
Abstract
Introduction
Chronic low back pain (LBP) is a serious medical and social problem and one of the common causes of disability and morbidity. Lower back pain is one of the most common complaints in clinical practice; its lifetime prevalence is estimated at 60–90%. 1 Most patients improve by noninvasive conservative treatment, except a few who progress to have chronic LBP, which is debilitating and continues to be the cause of functional disorders.
Facet joints (zygapophyseal joints) are paired structures at the back of each vertebra that form a working motion unit that allows movement between two vertebrae. Facet joint pathology is an important cause of LBP especially in the elderly. 2 Lumbar facet joint syndrome has been defined as a kind of LBP with or without referred pain to the buttock, groin, or proximal thigh deriving from lumbar facet joints. 3 Current studies have illustrated that among cases of LBP, 15% to 52% are caused by lumbar facet joint syndrome. 4
At present, the three main therapeutic methods for lumbar facet joint syndrome are conservative, interventional, and surgical management. Interventional management is increasingly being used in refractory cases. 5
Percutaneous conventional radiofrequency (CRF) denervation of the medial branches of the dorsal rami has been used for facet joint pain management. This is a neurodestructive procedure in which a constant high-frequency and high-temperature electrical current are applied to the target tissue. 6
Intra-articular block with steroids and local anesthetics for lumbar facet joint pain has also been used with varied efficacy. Steroids have anti-inflammatory and immunosuppressive effects largely due to the inhibition of phospholipase A2. However, the long-term relief of LBP after facet intra-articular steroid injection can range from 18% to 63%. 7
Steroid injections are commonly used in various chronic musculoskeletal disorders. Due to the risk of complications and need for repeated injections, PRP was studied and found superior to steroid injections in recalcitrant lateral epicondylitis and knee osteoarthritis.8,9
Lumbar intra-articular treatment with platelet-rich plasma (PRP)—an autologous blood derivative, is a new method in the treatment of LBP. It is suggested that healing occurs after PRP stimulates the recruitment, proliferation, and differentiation of cells involved in regeneration via growth factors and proteins released from the platelets.10,11
Initial reports support its long-term efficacy and safety in pain relief. With these biological properties, PRP seems to be a suitable novel option for the treatment of lumbar facet joint syndrome.
Therefore, it appears meaningful to apply PRP to assess its effectiveness and safety for the treatment of lumbar facet joint syndrome. In this prospective study, we aimed to compare and evaluate the effectiveness and safety of intra-articular PRP and steroid injection along with denervation of lumbar facet joint with radiofrequency ablation (RFA) in the treatment of chronic LBP.
Methods
This prospective clinical study was designed to randomly include patients of either sex presenting with LBP secondary to facet joint arthropathy in origin as evidenced by clinical and diagnostic medial bundle branch block in three study groups. Study protocol was approved by the institutional ethical committee No. IMS/EC/468 and written informed consent was obtained from all subjects.
The study was conducted in the department of anesthesiology and orthopedics of a university teaching hospital from June 2017 to July 2019. A total of 60 consecutive patients were assessed; 49 were included with 4 dropouts. Finally, 45 cases were analyzed. Consecutive patients fulfilling the inclusion criteria were included in the study. The study patients were randomly allocated into three groups: Group S: Steroid (Triamcinolone) plus RFA; Group P: PRP plus RFA; and Group R: RFA plus normal saline as control group.
Those with spondylolisthesis, internal disc disruption (IDD), and spinal canal stenosis on MRI, previous spinal surgery at the level to be treated, bleeding disorders, pregnancy, systemic infections, or local infections in the field of intervention or any known history of allergy to medications to be used were excluded.
Clinical and radiological evaluation: All patients included in the study were evaluated clinically by taking a detailed history and physical examination. The patient's age, sex, duration of symptoms, and facet joint level was noted. Plain radiographs were taken in antero-posterior and lateral views. MRI spine was assessed.
Interventional procedure: The procedure was explained and written informed consent was taken. Patients were then randomly allocated to one of the study groups. Before the final intervention, diagnostic medial branch block was given to confirm the diagnosis of facet joint arthropathy.
Diagnostic medial branch block: Patients were positioned prone with a convex support under the abdomen to open up the lumbar spine. Vital parameters (pulse rate, ECG, noninvasive blood pressure, and oxygen saturation) were monitored. Injection Ceftriaxone 1 g intravenous was given 30 min before the procedure after the test dose. Image intensifier (IITV) was used for guidance. Under strict aseptic precautions and local anesthesia, a 22 gauge, 90 mm spinal needle was gently inserted targeting the posterior surface of transverse process at its junction with superior articular process and superolateral margin of the pedicle (1 or 2 o’clock position) when the oblique ipsilateral IITV view shows “Scotty dog” appearance of vertebral segment. The position of the needle was confirmed by injecting 0.1–0.2 ml of nonionic contrast medium—Iohexol 15 g/50 ml. With the needle in place, 0.5 ml of 2% lidocaine was injected. Only patients who had >50% pain relief following the diagnostic block were considered to have lumbar facet joint pain and were included in the study.
Continuous radiofrequency (CRF) ablation procedure: The procedure was performed under strict aseptic precautions and local anesthesia without sedation. Prone position was similar to the diagnostic block. The IITV was angled cephalad and rotated until it was at a tangent to the site of medial branch of dorsal rami and the lumbar facet joint space. RFA was added for maximizing clinical benefit along with injections.
For CRF procedures in all groups, after local anesthesia (with 2% lidocaine), a 22-gauge, 10-cm length, 5-mm active tip radiofrequency (RF) needle was placed adjacent to the medial branch. The electrode tips were placed parallel to the target nerves at the angle between the superior articular process and the transverse process. After positioning of the needle, sensory stimulation (frequency, 50 Hz; pulse width, 1 millisecond, and voltage up to 0.5 V) and motor stimulation (frequency, 2 Hz; pulse width, 1 millisecond, and voltage up to 0.5 V) were performed using an RF lesion generator (Baylis RFP-100A). The safe distance of RFA probe from the exiting spinal nerve roots was assessed by a tingling sensation on sensory stimulation and contractions of multifidus muscle on motor stimulation. Subsequently, 1 ml of 2% lidocaine was injected through the RF needle to obtain profound local anesthesia. Duration of CRF for each nerve was 80°C for 90 s. The patient was observed for 4 h after the CRF procedure before discharge to look for significant complications like neurological deficit, pain, or bleeding.
Image-guided lumbar facet joint intra-articular injection: In the intra-articular group, a 22-gauge spinal needle was inserted under fluoroscopy. The intra-articular position was confirmed by injecting 0.2 ml of contrast (Iohexol) into the facet joint space. For the steroid group, we injected 10 mg (0.25 ml) Triamcinolone acetate mixed with 0.25 ml of 0.5% Bupivacaine using a 22-gauge, 10 cm spinal needle and for PRP group, 0.5 ml PRP was injected in at least two spaces.
Autologous PRP preparation: The standard two-step centrifugation method was used. In the immediate pre-therapeutic period, 5 to 10 ml of venous blood sample (the exact amount was based on the number of treated levels) was collected in sodium citrate anticoagulant tubes under sterile conditions. Then the sample was centrifuged first at 200×g for 10 min at room temperature. Two layers were obtained after this centrifugation. The erythrocytes remained at the bottom of the tube, whereas platelets and leukocytes remained at the top. The obtained plasma was centrifuged again at 400×g for 10 min to remove part of the platelet-poor plasma. Approximately 1 to 2 ml of buffy coat autologous PRP was prepared for lumbar facet joint injection. The concentration of platelets in native peripheral blood before the treatment and in PRP after standard centrifugations was tested to ensure that the platelet concentration in PRP was almost four to five times greater than that in native peripheral blood (100 to 300 × 109/ml).
Outcome and follow-up: In each group, patients were given pain medication—Paracetamol and Tramadol orally, if needed. Change in pain intensity was recorded using a VAS ranging from 0 to 10 (0: “no pain” to 10: “the worse pain”); physical functioning was evaluated using Oswestry Disability Index (ODI); and Patient Satisfaction Score (PSS) and use of NSAIDs was also recorded in all cases before and after intervention at day 1, 1 month, 3 months, and 6 months after treatment. Complications if any were noted.
Statistical analysis: The data were analyzed using statistical software SPSS v20 (IBM Corporation) and p < 0.05 was considered significant. Quantitative variables were expressed as mean and range and qualitative variables as percentages. Comparison between groups was made using Fisher's exact test. Student's t-test was used to compare the pre and postintervention scores.
Results
The study was conducted at the Institute of Medical Sciences of a university teaching hospital in the department of anesthesiology and orthopedics from June 2017 to July 2019. A total of 60 cases of back pain were assessed. Based on the inclusion and exclusion criteria, 49 patients were finally enrolled. There were four cases that dropped out due to increased pain postinjection and difficulty in traveling from far places. Forty-five cases were analyzed in this study with equal distribution in each study group—Group S: Steroid (Triamcinolone) plus RFA; Group P: PRP plus RFA and Group R: RFA plus normal saline as control group.
Mean age was 45.7 ± 13.6 years which was similar in all study groups (p = 0.9). Sixty percent were females which was similar in all groups (p = 0.9). Table 1 shows the patient profiles and other variables of each study group after randomization.
Comparison of patient profiles and other variables between three groups after randomization.
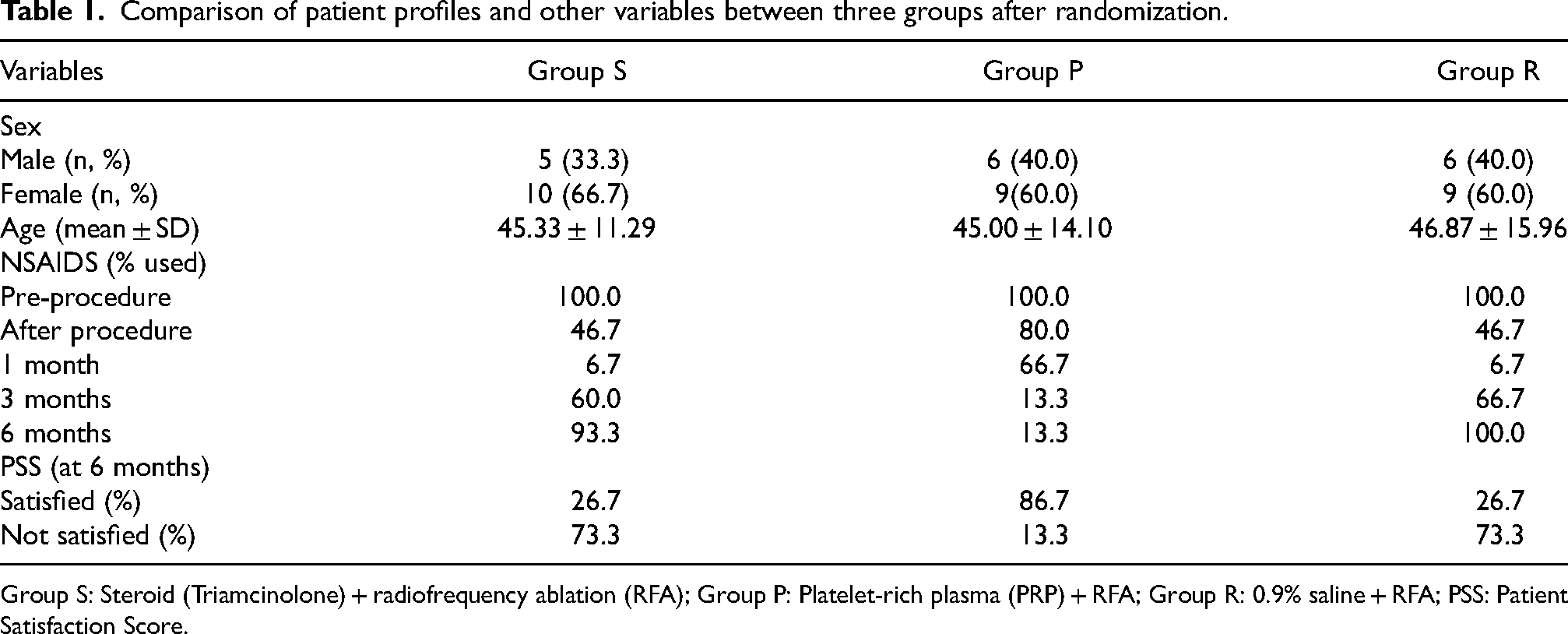
Group S: Steroid (Triamcinolone) + radiofrequency ablation (RFA); Group P: Platelet-rich plasma (PRP) + RFA; Group R: 0.9% saline + RFA; PSS: Patient Satisfaction Score.
Comparison of mean VAS score between the study groups at different time intervals is shown in Table 2. The baseline VAS was comparable. In Group S, there was a significant decrease in VAS on day 1 when compared with Group P. At 3 and 6 months, there was more decrease in VAS in Group P when compared to Group S (p < 0.001). There was an insignificant difference in VAS between Group S and Group R (control group) at all time intervals up to 6 months. There was a significant difference in VAS between Group P and Group R at 3 and 6 months (p < 0.001).
Comparison of mean visual analogue score (VAS) between three groups at different time intervals.
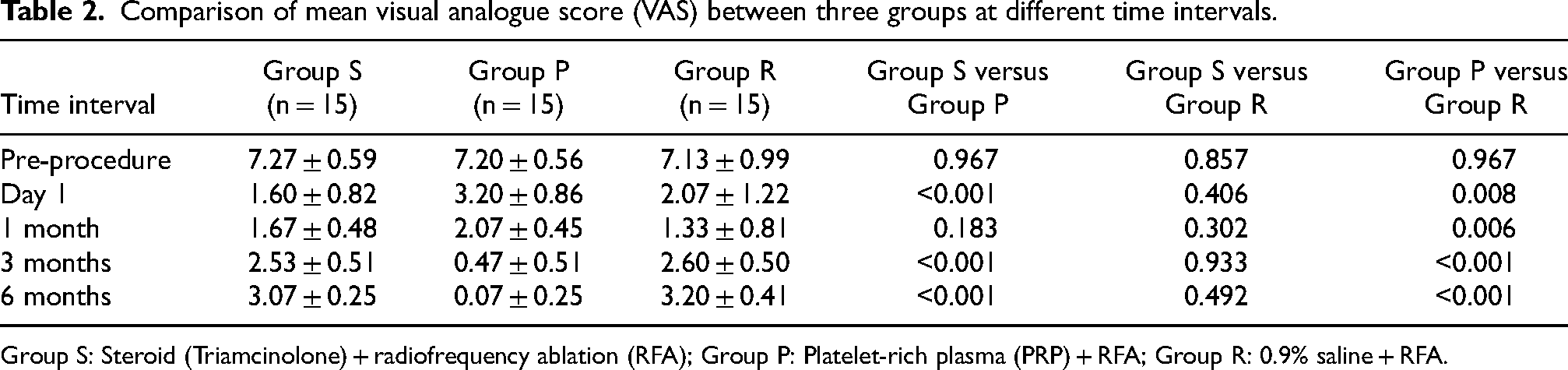
Group S: Steroid (Triamcinolone) + radiofrequency ablation (RFA); Group P: Platelet-rich plasma (PRP) + RFA; Group R: 0.9% saline + RFA.
Comparison of mean ODI between three groups at different time intervals is shown in Table 3. Baseline ODI was similar in all groups. There was a significant improvement in ODI score in all study groups (p < 0.01). On day 1 and at 1 month, Group S had better improvement than Group P but at 3 and 6 months, Group P had more decrease in ODI score (p < 0.001).
Comparison of mean Oswestry Disability Index (ODI) score between three groups at different time intervals.
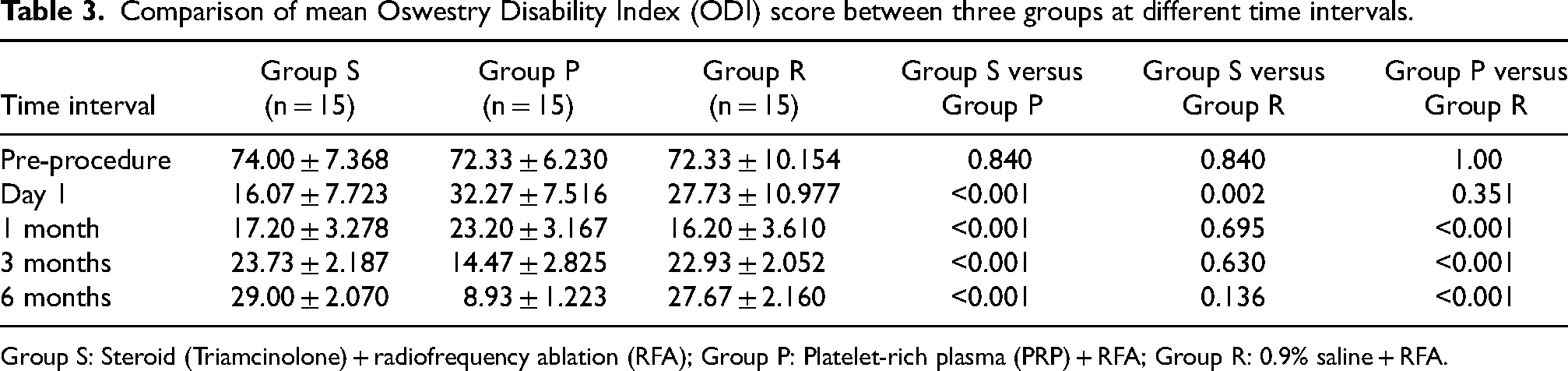
Group S: Steroid (Triamcinolone) + radiofrequency ablation (RFA); Group P: Platelet-rich plasma (PRP) + RFA; Group R: 0.9% saline + RFA.
Considering NSAID use, it reduced significantly in group S at day 1 and 1 month when compared to group P. However at 3 and 6 months, Group P had a more significant reduction in NSAID usage (vs. Group S) (Figure 1). Patient satisfaction was significantly better in Group P when compared to Group S and Group R at 6 months. Group S and Group R showed an insignificant difference in patient satisfaction at 6 months (Figure 2).
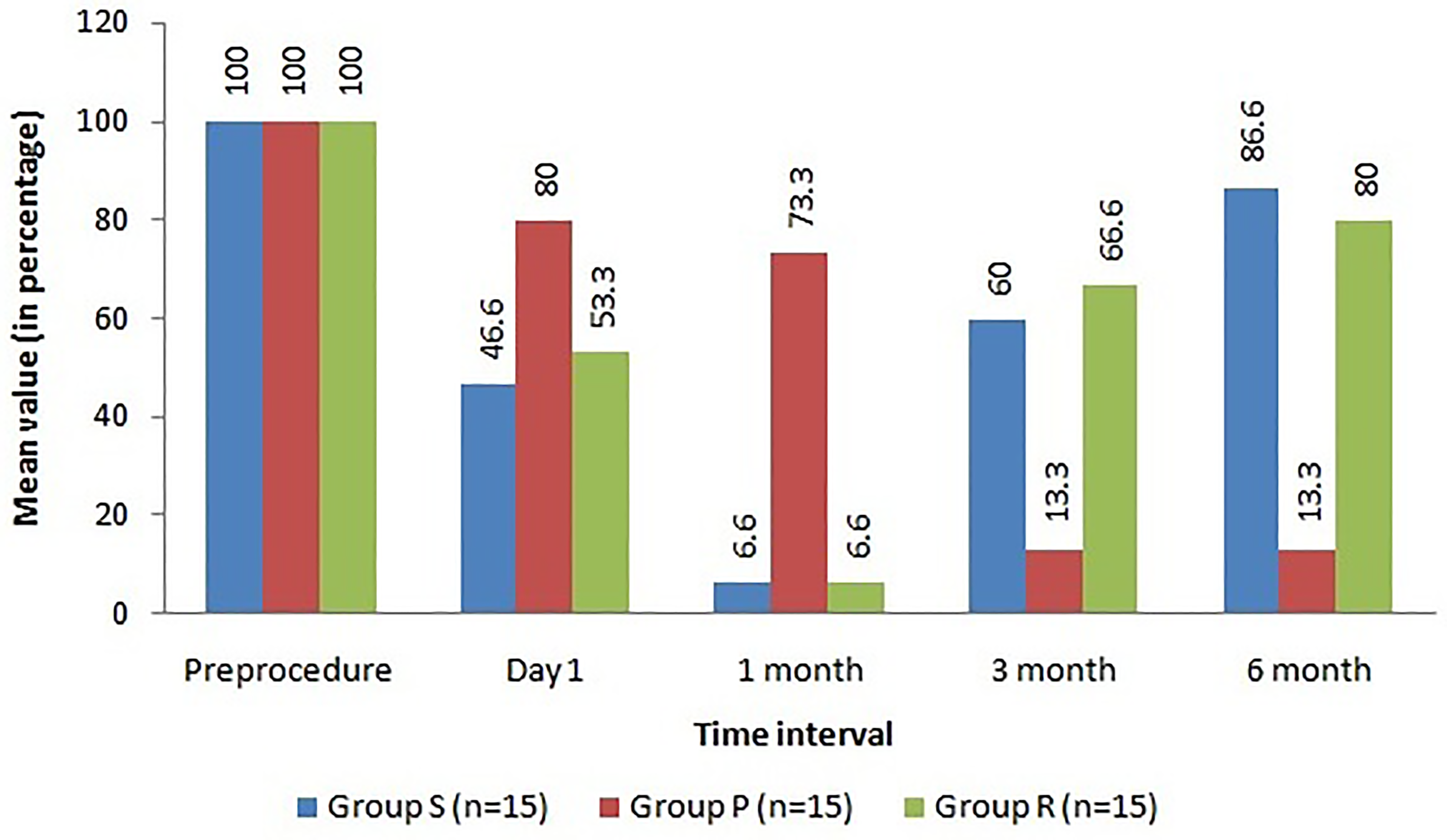
Comparison of use of NSAIDs between three groups at different time intervals (percentage of patients using NSAID).
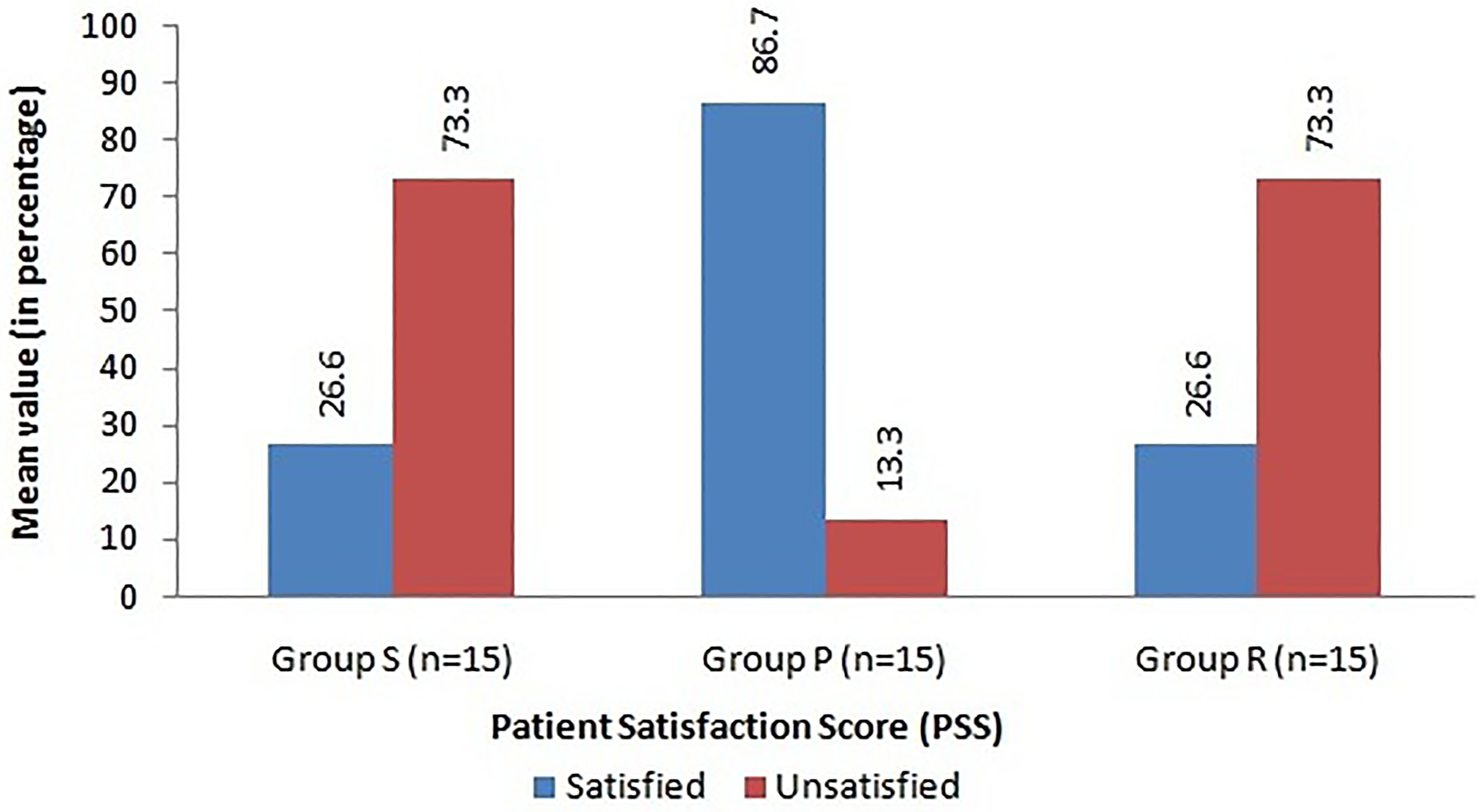
Comparison of Patient Satisfaction Score (PSS) between three groups at 6 months.
Discussion
Lumbar facet joint syndrome can be defined as LBP originating from the lumbar facet joints, which has a strong impact on daily activities. At present, different studies have described multiple therapeutic techniques to manage lumbar facet joint syndrome, and intra-articular injection is one of the most important methods.
Recently, PRP therapy has gained a lot of attention as a safe, nonsurgical, and biological treatment for osteoarthritis and musculoskeletal repair. 12 Since PRP is prepared from autologous blood, theoretically there are minimal risks for toxicity and side effects. Due to these features, PRP becomes a very appropriate material for intra-articular injection. However, to the best of our knowledge, there are only a few studies using autologous PRP to treat lumbar facet joint syndrome.
There is no conclusive evidence about the precise mechanism of autologous PRP. However, it can provide antinociceptive and anti-inflammatory effects by suppressing inflammatory mediator concentration and gene expression in synoviocytes and chondrocytes, especially in osteoarthritis of peripheral synovial joints—knee and hip.9,13 As the only synovial joints in the spine, it was contemplated that inflammatory arthritic changes have a significant role in lumbar facet joint pathology similar to other peripheral synovial joints. 14
Our results of PRP injection with RFA showed that the mean VAS scores at rest were 3.2, 2.1, 0.5 and 0.1 at day 1, 1 month, 3 months, and 6 months after treatment, respectively, and mean ODI scores at rest were 32.3, 23.2, 14.5 and 8.9 at day 1, 1 month, 3 months, and 6 months, respectively. These findings show that PRP is better for thr treatment of facet joint syndrome in the long term.
Similar observations were made by earlier workers. In a study by Wu et al., 19 patients were included to assess the feasibility and safety of PRP in treatment of lumbar facet joint syndrome for 3 months. The outcomes were assessed as “good” or “excellent” for 47% patients immediately after the treatment which increased to 79% at 3 months. No significant complications were noted. The investigators concluded that lumbar facet joint injection with autologous PRP is effective and safe in the short-term period of 3 months. 15
Therefore, we tried to use autologous PRP as one of the appropriate novel treatment options for lumbar facet joint syndrome and compare the effectiveness and safety of intra-articular autologous PRP injection with intra-articular corticosteroid injection in the treatment of lumbar facet joint syndrome with RFA as control group.
The corticosteroid with or without local anesthetic is one of the most common drugs for interventional lumbar facet joint injection treatment and seems to be the gold standard for comparison of newer injection therapies. Most experts believe that the rationale for lumbar facet joint corticosteroid injection is to treat the inflammation due to osteoarthritis, whereas local anesthetic is only for the apparent temporary alleviation of symptoms. 16 The results of intra-articular LA/corticosteroid injection to treat lumbar facet joint syndrome are variable with slight to significant pain relief and functional improvement being reported at 24 weeks in different studies.17,18
In the present study, our results of corticosteroid injection with RFA showed that the mean VAS scores at rest were 1.6, 1.7, 2.5 and 3.1 at day 1, 1 month, 3 months and 6 months after treatment, respectively, and mean ODI scores at rest were 16.1, 17.2, 23.7 and 29.0 at day 1, 1 month, 3 months and 6 months after treatment, respectively. There was an overall improvement over 6-month period. Initial 1 month pain relief was more encouraging than the subsequent follow-up period when compared to PRP group.
These results were in agreement with another study where 87% of patients with facet joint abnormalities had an improvement in the pain score at 1 month after corticosteroid and local anesthetic injections, but only 53% patients had the same results after 6 months. Interestingly, the lowest VAS score (4.7) occurred at 1 and 4 weeks after treatment, whereas the pain VAS score was 5.3 at 24 weeks.19,20
In our comparative study, demographic and clinical characteristics of patients with autologous PRP or corticosteroid injection and RFA treatment were similar at baseline.
Compared with baseline, both PRP and corticosteroid showed significant pain relief at rest and during flexion. In the short-term period (1 month), corticosteroid had a better outcome for pain relief than PRP. However, in the longer term period (6 months), for PRP, sustained reduction of pain VAS scores at rest and during flexion occurred after injection. For the steroid group, pain reduction was less marked at 6 months but remained statistically significant compared with baseline. These changes were consistent with lumbar functional improvements, which were assessed by the ODI and PSS. Other parameters like use of posttreatment analgesics (NSAIDS) were in concordance with these findings.
All of these outcomes demonstrated that autologous PRP was a superior treatment option for longer duration efficacy in the treatment of lumbar facet joint syndrome, compared with conventional corticosteroid and RFA.
In musculoskeletal disorders like hip and knee osteoarthritis, many studies have shown good pain relief and functional improvement by intra-articular PRP injection.21,22 Clinical outcomes of knee osteoarthritis were found to be significantly better after PRP injection versus hyaluronic acid injection at 3 to 12 months posttreatment in a systematic review. 23 Similarly at long-term follow-up PRP was reported to be more effective for lateral epicondylitis than corticosteroids with comparable results in short term. 24
Due to the lack of pathognomonic predictors that allows one to definitively differentiate patients with LBP of lumbar facet joint origin from other pain generators, the diagnosis of lumbar facet joint syndrome relies on clinical evaluation, radiologic findings, and invasive diagnostic blocks when necessary.
The combination of clinical factors and radiologic findings may be helpful for the initial diagnosis of lumbar facet joint syndrome, but they are less reliable.25,26 Even though the false-positive rate of a single diagnostic block could be as high as 38%, it is still generally accepted that diagnostic blocks (intra-articular or medial branch blocks) are the most reliable methods for diagnosing lumbar facet joints as LBP generators.27–29 For these reasons, we used the comprehensive criteria of clinical factors and radiologic findings for the initial diagnosis of lumbar facet joint syndrome, and applied diagnostic blocks for the confirmatory diagnosis.
We observed that after about 0.5 ml of the drug was injected into each lumbar facet joint, the injection pressure increased considerably. To avoid rupture of the facet joint capsule and efflux of medication, only 0.5 ml of various drugs was injected. This approach is in agreement with other studies. 30
Xuan et al. in a meta-analysis studied the efficacy of PRP in LBP involving 131 cases in 3 RCTs. They concluded that when compared with control intervention for LBP, PRP injection improved pain relief and patient satisfaction without any increase in adverse events. 31
The
In
Footnotes
Author’s contribution
Chandan Singh—Data curation (equal), formal analysis (equal), and investigation (lead).
Sanjay Yadav—Conceptualization (equal), writing—original draft (lead), and writing—review and editing (equal).
Sandeep Loha—Formal analysis (equal), investigation (equal), and writing—review and editing (equal).
Shashi Prakash—Data curation (equal), supervision (equal), and project administration (equal).
Anil Kumar Paswan—Conceptualization (lead), writing—review and editing (equal), and supervision (lead).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article