
Abstract
Introduction:
Osteoporotic hip fractures are a major problem. They increase mortality, morbidity, and functional decline. Recovery of ambulatory status is an essential prerequisite for older adults living in a normal environment. The main objective of this study was to investigate walking failure at 3 to 6 months after hip fracture surgery with the aim of identifying pre- and perioperative risk factors associated with it.
Methods:
A total of 120 participants (>65 years) were recruited following hip fracture surgery at a teaching hospital. Walking status was assessed on average 4.4 ± 1.3 months after hip fracture surgery and compared with prefracture walking status. The participants were divided into 2 groups according to walking status (group 1: ambulatory; group 2: nonambulatory) and risk factors associated with a failure to walk were determined using binominal logistic regression analysis.
Results:
The rate of recovery to prefracture ambulatory status was about 18.3% and 25% of participants could not walk at all. Risk factors for not being able to walk at all included poor prefracture ambulatory status and living at a long care facility as nonmodifiable factors, whereas a shorter length of stay before surgery and having a longer total hospitalization periods were modifiable factors.
Conclusion:
Walking recovery after hip fracture surgery was very poor at 3 to 6 months after hip fracture surgery. Based on our findings, older adults living in a long care facility should be provided their medical and functional needs through professional health-care providers and systematic health delivery systems. The therapeutic management for underlying diseases affecting surgery should precede unconditional early surgery. Older adults hospitalized during longer periods should be focused on their functional care.
Introduction
Osteoporotic hip fractures are an increasing burden to public health systems due to their increasing incidence with the aging of populations. 1 In South Korea, the percentage of people aged 65 years or older was about 13.9% in 2017 and is projected to be about 42.7% in 2040. 2 Similarly to other countries, in South Korea, hip fractures in those over 65 years of ages are frequent, with 60 687 (77%) of a total of 78 799 patients occurring in these patients. 3 This trend is also associated with a health-care burden, causing high mortality, morbidity, and reduced function with a lower quality of life. 4,5 Surgical treatment is standard to improve survival and physical function, but the consequences are often unsatisfactory. 5,6
The main indicator of functional recovery after hip fracture surgery is restoration of walking status to prefracture levels. 6,7 Recovery of walking status is an essential prerequisite for older adults living in a community-dwelling environment. 8 In addition, older adults recognize functional ability in daily life as a health indicator. 9 Therefore, walking status as a metric of physical recovery following hip fracture surgery is worthwhile to investigate. Currently, walking recovery following hip fracture surgery to prefracture status is poor with about 50% recovering in 6 months 10 to 1 year 7,11 and 38.6% in 2 years. 6 Although patients usually receive home exercise guidance before discharge, follow-ups for walking recovery are rarely conducted. 12 Thus, understanding post-hip fracture surgery walking status and its associated factors can provide health-care providers with valuable information for facilitating mobility and independence to the elderly.
Of note, some of the over-65s who could walk in and/or outdoors with or without aids preoperatively had become immobile postoperatively; 9.2% to 38.9% in 3 months, 13,14 an 18.7% in 1 year 11 after hip fracture surgery, respectively. The catastrophic impact after hip fracture surgery is likely to be explained by the percentage of immobile patients. To reduce disability and socioeconomic burden following hip fracture surgery, patients who experience walking failure should be identified. Several possible factors affecting poor recovery of walking have been reported, including age, 7,10,15 comorbidities, 6,10,13 prefracture mobility, 10,13,15 cognitive impairment, 6,15 length of stay (LOS) before/after surgery, 13,14 delirium, dependence on activities of daily living (ADL), 11 partial weight-bearing after surgery, 13 albumin and 25-hydroxyvitamin D, 10 prolonged catheterization, and living arrangements. 15 However, few studies have identified factors associated with walking failure as an immobile state after hip fracture surgery. 8,11
In this study, we present the walking status of over-65s before and at 3 to 6 months after hip fracture surgery. The main goals were to investigate walking failure after hip fracture surgery and to identify pre- and perioperative risk factors associated with it.
Methods
This study utilized baseline data from a previous study (accepted, RGN-2018-078R1). The data analyzed in this study were from a study evaluating ADL and instrumental ADL of the elderly with hip fractures that was approved by the university institutional review board. This is a retrospective study covering prefracture and surgical related data. All patients fulfilling the inclusion criteria (>65 years, 3-6 months of postoperative recovery, compos mentis, and communicative). Of the 188 hip fracture surgery patients who attended a routine follow-up at a teaching university hospital, 166 patients met the inclusion criteria. Of those, 137 were interested in this study and 120 patients were finally recruited and analyzed. Patients who showed abnormal fracture healing during follow-up had a previous history of surgery and experienced walking failure before the hip fracture were excluded.
As the primary outcome of the study, self-reported walking status after hip fracture surgery was assessed by a 4-level scale of ambulatory ability 13 : 1 = “able to walk outdoors independently,” 2 = “able to walk indoors independently,” 3 = “needs assistive devices to walk,” 4 = “unable to walk even with assistive devices.” Demographics and the number of chronic diseases were collected from hospital medical records. Previous walking status and use of walking device data was collected through interviewing patients during the outpatient period as prefracture information. Previous walking status was assessed using the same scale as that used for walking status after hip fracture surgery. 13 Information related to falling over regarding number of falls and location of falls were collected from the interview. Hospital information including type of hip surgery, LOS before surgery, total LOS, and the lowest hemoglobin value at admission was collected from hospital medical records. In addition, pain and current dwelling place were collected from the interview.
The Statistical Package for the Social Sciences version 22.0 software (SPSS, Chicago, Illinois) was used for the data analysis. We presented the changes in walking status after hip fracture surgery compared to before hip fracture surgery as the numbers, along with the percentage. Bivariate analysis was carried out for the 2 different postfracture walking status’ including walking and not walking even with walking devices. Age, gender, body mass index (BMI), education, living spouse, number of family members, current dwelling place, number of chronic diseases, number of falls, falling place, type of hip surgery, LOS before surgery, total LOS, use of walking devices before hip fracture, anemia at admission, and pain were included in the analysis, being possible independent risk factors. A χ2 test was performed to compare categorical data between 2 groups able or unable to walk after hip fracture surgery. The continuous variables, such as age, BMI, LOS before surgery, and total LOS were compared by a Mann-Whitney analysis between 2 groups. Logistic regression analysis was carried out across all patients to identify the variables for failure to walk postoperatively. Variables were removed one by one from this analysis using a backward elimination process with the same possible risk factors. The probability for entry was set at .05, and the probability for removal at .10. The goodness-of-fit in the logistic model was tested by the Hosmer-Lemeshow test and an α level of ≤0.05 was regarded as significant.
Results
Comparison of Walking Status Between Prefracture and 3 to 6 Months After Hip Fracture Surgery
The Self-reported walking status of 120 patients was on average 4.4 ± 1.3 months. There were 85 patients walking outdoors independently before hip fracture. Of the 85 patients, only 17 (20%) patients reported walking recovery to the prefracture state and 10 (11.8%) patients could not walk at all. Of the 22 patients to walk indoors independently preoperatively, 9 (40.9%) patients could not walk at all; 84.6% of patients reported an immobile state in the group of prefracture patients able to walk in- and outdoors with walking devices. The rate of recovery to prefracture walking status was about 18.3%. The numbers of the patient walking outdoors independently, indoors independently, walking in- and outdoors with aids, and not walking at all within 3 to 6 months post-hip fracture surgery were 17 (14.2%), 23 (19.2%), 50 (41.7%), and 30 (25.0%), respectively (Table 1).
Changes in Walking Status at 3 to 6 Months After Hip Fracture Surgery.

aN = 120.
Postoperative Comparison of Patients’ Information Between Groups of Walking and Not Walking Even With Walking Devices
Table 2 shows the characteristics of all patients and 2 groups stratified by walking status. There were significant differences among 2 groups in relation to patients’ gender, education, current dwelling place, number of chronic disease, falling place, and use of walking devices before hip fracture. Postoperative walking success was significantly correlated with being male. It was also significantly better in people with graduate-level education and those living at home. In contrast, it was significantly worse in people with more chronic diseases. Patients unable to walk postoperatively experienced significantly more instances of falling indoors rather than outdoors and used walking devices before hip fracture. There were no differences in BMI, living spouse, number of family members, number of falls, type of hip surgery, LOS before surgery, total LOS, anemia at admission, and pain.
Comparison of Patients’ Clinical Characteristics at 3 to 6 Months After Hip Fracture Surgery Between Groups of Walking and Not Walking at all Postoperatively.a

Abbreviations: BMI, body mass index, LOS, length of stay.
aN = 120.
bMann-Whitney analysis.
cMean ± standard deviation.
d P < .05.
e P < .001.
Predictors of Failing to Walk After Hip Fracture Surgery
The outcome of risk factors for not walking at all on average 4.4 ± 1.3 months after surgery is shown in Table 3. The risk factors were living at a long care facility as current dwelling place (odds ratio [OR] = 0.289, P = .036), shorter LOS before surgery (OR = 0.813, P = .007), longer total LOS (OR = 1.109, P = .006), and use of walking devices before hip fracture (OR = 0.102, P < .001). The predictive accuracy of this model was good as the classification accuracy was 75%. The Hosmer-Lemeshow Goodness-of-fit test was used to test the fit of the model and the P value was .884, showing statistical fit.
Predictors of Walking Status at 3 to 6 Months After Hip Fracture Surgery.a
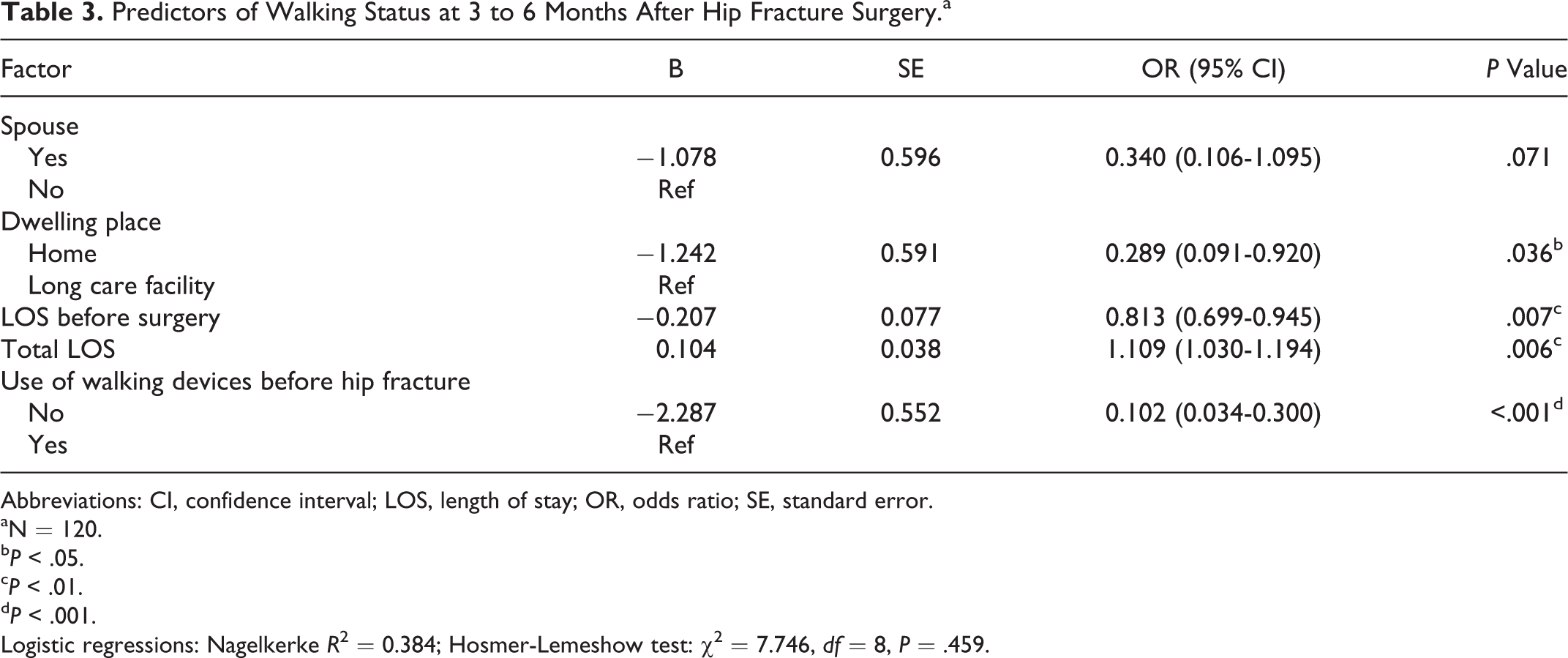
Abbreviations: CI, confidence interval; LOS, length of stay; OR, odds ratio; SE, standard error.
aN = 120.
b P < .05.
c P < .01.
d P < .001.
Logistic regressions: Nagelkerke R 2 = 0.384; Hosmer-Lemeshow test: χ2 = 7.746, df = 8, P = .459.
Discussion
In the present study, most of the patients had not regained their walking status on average 4.4 ± 1.3 months after hip fracture surgery. The number of not walking at all postoperatively was 30 patients (25%) even though patients immobile before surgery were excluded to investigate catastrophic decline in this study. Early identification of the cause of walking failure in patients who could walk before the hip fracture can provide a way to reduce this catastrophic decline in walking ability, since significant functional recovery had been occurred 3 to 6 months after hip fracture surgery. 5,11 Elderly patients undergoing hip fracture surgery may already have significant frailty 16 due to their advanced age, 7,10,15 comorbidities, 6,10,13 and poor nutrition. 10 A high level of frailty can result in walking failure. 16 This study compared patient walking status before and after hip fracture surgery as an index of frailty. The results showed that the poorer the pre fracture walking status, the greater the rate of walking failure after hip fracture surgery.
The rate of walking recovery was much lower than studies from European countries in which approximately 50% patients regained prefracture walking status at 3 or 6 months postoperatively. 10,11 On the other hand, a previous study 6 observing Korean patients reported lower functional recovery rate at 38.6% by the second year after hip fracture surgery. Furthermore, the rate of post-hip fracture walking failure was almost the same as with patients from Japan, whereas the rate of postoperative walking inability was only 9.2% in patients from the United States. 13 Delayed partial weight-bearing after surgery has been reported to predict lower walking ability at 3 months after surgery. 13 The number of average days initiating partial weight-bearing is 8 in South Korea 17 and Japan, yet 3 in the United States. 13 Identifying the start time of partial weight-bearing after surgery is necessary for initiating it at the earliest possible time.
Previous studies 18,19 reported that functional recovery of individuals of the Caucasian race was higher than Hispanic and Asian people. However, they 18,19 suggested that the result could not reach a meaningful conclusion due to a lack of specific distinctions for race or ethnicity. Thus, studies concerning the influence of race or ethnicity on differences in walking recovery cannot be confirmed. In addition, health-care delivery systems for hip fracture care may be different, affecting functional recovery according to race/ethnicity. 18,19 In Korea, most patients do not have a rehabilitation linkage system after hip fracture surgery, compared to the United States, which receives rehabilitation benefits through Medicare. 20 The absence of a smooth transition in a postdischarge rehabilitation hospital for patients who have undergone hip fracture surgery may also negatively affect functional recovery.
Walking failure following hip fracture surgery occurred more often in female older adults (>65 years of age) who had a poor education, were admitted in long care facilities, had more chronic diseases and, experiences of indoor falls, and use of walking devices before hip fracture surgery in this study. The results of previous studies with respect to poor education, 21 admittance to long care facilities, 5,15 more chronic diseases, 10 indoor falls, 8 and using walking devices before hip fracture surgery 8,10,11,15 were consistent with those of our study. Meanwhile, the difference of walking status on gender was inconsistent according to studies. Previous studies 10,19 reported that male patients had a slight or significant advantage in terms of walking recovery, while Beaupre et al 22 found no such difference. Further studies are necessary to help understand gender influence on walking status after hip fracture surgery.
In this study, one of the risk factors associated with not walking at all was current dwelling place. Patients living in homes could walk well compared to those in long care facilities, consistent with a previous study. 10 Most older adults (>65 years) at 3 to 6 months post-hip fracture surgery might go to homes or long care facilities as available options in South Korea. Although we did not know how many patients went to rehabilitation hospitals immediately after discharge, they would have already been discharged from the rehabilitation hospitals before 3 to 6 months after hip fracture surgery. This result is reasonable considering that older adults (>65 years) dwelling in long care facilities cannot perform independent activities due to physical and functional decline and extensive medical needs. 23 In addition, policies of long care facilities tend to focus more on patient safety and completion of staff duties rather than care to promote patient physical function. 24 The culture of care focused on patient safety may impair patient mobilization and, therefore, walking recovery. The focus of care for older adults (>65 years) in long care facilities should be changed to accomplish and maintain the highest functional level.
A shorter LOS before surgery negatively affected walking status after hip fracture surgery. The effect of the LOS before surgery is controversial. A previous study 15 was similar with this result whereas other studies 13,14,25 indicated that longer LOS before surgery negatively affected walking ability, causing longer preoperative immobile status. There is moderate evidence that hip fracture surgery within 48 hours after admission improves mobility and survival. 26 However, elderly patients who undergo hip fracture surgery face significant challenges, due to their comorbidities and taking medications affecting surgery. Optimal perioperative care has been suggested to improve their recovery 27 ; however, this study could not clarify why a longer LOS before surgery was required. A possible reason could be that if patients had a longer LOS before surgery for management of underlying diseases affecting surgery, the management itself might positively affect their physical recovery. Further studies related to LOS before surgery are needed in order to identify the factors associated with LOS before surgery. This study also suggests that the diagnosis and treatment of elderly patients should be performed as soon as possible after admission.
A longer total LOS was associated with walking failure after hip fracture surgery. However, there was a significant difference as a result of longer hospitalization between South Korea and Japan. That is, longer hospitalization positively affected walking status in Japan, 14,28 whereas in South Korea it did not. Kondo et al 14 reported that if frail elderly patients are discharged without general condition being restored, they will suffer more negatively in terms of walking and mortality. Interestingly, participants in this study were discharged without systematic rehabilitation during hospitalization. If they had longer total LOS without systematic rehabilitation, longer hospitalization itself may extend the amount of bed rest, thereby worsening walking status. Therefore, older adults (>65 years) hospitalized during longer periods should also be focused on their functional care.
Using walking devices prior to hip fracture surgery was the most nonmodifiable factor affecting failure to walk postoperatively in this study, aligning with the results of several studies. 8,10,11,15 Based on this result, anticipation of postoperative walking ability needs to be tailored preoperatively in the patients by means of walking devices before hip fracture surgery. Customized rehabilitation interventions should be conducted on the level of walking status before hip fracture surgery. In this study, 11.8% of the independent patients without walking devices before hip fracture surgery could not walk at all at 3 to 6 months following hip fracture surgery. Future studies are needed to identify risk factors for the catastrophic decline in walking status in these patients.
The principal limitation of this study is that walking status during the follow-up appointment was self-reported and no objective measures, such as gait speed or Timed Up and Go, were used. Secondly, we could not analyze other factors including cognitive deficits, abnormal fracture healing, and a previous history of hip fracture that might affect the inability to walk due to the second analysis. Thus, this study cannot draw any conclusions for patients with these factors. Further research is required to investigate other factors that may affect walking failure. Thirdly, this study could examine only the number of chronic diseases, and not their types and severities. Therefore, the result pertaining to chronic disease should be interpreted with caution. Finally, this study could not ascertain long-term walking status as data were only investigated on average 4.4 ± 1.3 months postoperatively.
Conclusion
Walking status on average 4.4 ± 1.3 months after hip fracture surgery was very poor. Based on our findings, older adults (> 65 years old) living in a long care facility should be supplied their medical and functional needs through professional health-care providers and systematic health delivery systems. The therapeutic management for underlying diseases affecting surgery should precede unconditional early surgery. Older adults (>65 years) hospitalized during longer periods should also be focused toward their functional care.
Footnotes
Authors’ Note
Primary data were approved from an institutional review board (KNUH 2015-02-017) and all patients provided written informed consent postoperatively. The abstract was presented as poster at the 25th World Congress on Nursing Care, July 24-26, 2017 in Melbourne, Australia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.