the occurrence of postoperative pain. The expression levels of various inflammatory markers, IL-6, CRP and ESR in the group with CSS (group B) were lower than those in the group without CSS (group A). TXA can inhibit the conversion of plasmapherin to plasma protein and thus inhibit postoperative inflammation and vascular permeability in patients. Therefore, the mechanism of CSS and TXA combined to inhibit inflammation needs to be further studied. There was no significant difference in postoperative pain scores between the two groups. This may be related to the implementation of the accelerated rehabilitation model in our department. We also found that the two groups in postoperative hip range, related complications or incidence of VTE has no significant difference. In this study, we found that caroside sodium sulfonate combined with tranexamic acid could reduce perioperative blood loss, transfusion rate and inflammatory cytokine levels. However, there was no significant difference in early postoperative hip function and pain relief between the two groups. The addition of CSS to TXA did not increase the incidence of VTE or its associated complications.
Limitations
CSS and TXA’s advocacy in terms of safety profile in difficult clinical situations like SBTHA needs to be proclaimed in a guarded fashion and studied over a longer term before it can be proclaimed to have a safety profile at usage, although we have shown that CSS and TXA could be useful in TKA. In the future,we will study CSS and TXA over a longer term to verify its safety.
Footnotes
Acknowledgements
Not applicable.
Author Contributions
Guangtao Han,Pengde Kang wrote the article and provided all figures, and Qin Wang, Lijun Cai read the final manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation (No.8217090607).
Code availability
Not available.
Ethical statement
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.