
Abstract
Purpose:
To compare patient subjective satisfaction between medial opening-wedge high tibial osteotomy (HTO) and total knee arthroplasty (TKA).
Methods:
This study enrolled 110 knees, including comprising 49 knees in the HTO group, and 61 knees in the TKA group. We assessed the overall satisfaction using a three-point questionnaire. The satisfaction questionnaire included three questions: (1) How satisfied are you with the results of your knee surgery? (2) How satisfied are you with your most recent knee surgery for reducing your pain? and (3) How satisfied are you with your most recent knee surgery for improving your ability to perform functions? Furthermore, we assessed knee pain and function by using the Knee Society Function Score (KSS) and Knee Injury and Osteoarthritis Outcome Score (KOOS) systems.
Results:
Overall, 93.8% of patients from the HTO group and 95.1% from the TKA group indicated subjective satisfaction (very satisfied and satisfied) with their surgeries. For pain relief, the HTO group showed significantly better outcomes for overall satisfaction (p = 0.04 in walking on a flat surface and p = 0.02 in going upstairs or downstairs). For restored function, the HTO group scored significantly better on ascending stairs than the TKA group (p = 0.007). Functional outcomes using the KSS scoring system did not show significant differences between the two groups. The KOOS pain score was significantly higher in the TKA group (89.9 ± 6.4) than in the HTO group (80.3 ± 12.5).
Conclusion:
HTO and TKA have comparable outcomes with respect to overall patient satisfaction.
Level of evidence:
Level III, therapeutic case series.
Keywords
Introduction
Total knee arthroplasty (TKA) and medial opening-wedge high tibial osteotomy (HTO) are established procedures and are reliable treatment options for end-stage knee osteoarthritis (OA). 1,2 HTO helps by halting the destructive changes of the medial compartment. HTO has several advantages over TKA, including minimal invasiveness, lower blood loss, preservation of joint, and nearly normal kinematics of the knee joint. 3,4 Despite these strengths, TKA is considered the gold standard of operative treatment for OA of the knee, although it is limited to unicompartment. 5 This is due to the superior long-term survivorship and lower risk of revision rate for TKA compared to HTO. 6 –8 However, several studies have shown excellent long-term survivorship and similar revision rates for HTO compared to TKA. 3,9 Consequently, controversy exists regarding the best treatment option between TKA and HTO for patients with end-stage unicompartmental knee OA.
Patient satisfaction is an important outcome because discrepancy is well-documented between clinician and patient ratings of mental and physical health statuses. A recent report investigating patient-reported outcomes after TKA indicated that patient satisfaction levels for TKA were between 80% and 90% in patients. 10 –19 The risk factors for poor subjective outcomes include patient age, severity of arthritis, comorbidities, pain profile, psychological status, expectations, and joint laxity. 14,20 –23
On the other hand, a variety of studies have shown outcomes and related factors following HTO. 24 –27 Most previous studies have used radiologic results, clinical scores, survivorship, or complications to assess the outcomes. However, there is scant published information regarding a patient’s subjective and self-reported satisfaction following HTO. Because of the well-documented discrepancies between clinicians’ and patients’ health status ratings, patients’ subjective satisfaction could be an important outcome measure. 28,29 Patients’ opinions and sense of satisfaction regarding their HTO results are important and should be considered in evaluation studies. 4
We hypothesized that medial opening-wedge HTO is as good as the TKA in terms of achieving patient satisfaction. In this study, we assessed patients’ subjective satisfaction (outcome reported by patients) following medial opening-wedge HTO compared with that following TKA.
Materials and methods
Participants
Patients who visited our hospital for scheduled postoperative follow-up from October 2016 to September 2017 and who consented to participate were enrolled in this study. Enrolled subjects included adults (age, 47–87 years) who were scheduled for primary TKA or medial opening-wedge HTO, which was performed by two experienced surgeons at a single center. The preoperative diagnosis was OA or idiopathic osteonecrosis of the knee. All patients were received the operation more than a year ago. Patients with a history of arthroplasty, severe extra-articular deformity, rheumatoid arthritis, inflammatory disease, or fractures around the knee were excluded; 15 patients were thus excluded from this study. The study was approved by the institutional review board of the author’s institution, and informed consent was obtained from all participants.
Surgical procedures
Medial opening-wedge HTO
During conventional preoperative planning, using the method by Miniaci et al., 30 the valgus correction angle and the distance between the upper and lower edges of the opened posteromedial osteotomy site were measured on the radiograph for prediction. The aim was to obtain a mechanical axis of the lower extremity (Mikulicz line) that passes through Fujisawa point (a point at 62.5% of the tibial plateau from the medial edge). 31 All procedures were performed following the previously reported procedure. 32 Briefly, a longitudinal skin incision, approximately 6 cm in length, was made over the pes anserinus insertion at the anteromedial aspect of the tibia. The medial aspect of the proximal tibia was exposed. Then, two Kirschner wires, 2.0 mm in diameter, were inserted into the tibia as an osteotomy guide under an image intensifier, and biplane osteotomy was performed. With the help of an image intensifier, the osteotomy line was gradually opened, and two b-tricalcium phosphate wedges (OSferion60; Olympus Terumo Biomaterials, Tokyo, Japan) were trimmed to the size of the opening gap during surgery. The wedges were then inserted into the osteotomy gap horizontally. The medial osteotomy site was then rigidly fixed using a TOMOFIX Osteotomy system (DePuy Synthes Japan, Yokyo, Japan) or Tris Plate system (Olympus Terumo Biomaterials, Tokyo, Japan) over the osteotomy site.
Total knee arthroplasty
To stabilize positioning during surgery, patients were restrained against the operating table using surgical tape. All TKA procedures were performed as previously described 33 through a midline skin incision measuring 12–14 cm in length under general anesthesia. The knee joint was exposed using a medial parapatellar approach, and the anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) were resected. A distal femoral cut was performed, followed by a gap balancing procedure to determine the rotation of the femoral component, which balances the tension among the soft tissues of the knee. The tibial and femoral components were then implanted with cement. Vanguard RP (Zimmer Biomet Japan, Tokyo, Japan) was used in all patients.
Outcome measures
We assessed overall satisfaction, using the questionnaire as previously reported. 11 The satisfaction questionnaire included three questions: (1) Overall, how satisfied are you with the results of your knee surgery? (2) How satisfied are you with your most recent knee surgery for reducing your pain (walking on a flat surface, going upstairs or downstairs, sitting or lying down)? (3) How satisfied are you with your most recent knee surgery for improving your ability to perform five functions (going upstairs, getting in/out of a car or on/off a bus, rising from bed, lying in bed, performing light domestic duties) 34 ? Patients were asked to grade their level of satisfaction for each question on a scale of 1–5 points (i.e. Very dissatisfied (1 point), Dissatisfied (2 points), Neutral (3 points), Satisfied (4 points), or Very satisfied (5 points)).
Furthermore, we assessed knee pain and function by using the Knee Society Score (KSS) 35 and the Knee Injury and Osteoarthritis Outcome Score (KOOS). KOOS is a self-reported questionnaire with 42 items in 5 separately analyzed subscales of patient’s pain (including frequency); symptoms (including stiffness, swelling, and clicking); activities of daily living (ADL) for physical function, sport, and recreation function; and knee-related quality of life (QOL). 36,37 Standardized answer options were given, and each question was assigned a score ranging from 0 to 4. A normalized score (100, indicating no symptoms) was calculated for each subscale. A separate score was then calculated and normalized for each of the 5 subscales, on a scale of 0 to 100.
Statistical analysis
Differences between the TKA and HTO groups were compared using the Mann–Whitney U test for quantitative data and the χ 2 test for qualitative data. All statistical analyses were performed using Prism 5.0 software (GraphPad, La Jolla, California, USA), with a p value < 0.05 regarded as indicating significance.
Results
This study enrolled 110 knees, including 49 knees (from 6 male and 43 female patients) in the HTO group and 61 knees (from 6 male and 55 female patients) in the TKA group. The breakup of the preoperative diagnosis was as follows: 37 cases of OA and 12 cases of osteonecrosis in the HTO group, and 58 instances of OA and 3 cases of osteonecrosis in the TKA group. The mean follow-up period for the assessment was 2.8 years (range, 1–5.5 years) in the HTO group and 3.8 years (range, 1–7.5 years) in the TKA group. The mean range of motion and mean KSS functional score at assessment were 132.3 ± 11.3 and 97.0 ± 4.1 in the HTO group and 132.3 ± 11.3 and 97.0 ± 4.1 in the TKA group, respectively (Table 1). There were no complications including infections, fractures, and no revisions in both groups.
The preoperative patient characteristics.

HTO: high tibial osteotomy; TKA: total knee arthroplasty; OA: osteoarthritis; ROM: range of motion.
*p<0.05.
Overall satisfaction, which was used as a proxy for the satisfaction outcome, revealed that 57.1% (N = 28) of patients claimed that they were very satisfied and 36.7% (N = 18) were satisfied in the HTO group, whereas 41.0% (N = 25) were very satisfied and 54.1% (N = 33) were satisfied in the TKA group. A total of 6.1% (N = 3) were neutral in the HTO group, whereas 5.1% (N = 3) were neutral in the TKA group (Figure 1). There were no dissatisfied or very dissatisfied instances in either of the two groups. There were no significant differences between the two groups.

Overall satisfaction outcomes in HTO and TKA groups. HTO: high tibial osteotomy; TKA: total knee arthroplasty.
For pain relief, which was used as a proxy for the satisfaction outcome, 71.4% (N = 35) were very satisfied with their ability to walk on a flat surface in the HTO group, while 49.2% (N = 30) were very satisfied in the TKA group. A total of 57.1% (N = 28) were very satisfied with their ability to go upstairs or downstairs in the HTO group, while 32.8% (N = 20) represented that functionality in the TKA group. For pain relief with sitting or lying, 51.0% (N = 25) were very satisfied in the HTO group, while it was 19.7% (N = 12) in the TKA group. Overall pain relief satisfaction in walking on a flat surface and going upstairs or downstairs were significantly better outcomes in the HTO group than in the TKA group (p = 0.04 in walking on a flat surface and p = 0.02 in going upstairs or downstairs (Figure 2)).
For restored function, the HTO group was significantly better with ascending stairs compared to the TKA group (p = 0.007). A total of 51.0% (N = 25) were very satisfied with their restored function to ascend stairs in the HTO group, while 27.9% (N = 19) were very satisfied in the TKA group. A total of 10.3% (N = 5) in the HTO group and 16.8% (N = 10) in the TKA group were very dissatisfied, dissatisfied, or neutral with regard to ascending stairs. Nearly 90% of the patients were satisfied or very satisfied with getting in or out of cars (89.8% in the HTO group and 89.1% in the TKA group). In the activities of rising from a bed, lying in a bed, and performing light domestic duties, over 80% of patients were satisfied or very satisfied in both groups. There were no significant differences between the two groups (Figure 2).

Satisfaction after HTO or TKA, assessed by overall satisfaction and satisfaction with pain relief and ADL. HTO: high tibial osteotomy; TKA: total knee arthroplasty; ADL: activities of daily living.
Functional outcomes using the KSS score did not reveal significant differences between the two groups (97.0 ± 4.1 in the HTO group and 95.9 ± 6.4 in the TKA group). The KOOS pain score was significantly higher in the TKA group (89.9 ± 6.4) compared to the HTO group (80.3 ± 12.5). Additionally, the KOOS symptom score was significantly better in the TKA group (87.5 ± 11.3) compared to the HTO group (80.0 ± 15.1). There were no significant differences in KOOS QOL, sports activity, and ADL scores between the two groups (KOOS QOL: 62.5 ± 16.1 vs. 66.9 ± 23.9 in the HTO and TKA groups, respectively; KOOS sports activity: 47.1 ± 24.7 vs. 42.6 ± 31.8 in the HTO and TKA groups, respectively; KOOS ADL: 87.2 ± 8.2 vs. 83.5 ± 13.5 in the HTO and TKA groups, respectively; Figure 3).
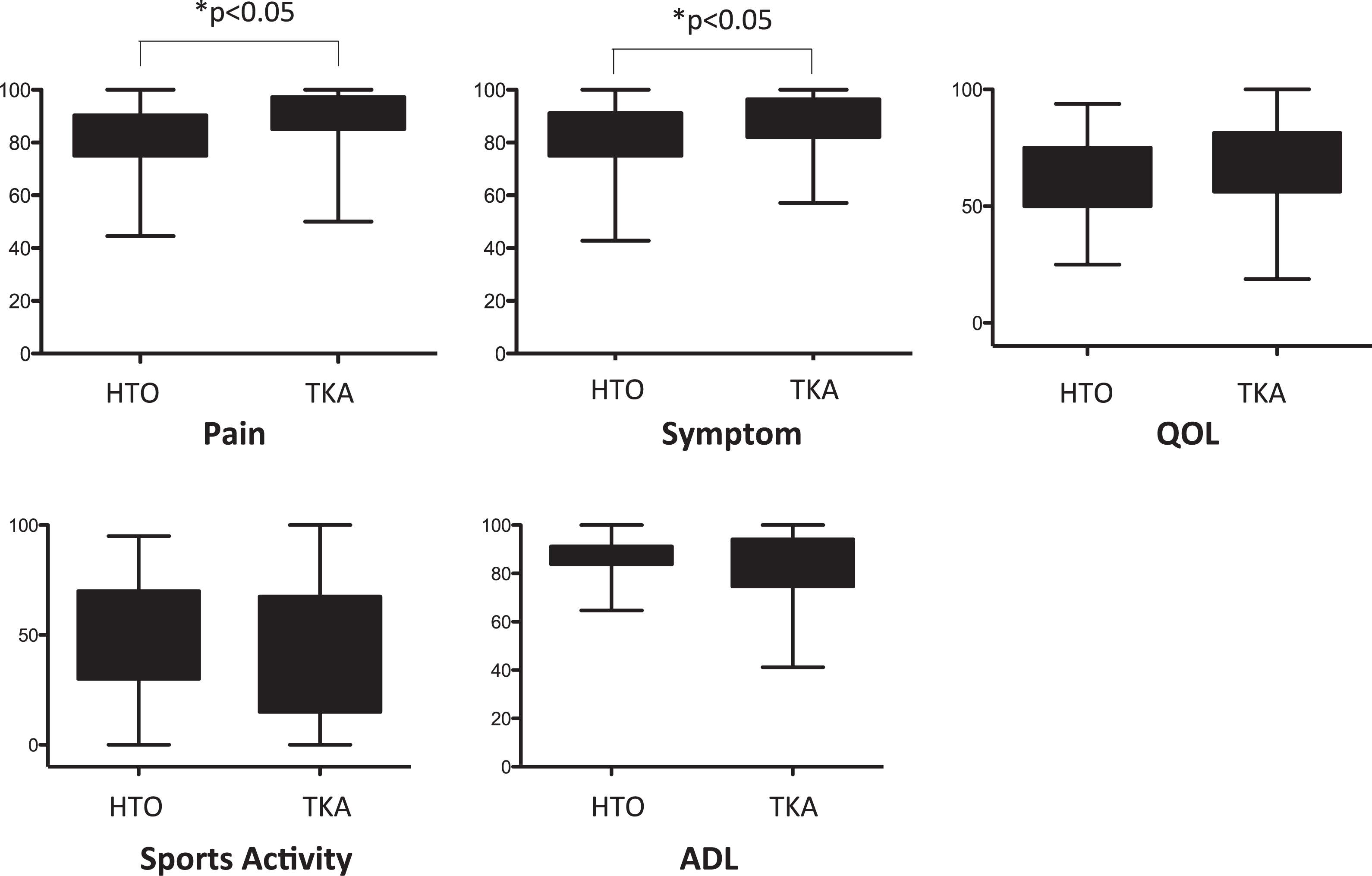
KOOS pain, symptom, QOL, sports activity, and ADL scores in HTO and TKA groups. KOOS: Knee Injury and Osteoarthritis Outcome Score; QOL: quality of life; ADL: activities of daily living; HTO: high tibial osteotomy; TKA: total knee arthroplasty.
Discussion
The most important finding of this study was that over 90% of the patients were satisfied with their HTO and TKA, which coincided with better objective clinical outcomes over a final follow-up period. Overall, 93.8% of the enrolled patients in the HTO group and 95.1% in the TKA group showed subjective satisfaction with their surgeries. This overall satisfaction indicates that HTO is as satisfactory a surgical procedure as TKA is for patients.
TKA and HTO are well-established surgical procedures. There is a well-documented discrepancy between the patients’ and surgeons’ perception on the success of each type of surgery. Various factors may influence the patients’ level of satisfaction. These include physical, psychological, and socioeconomic factors. Patient satisfaction is the main priority in these procedures because the main aim is to improve the QOL for the patients. As a result, patient-derived outcome scales have become increasingly important. 11 Numerous studies indicate that patient satisfaction after TKA is between 80% and 90%. 10 –19 There have been several studies regarding postoperative satisfaction after HTO, showing consistently relatively high satisfaction ratings. 32,38 –43 However, these previous studies for the most part only estimated overall satisfactory outcomes using a simple satisfaction index, without further comparison with other surgical procedures, including TKA. In the case of HTO, Miller et al. 42 demonstrated that the mean satisfaction score was 7.6 of 10 and that there was a positive correlation observed between the satisfaction score and the objective Lysholm score after medial openeing-wedge HTO (MOWHTO) using an external fixator and Puddu plate. Schallberger et al. 40 reported that the median satisfaction index was 80% after opening- and closing-wedge osteotomies without a statistically significant difference between the two surgical methods. In this study, overall satisfaction (very satisfied and satisfied) was 93.8% with HTO and 95.1% with TKA, without statistically significant differences. These results were comparable with previous reports and indicate that these two procedures could provide a relatively high rate of satisfaction.
In this study, KOOS pain and symptom score was significantly better with TKA compared to HTO. There have been several studies until now that have evaluated postoperative outcomes after HTO by KOOS score. Hohloch et al. 44 evaluated the effect of the size of axis correction on functional outcomes in patients undergoing a valgus HTO by KOOS score. They described that the KOOS pain score ranged from 72 to 83 and that the pain score depended on the extent of axis correction. Petersen and Metzlaff 45 also reported the comparison of clinical results by KOOS score after open-wedge HTO and medial unicondylar arthroplasty (UKA) in patients aged between 55 and 65. They described that KOOS pain, symptoms, and QOL scores were significantly better in the UKA group compared to the HTO group. In this study, the KOOS pain and symptom score showed significantly better results in the TKA group, indicating that pain relief or improvement of symptoms may be superior with TKA compared to HTO.
One of the interesting points in this study was that pain relief satisfaction was significantly higher in the HTO group compared to the TKA group, especially when walking on a flat surface and going upstairs or downstairs. Taken into consideration the results of KOOS, patients who were treated with HTO felt some pain during daily activities, but pain relief satisfaction, especially with walking on a flat surface and going upstairs or downstairs is high. HTO is a realignment procedure that aims to transfer the weight-bearing load from the affected compartment to a relatively intact compartment of the knee. HTO retains almost normal kinematics of the knee joint, but TKA does not. Bourne et al. 11 reported that patient satisfaction was relatively low when going upstairs or downstairs in the TKA group. This may be due to the ACL and/or the PCL deficiency in TKA which thereby affects the patient satisfaction.
This study has several limitations. First, this study has a selection bias. We usually recommended HTO, and not TKA, to more active patients; patients of the HTO group were younger and had better functional knee joints. This aspect may affect the results. Second, we investigated and analyzed postoperative outcomes only from the population of a single Asian country. Patient activities and expectations after their surgeries may differ from country to country. Thus, a study with patients from different countries could suggest findings that are more generalized. Furthermore, this study was not of a prospective design. Higher levels of evidence can be expected in this type of study by prospective and age-matched randomized trials.
In conclusion, the overall patient subjective satisfaction outcome following either the medial opening-wedge HTO or TKA was comparable, with relatively high satisfaction for patients. Pain relief in the TKA group was superior to the HTO group, but patient satisfaction was opposite. Thus, the characteristics of satisfaction were different between both procedures, and this aspect may provide the useful information to consider the operation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.