
Abstract
Background
The degree of joint space narrowing measured on radiographs provide a reliable estimate of the extent and severity of Osteoarthritis (OA) of the knee. While the standing antero-posterior (AP) view radiographs have been used traditionally, recent studies suggest that the Lyon-Schuss (LS) view is able to detect early OA changes better. The present study was, therefore, conducted to make an objective comparison between the two views with respect to their corelation with the patient's clinical and radiological scores.
Methods
Forty patients (80 knees) were included in this cross-sectional study. Medial as well as lateral tibiofemoral joint space widths (JSW) were measured using vernier callipers on printed, calibrated radiographic images. Knee Society Score (Function) (KSS-F) was used as the clinical outcome measure while Ahlbäck grade was used for determining radiological severity. JSW was correlated with KSS-F and the Ahlbäck grade using Spearman's rho correlation coefficient. Reproducibility of the method was assessed using the intra-class correlation coefficient (ICC).
Results
Average age of the participants was 60 ± 7.65 (range 50–78) years, with 18 males and 22 females. ICC for intraobserver reliability was 0.97 and for inter-observer reliability, was 0.91 (AP view) and 0.92 (LS view), respectively. Medial JSW measurements taken on the AP view were found to have a significantly higher degree of correlation with both KSS-F and Ahlbäck grade (p < 0.05) than those obtained from the LS view.
Conclusion
Although the LS view may be more sensitive for detecting early OA changes in knee, particularly in the lateral tibiofemoral compartment, the present study shows that AP view correlates better with the patient's overall clinical and radiological profile.
Introduction
Osteoarthritis (OA) of the knee is a chronic degenerative pathology which has been implicated as a major cause of disability in the community, imposing significant social as well as economic costs. According to the National Health Interview Survey, approximately 14 million people in the United States of America have symptomatic knee OA. 1 In the Indian subcontinent, estimated prevalence varies from 22–39%.2–4 OA is a slowly evolving disorder of synovial joints in which a complex combination of degenerative and reparative processes alters the normal anatomy and matrix composition of the articular cartilage and subchondral bone. 5 In most instances, OA of the knee is idiopathic in origin (primary OA). However, in some cases OA may result secondary to an underlying cause such as rheumatoid arthritis (RA), trauma, infection etc.2,6 Other risk factors include age, female sex, obesity, high bone mineral density, previous surgery as well as local biomechanical forces acting on the joint.2,7
Although magnetic resonance imaging (MRI) is the most sensitive imaging modality for detecting articular cartilage damage, 8 plain radiography offers a far more economical and easily available option. 9 Radiographs are also useful for determining the extent as well as severity of the disease such as joint space narrowing (JSN) of the tibiofemoral compartments which is still considered the hallmark of progression of knee OA. 10 Moreover, measurement of joint space width (JSW) has not only been recommended as a valuable tool to determine the endpoint in clinical trials concerning disease-modifying osteoarthritis drugs (DMOADs), 11 but also as an adjunct to evaluate the extent of articular cartilage thickness as well as destruction.12,13
It is important that the technique used to make an absolute measurement of the JSW be as accurate as possible. However, it has been shown that there are several factors which influence the outcome of JSW measurement, such as the alignment of the medial tibial plateau with the X ray beam, degree of knee flexion, weight bearing, rotation of the ipsilateral foot, angle subtended by the X ray beam etc.14–16 Some of these factors, such as weight bearing X rays, have been previously utilized to make a more accurate calculation of the JSW which is helpful in the early diagnosis of OA.10,17,18 However, the precision of JSW assessment with the various flexion views of the knee, such as the Lyon-Schuss (LS) view, have not been studied in great detail. The latter is a postero-anterior (PA) view of the knee in 20–30 degrees of flexion and is considered by some authors to more sensitive to JSN than the standard antero-posterior (AP) view.10,18,19 The rationale behind this is the fact that major contact stresses in the tibiofemoral articulation occur when the knee is flexed to 28 degrees. 20
While knee JSW has been shown to correlate significantly with the patient's Knee injury and osteoarthritis outcome score (KOOS) parameters viz. pain, symptom and quality of life, 21 an objective comparison between the AP and the LS radiographic view JSW measurements with respect to the patient's clinico-radiographic scoring has not been carried out till date. The present study was, therefore, undertaken with the objective of determining which of the above two views had a better correlation with the Knee society score (KSS) as well as Ahlback grade and see if the LS view could be used as an alternative to the more commonly performed AP view.
Materials and methods
This was a cross-sectional study involving 40 patients (80 knees) who attended the outpatient department of a tertiary care institution in north-western India. Subjects from both gender with age more than 18 years were included in the study. Patients with secondary OA of the knees, flexion deformity more than 30 degrees and those who refused to give consent for study, were excluded. Approval was taken from the Institutional ethics committee. Written informed consent was obtained from all the patients included in the study.
Clinical assessment of the subjects was performed by two senior orthopaedic surgeons (AE and DJ). For each case, a detailed history was taken followed by a thorough physical examination of both the knees. The KSS-F(Function) was used as the primary clinical evaluation tool and calculated for all the patients.
Every patient was subjected to a conventional weight bearing AP view of the knee (in full extension) as well as the LS view with knee in 20–30 degrees of flexion (Figure 1).10,19 Accuracy of the radiographic view was assessed by noting the vertical distance between the anterior and posterior tibial condylar projections. A difference of more than 1 mm was treated as an incorrect projection and hence, rejected. All radiographs were read and assessed by the senior radiologist (PK), who was blinded to the patient's clinical details and their corresponding KSS-F scores. OA severity was graded according to the classification system given by Ahlbäck. 17
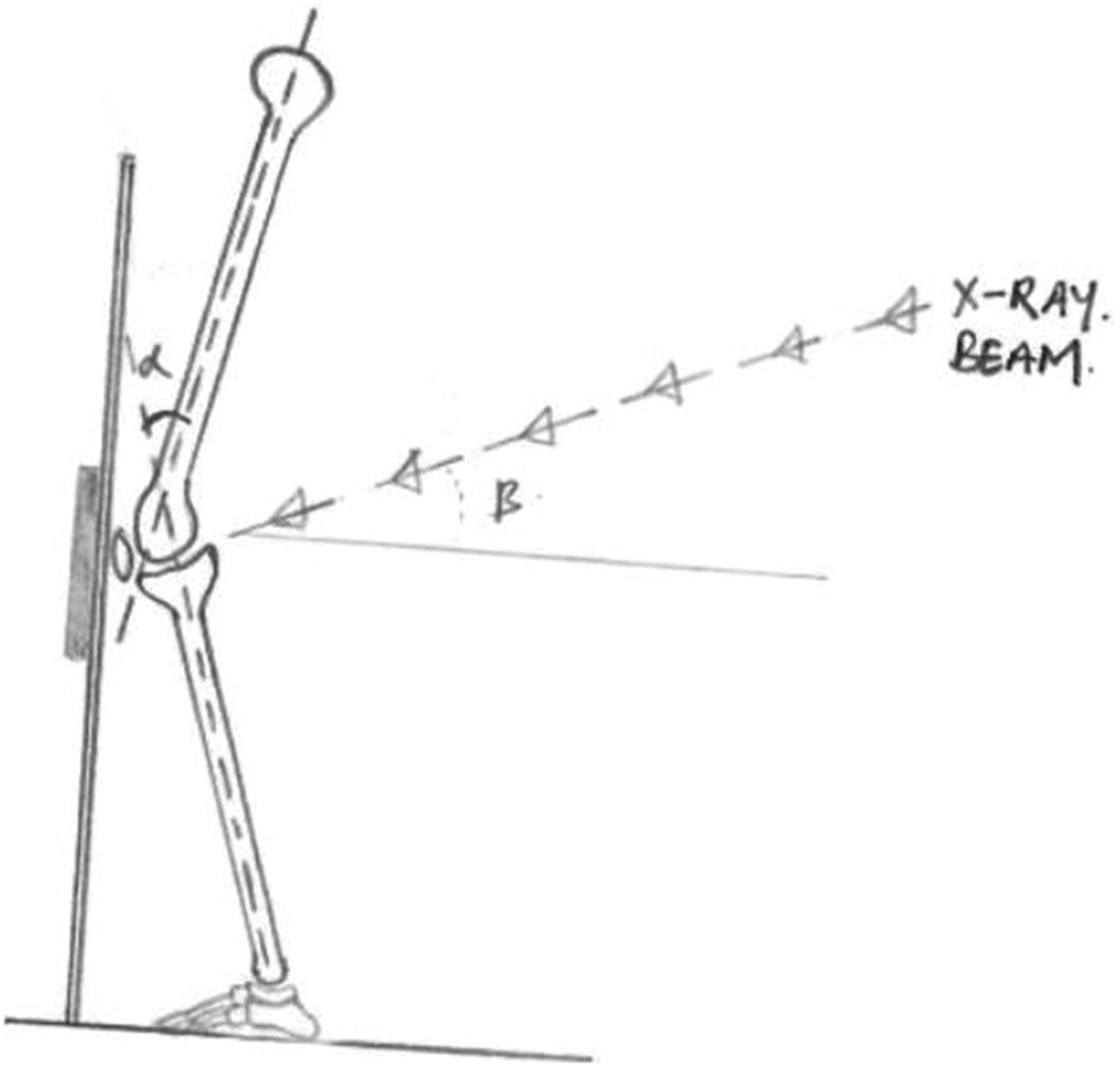
Diagrammatic representation of the position of the knee and the direction of the X ray beam during the lyon-schuss view [α = 20–30 degrees; β = around 10 degrees].
JSN and osteophytes were documented for each knee. Quantification of JSN was done by two independent observers (SS and AG) using a printed, calibrated digital radiographic images. Magnification of the image was set at zero. Measurements were done using a vernier calliper. For both medial and lateral tibiofemoral compartments, JSW was taken as the average of three readings measured at a prefixed distance of 5 mm, 10 mm and 15 mm from the tibial intercondylar eminence (Figure 2). Careful evaluation of the marginal osteophytes was done and they were excluded from the distance measurements. For determining the reproducibility of results obtained using our technique, two measurements of ten separate LS and standing AP radiographs were carried out. The latter was not a part of the original study sample but resembled the study population demographically. In all ten X rays, JSW was measured in the medial tibiofemoral compartment only. These measurements were repeated after two weeks. Both observers were blinded to each other as well as to the results of the previous assessment.
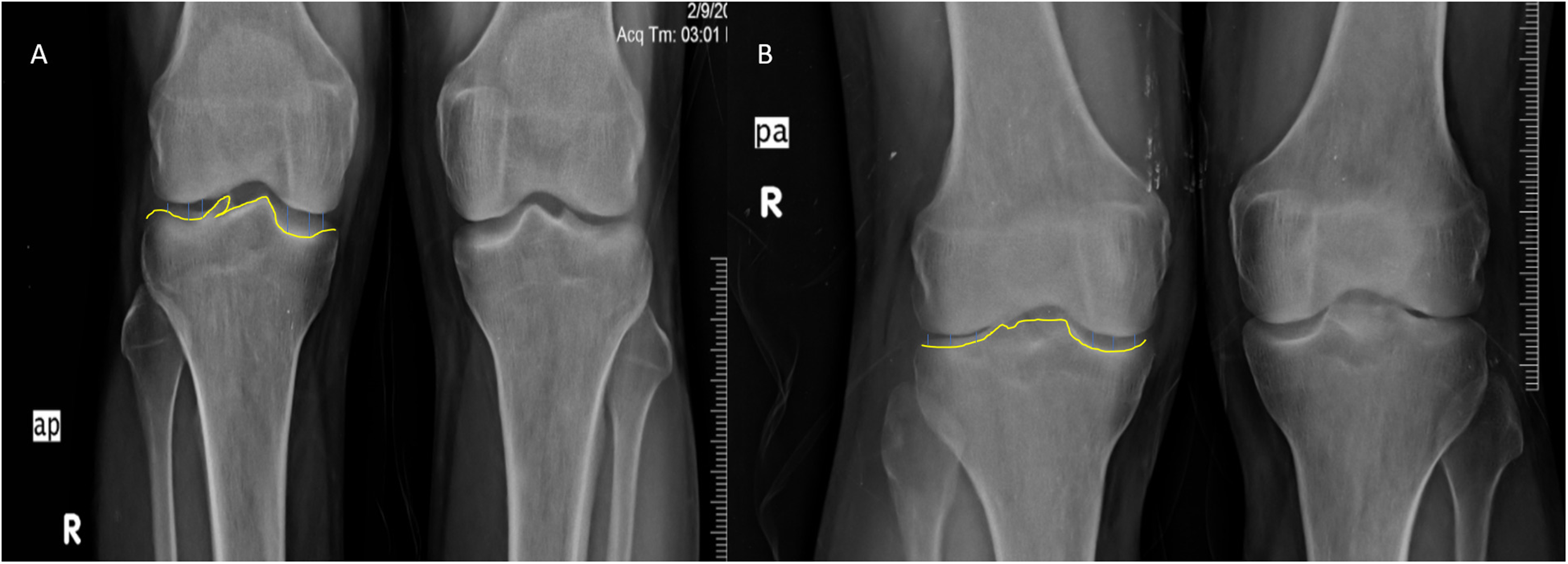
X-ray images depicting: (A) Antero-posterior view of the knees in standing position with joint space width measurements at the designated levels; (B) Lyon-Schuss view of both knee joints of the same patient depicting joint space measurements.
Results
Average age of the participants was 60 ± 7.65 (range 50–78) years. The study population comprised of 18 males and 22 females. The degree of severity of OA was slightly higher in males (mean Ahlbäck grade 1.7 ± 0.7) than females (mean Ahlbäck grade 1.6 ± 0.7). This corroborated with a better average KSS-F in women (83.5 ± 14.9) vis-à-vis men (70 ± 22).
The ICC for intra-observer reliability was 0.97 for both AP and the LS views and for inter-observer reproducibility, were 0.91 (AP view) and 0.92 (LS view) respectively. Initial correlation of the MJSW and LJSW with KSS-F showed that quantitative medial JSN had a significantly higher (p < 0.05) degree of association with the patient's clinical as well as radiological scores than that seen in the lateral tibiofemoral compartment. Moreover, MJSW measurements taken in the AP view correlated significantly better (p < 0.05) with KSS-F and Ahlbäck grade than those obtained using the LS view (Tables 1 and 2).
Correlation of the joint space width measurements with the functional score KSS-F (AP view and the LS view).

KSS-F: Knee Society Score (Function); MJSW: Medial joint space width; AP: Antero-posterior; LS: Lyon-Schuss.
Correlation of the tibiofemoral joint space width (medial compartment) with the Ahlbäck grade (AP view vis-a-vis the LS view).
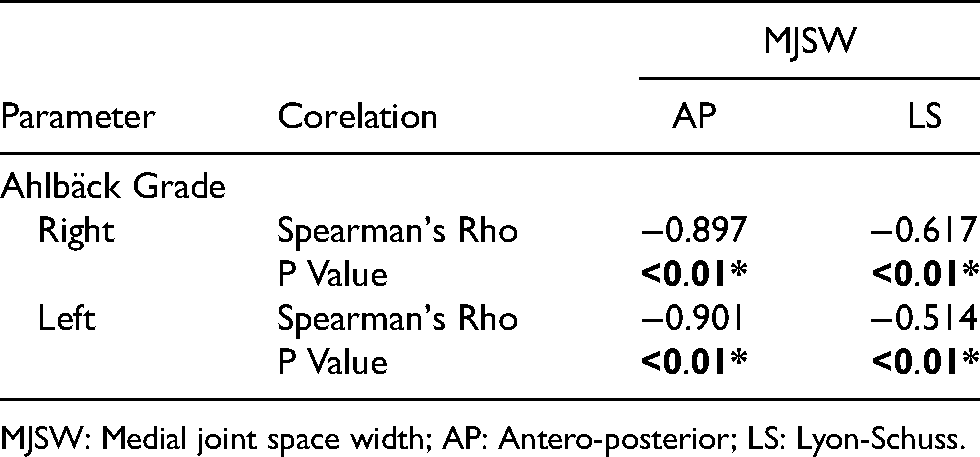
MJSW: Medial joint space width; AP: Antero-posterior; LS: Lyon-Schuss.
Discussion
The progression in the severity of OA knee as seen on radiographs, mirrors worsening of the patient's clinical symptoms.21–23 Using KOOS as the primary clinical outcome evaluation tool, Oak et al. 21 showed that lower baseline minimum JSW and a greater decrease in 4-year JSW corelated significantly with a deteriorated patient profile. The same was validated by Fukui et al. 24 using outcomes derived from the Japanese Knee Osteoarthritis Measure. A cross-sectional analysis by Duncan et al. 23 also concluded that a higher Kellgren-Lawrence (KL) grade correlated significantly with a higher pain, stiffness and disability Western Ontario and McMaster Universities (WOMAC) Osteoarthritis Index scores. However, the KL classification system suffers from several drawbacks. It is highly subjective in nature and mixes multiple pathologies (JSN and osteophytosis) into one single scale. Moreover, it is less sensitive to the linear progression of the disease pathology and hence, we did not use the KL grading in our study. Medial tibiofemoral JSW was found to have a significant association with the patient's clinical symptoms as well as the Ahlbäck grade. This observation was irrespective of the type of view taken.
While several techniques have been described to quantitatively measure knee JSW from digital radiographs, both accuracy and reproducibility of the method depend on the quality of the radiographic procedure performed as well as positioning of the joint.16,25 Carrying out X rays of the knee with the patient standing on the homolateral foot has been shown to make the technique more sensitive to JSN. 10 The same also holds true for radiographs taken in various degrees of knee flexion such as – AP view with the knees in 30 degrees flexion and X ray beam parallel to the tibial plateau, 26 PA view with 45 degrees knee flexion and beam angled 10 degrees caudally 27 and finally, PA view with knees in 20–30 degrees flexion (LS view). 19 According to Conrozier et al., 16 correct radiographic assessment of the knee must fulfil two conditions. First, good superimposition of serial radiographs must be achieved by standardizing the knee position and the direction of X ray beam. Secondly, a good alignment of the anterior and posterior margins of the tibial plateau must be achieved. In our study, all radiographs with more than 1 mm difference between the anterior and posterior rims of the tibial plateau were excluded from analysis.
Our study demonstrated that both AP and the LS views had a relatively good intra-observer as well as inter-observer reproducibility (the respective ICC values being 0.97 and 0.91/0.92). However, this was less than that reported by Merle-Vincent et al. 18 (ICC = 0.99), Vignon et al. 19 (ICC = 0.98) and Le Graverand et al. 28 (ICC = 0.99). Also, in our study the reproducibility was assessed by repeated measurements of the JSW in the same image rather than the same joint. For precise determination of the extent of JSN, serial evaluation of the knee is needed. As such, the JSN noted may vary due to differences in positioning as well as radiographic procedure. 19
The superiority of the LS over the conventional standing AP view, to detect early OA changes, especially lateral compartment OA, is well documented in literature.18,29 However, no study has compared the degree of correlation of the measurements (taken in both views) with the corresponding knee function score (KSS-F). Our results showed that AP view measurements had a higher degree of corelation not only with the patient's KSS-F but also with the Ahlbäck grade, than those obtained on the Schuss view radiographs. This finding clearly suggests that while AP view of the knee may not be as accurate as the LS view for detecting OA changes in the lateral compartment, nevertheless, it still retains significant utility for estimating the progression of the disease pathology both clinically and radiologically. Moreover, Schuss views are fluoroscopically assisted views and hence are associated with a higher dose of radiation exposure. They are more cumbersome, time consuming and may not be available at all centres. 29
There were a few limitations in our study. One was the cross-sectional method which is not the ideal study design. The second limitation was the small sample size. Future trends call for studies with a better design and a larger cohort to compare the two views and draw a definite conclusion.
Conclusion
Weight bearing/standing AP view radiographs is one of the most commonly performed investigations for OA knee to assess the severity and progression of the disease. While flexion views may help in detecting early OA changes in the lateral tibiofemoral compartment, the AP view still has a better correlation with the patient's clinical symptoms and radiological grading.
Supplemental Material
sj-xlsx-1-otr-10.1177_22104917221080561 - Supplemental material for Correlation of tibiofemoral joint-space width with the clinico-radiological scoring of knee osteoarthritis – a comparison between anteroposterior and lyon-schuss radiographic views
Supplemental material, sj-xlsx-1-otr-10.1177_22104917221080561 for Correlation of tibiofemoral joint-space width with the clinico-radiological scoring of knee osteoarthritis – a comparison between anteroposterior and lyon-schuss radiographic views by Divesh Jalan, Akshat Gupta, Pushpinder Khera, Suvinay Saxena, Deepak Maley and Abhay Elhence in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgements
The authors wish to acknowledge and thank all the patients for giving them permission to publish their clinical data
Declaration of conflicting interests
The Author(s) declare(s) that there is no conflict of interest
Source of funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.