
Abstract
Introduction
In sub-Saharan Africa, the elderly represent 4 to 8% of the population.1,2 Due to the progressive aging of the population, the proportion of the elderly in general and that of the very old in particular continues to increase. 2 The result being the emergence of health problems related to osteoporosis. 3 Chiefly, low-energy hip fractures which, due to bone demineralization, occur more frequently.4,5 They represent the leading cause of admission to trauma wards worldwide, with an estimated 10 million cases in 2050. 6 Their incidence increases exponentially with age, peaking between 90 and 95 years.5,7 This is a real public health problem in the world because they increase morbidity and mortality and the cost of their care is still quite high in low-income countries.8,9 In the elderly, they pose the problem of the sudden deterioration of physical autonomy which was already reduced with advanced age.10,11 Psychic autonomy is also impaired and the prevalence of mental depression caused by these fractures is estimated at 23%.12,13 Prosthetic replacement surgery or internal fixation remains their main means of treatment. 14 Compared to functional treatment, the indications of which are increasingly limited, surgical treatment reduces mortality by approximately 4 times more. 15 At over 90 years of age, the impact of surgery for fractures of the proximal femur on restoring physical autonomy prior to the trauma is little known in the literature. Also this study proposes, on the one hand, to evaluate the result of the surgery on the physical autonomy of the elderly after a fracture of the proximal femur. On the other hand, to determine the factors associated with the degradation of this autonomy after surgical treatment
Matrials and methods
Study design
A prospective study was carried out on 66 patients aged at least 90 years, hospitalized and treated for a fracture of the proximal femur between 2008 and 2017 in the department of Orthopedics and Trauma Surgery of the General Hospital Idrissa Pouye of Dakar. We recruited from the electronic hospitalization register. The files obtained from the archives were searched. We excluded patients with pertrochanteric or femoral neck nonunion. The institutional review board approved this study.
Data collected
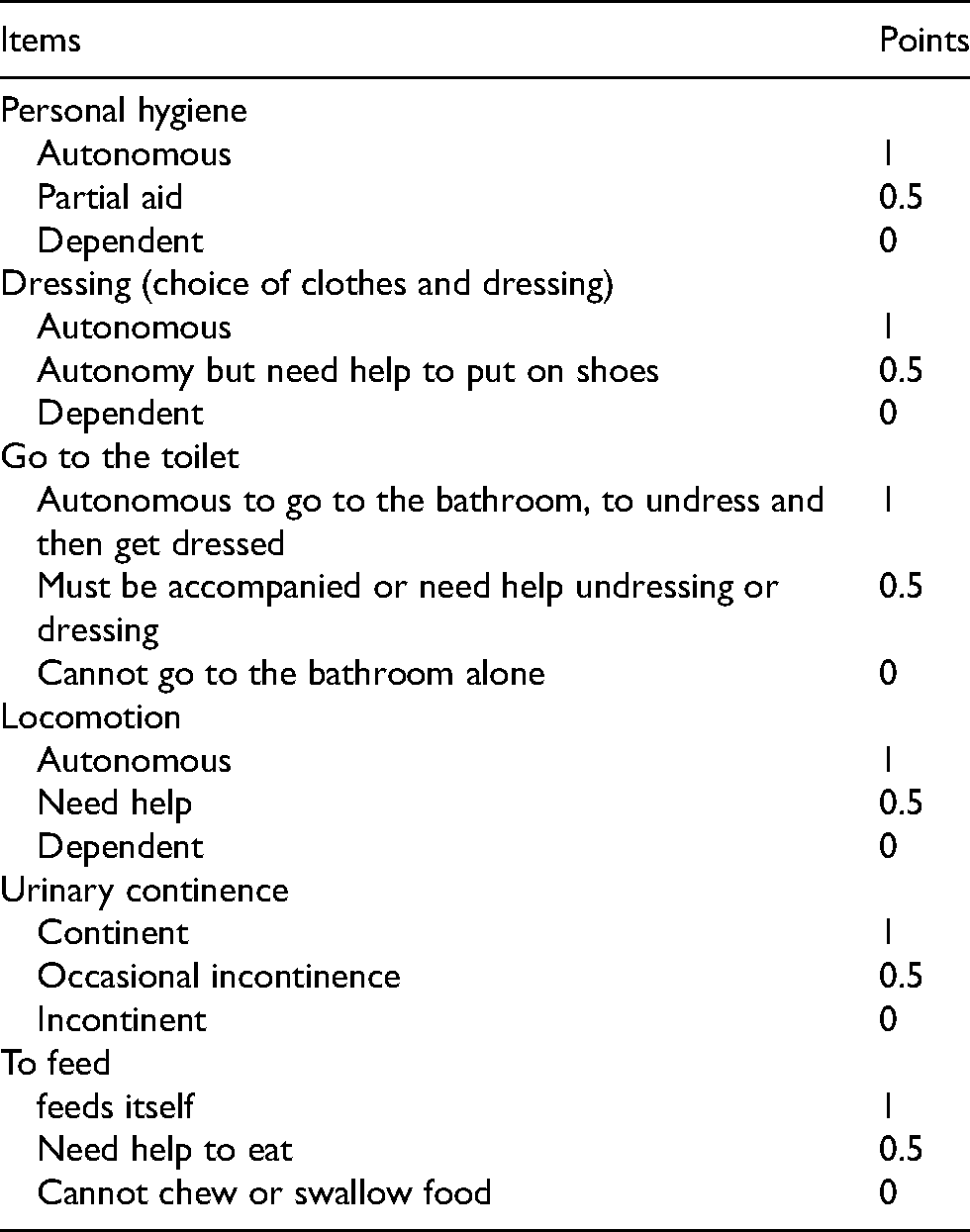
Data collected included age, sex, previous co-morbidities, anesthetic risk, systolic ejection function, hemoglobin level, history of rhythm or conduction disturbances, time to hospital treatment., the initial traditional management, the length of hospitalization, the time to verticalization, the definitive treatment used, complications of recumbency. Autonomy assessment using the Katz scale. 16 The autonomy evaluations by the Katz scale (Table 1) were made at different periods: 15 days before the trauma, between the trauma and the surgery, on the first, third, sixth and twelveth months after surgery. Three levels of physical autonomy were retained: dependent patient for a score of ≤ 3, semi-autonomous patient between 4 and 5, autonomous patient for a score of 6.
Items and score of the Katz scale on the assessment of physical autonomy on the activity of daily living.
Patients caracteristics
The median age of the patients was 91 years, with extremes of 90 and 107 years. 36 women and 30 men. The predominant cardiovascular and metabolic comorbidities found in the patients were high blood pressure in 21.2%, followed by diabetes in 12.1%, chronic kidney disease in 10.6% and heart failure in 4.6. %. The hemoglobin level on admission was on average 10.8 (± 1.8) g / dl, 69.6% of patients had anemia of which 13.6% moderate and 1.5% severe. The mean systolic ejection function was 65.9% with an alteration in 18.2% of patients. On the electrocardiographic recordings, one noted respectively a rhythm disturbance in 30.4% of the patients and a conduction disturbance in 53.6%. Femoral neck fractures accounted for 53% of cases, compared to 47% of pertrochanteric fractures. The time to hospital treatment was on average 5.8 (± 9.7) days with a median time of one day. In 26.7% of cases, there was prehospital care in the bonesetters, increasing the time to hospital care. The surgery was performed under general anesthesia in 20 patients and under locoregional in 46. Pertrochanteric fractures were treated by a Dynamic Hip Screw (DHS) in 68.2% and by Gamma nail in 18.2%. 35 patients with femoral neck fractures underwent prosthetic hip replacement. The prostheses used were those of Moore in 30 patients and bipolar in 5. Surgery in patients with pertrochanteric fracture was performed on average 11.9 ± 9.8 days after fracture, while that for femoral neck fractures averaged 19.1 ± 15.1 days after fracture trauma. Morbid complications related to the decubitus have arisen between the trauma and the verticalization of the patients. They were mainly represented by muscular atrophy at 49.2%, bedsores (heels and buttocks) at 43.8%, constipation at 36.9%, urinary tract infections at 21.9% and decompensation of pre-existing defects in 8% of cases.
Statistics
Data were entered using Epi InfoTM software version 7.1.5.2 and analysis was performed using R Studio statistical software Version 1.0.143 (R Development Core Team, Vienna, Austria). The general and clinical characteristics of the patients were described using standard descriptive statistics. Medians and quartiles or means with standard deviation were calculated for the quantitative variables. The counts and percentages were calculated for the qualitative variables. Student's t-test was performed for the comparison of quantitative variables. The significance level was set at P < 0.05. We investigated the factors associated with patient autonomy one month postoperatively using bivariate logistic regression models. A multivariate logistic regression model was then fitted with the selected explanatory variables using a top-down walkthrough. Raw and adjusted odds ratios (OR) and their confidence intervals (CI) were calculated. The precision and significance of the associations were established using the Wald test.
Results
Impact of surgery on restoring the level of autonomy
Before the trauma, 60% of patients had complete autonomy compared to 40% semi-autonomous according to the Katz scale. 16 of the 66 patients died within a year of the injury, a mortality rate of 24%. This mortality was higher in the twelveth postoperative month, by around 20%. Between the trauma and the start of verticalization, all of the patients became completely dependent. After that, in the patient follow-up, the previous level of autonomy was found in 9.1% at 1 month, 17.5% at 3 months, 23.5% at 6 months and 22% at 1 year (Figure 1). The level of autonomy between the different evaluation periods was statistically significant between each evaluation period.
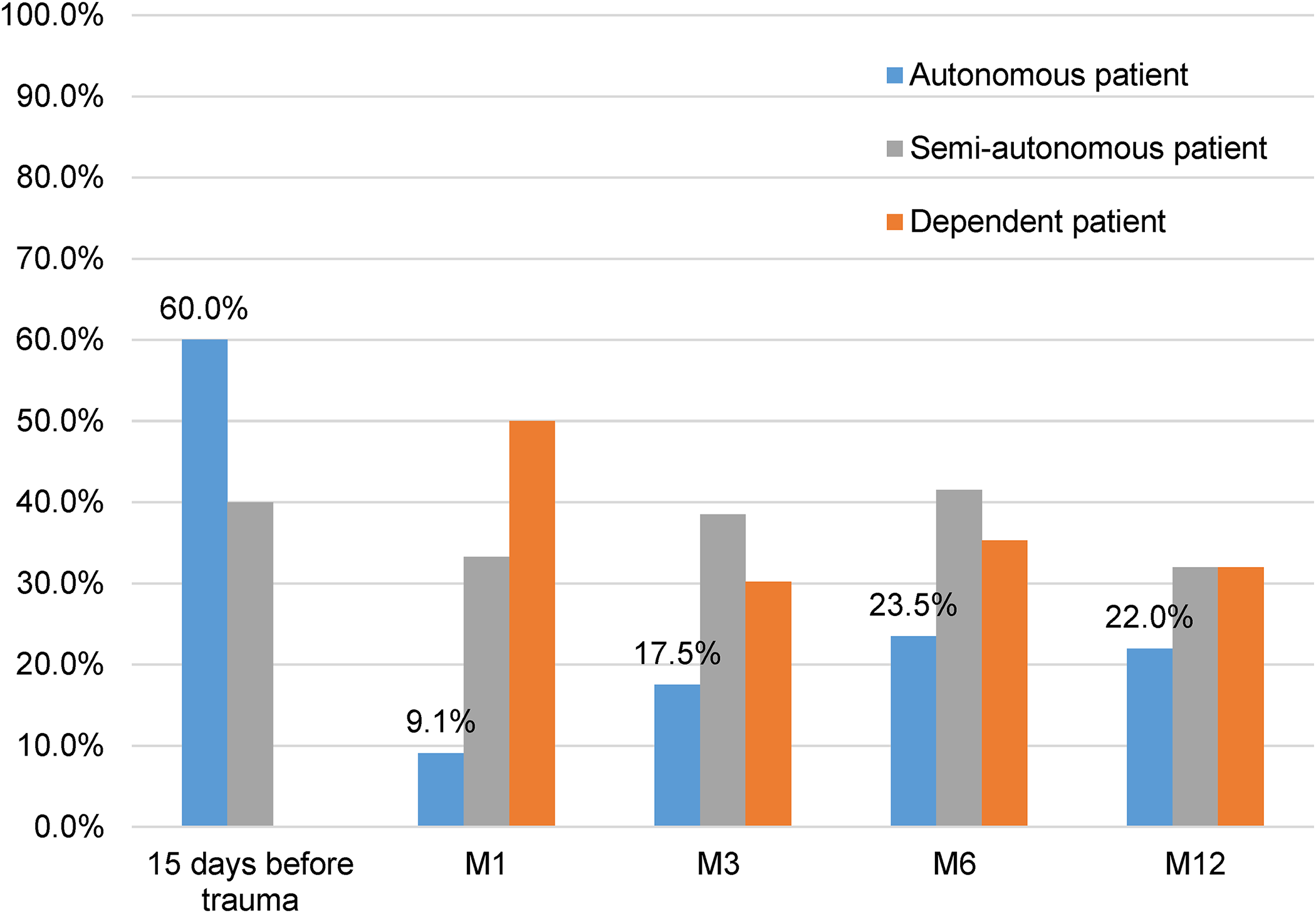
Variation of the level of autonomy before and after surgery.
Factors associated with impaired physical autonomy
In univariate analysis (Table 2), the risk of deterioration of autonomy in patients at 1 month postoperatively was significantly higher in patients admitted late (OR : 6.2; CI 95% : 1.5–42.7; P = 0.02). It was also higher in patients with a verticalization time greater than 15 days compared to those with a shorter time (OR : 3.8; CI 95%: 1.3–11.6; P = 0.02). Patients who presented at least one complication of recumbency also had a significantly higher risk of deterioration of autonomy at 1 month postoperatively compared to those who presented no complications (OR: 4.8; CI 95%: 1.7–14.9; P = 0.004). The comparison of the autonomy between hip fixation and hip prosthetic replacement did not show a significant difference in the first postoperative month.
Factors associated with impaired physical autonomy 1 month postoperatively.
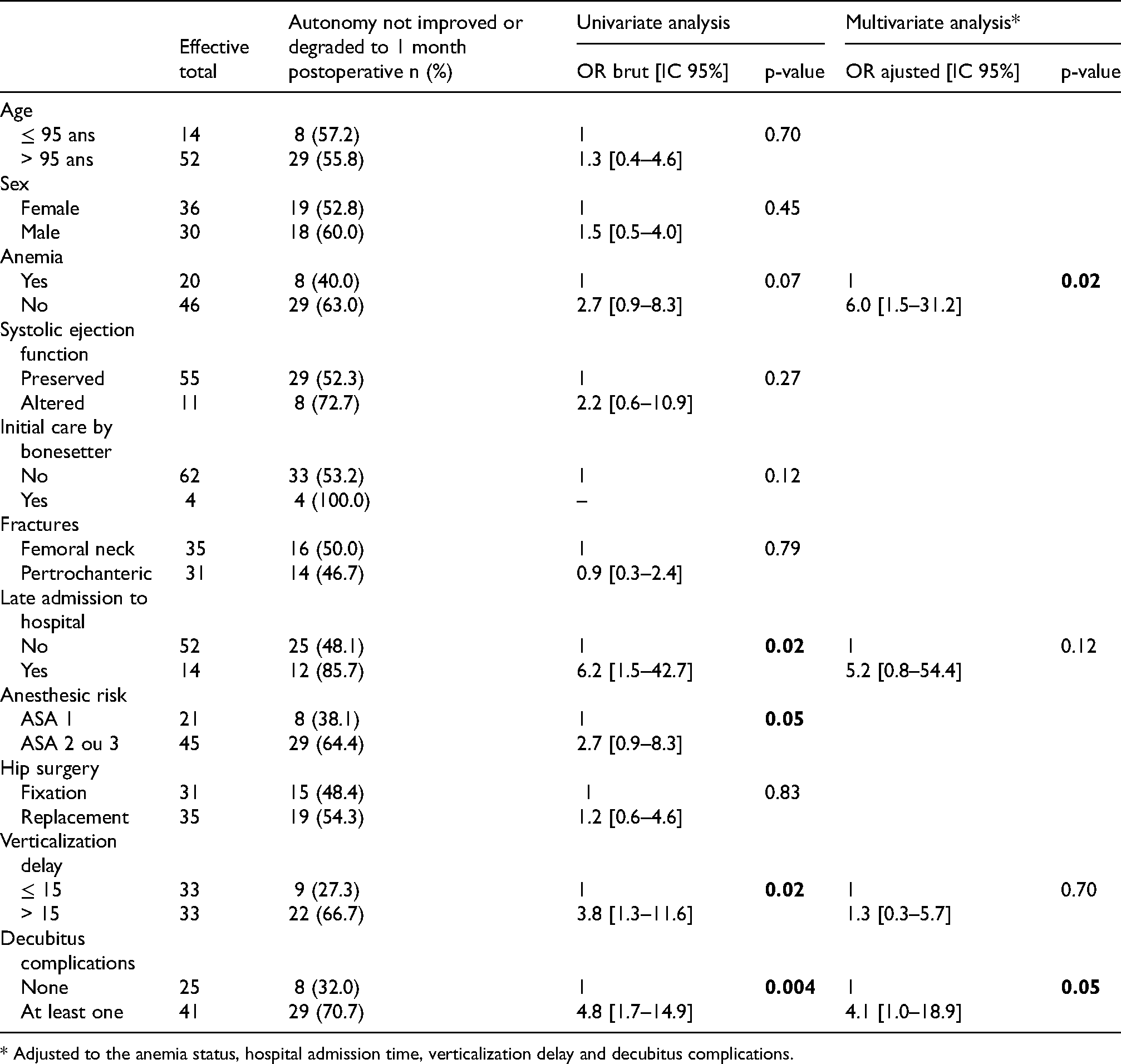
* Adjusted to the anemia status, hospital admission time, verticalization delay and decubitus complications.
A multivariate analysis (Table 2) was carried out taking into account late admission or not, the delay in standing up, the occurrence or not of a complication of recumbency. After this multivariate analysis, the presence of anemia (OR: 6.0; CI 95%: 1.5–31.2; P = 0.02) and an ASA score ≥ 2 (OR: 2.7; CI 95%: 0.9–8.3; P = 0.05) became significantly associated with the deterioration of the level of autonomy of patients at 1 month postoperatively
In this multivariate analysis, late admission to hospital and the delay in standing up were no longer significantly associated with the deterioration in the level of patient autonomy one month after surgery.
Discussion
The natural history of fracture of the proximal femur in the elderly is almost always associated with a loss of physical autonomy in the activities of daily living. 17 Restoring physical autonomy before the trauma is a challenge for orthopedic surgeons and physiotherapists to avoid all the complications of lying down and promote a return to daily activities. 18 In this study, surgical treatment restored a previous level of autonomy of 17.5% at 3 months, 23.5% at 6th month and 22% at 1 year. These results are lower than the level found by some authors. Candel-Parra et al. 19 found a result of 33.6% at 6 months. Corcoles-Jimenez et al. 20 regained a previous level of physical autonomy of 22.3% at 3 months, 33.5% at 6 months and 47.9% at 1 year. Petros et al. 21 found, for their part, found a restoration of previous autonomy in 44.4% of cases at 1 year. This difference can be explained by the fact that the patients in these three studies were younger than those in our series. In these studies, the degree of autonomy was assessed using the Barthel index, 22 and in ours it was Katz's index that was used. Despite the fact that these two tools for measuring the degree of physical autonomy share some items in common, the scoring of their items may result in some differences in the value found. 23
Several other factors may explain this low rate of restoration of prior autonomy. Patients in similar studies had an average age lower than ours; 80.46 ± 6.91 years in the series of Corcoles-Jimenez et al. 20 et 80.17 ± 6.95 years in that of Candel-Parra et al.. 19 In that of Petros et al., 21 the patients had an average age of 84 ± 7.2 years. In our study, it was 91.0 years, with extremes of 90 and 107 years. Similar studies on an age strictly greater than or equal to 90 years were almost non-existent.
The delay of surgery after the hip fracture was also quite low at 5 ± 2.9 days in the series by Corcoles-Jimenez et al., 20 compared with 12 to 19 days in our series. This delay is linked to the late admission of patients and the lack of health insurance which did not allow them to operate quickly. Using Parker's score, 24 Gomez et al. 11 showed that physical autonomy prior to the fracture of the proximal femur was almost restored at 1 year after surgery performed within 24 h. Patients in the above studies also had a low proportion of comorbidities. 17.1% of patients in the series by Corcoles-Jimenez et al. 20 against 70.7% in our. Added to this is the fact that in sub-Saharan Africa, the elderly almost systematically live with their families. They are permanently assisted by a third person in the daily tasks. Which ends up making them quite dependent even outside the context of a fracture of the proximal femur.
Late admission to hospital was found to be associated with deterioration in autonomy after surgery. The delay in consultation, the coverage by the bonesetters, the cost of the coverage and the lack of health insurance largely explain this delay. This already reduced physical autonomy preoperatively. According to Zuckerman et al.,25,26 preoperative autonomy influences the level of postoperative restoration of a fracture of the proximal femur. The weaker it is preoperatively, the weaker the postoperative restoration degree will be. In our study, an anesthetic risk greater than or equal to 2 according to the American Society of Anesthesiologist classification was also a factor of non-improvement in autonomy at one month postoperatively. This result is also found by Schemitsch et al. 27 Contrarily, Michel et al. 28 found no influence of the ASA score on the restoration of autonomy. In their study, physical autonomy was assessed by two elements, namely mobility and difficulty in walking. However, the limitation of the physical functioning is a parameter which the ASA classification takes into account from class 3. 29 Like Morri et al., 30 our study showed that the delay in the initiation of verticalization postoperatively, the presence of at least one complication of recumbency, a Charlson score greater than 1 were factors of poor prognosis for the restoration of physical autonomy prior to the fracture. Our study did not find an influence of the type of fracture or the surgical technique on the restoration of postoperative autonomy. This observation was also made by Michel et al. 28 who nevertheless specifies that, in postoperatively there was greater difficulty in walking in intracapsular fractures. Our study showed that anemia is a factor in the deterioration of postoperative physical autonomy. The pejorative role that anemia plays in restoring physical autonomy after surgical treatment of a fracture of the proximal femur in the elderly has been highlighted by several authors. In their randomized clinical trial, Gregersen et al. 31 showed that in patients operated on for fracture of the proximal femur, the group who received a blood transfusion to maintain a hemoglobin level above 11g/dl had a significant improvement in their physical performance.
One of the limitations of this study is that there are no control groups that have not undergone surgery to do a comparative analysis. The limitation of the memory bias was done using the standardized Katz questionnaire, the items of which are quite precise. Other limitations are the small sample size and an autonomy assessment of up to one year, which may be considered too short. This was considered to be the time when hip function peaks after surgery. Comparative studies are needed to measure the impact of surgery on restoring the physical autonomy of the elderly.
Conclusion
Fractures of the proximal femur are a growing problem in sub-Saharan Africa. This study showed that even at over 90 years of age, surgery can significantly restore previous autonomy. In addition, almost all of the factors found associated with a deterioration in physical autonomy are modifiable. The early admission and management of patients, the prevention of complications in decubitus, the early emergence after surgery and the management of anemia are key points in restoring physical autonomy after a bone fracture. proximal femur of the great old man are modifiable. Measures to prevent their occurrence should be of interest to health policies given the progressive aging of the sub-Saharan population.
Footnotes
Acknowledgements
We gratefully acknowledge the participants of this research for contributing their time and effort.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.