
Abstract
Background
The study compares single versus combination fixation of distal femur fractures.
Method
We retrospectively reviewed patients over 60 between January 2016 and December 2022. Union rate, ambulatory status and complication rate were primary outcomes. Secondary outcomes included quality of reduction, operative time and rate of blood transfusion.
Results
A total of 92 patients received single fixation, and 22 patients received combination fixation. There was no difference in rate or time of fracture union. Patients with dual fixation were allowed to weight bear on discharge significantly more than single fixation patients (50% vs. 18.9%, p = 0.003). Intramedullary nail fixation, as a single method or combined with lateral plating, was associated with earlier weight bearing. Immediate post-operative weight bearing significantly increased the likelihood of discharging to home or rehabilitation versus discharging to a transitional care facility (p < 0.00001). There was no difference in the rate of blood transfusion, complication or mortality. Medial translation of the distal articular block was significantly lower with dual fixation (1.2% vs. 3.4%, p = 0.021). Operation time was longer with combination fixation (183 min vs. 134 min p < 0.001).
Conclusion
Combination fixation allows earlier weight bearing, at the cost of longer operation time.
Introduction
Distal femur fractures occur at high rates in the elderly and predominantly affect women over the age of 60.1,2 With prevalent comorbidity among this age group, patients are vulnerable to early morbidity and mortality following this orthopaedic injury.1–3
Distal femur fractures have traditionally been stabilised with either a lateral locking plate or retrograde intramedullary nail. Current literature proposes limitations to these interventions with studies showing that up to one in four patients are at risk of fracture non-union.4–8 Furthermore, patients are often instructed to remain non weight bearing (or touch weight bearing) for months following surgery. This reduction in mobility postoperatively is associated with high rates of physical disability and complications which include infection, delirium and venous thromboembolism.8,9
Over recent years, surgical recommendations have evolved, with promising outcomes reported with combination fixation techniques using dual plates or both lateral locking plate plus intramedullary nail.6,7,10,11 Proposed advantages of combination fixation include earlier weight bearing and lower fixation failures.1,11 Unfortunately, there remains insufficient quality evidence in current literature to inform surgical practice. The aim of this study is to provide additional information on the comparison of single versus combination fixation techniques in the surgical management of distal femur fractures.
Methods
Study design and data collection
Patients over the age of 60 admitted to Christchurch Hospital, a level one trauma centre, with a distal femur fracture between 1 January 2016 and 31 December 2022 were reviewed retrospectively for inclusion into this study. Patients were identified using the International Classification of Diseases coding (ICD-10), specifically; S723, S7240. Patient demographics, fracture characteristics, operative details and follow-up data were recorded. Periprosthetic fractures were also included. Patients with pathological fractures, segmental fractures, fractures managed conservatively and fractures treated with distal femur replacement were excluded.
All patients were divided into two cohorts according to their surgical treatment. Patients who received single fixation, with a lateral locking plate or retrograde femoral nail, were placed into one group. Patients who received combination fixation, with dual plating or retrograde intramedullary nail plus lateral plating, were placed into the combination fixation group.
Baseline demographics of each patient, including age, sex, body mass index (BMI), smoking status, diabetes status and American Society of Anaesthesiologist (ASA) score were extracted from medical records. Individual radiographs were analysed by the authors to stratify fractures by the AO classification system: Type 33A, 33B and 33C. Open and periprosthetic fractures were also identified. Medial comminution was determined on preoperative films, if present.
The primary outcomes of interest compared the rate of fracture union, ambulation status at discharge and rate of postoperative complications. These were recorded by reviewing follow-up radiographs and health records. Secondary measures recorded rate of blood transfusion, length of operation time, quality of reduction and length of hospital stay. Mortality rate was measured at 30 days and 12 months.
Quality of reduction was measured by two techniques; medial translation of the distal articular block and the anatomical lateral distal femur angle (aLDFA) as described by Lee et al. in their multicentre retrospective cohort study.6 Medical records were reviewed to record operation time in minutes and length of hospital stay in days.
Fracture union was identified both clinically and radiologically from patient records as described in a study by Bologna et al.7 Clinical notes were reviewed to identify painless weight bearing and progressive plain films were analysed to identify at least three healed cortices and/or the presence of callus formation. Time to union was measured in weeks. Delay in fracture union was defined as a fracture taking longer than six months to heal and/or requiring revision surgery during follow up for delayed fracture union or non-union.
Operative technique
Lateral plating was standardised using a stainless steel anatomical fixed or variable angle locking plate, augmented with cables or screws outside the plate as dictated by the fracture pattern. Minimally invasive bridging technique was preferred, however, when alignment was suboptimal through indirect techniques, an open reduction was performed.
In dual plating, an additional medial incision was made using a medial subvastus approach. The medial column was then stabilised with a buttress plate. The choice of medial plate was at the discretion of the operating surgeon, and since there are no pre-contoured medial distal femur locking plates, a variety of implants were used.
Retrograde femoral nail was completed through a medial parapatellar arthrotomy, using indirect reduction techniques. Nail-plate fixation started with a short retrograde femoral nail, with proximal and distal locking. This was followed by a long lateral locking plate, usually spanning the length of the femur via a minimally invasive technique to end at the level of the lesser trochanter (Figure 1). Locking screws into the plate was directed anterior and posterior to the retrograde nail in the distal femur. Selection of surgical technique was rationalised on an individual basis, the majority according to surgeon preference and familiarity of technique.
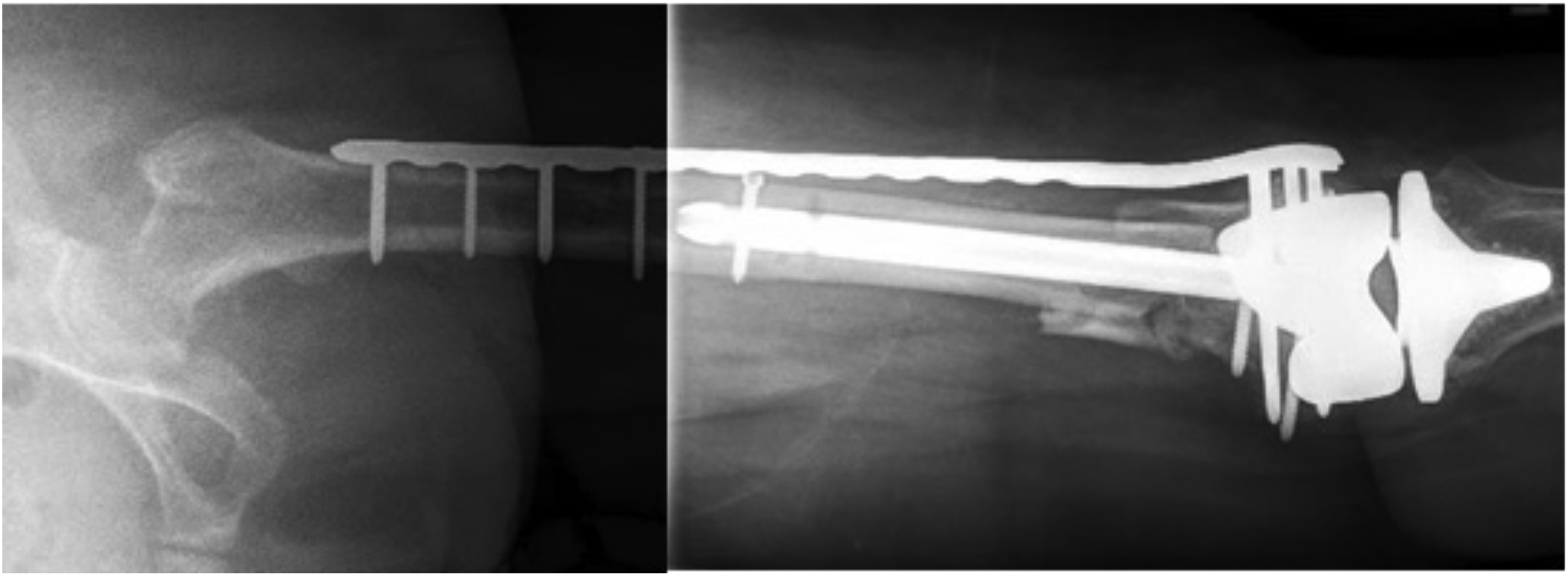
Postoperative X-ray of combined intramedullary nail plus plate fixation.
Post-operative protocol was standardised using antibiotic prophylaxis and venous thromboembolism prophylaxis. The knee was allowed full range of motion. The weight bearing status of each patient at the end of the procedure was determined at individual surgeon discretion.
Ethics
The study was approved by the institutional review board. All data was anonymised and only accessed through secure password-protected computers.
Statistical analysis
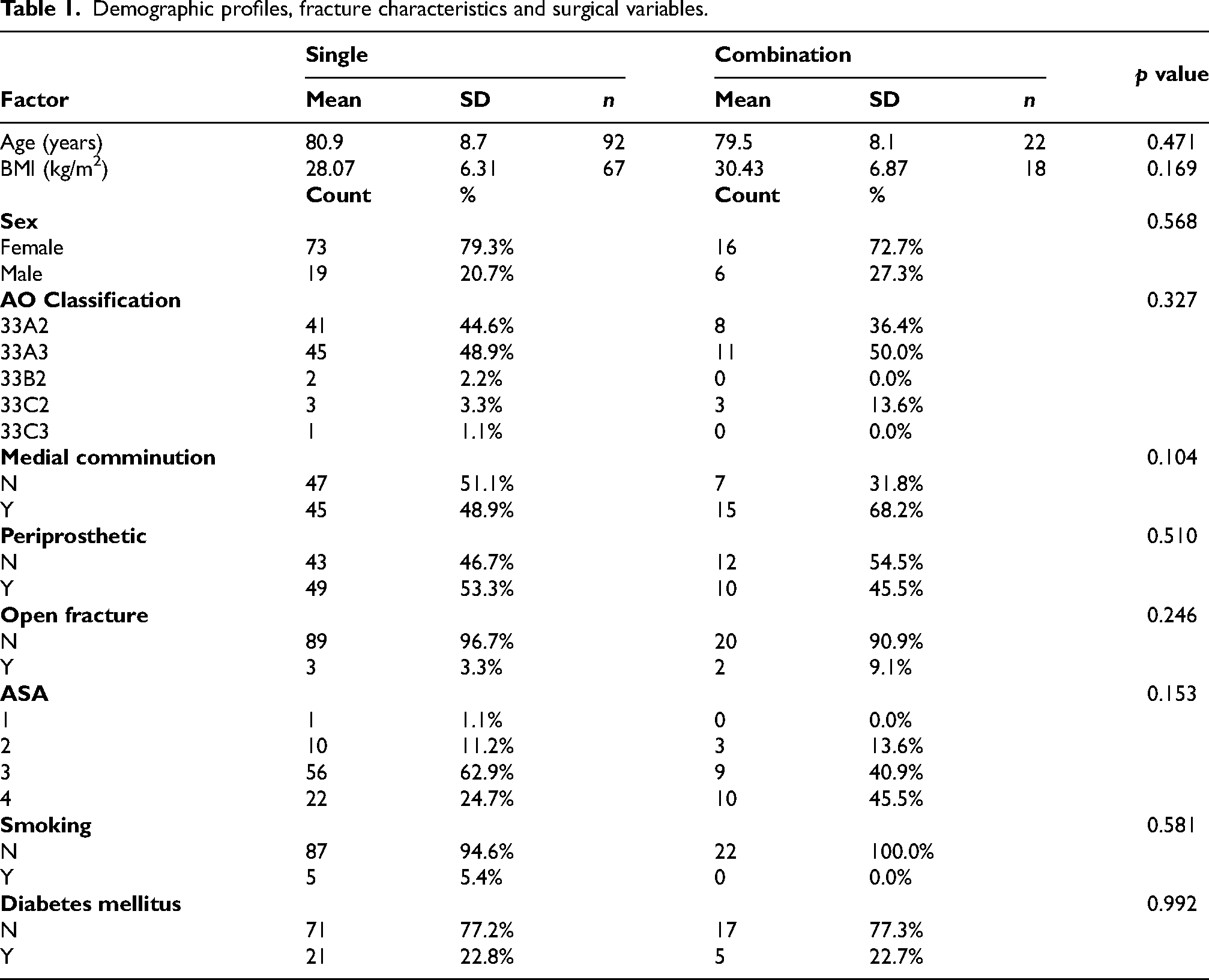
Data on patient demographics, fracture characteristics and surgical details was gathered and summarised in Table 1. A biostatistician was recruited to analyse the data. Individual counts and percentages were used to measure categorical variables, while mean and standard deviation (SD) were used to record continuous variables. The demographic and clinical features were compared between the two treatment groups using Chi-square tests, independent t-tests and Mann–Whitney U tests as appropriate. The continuous outcome measures were compared using Mann–Whitney U tests and the dichotomous outcomes using Chi-square or Fishers exact tests. All analyses were undertaken using SPSS v28, and a two-tailed p-value <0.05 was taken to indicate statistical significance.
Demographic profiles, fracture characteristics and surgical variables.
Results
A total of 114 patients met criteria for inclusion into the study. These patients were subsequently divided into two groups according to their surgical management. A total of 92 patients received single fixation with lateral locking plate or intramedullary nail, and 22 patients received combination fixation with dual plate or lateral locking plate plus intramedullary nail.
There were significantly more females included in the study with 79.3% females in the single fixation group and 72.7% females in the dual fixation group. The mean age was 80.9 (SD 8.7) in the single group and 79.5 (SD 8.1) in the combination group. Other patient factors such as BMI, medical history of diabetes mellitus (DM) and current smoking status were reviewed. The mean BMI among the entire group fell within the overweight range at 29.3 kg/m2. In this study, 22.8% of all patients had DM. Of the patients who received single fixation, 5.4% were actively smoking compared to no active smokers in the combination group; however, this difference was not statistically significant. The majority of patients in this study were classified as ASA three or four, reflecting significant comorbidities across the two cohorts.
There was no difference in AO fracture classification between the two cohorts. Additionally, there was no variation of open or periprosthetic fractures or fractures with medial comminution between each group. Overall there was no significant difference in patient factors or fracture characteristics across the study (p > 0.05 for all), and baseline characteristics were considered to be homogenous.
Outcomes are summarised in Table 2. Fracture union occurred in 78.3% of all cases, at a mean of 13 weeks with single fixation versus 16 weeks with combination fixation (p = 0.874). There was no significant variation in non-union between each cohort, with 22.4% in the single-implant fixation group versus 21.1% in the combination fixation group (p = 1.000). Postoperative complications – excluding non-union and delayed union – did not vary significantly between each group (7.6% vs. 13.6%; p = 0.403).
Outcomes.
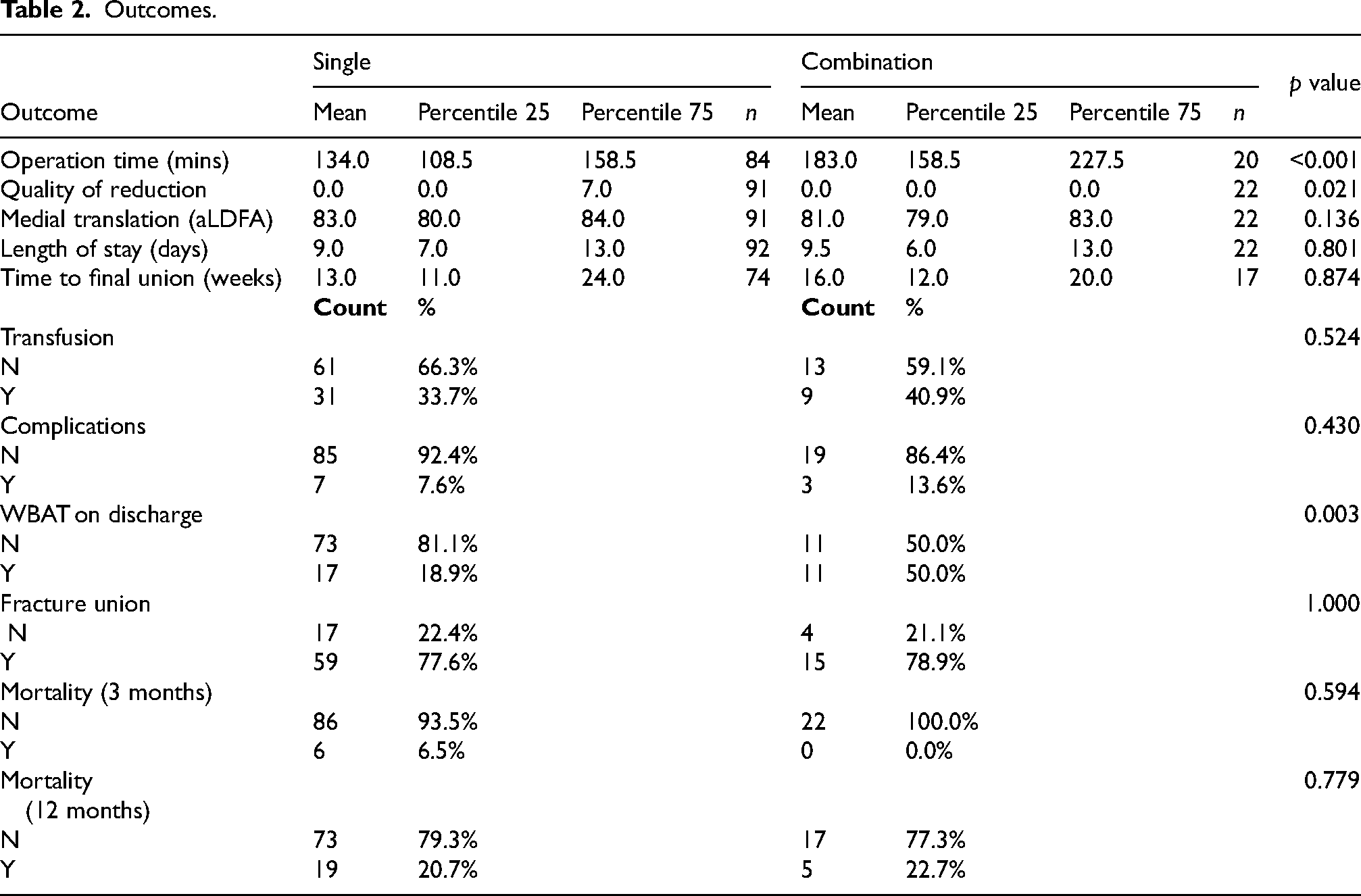
Of significance, while 18.9% of patients receiving single fixation were able to weight bear as tolerated (WBAT) on discharge, up to 50% of patients treated with combination fixation were allowed to WBAT (p = 0.003). The rate of patients able to WBAT in the single fixation group can be broken down into 27.3% in the retrograde nail group, and 17.3% in the lateral locking plate group. Among those receiving combination fixation, 81.8% of patients who underwent nail-plate fixation were allowed to WBAT, compared with only 18.2% of patients in the dual-plate cohort. Patients able to WBAT were much more likely to discharge to home or directly to rehabilitation compared with discharging to a transitional level care (TLC) facility for up to three months of non weight bearing (p < 0.00001) (Figure 2).
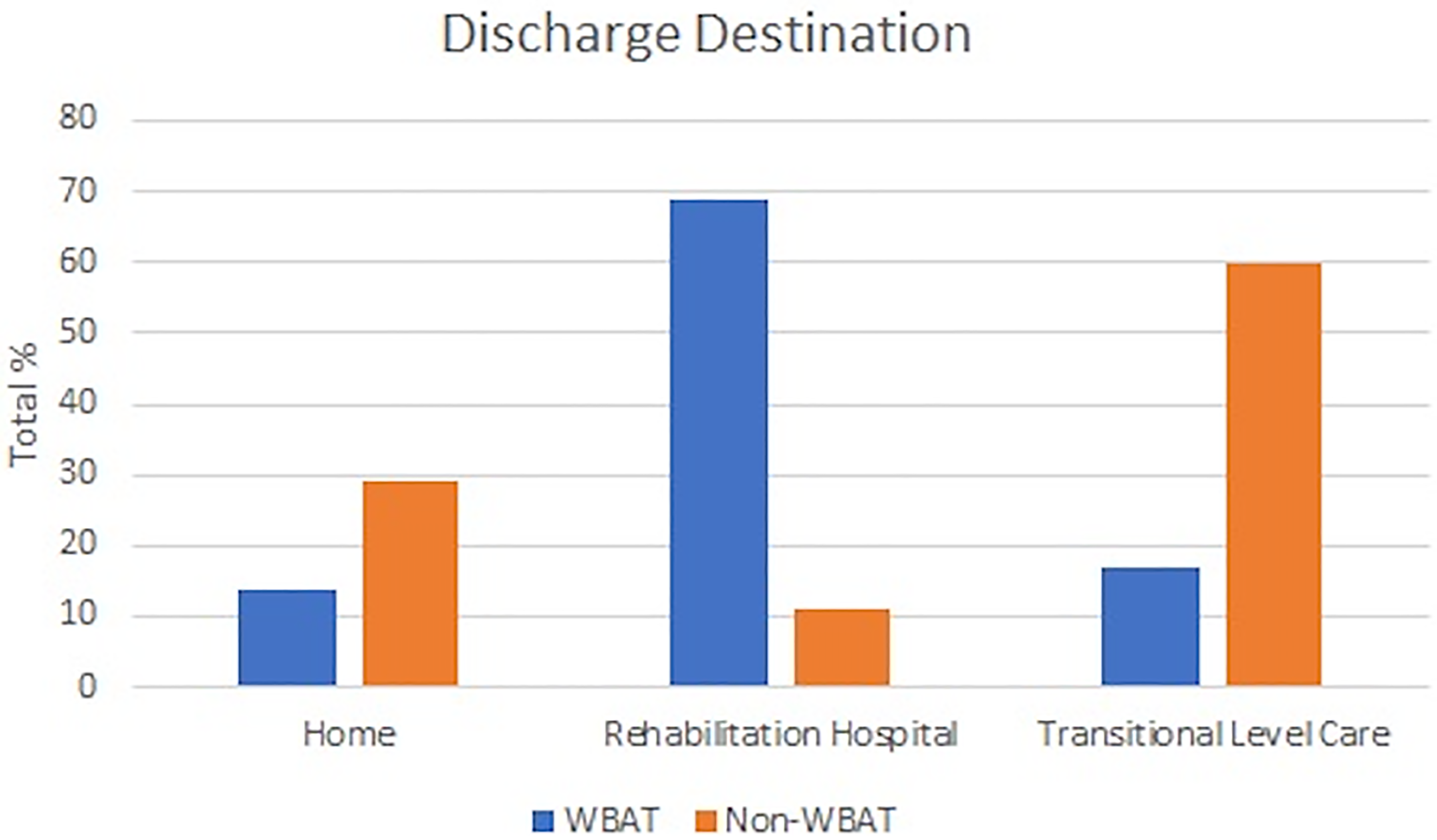
Graph demonstrating ambulation status according to discharge destination.
There was no statistically significant difference between groups for rate of red blood cell transfusion. Operation time was significantly longer in the combination group when compared with the single fixation group (183 min vs. 134 min; p < 0.001). Medial translation of the distal articular block was significantly lower in the combination fixation cohort (1.2% vs. 3.4%; p = 0.021), while aLDFA had no statistically significant variation. Length of hospital stay was recorded as a median of 9.0 days in the single group and 9.5 days in the combination group.
There was no difference in rate of mortality at 30 days and 12 months (p > 0.05). Among all patients included in this study, a total of seven patients were lost to follow up; four patients in the single fixation group versus three patients in the combination fixation group. Ten patients died prior to fracture healing; nine deaths were recorded in the single fixation group and one in the combination fixation group.
Discussion
Patients over the age of 60, who received either single or combination fixation for a distal femur fracture between a six-year period, were evaluated to compare surgical techniques. There were no significant baseline differences in patient demographics. No patient characteristic was identified as being specifically predictive of the primary outcome. In contrast, other studies have outlined BMI and DM as risk factors for reduced fracture union and reoperation.6,12,13 This is likely related to the underlying pathophysiological changes which impair fracture healing through increased joint stress, poorer bone quality and systemic inflammation.14 Notably, the majority of patients included in this study had BMI classified in the overweight category, with an ASA score indicating the presence of significant underlying comorbidities. With an ageing population and increasing rates of obesity internationally, the prevalence of systemic disease is likely to influence outcomes for orthopaedic patients. This health issue indicates a need for more powerful evidence to inform surgical practice in order to reduce morbidity and mortality in geriatric distal femur fractures.
Fracture characteristics were also similar between both groups, meaning more complex fractures were not necessarily more likely to receive combination fixation. Fracture characteristics also lacked significant correlation with the measured outcomes. This is in contrast to current evidence which describes increased risk of fracture non-union with medial comminution and open fractures.6,7,13 This is likely to be secondary to more complicated operative management and higher infection rates.11
Union has been defined both clinically and radiographically as the ability to weight bear without pain and evidence of a bridging callus forming across a minimum of three cortices. This study did not show increased rate of union with combination fixation, nor was there a significant difference between time to union in each group. This is in contrast to similar sized studies which found reduced rate of fracture non-union or delayed union and significantly decreased time to fracture healing with combination fixation.1,7,11
The data demonstrates a significant difference in ambulation status at discharge, with combination fixation allowing for earlier weight bearing. This clinically significant finding is also described in the study by Garala et al.1 This is an important outcome, as allowing for immediate ambulation reduces physical disability, postoperative complications and acute mortality.9 Furthermore, elderly patients are at higher risk of acute and chronic cognitive impairment which can be a barrier when complying with restricted weight bearing to support fracture healing. Therefore, removing this barrier will likely facilitate fracture union among the geriatric population.
Of interest, the rate of patients able to WBAT in the dual-plate fixation group is similar to the single-implant fixation cohort, while fixation with intramedullary nail using single or combined techniques was associated with earlier weight bearing. We cannot explain this finding retrospectively, though hypothesise some of the dual-plate patients may have had additional medial plate as a reduction aid, and not necessarily to increase the stiffness of the osteosynthesis. Medial translation of the distal articular femoral block was a significant finding, suggesting improved quality of reduction with combination fixation. Yet, this finding did not have any significant impact on the primary and secondary outcomes evaluated in this study.
Allowing for WBAT was associated with significantly more discharges to home or to the rehabilitation hospital rather than to a temporary TLC facility (Figure 2). Any weight bearing status other than WBAT was associated with more discharges to TLC. These facilities are where patients convalesce with increased nursing care whilst having restrictions on their weight bearing – this placement could be for up to 12 weeks. To note, there is limited rehabilitation of patients at these facilities. If patients are allowed to WBAT, they are more likely to return to baseline function with discharge to home, or to earlier rehabilitation, avoiding months spent in TLC. There is also a cost-saving difference, if there are less discharges to TLC. Overall, earlier weight-bearing has clinically favourable outcomes on multiple levels.
In keeping with the findings in a recent meta-analysis by Tripathy et al., there was no significant difference in blood transfusion, complication or union rate between single fixation and dual plating methods. This highlights several operative risks that are similar between each group, suggesting no significant increase in harm with combined fixation techniques. The caveat of this positive outcome is longer operation time which can be associated with important disadvantages. Risks associated with longer operation time have been described in a meta-analysis by Hang et al.15 Across all surgical specialties there was a statistically significant increase in complications in operations that were prolonged by increments of 30 min (14%) and 60 min (21%). In this study, combination fixation took an average of 49 minutes longer. Specific to orthopaedic surgeries, higher risk of complications with prolonged operative time included surgical site infection, urinary and chest infection, cardiac complications and sepsis.15 These results are not specific to distal femur fractures, but significantly longer operation times in combined fixation poses a theoretical risk in light of these findings. It is likely that as dual fixation becomes increasingly more popular, the surgical technique itself will be refined and the operation times may be optimised.
Limitations to this study have been considered. This study retrospectively evaluates a small sample population and the values may be underpowered. However, the sample size in this study is comparable or even exceeds other similar studies published in the literature. Garala et al. had 67 patients to compare single locking plate versus nail plus plate fixation,1 Bologna et al. studied 21 patients in their review of single versus dual fixation,7 and Claireaux et al.'s systematic review (including 14 studies for a total sample size of 753) averaged only around 50 patients per study.5 The limited overall number of patients receiving combination fixation in this hospital reflects a temporal difference with all cases occurring in the last three years of the study. This is a result of increasing popularity of this technique with emerging evidence highlighted in the forementioned studies.
The inherent properties of a retrospective cohort analysis make it difficult to determine a direct correlation between the surgical intervention and its outcomes. Dual plate and plate plus nail fixation were placed in one cohort, however, there are differences between these fixation strategies. The overall quality of this research may also be compromised by poor documentation in health records and natural human error.
The above considerations have potential to explain gaps in this study. Firstly, the absence of correlation between improved reduction quality and rate of fracture union is likely multifactorial. This finding has been described with combination fixation in other studies, suggesting an additional advantage for this technique.7 Quality of reduction was individually calculated on radiographs by the authors, therefore, a variation in this technique may have introduced a measurement bias that skewed the results. Another important consideration is that complications other than problems with fracture union were categorised together as a rate. Therefore, the general outcomes for each case are unclear, and patient satisfaction was not considered. Finally, few patients were lost to follow up or passed away prior to fracture union which may influence the internal validity of the outcomes. The remaining findings are otherwise consistent with available research, and the homogeneity between the two cohorts reflects a well-balanced population.
This study did not evaluate methods of single versus combination fixation separately, as the small sample size limited further stratification of the two cohorts and prevented valid subgroup comparative statistical analysis. There are some theoretical differences between dual-plate fixation and nail-plate fixation. Dual plating is debatably associated with higher risk of soft-tissue damage and potential to disrupt blood supply to the periosteum, increasing infection risk.16 In contrast, intramedullary nail plus plate fixation encourages smoother transfer of force through the implant along with the anatomical axis, providing equal stability without soft-tissue damage.16 Fractures with articular comminution or surrounding an existing prosthesis may limit use of this method of fixation.
Regardless of the theoretical differences, the proposed biomechanical advantage of combination fixation is greater stability around the fracture site.17 Biomechanical studies show there is increased axial stiffness with both dual-plate and nail plate fixation compared to single implant fixation, providing the rationale for earlier weight bearing and reduced risk of implant failure.11,18 Without further stratification of the two combined fixation techniques in this study, the optimal fixation of distal femur fractures remains unclear.
There are a number of small studies that evaluate single versus dual plating4,10; however, there remain even fewer studies which compare these methods to lateral locking plate plus intramedullary nail fixation. Future studies should evaluate these combination techniques in a larger sample of patients prospectively, to provide higher quality evidence for the treatment of distal femur fractures. A new study Dual Implant Versus Single Implant Distal End of Femur is a randomised control trial which is in the process of evaluating these interventions and will likely provide further data to address this clinical question.19 Distal femoral replacement is also under investigation as a potential improvement on our standard single fixation methods,20 and new studies to compare the outcomes of this technique will help guide future orthopaedic practice.
In conclusion, combination fixation shows promising advantages over single fixation of distal femur fractures, with early weight bearing demonstrating the most significant outcome. Although considerations should be made of risks associated with longer operation times, valuable health benefits are associated with immediate mobilisation following surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.