
Abstract
Synovial Chondromatosis is a rare disease of the synovial membrane characterised by formation of multiple loose bodies in a joint. Knee is the most common joint to be affected by this disease. Though, this disease can be managed by synovectomy and removal of loose bodies with a favourable functional outcome but in some cases where there is damage of articular cartilage, simple synovectomy might not be sufficient. Here, we present a case of right knee pain in a 53 year old male since 4 years with a established diagnosis of synovial chondromatosis. No other joint was affected. Pain was associated with a fixed flexion deformity and restriction of knee range of motion and multiple slipping bodies. Radiography showed multiple loose bodies in the tibio-femoral as well as in patello femoral compartment. MRI of knee revealed several damaged areas in the knee articular surface. As a result, decision was taken to perform total knee arthroplasty. Intraoperatively all the loose bodies were removed along with the affected synovium and arthroplasty was done. Patient was discharged in fourth post operative day with proper instructions and was called for follow up at 1 month, 3 month, 6 month, 1 year. Functional outcome was assessed by Tegner Lysholm knee score, Knee Society score and Visual Assessment Scale.
Introduction
Synovial Chondromatosis is a rare and benign disorder of the synovium layer. In this disease, metaplasia of the synovium leads to the formation of loose bodies. It may be primary or secondary to several conditions like osteoarthritis, osteochondritis dessicans, Charcot joint or advanced neuropathy. 1,2 The exact incidence is unknown but it is reported to occur in 1.8 people per milion. 3 This disease occurs in the third to sixth decade of life in diarthrodial weight bearing joints. It is reported that males have a 2:1 preponderance compared to female. 1,3,4 –7 The knee is most commonly affected followed by hip, shoulder, elbow, ankle, wrist. 3,8– 10 Synovial Chondromatosis has also been reported to occur in the intervertebral disc, temporomandibular junction, and several tenosynovial locations. Patients may be asymptomatic but if symptomatic, present with decreased range of motion, swelling, recurrent effusions, pain, crepitus, or locking. 4,8 Management include either open or closed synovectomy with loose body removal. 4,9 In cases when the loose bodies cause damage to the articular cartilage, a more aggressive approach is required like total knee arthroplasty in case of neglected synovial chondromatosis of knee joint with disabling osteoarthritis.
Case report
Here we present a case of a 53 years old male coming with chief complaints of pain and restriction of motion in the right knee for 4 years. Patient was apparently well 7 years back, then he had a trauma to the right knee which was managed conservatively then. Three years later he started having pain the right knee which was insidious in onset, gradually progressive, dull aching in nature, aggravated on movement and relieved on rest and medication and is associated with restriction of movement. Four months back he was treated in another set up where the knee joint was operated and synovial tissue was taken for biopsy which came out to be synovial chondromatosis. He is a known case of uncontrolled diabetes mellitus. He had impeccable family and personal history.
On examination there was diffused swelling over the right knee with a 7 × 2 cm healed surgical scar over the superolateral aspect of the knee. The swelling had a diffused doughy feel with multiple slipping hard loose bodies. He had a fixed flexion deformity of 20 degrees with further active flexion of 50 degrees more. There was no ligamentous laxity of the knee joint.
X rays showed bicompartmental osteoarthritis with multiple loose bodies in the joint capsule. The patient was evaluated from a rheumatological point of view with ESR, CRP, antiCCP, RA factor. All reports came to be within normal limits. MRI was advised in order to assess the status of the articular cartilage which revealed several areas of cartilage erosion (Figure 1).
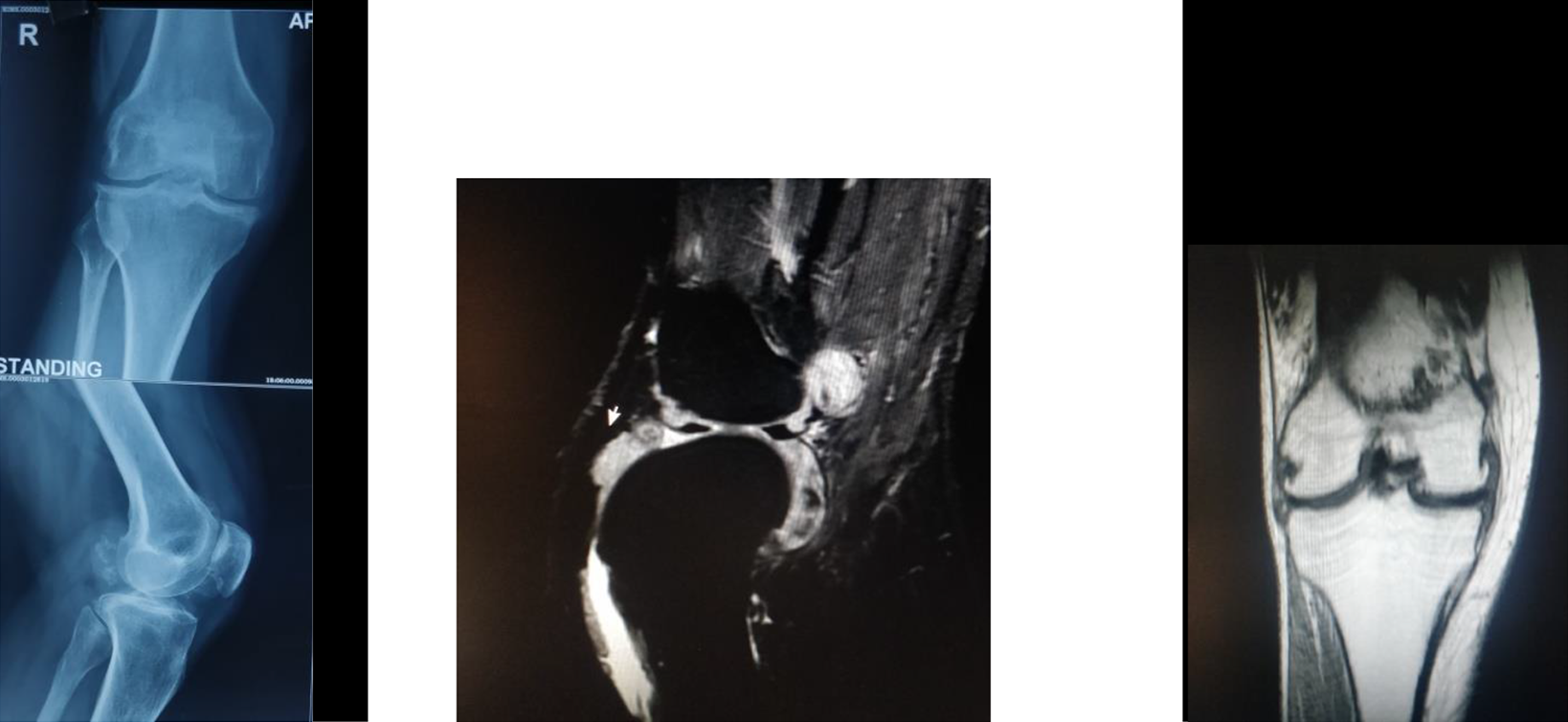
Radiographic features.
Surgical planning was done for removal of all loose bodies along with the affected synovium followed by total knee arthroplasty. Intraoperatively, exposure was done by subvastas approach and patella reteacted. Multiple loose bodies in all the three compartments of the knee joint was seen with inflamed synovium. All the loose bodies were removed and affected synovium was debrided. Tibial, femoral and patellar articular cartilage was removed and total knee arthroplasty done (Figure 2).

Operative finding (loose bodies).
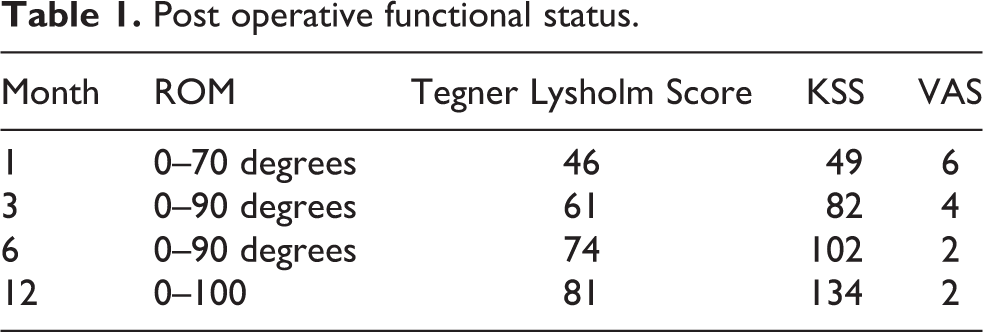
Knee range of motion exercises and full weight bearing started from second post operative day as tolerated by patient. Patient was discharged and followed up at 1,3,6 months and 1 year (Figure 3). Functional assessment was done by means of Tegnar Lysholm score, Knee Scociety score and Visual assessment scale (Table 1).

Post operative follow up.
Post operative functional status.
Discussion
Synovial chondromatosis was first described in 1558 in the knee joint by Pare in and as intraarticular loose bodies arising from sub synovial layer by Laennac. 3 It can also be referred to as synovial osteochondromatosis, Reichel syndrome, synovial chondrometaplesia.
Synovial chondromatosis can be both intraarticular and extraarticular. The foci of synovial chondromatosis start as a sessile attachment in the synovial layer. As they become more pedunculated, they break off and form intraarticular or periarticular loose bodies. 1 Once free they bathe in the synovial fluid, draw nutrition from it and continue to grow. Some of them ossify by endochondral ossification. Loose bodies are generally found in synovium lined areas like joints but some may escape through the joint capsule to reside into the tendon sheath or bursa. 1,4
In 1977 Milgram described three stages of the disease. In the first stage, subsynovial fibroblasts undergo metaplasia and form cartilage nodules in the synovium. Many of these nodules become calcified and undergo endochondral ossification. Ossification of these nodules has led to affection being called synovial chondromatosis. In the second stage, these nodules gradually migrate to the synovial surface and become detached to form loose bodies in the joint. The high concentration of procollagen II C peptide in these cases suggests chondrogenesis. Finally, joint is filled with numerous cartilaginous and osseocartilaginous loose bodies of varying sizes.
Microscopically synovial membrane shows multiple nodules of hyaline cartilage in various stages of calcification and ossification. The chondrocytes often show mild atypia, binucleated chondrocytes and rare mitotic figures.
The clinical picture is due to pressure effect. Synovial chondromatosis is generally insidious in onset and gradually progressive which hinders with its early diagnosis. However, its late diagnosis and neglect may give rise to long term sequelae like irreversible articular cartilage erosion. 4,5
Synovial chondromatosis is usually not prefixed with the word primary, but there is a similar clinical entity of different aetiology and this is commonly termed as ‘Secondary Synovial Chondromatosis’. In many joint diseases like osteoarthritis and osteonecrosis, small fragments of articular cartilage and subchondral bone get detached and may become embedded in the synovial membrane where they stimulate cartilage metaplasia. These metaplastic cartilage nodules are variable in sizes depending largely on the size of the detached cartilage-bone fragment and gradually tend to calcify and ossify and form osteocartilaginous bodies like the ones seen in primary synovial chondromatosis. Histologically, nodules show central nidus of articular cartilage with pale basophilic matrix sometimes along with a fragment of necrotic bone. Metaplastic cartilage is arranged in concentric rings around the nidus because of lamellar growth. Growth in size from further accretion of metaplastic cartilage may continue even when the nodule becomes a loose body in the joint. Secondary synovial chondromatosis is usually seen in older individuals and affects multiple joints. Larger loose bodies can cause locking and pain and need to be removed. In secondary synovial chondromatosis loose bodies are fewer in number, are of different sizes and joint space is reduced. Whereas in synovial chondromatosis (primarily a disease of the synovial membrane), the loose bodies are numerous and of nearly similar size and joint space becomes reduced only after a long standing disease due to the development of secondary degenerative osteoarthritis in the joint.
Radiography is the main modality of diagnosis of Synovial chondromatosis. On x rays, several osteophytic nodules with radio-opaque periphery and radiolucent centre may be seen. But it must be kept in mind that ossification of loose bodies is a time dependent phenomenon. As a result MRI becomes the investigation of choice of synovial chondromatosis where hyperdense shadows in the T2 weighted image can be seen due to high water content of the loose bodies. 4 Ossified loose bodies are hypodense in all sequences and can better be assessed by CT. Moreover, MRI and CT help to assess the condition of joint and articular cartilage.
Management includes removal of loose bodies either by open method or arthroscopically with adjuvant of synovectomy. Though it is Intuitive that synovectomy is required in a synovium based disease but at present, there is very little evidence that synovectomy improves the outcome. 4 The role of synovectomy in conjugation of loose bodies removal is a matter of debate and warrants its own discussion. In case of intractable knee pain due to erosion of articular cartilage there is no other way rather than a total knee arthroplasty along with the removal of all corpora libra to safeguard the prosthesis. Routine check up of the patient should be done in order to evaluate new of growing osteochondromas.
Summary
Synovial chondromatosis is a rare benign disease of synovial membrane, knee being the most affected joint. It may be primary or secondary to various diseases and trauma. Though asymptomatic in most of the cases, it may manifest with pain and joint stiffness in some instances. In this case it presented as right knee pain in a 53 year old male who underwent biopsy of synovium which gave the diagnosis of synovial chondromatosis. He had a fixed flexion deformity of 20 degrees with a motion arch of only 30 degrees. On Imaging, there were multiple loose bodies with inflamed synovium and erosion of articular surface. Patient was managed by removal of all loose bodies and debridement of the affected synovium followed by total knee arthroplasty. Range of motion exercise and weight bearing was started in second post operative day and proper education was given to the patient before discharge. Patient was called for follow up in 1,3,6 and 12 months and functional outcome was assessed by of Tegnar Lysholm score, Knee Scociety score and Visual assessment scale. There was a dramatic relief of pain and range of motion improved in time with gradual improvement in the quality of life as evident from increasing scores.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.