
Abstract
Introduction
The elderly population is increasing due to improvements in medical science, which have also enhanced quality of life. 1 This has led to an increase in the incidence of fragility hip fractures, which poses a significant health burden worldwide. Hip fractures in the elderly are often accompanied by pain, disability, and physical limitations, leading to diminished quality of life, a greater need for long-term care, and mortality. 2
Surgery is the best treatment for most hip fractures, but is associated with a wide range of complications. Surgical complications, such as wound infection and loss of reduction are rare, but, non-surgical complications, such as delirium, pneumonia, and heart failure, are commonly encountered. 3 It has been reported that delirium and pneumonia are associated with increased mortality after hip fracture surgery. 4
In clinical practice, even with standard therapy and intensive monitoring, patients with postoperative pneumonia (POP) have high mortality rates and unsatisfactory outcome. 5 In total, 14% of hip fracture patients with POP die within 30 days, compared to only 1.7% of those without POP. 6 Antibiotics are useful for the treatment of pneumonia, but older hip fracture patients often have chronic diseases and a reduced ability to cope with the physiological stress associated with the fracture. 7 Therefore, it is important to prevent the occurrence of pneumonia and reduce postoperative mortality rates by identifying at-risk patients.
Several studies have reported risk factors for POP, but there have been no comprehensive evaluations. Thus, it is necessary to review the results of recently published research to identify the risk factors. This meta-analysis aimed to explore the risk factors for the development of POP in older patients after hip fracture surgery.
Methods
Data Sources and Search Strategy
We identified relevant studies published in the PubMed, Embase, and Cochrane Library databases up to June 30, 2021. The search terms were as follows: (risk [Title/Abstract] OR predictor [Title/Abstract] OR factor [Title/Abstract]) AND pneumonia [Title/Abstract] AND (hip [Title/Abstract] OR femur [Title/Abstract]) AND fracture [Title/Abstract] AND (postoperative [Title/Abstract] OR surgery [Title/Abstract]).
Study Selection
Two reviewers (KUK and SHL) independently scanned the titles and abstracts identified by the initial search and selected potentially relevant studies. Full texts were obtained if the information provided in the title or abstract met the selection criteria.
Data Extraction
Data extraction was completed by two researchers (KUK and SHL) working independently, and any disagreements were resolved by consensus. The following data were extracted from the included papers: author’s first name, year of publication, study design, sample size, age cutoffs or mean age, and fully adjusted odds ratios (ORs), hazard ratios (HRs), and 95% confidence intervals (95% CIs) for the identified risk factors or predictors.
Quality Assessment
The quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS) for cohort studies. 8 The NOS was developed to assess the quality of nonrandomized studies in three areas: selection of the study groups (four items); comparability of the groups (two items); and ascertainment of the exposure variable and outcome of interest for case-control and cohort studies respectively (three items). Items judged as adequate receive a star and one point. Overall NOS scores range from between 0 and 9; a score ≥6 represents a high-quality study.
The overall quality of the evidence for each risk factor in the pooled analysis was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines. 9 Each study was assessed in four domains: limitations, inconsistencies, indirectness, and imprecision. Based on these domains, the evidence for each specific outcome was rated as high, moderate, low, or very low quality. 9
Statistical Analysis
Data were analyzed using Review Manager 5.4 (The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark) and R software (3.6.3 for Windows; RStudio, Boston, MA, USA). For all analyses, 95% CIs and forest plots were calculated. Statistical heterogeneity was estimated using the I2 statistic. If I2 was 20% or more, a random-effects model was used, and if it was less than 20%, a fixed-effects model was used. We did not assess publication bias because of the small number of studies eligible for this meta-analysis; the Cochrane Handbook for Systematic Reviews of Interventions (https://training.cochrane.org/handbook) states that a minimum of 10 studies are required to perform a publication bias assessment when using funnel plots.
Results
Search Results and Quality Assessment
A total of 327 studies were identified in the initial search. After omitting duplicates, 194 studies remained. Of these, 142 were excluded after scanning the titles and abstracts, and another 28 were excluded after full-text review. Thus, 24 studies were finally included in the analysis Figure 1. The point prevalence of POP in the 24 individual study populations ranged between .4% and 18.3%, with an overall prevalence of 5.0% (95% CI: 3.0-7.0). The level of heterogeneity was high (I2 = 99%) Figure 2. The study characteristics are shown in Table 1. NOS was used to assess the quality of the included studies. Ten studies scored 9 points, 8 scored 8 points, and 6 scored 7 points. Details of each included studies assessment are shown in Supplementary Table 1. Flow chart of literature screening. The prevalence of postoperative pneumonia with 24 study populations. Characteristics of Included Studies.

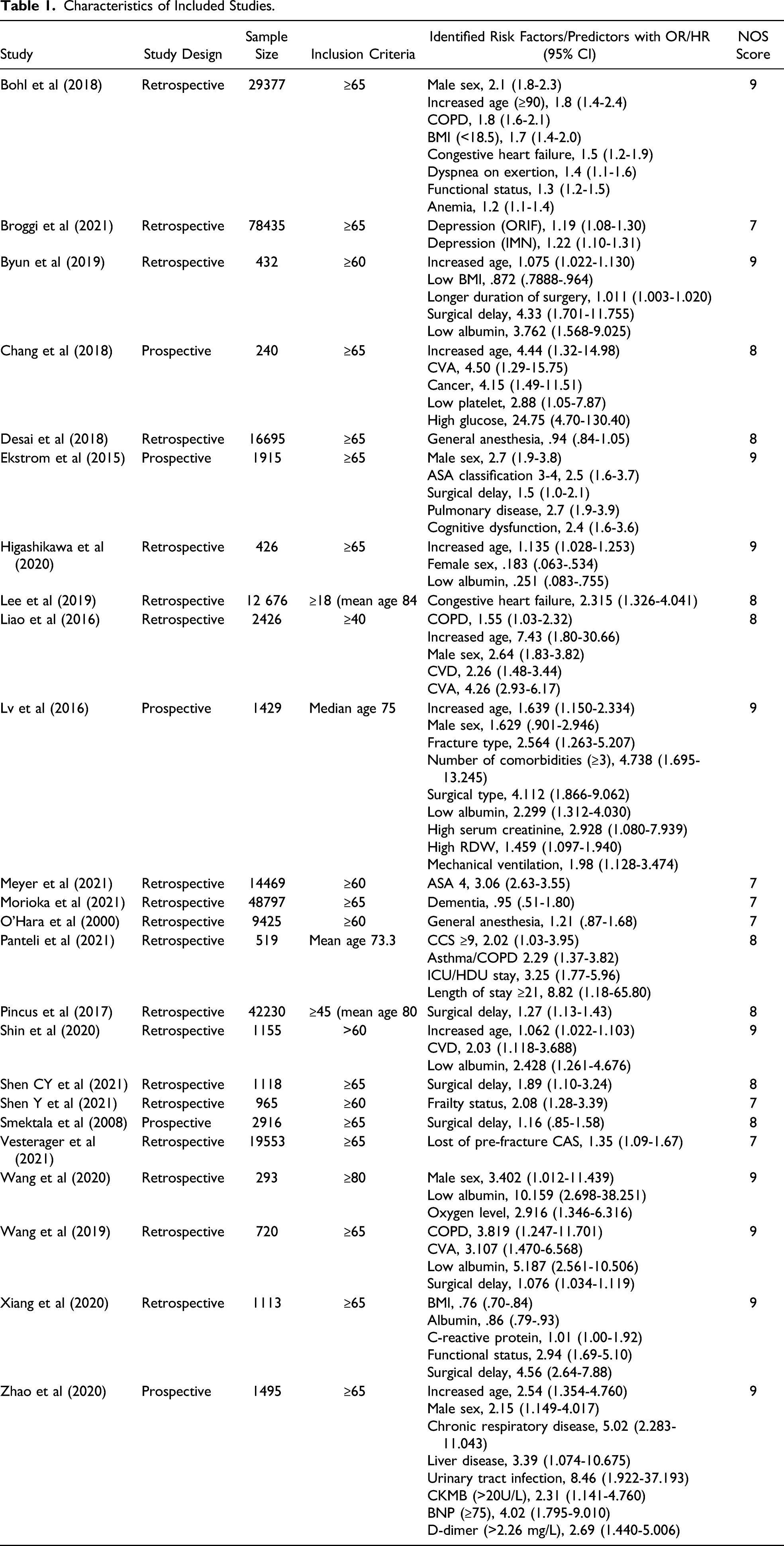
Characteristics of Included Studies
Factors associated with POP reported in the included studies were age, sex, delayed surgery, chronic respiratory diseases, serum albumin, cardiovascular diseases, body mass index (BMI), general anesthesia, ASA score, mobility function, cognitive disorder, congestive heart failure, functional status, fracture type, anemia, depression, and duration and type of surgery. The effect sizes of these risk factors are listed in Table 1.
Risk Factors for Postoperative Pneumonia
There were a total of 36 risk factors, and the meta-analysis included the five most common ones: age (OR: 1.25, 95% CI:1.11-1.40), delayed surgery (OR: 1.84, 95% CI: 1.29-2.63), low serum albumin (OR: 2.34, 95% CI: .82-6.73), chronic respiratory diseases (OR: 2.42, 95% CI: 1.82-3.24), and male sex (OR: 2.22, 95% CI: 2.00-2.47) Figure 3,4. According to GRADE, male sex, delayed surgery and chronic respiratory diseases had moderate-quality evidence, while age and serum albumin had very low and low-quality evidence, respectively, Table 2. Factors associated with postoperative pneumonia in a random-effects model. Factor associated with postoperative pneumonia in a fixed-effects model. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) of Pooled Meta-Analysis Studies. 1There is substantial heterogeneity among studies in meta-analysis (I2 ≥ 50%). The enrolled population of the study by Liao, 2016, are ≥40 years. The 95% CIs of the studies by Liao, 2016, and Wang, 2020, are too wide. 4The odds ratio = around 2.5 for moderate effect, ≥ 4.25 for large effect.


Discussion
The present study investigated the prevalence and risk factors for POP following geriatric hip fracture surgery through a meta-analysis. The prevalence of POP was 5% among 24 studies; 6 studies reported a prevalence of more than 10%.7,10-14 In particular, one study a very high prevalence of 18%. 11 That study was conducted on patients who underwent subtrochanteric fracture surgery, a relatively high proportion of whom had lung malignancies (6.3%).
Our meta-analysis of five important risk factors revealed that age, male sex, chronic respiratory diseases, delayed surgery and low serum albumin were all significantly associated with the occurrence of POP. Age and sex are known risk factors for morbidity and mortality after hip fracture. 15 The meta-analysis included 8 studies that analyzed age as a risk factor. Although the age cutoff for high risk of POP following geriatric hip fracture surgery was variable, three studies reported that patients aged >80 years were at a particularly high risk for POP.14,16,17 Furthermore, the risk for POP increases with age, and older patients who developed POP had longer hospital stays and higher mortality rates. 18 This suggests that the elderly, especially those over the age of 80 years, are more likely to develop POP after hip fracture surgery and thus require special attention. In 6 studies, males were found to be at a greater risk for POP after hip fracture despite a higher incidence of hip fractures in females. This may be explained by the fact that males tend to have poorer health and more comorbidities compared to females. 17
We found that delayed surgery was a risk factor for POP, based on moderate-quality of evidence. Many studies and guidelines recommend that older hip fracture patients undergo surgery as soon as possible to reduce the risk of postoperative complications especially pneumonia. 19 Early surgery leads to early restoration of motor function and fewer of the complications associated with bed rest. 13 Six papers on surgical delay were included in our meta-analysis. One study found that a delay of more than 24 h was associated with an increased risk of POP, while two others found that a delay of more than 36 h increased the risk (although in one of these studies the association lacked statistical significance). The remaining three studies demonstrated an increased risk of POP with a delay of more than 48 h. Therefore, it is important to perform the surgery as soon as possible, preferably within 48 h, to prevent POP.
Chronic respiratory diseases were also found to be associated with the risk of POP after hip fracture surgery in five studies. Four of those studies reported an increased risk with chronic obstructive pulmonary disease (COPD).2,11,16,17 In one study, COPD patients had higher rates of postoperative complications, including 30-day pneumonia, 30-day readmission, 30-day acute respiratory failure, and 1-year mortality, as well as longer hospital stays. 2 Prevention and early management of fractures is important in COPD patients. Most COPD patients are elderly, smokers, and oral- or inhaled-steroid users, so the risk of osteoporosis and fractures is high. 20 Pharmacologic therapies such as inhalers are effective for improving lung function and preventing acute COPD exacerbations. Although the effectiveness of inhalers for preventing complications, such as pneumonia, after hip fracture surgery has not been well studied, use of an inhaler and chest care after surgery may help prevent complications after surgery in COPD patients.
Our results demonstrated that a low serum albumin level was a risk factor for POP after hip fracture surgery. Serum levels of albumin, a negative acute phase protein produced in the liver at a rate of 12-25 g/d, reflect nutritional status. 21 Serum albumin concentrations are influenced by multiple factors, including nutritional status, liver failure, malignancy, surgical trauma, inflammation, comorbidities, and other conditions. 22 Low serum albumin levels may compromise the immune system. 23 Patients with hypoalbuminemia have lower nutritional reserves and weaker immune systems. 12 Previous studies have reported that preoperative hypoalbuminemia is a risk factor for postoperative complications in various types of surgery. 24 Malnutrition is particularly prevalent among the elderly, and is an independent risk factor for POP after hip fracture surgery. 12 Measuring the serum albumin level is a simple method to assess protein energy malnutrition, which is a modifiable factor. 25 Nutritional supplementation for hypoalbuminemia may reduce the incidence of POP in elderly hip fracture patients.
Our study was the first to analyze the risk factors for POP in elderly hip fracture patients, through a meta-analysis of recent studies. However, this study had several limitations. First, although designed as a meta-analysis of elderly patients, it also included studies conducted on adult patients in other age groups. However, in line with hip fractures occurring mainly in the elderly, the mean age of the patients in these studies was over 65 years. Second, it was not possible to determine the cause of POP because most of the studies did not distinguish between aspiration pneumonia and other types. Third, we used the original data from the studies, and confounding factors and bias caused by basic comorbidities were not fully addressed. Finally, methodological issues existed for all included studies that might influence conclusions, and this is especially the case for included retrospective nonrandomized studies. Furthermore, limitations include the small number of eligible studies and the significant heterogeneity between the included studies regarding outcomes reported. Although the random effect model was used to address heterogeneity among the studies evaluated, the conclusions should be carefully interpreted.
Conclusions
In clinical practice, it is not easy to predict the occurrence of pneumonia after surgery. Pneumonia is a debilitating condition in elderly patients, and it is necessary to be aware of the risk factors to prevent it. Age, male sex, chronic respiratory diseases, delayed surgery, and a low serum albumin level are all significant risk factors that must be taken into account.
Supplemental Material
sj-xlsx-1-gos-10.1177_21514593221083825 – Supplemental Material for Risk Factors for Postoperative Pneumonia in the Elderly Following Hip Fracture Surgery: A Systematic Review and Meta-Analysis
Supplemental Material, sj-xlsx-1-gos-10.1177_21514593221083825 for Risk Factors for Postoperative Pneumonia in the Elderly Following Hip Fracture Surgery: A Systematic Review and Meta-Analysis by Sang Hee Lee and Ki Uk Kim in Geriatric Orthopaedic Surgery and Rehabilitation
Footnotes
Acknowledgments
This research was supported by the Wonkwang University in 2022.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.