
Abstract
Purpose
It remains unclear whether simultaneous bilateral total hip arthroplasty (SimBTHA) or staged bilateral total hip arthroplasty (StaBTHA) is clinically superior. No study has compared these two procedures matching surgical approach and patient background. This study aimed to clarify the differences between SimBTHA using direct anterior approach (SimBTHA-DAA) and StaBTHA using the direct anterior approach (StaBTHA-DAA).
Methods
Patients who underwent THA between 2012 and 2020 were enrolled, resulting in a total of 1658 hips of 1388 patients. After propensity score matching for patient background, 204 hips of 102 patients (51 patients in each group) were examined. Clinical and radiographic outcomes, complications, intraoperative blood loss and blood transfusions (BT) were evaluated. In complications, we evaluated periprosthetic fractures, pulmonary embolism, deep venous thrombosis, surgical site infection and dislocation.
Results
At the final follow-up, clinical and radiographic outcomes and complications were not significantly different between the groups. Intraoperative blood loss was equivalent for SimBTHA and the sum in the first- and second-stage StaBTHA. The total-BT rate was significantly higher for SimBTHA-DAA than for StaBTHA-DAA (p < .0001). The allogeneic BT rate was significantly higher in SimBTHA-DAA in the supine position (32.3%) than in StaBTHA-DAA (8.3%) (p = .007). However, no patient who received autologous BT required allogeneic BT.
Conclusions
Clinical and radiographic outcomes were equivalent between SimBTHA-DAA and StaBTHA-DAA. The allogeneic BT rate was significantly higher in SimBTHA-DAA than in StaBTHA-DAA. Autologous BT reduced the use of allogeneic BT in SimBTHA-DAA. Auto-BT may be useful for avoiding allo-BT in SimBTHA.
Keywords
Introduction
Primary total hip arthroplasty (THA) is a useful surgery for reducing pain and improving hip function in cases with a follow-up period of >20 years.1,2 The incidence of bilateral hip osteoarthritis (OA) is 42% in Black and White populations. 3 In Japan, developmental dysplasia of the hip is the main cause of hip OA, and the incidence of bilateral hip OA secondary to developmental dysplasia of the hip is reported to be 84%. 4 Of patients who undergo uniliteral THA, 16–85% are likely to require contralateral THA.5–9 However, there is no consensus regarding whether patients with bilateral hip OA should be treated with simultaneous bilateral THA (SimBTHA) or staged bilateral THA (StaBTHA). Several studies indicate that SimBTHA involves lower hospitalization costs with one-time use of anesthesia, and shorter total hospital stay than StaBTHA.10–12 Contrastingly, SimBTHA results in more frequent complications, including deep venous thrombosis (DVT) and respiratory diseases.13,14 Limitations of these articles are not randomized controlled trials and different patients background, such as sex and age, affecting the reliability of the postoperative results.
Surgical approach is another important factor that affects postoperative results. Most studies on bilateral THA discuss cases that use the posterior approach (THA-PA) with the lateral position; only a few reports discuss the direct anterior approach (DAA).115–18 The DAA is commonly used as a minimally invasive and complete muscle-tendon-sparing approach that is usually performed with the patient in the supine. 19 Higgins et al. reported that the DAA is superior to the posterior approach in terms of early postoperative pain and functional improvement. 20 However, the right lateral position may increase the risk of postoperative pulmonary embolism (PE). 21 Moreover, because there is no need to change postures intraoperatively during SimBTHA using the DAA (SimBTHA-DAA), time and effort may be saved. After StaBTHA, some reports suggest that contralateral hip pain and limited range of motion (ROM) after the first THA adversely affect functional impairment after the second procedure.22,23 Therefore, we hypothesized that SimBTHA-DAA contributes to better physician-reported outcomes, patient-reported outcomes, and lower complication rates than StaBTHA using the DAA (StaBTHA-DAA).
This study aimed to determine whether physician-reported outcomes, patient-reported outcomes, blood transfusion rates, complications, and radiographic outcomes differ between SimBTHA-DAA and StaBTHA-DAA for bilateral hip disease. These outcomes were assessed after propensity score-matched analysis to match the patient background in the two groups.
Materials and methods
Study design and patients
This retrospective, case-control study has been approved by the IRB of the authors’ affiliated institutions (2020-J029). The participants had the opportunity to opt out of the study.
A total of 1658 primary THAs were performed in 1388 patients at our institution between January 2012 and April 2020. Of these, 502 hips (251 patients) that underwent SimBTHA-DAA or StaBTHA-DAA were enrolled. Further, 102 hips (51 patients) who underwent second-stage THA with more than a 1-year interval from first THA in StaBTHA-DAA were excluded. Overall, 256 hips of 128 patients who underwent SimBTHA-DAA and 144 hips of 72 patients who underwent StaBTHA-DAA were included. After propensity score matching for age, sex, height, weight, and American Society of Anesthesiologists (ASA) classification, 102 hips of 51 matched patients were evaluated respectively (Figure 1). The patient characteristics were no significant difference in two groups (Table 1). The postoperative follow-up periods were 44.9 ± 22.8 months in SimBTHA-DAA and 58.0 ± 27.0 months from first-stage THA and 51.0 ± 27.2 months from second-stage THA in StaBTHA-DAA. There was no significant difference in the diagnosis, Crowe classification,
24
types of acetabular components, or femoral components according to Khanuja et al.’s
25
between the two groups (Table 1). Flow chart of study diagram. Comparison of patient characteristics and implant types. SimBTHA-DAA, simultaneous bilateral total hip arthroplasty using the direct anterior approach; StaBTHA-DAA, staged bilateral total hip arthroplasty using the direct anterior approach; SD, standard deviation; ASA, American society of anesthesiologists; ONFH, osteonecrosis of the femoral head; RA, rheumatoid arthritis; 3D, three-dimensional; HA, hydroxyapatite.

Surgical procedure and indication
All surgical procedures were performed using the DAA with the patients in the supine position.26,27 One team performed all surgeries under the supervision of a senior hip arthroplasty surgeon with >30 years of experience (T.H.). Patients with bilateral hip disease underwent SimBTHA-DAA or StaBTHA-DAA as a result of the informed decision process. Patients were excluded if they had an ASA score of IV or ASA scores of II/III with active ischemic heart disease or decreased left ventricular function <45%. Prior to surgery, the anesthesiologist assessed each patient’s eligibility for SimBTHA-DAA. Patients with hip contractures tended to be assigned to SimBTHA-DAA by surgeons.
We decided to perform autologous blood transfusion (auto-BT) based on the Japanese Society of Autologous Blood Transfusion guidelines. 28 Auto-BT was initially considered for patients with hemoglobin levels >11 g/dL, and the final decision was made according to the patient’s wishes. Full weight-bearing was allowed from 1 day after surgery.
Evaluations
Clinical outcomes were assessed using the following items: the pre- and postoperative Japanese Orthopaedic Association (JOA) score as a physician-reported outcome, 29 the postoperative Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ) score at the final evaluation as a patient-reported outcome, 30 pre- and postoperative ROM and postoperative ROM improvement in flexion and abduction. Postoperative ROM improvement defined as postoperative minus preoperative value. JOA scores ranged from 0 (worst) to 100 (best), and consist of four subcategories: pain, ROM, walking ability, and activities of daily living. The JHEQ scores involves seven questions grouped into the categories of pain, movement, and mental status. Each category score ranged from 0 (worst) to 28 (best), giving a total score from 0 to 84. The measurements of clinical outcomes were assessed by a physical therapist who was blinded to whether SimBTHA or StaBTHA was assessed.
Complications included periprosthetic fractures (PPF), PE, DVT, dermatological problems, surgical site infection (SSI), and dislocation. Perioperative outcomes included operative time, intraoperative blood loss, total blood transfusion (total-BT) rate, auto-BT and allogeneic blood transfusion (allo-BT) rate. These data were accumulated for the first- and second-stage THAs in StaBTHA-DAA.
Radiographic outcomes included aseptic loosening of components, stem sinking, and leg length discrepancy (LLD). Postoperative stem sinking was considered significant at ≥3 mm. 31 We defined LLD as the laterality of the distance from the inferior margin of the acetabular teardrop to the most prominent point of the lesser trochanter anteroposterior radiographic view. 32 Radiographic outcomes were assessed by orthopedic surgeon who were not involved in surgery.
Statistical analysis
Continuous variable data are presented as mean ± standard deviation. Continuous and categorical data were analyzed using the Mann–Whitney U test and chi-squared test, respectively. The significant sample size was calculated with an alpha value of 0.05 and power of 0.8 using G*Power (G*Power 3.1; Düsseldorf, Germany), resulting in a required sample size of 44 patients for each group. 33 All statistical analyses were performed using JMP version 14 (SAS Institute Inc., Cary, NC, USA). Differences were considered statistically significant at a p-value of 0.05.
Results
Clinical outcomes and complications
Comparison of clinical outcomes and complications.
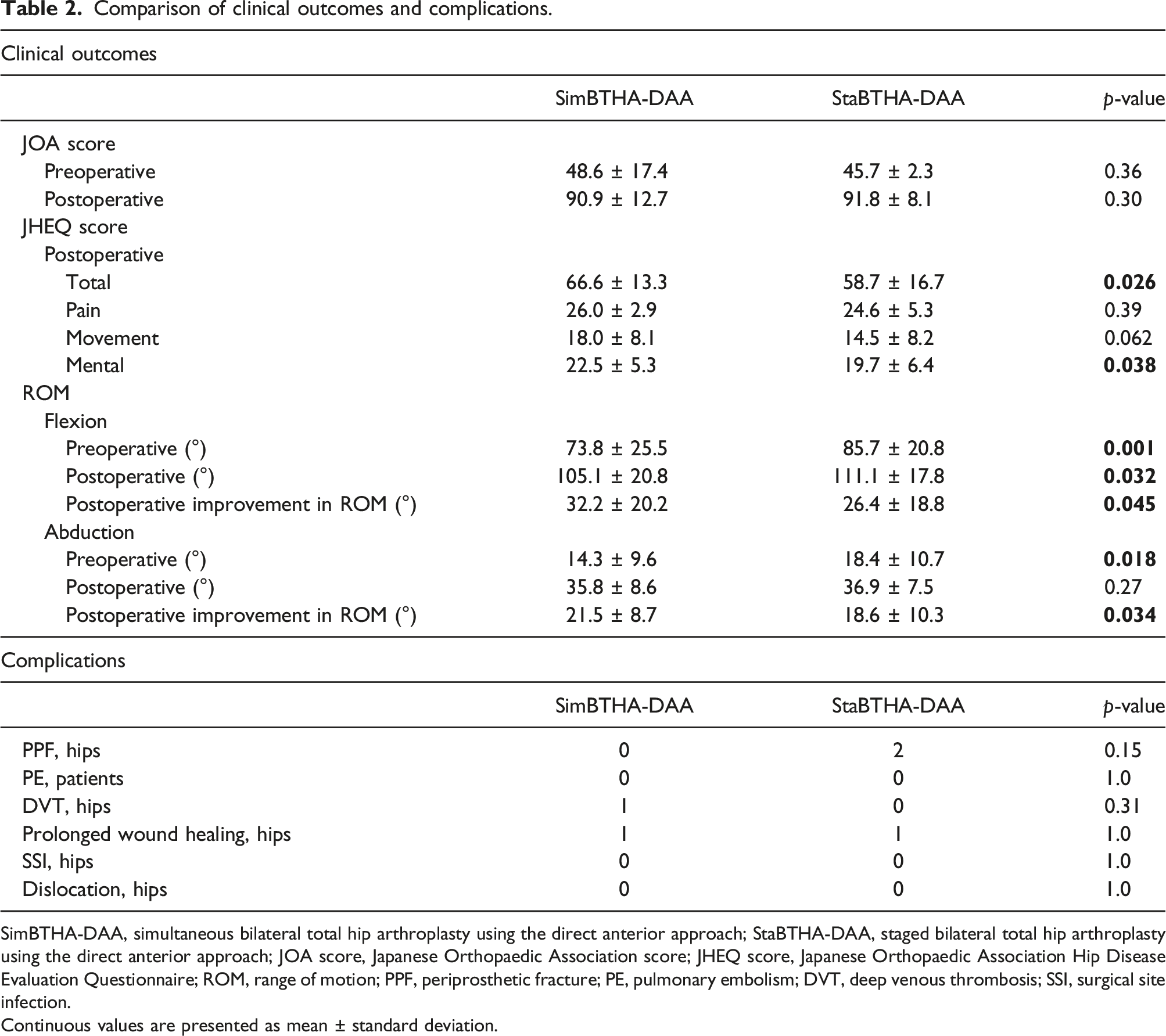
SimBTHA-DAA, simultaneous bilateral total hip arthroplasty using the direct anterior approach; StaBTHA-DAA, staged bilateral total hip arthroplasty using the direct anterior approach; JOA score, Japanese Orthopaedic Association score; JHEQ score, Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire; ROM, range of motion; PPF, periprosthetic fracture; PE, pulmonary embolism; DVT, deep venous thrombosis; SSI, surgical site infection.
Continuous values are presented as mean ± standard deviation.
Perioperative outcomes
Comparison of perioperative and radiographic outcomes.

SimBTHA-DAA, simultaneous bilateral total hip arthroplasty using the direct anterior approach; StaBTHA-DAA, staged bilateral total hip arthroplasty using the direct anterior approach.
Continuous values are presented as mean ± standard deviation.
Radiographic outcomes
There were no aseptic loosening cases in either group, and there were no significant differences in stem sinking and LLD between the two groups (Table 3).
Discussion
Summary of the literature discussing simultaneous versus staged bilateral total hip arthroplasty via the direct anterior approach.
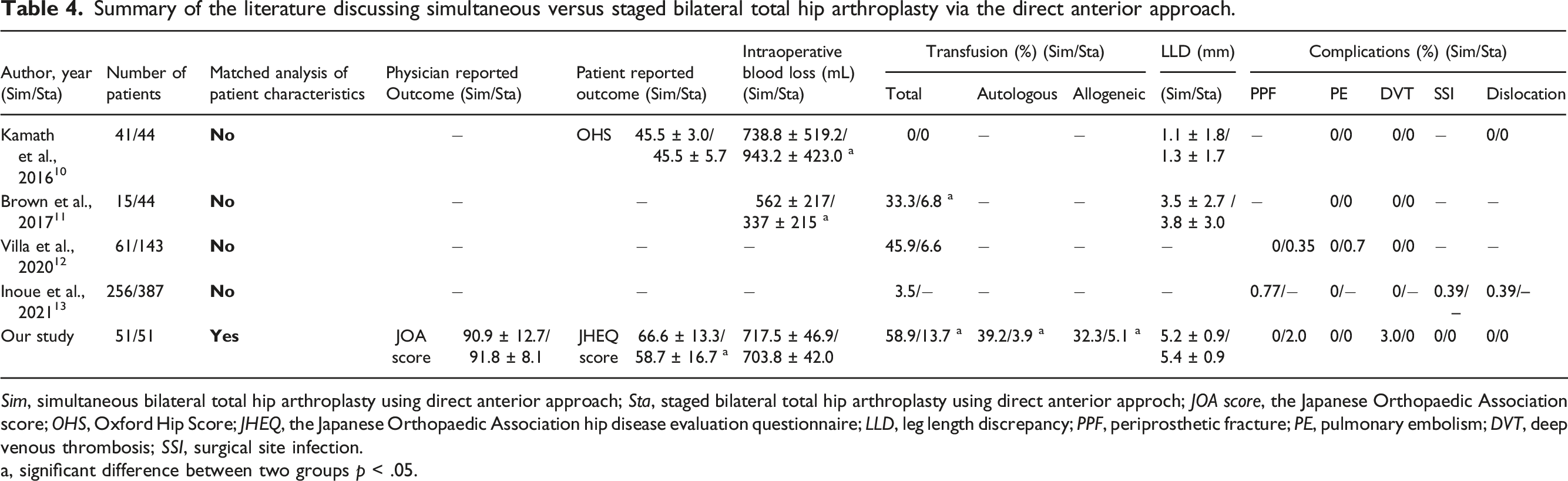
Sim, simultaneous bilateral total hip arthroplasty using direct anterior approach; Sta, staged bilateral total hip arthroplasty using direct anterior approch; JOA score, the Japanese Orthopaedic Association score; OHS, Oxford Hip Score; JHEQ, the Japanese Orthopaedic Association hip disease evaluation questionnaire; LLD, leg length discrepancy; PPF, periprosthetic fracture; PE, pulmonary embolism; DVT, deep venous thrombosis; SSI, surgical site infection.
a, significant difference between two groups p < .05.
The present study showed that the postoperative JOA score, as a physician-reported outcome, was not significantly different between the two groups. Bhan et al. similarly indicated no significant difference in Harris Hip Score between SimBTHA using the posterior approach (SimBTHA-PA) and StaBTHA-PA 6 months after surgery. 12 In this study, the total JHEQ score was significantly higher in the SimBTHA group than in the StaBTHA group. In contrast, a similar patient-based assessment, the Oxford Hip Score (OHS), reported no difference between the SimBTHA and StaBTHA groups. 15 The mental JHEQ score was significantly different between the two groups, and this may have influenced the difference between OHS and JHEQ because OHS has no mental score component. However, because preoperative JHEQ evaluation was not performed, the possibility of selection bias cannot be ruled out. Further studies are needed to clarify the influence of the mental score.
Because the postoperative ROM in flexion was significantly better in the StaBTHA than in SimBTHA, although pre-and postoperative ROM improvements in flexion and abduction were statistically different between the SimBTHA and StaBTHA groups, it cannot be concluded that the SimBTHA group had better ROM improvement than the StaBTHA group. In the present study, the SimBTHA group is indicated for the worse ROM patient, and preoperative flexion is significantly different between the two groups. As Yoshii et al. reported, after simultaneous THA, the patients can exercise sitting and squatting that need bilateral hip flexion. 23 A matched analysis with a preoperative ROM is needed to testify whether SimBTHA is better than StaBTHA in the future.
The complication rates were not significantly different between the two groups. In a study using registry data, Partridge et al. reported that complications, including PE, were more commonly associated with SimBTHA than with StaBTHA when using various surgical approaches. 13 Contrarily, the rates of PE, DVT, SSI, and dislocation were not significantly different between SimBTHA and StaBTHA. 12 Similar to the findings of previous studies using the DAA, we found no significant differences in complications, such as PE, DVT, SSI, and dislocation, between the groups (Table 4). In this study focusing on the DAA in matched patient background, we found that SimBTHA-DAA was comparable to StaBTHA-DAA in terms of complications.
Intraoperative blood loss was not significantly different between the two groups in this study. Contrastingly, the blood transfusion rate was higher in the SimBTHA-DAA than in the StaBTHA-DAA. These results indicate that blood loss per surgery was higher in SimBTHA-DAA because blood loss was expressed as the sum of the first- and second-stage surgeries. While increased blood loss may be a disadvantage of SimBTHA-DAA, no patients who received auto-BT required allo-BT later. Romagnoli et al. 5 showed that appropriate transfusion protocols could reduce the use of allo-BT in SimBTHA. Sarpong et al. 34 suggested that risk factors for allo-BT in SimBTHA were female sex and lower preoperative hemoglobin levels (<12 g/dL). Considering these studies, auto-BT should be considered, especially for female patients with low hemoglobin levels, to avoid allo-BT in SimBTHA-DAA.
Postoperative LLD was not significantly different between the two groups. Residual LLD after THA is associated with poor postoperative outcomes and patient satisfaction. Lecoanet et al. 35 showed that the DAA with a supine position made it easier to limit LLD, as the surgeon identified the anatomical landmark accurately. This study showed that leg length control was useful in both groups.
This study has some limitations. First, the sample size was relatively small; however, the sample size was considered sufficient for the study, based on the G*power calculation for each group. Second, because this was retrospective study, selection bias for surgical procedures may have occurred. Finally, preoperative JHEQ score was not available. The possibility of preoperative patient status differences cannot be excluded. In the future, a large-scale randomized controlled trial is needed to confirm these results.
Conclusion
In this study of propensity score matched patient groups, the allo-BT rate was significantly higher in SimBTHA-DAA group in the supine position than in StaBTHA-DAA group. The two groups showed no significant differences in physician-reported outcomes, radiographic outcomes and complications. With these observations we can conclude that SimBTHA through DAA leads to similar outcomes after StaBTHA through DAA except for an increase in blood transfusion requirements in the SimBTHA group. Auto-BT may be useful for avoiding allo-BT in SimBTHA.
Footnotes
Acknowledgements
The authors would like to thank Dr. Makoto Akagawa and Dr. Takenobu Fujisawa for their surgical contributions to the cases in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.