
Abstract
Femoral neck system (FNS) is a novel fixed-angle gliding device combining a sliding bolt and an anti-rotational screw to treat femoral neck fractures. It was proven to have comparable biomechanical strength to sliding hip screws. Tip-to-apex distance (TAD) is an established assessment for fixation quality in sliding hip screws. The purpose of our study was to evaluate whether TAD can be used in FNS implant to predict fixation failure. Seventy-six patients receiving FNS fixation for intra-capsular hip fracture were included. TAD was measured from post-operative radiographs and clinical outcomes were collected with a mean follow-up of 14.1 months. The mean TAD for patients who experienced fixation failure was 20.7 mm, versus 19.7 mm for those who did not (p = 0.395). Subgroup analysis among fractures with good reduction quality, defined as no varus angulation, less than 5 degrees of retroversion, and less than 4 mm cortical translation, did not demonstrate statistically significant difference in the mean TAD between failure and non-failure group (20.7 mm vs 19.5 mm, p = 0.68). We conclude that in our study of modest sample size, there was not demonstrable association between TAD and fixation failure in intra-capsular neck of femur patients treated with FNS.
Introduction
Despite technological advances, complication rates associated with fixation of intra-capsular hip fractures are still high, with re-operation rates up to 21% in a large scale randomized controlled trial. 1 Femoral neck system (FNS) is a recently developed implant designed to address the clinical challenges associated with hip fracture fixation. It is a fixed-angle gliding screw-plate construct that contains a sliding bolt and an anti-rotational screw that provides controlled collapse and rotational ability at the same time. It has similar biomechanical performance as a dynamic hip screw with an anti-rotational screw. 2
Comparative studies and meta-analysis have shown early promising results in FNS implants, with lower complication rates and faster union times.3,4 Previous biomechanical study has shown that cut-out, instead of screw-backout, was the primary mode of failure of FNS, as in the case with dynamic hip screws. 2
Tip-to-apex distance (TAD) has been shown to predict mechanical failure in fixation of trochanteric hip fractures.5,6 Whether it could be applied to a similar angular device with a similar mode of failure, such as FNS, is unknown – this is a clinically important question as it could potentially guide intraoperative decision and management to optimize fixation outcomes. Therefore, the aim of the study was to determine if TAD and other implant related factors such as implant position could predict fixation failure.
Methods
This is a multicenter retrospective study involving of patients treated with FNS between 1 May 2020 and 1 May 2021 across five regional hospitals. Clinical data was obtained through an electronic database query (Clinical Data Analysis and Reporting System) and review of medical records. Inclusion criteria involved patients receiving surgical fixation with FNS for neck of femur fracture (AO/OTA type 31.B1-2). Exclusion criteria were patients with fracture without prior history of trauma, pathological fractures, and fractures involving both the neck and trochanter of femur. Ethics approval was obtained and need for informed consent was waived due to the retrospective nature of this study.
Baseline data including age at surgery, sex, operative side, and types of the fracture were recorded. Radiological assessment of implant position and reduction quality were made using the first post-operative radiograph. All radiological data were collected and analyzed by three authors (one orthopedic specialist and two higher orthopedic trainees), with discrepant measurements re-measured until agreement was reached between at least two authors.
The position of the bolt was classified into superior, central, or inferior third on anteroposterior view, and anterior, central, or posterior third on lateral view by the position of bolt in the femoral head. TAD was measured with a similar technique published by Baumgaertner et al., 5 and defined by the distance between tip of the bolt to the apex of femoral head. Measurement was taken from both anteroposterior and lateral views. The measured distance was corrected for radiographic magnification which is determined by dividing the known bolt diameter (10 mm) with the apparent bolt diameter measured on the radiograph (Figure 1).
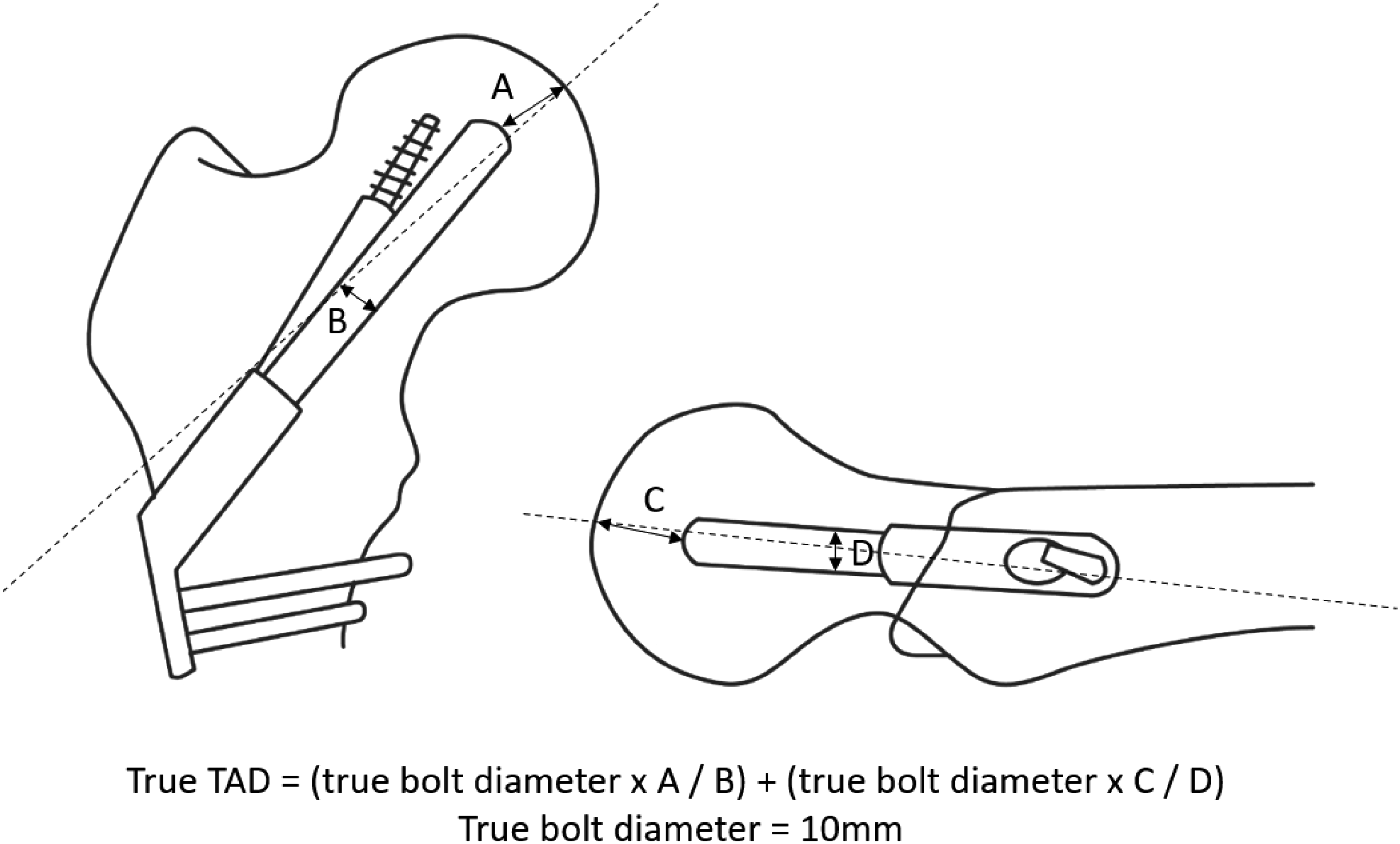
Calculation of tip-to-apex distance on FNS implant.
The quality of reduction was also assessed. The reduction was categorized into good if there was absence of varus reduction, 7 retroversion of more than 5 degrees, or cortical translation of less than 4 mm. 1 If the above criteria were not fulfilled, the reduction would be categorized as poor. Complications were evaluated by reviewing territory-wide electronic medical records of post-operative follow-up radiographs. Primary outcome involved fixation failure as defined by presence of cut-out, varus collapse, or avascular necrosis as outlined by Ficat stages III and IV. 8
SPSS software (version 26, IBM, Armonk, USA) was utilized to analyzed the data. Mann–Whitney U test was used for comparison of TAD between fractures that resulted in fixation failure versus those which did not. Fisher's exact test was used to compare differences in bolt positions between the two groups. p-Value of <0.05 taken was taken as statistically significant.
Results
Seventy-six patients with intra-capsular hip fractures treated with FNS between the study period were included in analysis. The mean age of patients was 74.4 ± 15.4 years. There were 15 males and 61 females. There were 65 undisplaced fractures (Garden I or II) and 11 displaced fractures (Garden III or IV). Sixty-seven (88%) have met the criteria for good reduction. The mean duration of follow-up was 14.1 months.
Ten patients developed fixation failure (13.2%), among which 5 had serial implant displacement with varus collapse and subsequent nonunion. Three developed concomitant avascular necrosis. Four was revised to hemiarthroplasty or total hip arthroplasty and one opted not for re-operation due to old age.
There were a total of 11 cases of avascular necrosis (14.5%) with 8 showing fracture union at time of AVN. Re-operation rate was 7.9% (n = 6), with 5 revised to arthroplasty and 1 had implant removed due to impingement. Deep surgical infection was ruled out in failure cases.
Among the 76 patients who received FNS fixation, 71 of them received a one-hole plate while 5 of them received a two-hole plate. Mean TAD was 19.8 ± 5.6 mm (Figure 2). 90.7% of the implants were put in center or inferior third on anteroposterior radiograph, while 84.2% were put in center or posterior third on lateral radiograph (Table 1).
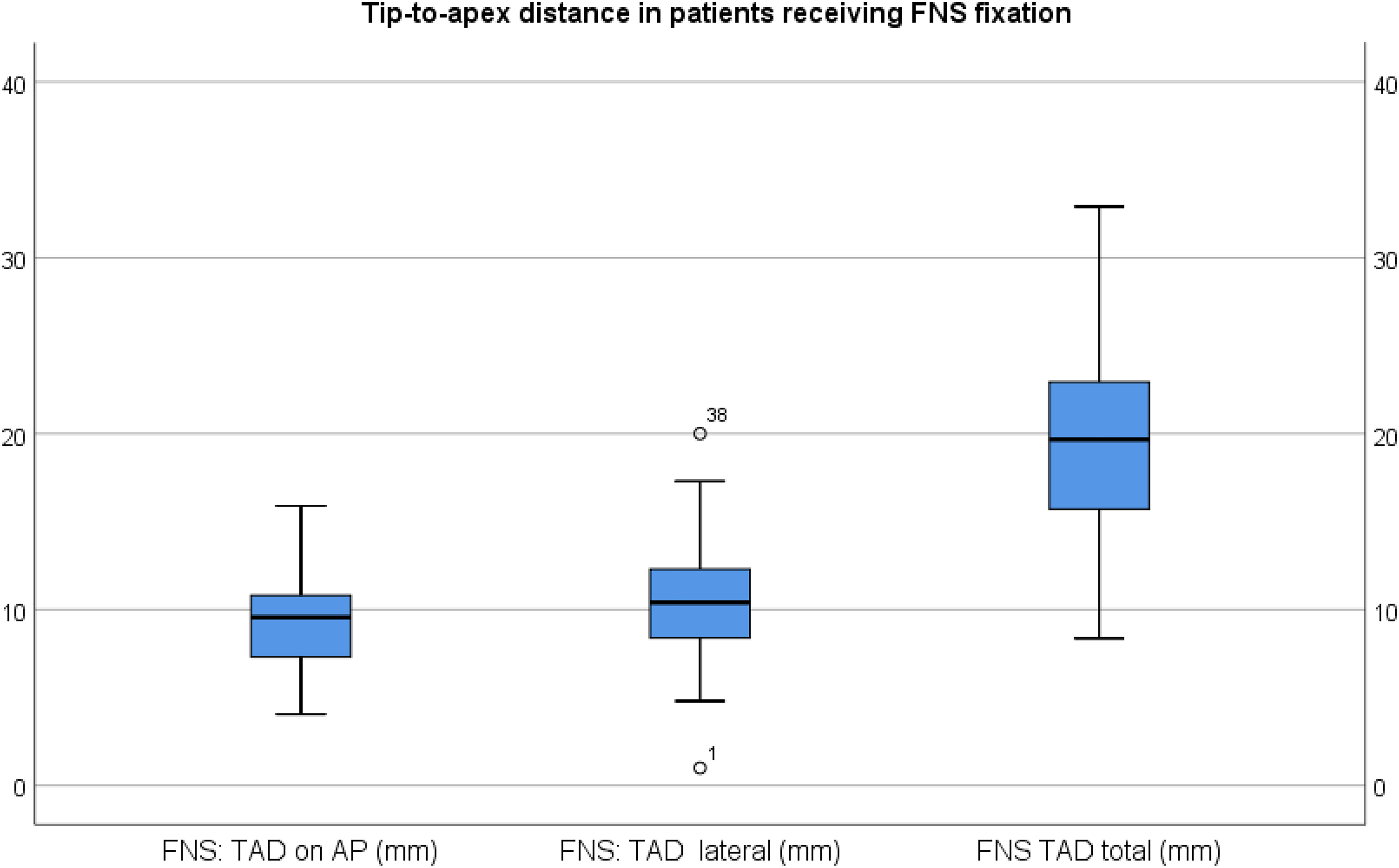
Tip-to-apex distance in AP view, lateral view, and combined.
Position of bolt related to the occurrence of fixation failure.
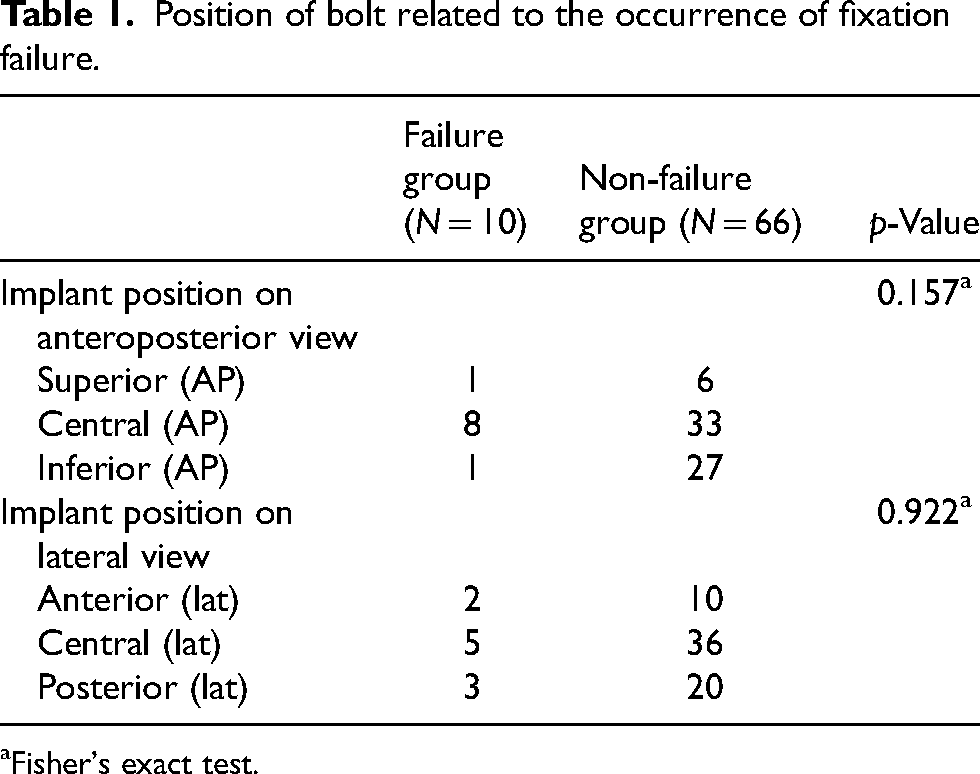
Fisher's exact test.
Table 2 shows the distribution of bolt position and TAD with respect to complications. The mean combined TAD of the failure group was 20.7 mm, versus 19.5 mm in the non-failure group (p = 0.678), the difference of which was not statistically significant. Bolt positions were also not found to be significantly associated with fixation failure (p-value >0.05).
Tip-to-apex distance related to occurrence of fixation failure.
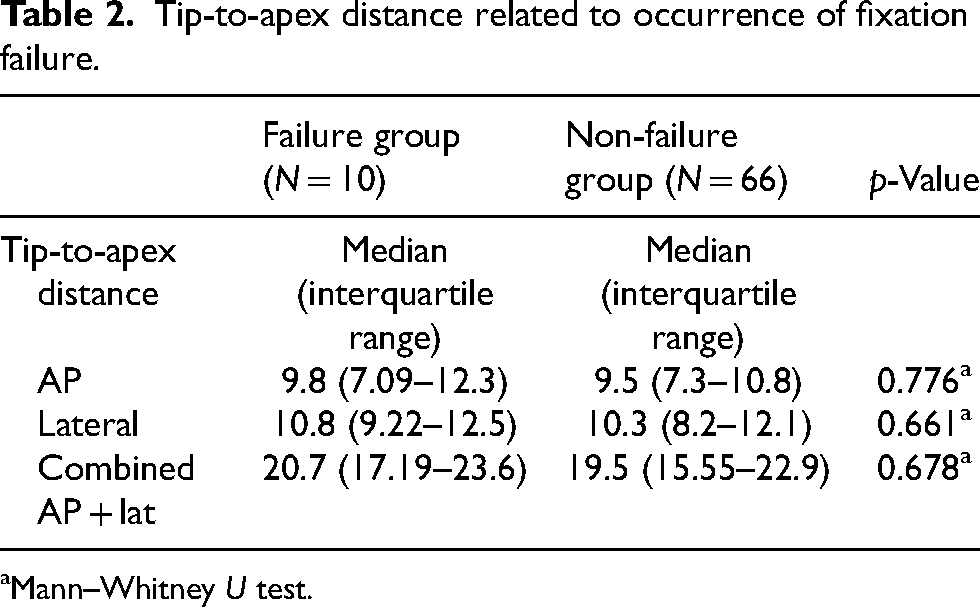
Mann–Whitney U test.
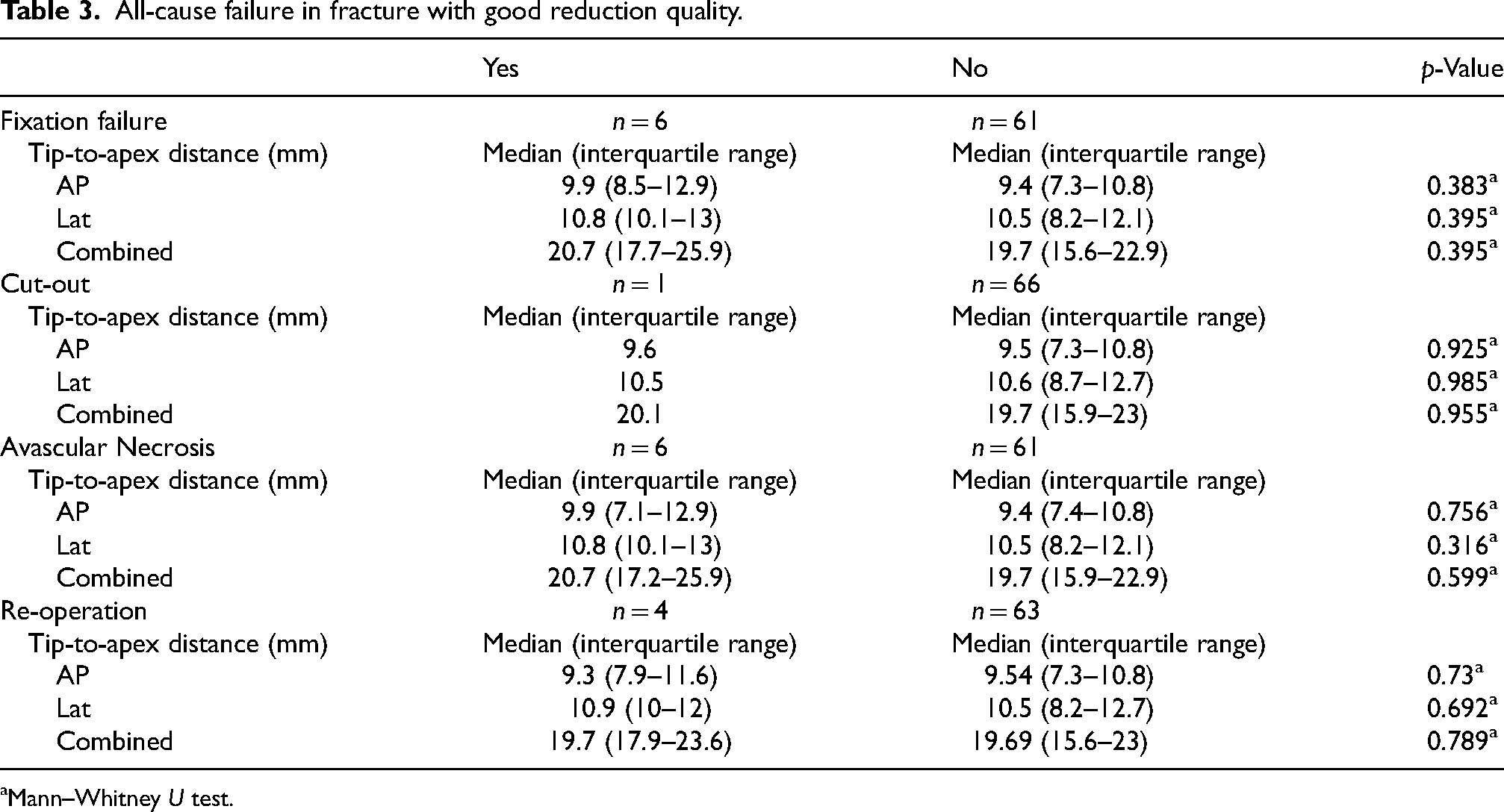
Subgroup analysis among fracture with good reduction quality showed no significant association between TAD and overall fixation failure rate (p = 0.395), cut-out (p = 0.955), avascular necrosis (p = 0.599), or rate of re-operation (p = 0.789) (Table 3).
All-cause failure in fracture with good reduction quality.
Mann–Whitney U test.
Discussion
Our findings suggested that neither the TAD nor the position of the implant had a significant effect on the fixation failure rate. Implant position has been extensively reviewed in sliding hip screws, with recommendations including low in inferior neck position, center-center position, and a TAD <25 mm.5,9 Surgical technique advocated by the AO group 10 and by the FNS manual 11 suggested a center-center position and subchondral placement of the guide pin mainly based on previous findings from studies for sliding hip screws. Our results have, however, indicated that failure could still occur in FNS bolts positioned in center-center positions. Furthermore, despite failure cases showing a slightly larger TAD (20.7 mm vs 19.5 mm), the difference was small and did not reach statistical significance. This is consistent with the previous report by Davidson et al. 12 who found no difference in TAD between revision and no revision group in 102 patients who had received FNS fixation. This may suggest that factors other than implant position may contribute to FNS fixation failure, and over-zealous pursuits in minimizing TAD (with risk of intra-articular implant protrusion) may not be warranted.
Our early experience with FNS implant have shown a mode of failure similar to sliding hip screws, with varus collapse and progressive cut-out in 6 out of 10 cases. Our study is the first to specifically evaluate the position of FNS implant and TAD in correlation with various complications. In this study, we failed to demonstrate any significant effect of implant position on the failure rate. It is possible that the FNS implant behaved differently as sliding hip screws because of the anti-rotational screw that has provided additional stability, making it less susceptible to implant mal-positioning. Another possibility is that with the awareness of the effect of TAD on angular stable implant, operating surgeons had kept TAD within a certain standard so that the minute difference between two groups could not produce significant clinical difference in outcomes.
Strengths of our study include its multicentricity, territory-wide follow-up to allow detection of fixation failures, and mean duration of follow-up (14 months) for a relatively recent implant to detect early mechanical failure. As compared to previous reports in literature, this study offered additional insight through more granular analysis investigating different outcomes besides aggregate re-operation rates. Subgroup analysis focusing on fractures who had received good reduction mitigates the confounding effect of poorly-reduced fractures as mal-reduction is a well-recognized factor for fixation related complications. 7 Our study is limited by its retrospective nature. The relatively small variation in TAD and modest sample size limit statistical power in detecting differences in outcomes. Future studies may focus on exploring other variables and their potential associations with fixation failure, such as bone mineral density, patient comorbidities, and host factors.
In conclusion, TAD and the position of FNS implant were not found to be significantly associated with fixation failure, cut-out, varus collapse, avascular necrosis, and re-operations.
Footnotes
Acknowledgements
Spacey Chau Wa Ho, an illustrator and designer, has helped in graphic illustration of tip-to-apex distance calculation.
Authors’ contributions
HYL contributed to the design of the study and protocol. HYL, CT, and CF contributed to data collection. HYL and JSHW managed the data and performed analysis. HYL wrote the manuscript. CF and JSHW revised the manuscript. All authors reviewed the manuscript and approved the final version to be published.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christian Fang is a shareholder of Lifespans Ltd and is also a speaker for Depuy Synthes. He has received research support from AO Foundation and Agnovos LLC. All other authors declare no conflicts of interest.
Ethical approval
This multicenter retrospective study protocol was approved by our institutional review board, who waived the need for informed consent due to the retrospective nature of the study (Institutional Review Board of the University of Hong Kong / Hospital Authority Hong Kong West Cluster, reference number: UW-22-333). All steps and methods were performed in accordance with the relevant guidelines and regulations.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.