
Abstract
Introduction:
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disorder that involves symmetrical small and large joints. Despite DMARDs, biological agents and anti-inflammatory agents, severe damage to the joint cartilage occurs, mainly due to the growing synovium. Total knee replacement in RA has been an enormous boon to those who are suffering from pain and deformity because of severe restriction of knee joint movement.
Objectives:
To evaluate the clinical, functional and radiological outcomes after TKR for inflammatory arthropathy and to identify potential factors that affect the functional outcome after TKR for Rheumatoid Arthritis.
Materials and Methods:
Patients who underwent total knee arthroplasty for rheumatoid arthritis during the period 2011–2018 were recruited for the study after informed consent. The American Knee Society scores and functional scores were used for the functional outcome and assessment. Preoperative scores were obtained from previous medical records. Paired t test was done to determine the significance in changes between the preoperative and postoperative scores. Bivariate analysis using Spearman correlation and logistic regression analysis was performed to assess the influence of various factors on the postoperative knee scores.
Results:
The average age of patients at the time of TKR was 54 years, all were in stage IV disease, and the majority were women (n = 20). The significant improvement (p = 0.000) was observed between the preoperative (57.3) and postoperative (97.4) Knee Society scores, as well as improvement in functional scores from 36.3 preoperative to 85.2 points postoperatively after TKR. Steroid usage had a significant positive correlation. The duration of disease and involvement of the other joint had a significant negative correlation to postoperative functional scores.
Conclusion:
Total Knee Replacement has been proved as one of the most successful surgical interventions for reducing pain and enhancing physical function in inflammatory arthritis patients.
Introduction
Total Knee Replacement (TKR) is one among the most commonly performed orthopedic surgical procedures, to treat severe arthritis of the knee joint either due to osteoarthritis or due to inflammatory arthropathy. 1 When there is cartilage damage in either medial, lateral compartment or patellofemoral joint, severe pain with deformity develops subsequently necessitating a total joint replacement. When anti-inflammatory medications, lifestyle modification and physiotherapy do not succeed in relieving symptoms of pain and improving functional capacity, joint replacement is considered as the last resort. 2
The prosthesis used in total knee replacement has a very good long-term survival, which depends on the activity level of the patient and the type of prosthesis. Hence, TKR done for symptoms of osteoarthritis, the patients are generally older than the patients who undergo TKR for inflammatory arthropathy.
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory disorder that involves symmetrical small and large joints. If it is not identified early and treated, the damage to the bone and cartilage would become irreversible, leading to severe pain and deformity associated with loss of function. 3 –7 Owing to these reasons, the therapy for rheumatoid arthritis (RA) is mainly focused on restricting the progress of synovitis and the protection of joint from injury. Within 10–20 years of the onset of the disease, despite disease modifying anti rheumatoid drugs (DMARDs), biological agents and anti-inflammatory agents, severe damage to the joint cartilage occurs, mainly due to the growing synovium. 8 Total knee replacement in RA has been an enormous boon to those who are suffering from pain and deformity because of severe restriction of knee joint movement. 9,10 Hence the present study was to assess the clinical, functional and radiological outcome after TKR in inflammatory arthropathy and to identify potential factors that affect the functional outcome after TKR for Rheumatoid Arthritis.
Materials and methods
With a level IV evidence, a retrospective observational cohort study was performed from September 2011 to August 2018 in the department of Orthopaedics, JJM Medical College, Davangere, Karnataka, India. The patients who have undergone TKR for Rheumatoid Arthritis with positive RA factor and patients with seronegative Inflammatory Arthritis of knee were included in the study. The patients who underwent TKR for primary and secondary osteoarthritis of knee were excluded from the study.
All patients with rheumatoid arthritis, who underwent total knee replacement between September 2011 and August 2018, were followed up in out-patient department and assessment of their clinical, functional and radiological outcomes based on American knee society scoring was performed. The telephonic interview were held with eligible patients and were asked to come for follow-up in Ortho OPD in the interval of every 3 months once for 2 years. The functional scoring was assessed using the American Knee Society score. Plain Radiograph of both knees, AP & lateral views were taken before surgery and at the follow-up visit (as shown in Figures 1 and 2) and radiological assessment of the joint was done. Their preop American Knee society and functional score was obtained from patient’s records from the hospital database. Other variables like demography of the patient, BMI, duration of rheumatoid arthritis, intake & duration of medical management with Methotrexate (DMARDS) & steroids and category of patient were also analyzed during the follow-up visit. The final post op measurements were made
Results
A total of 47 total knee replacement has been performed for rheumatoid arthritis in 7 years. Out of 47 cases, the follow-up data of 36 cases are available (26 U/L TKR and 10 B/L TKR). The data of all patients were tabulated and analyzed with IBM SPSS Statistics for Windows, Version 26.0, IBM Corp, Chicago, IL. To compare the improvement between pre and postoperative Knee society and functional scores, paired “t” was used. To determine the correlation between age, BMI, duration of disease, use of methotrexate, use of steroid, with the Knee society and Functional scores, logistic regression analysis was done.
The mean (±SD) age of the cases in our study was 54 ± 11.5 years, the maximum cases were between 51 and 60 years of age. The mean BMI of the cases studied was 27.04 ± 4.02 kg/m2 (2 cases were underweight, 4 were normal, 2 were overweight and 18 were obese). Only 6 cases (27%) were males and 20 cases (73%) were females. Only two male patients had bilateral knee replaced and eight women had bilateral knee replaced.
The relationship of the index knee with the opposite knee and other joints: A total of 13 cases had unilateral knee replacement or both knees were replaced, 14 cases had unilateral TKR, with the opposite symptomatic knee joint and 9 cases had other joints involvement (like hip, shoulder etc.) with deformity requiring arthroplasty.
Duration of the disease prior to the replacement: 13 cases had less than 5 years and 12 cases had 6–10 years of duration of illness prior to the surgery. Eleven cases underwent TKR after 10 years of duration of the disease. At the time of recruitment, the average duration of disease was 8.86 ± 6.25 years. All the patients recruited were in stage IV of the disease. On Radiological examination, none of the patients had evidence of lysis seen in the x-ray.
Usage of Methotrexate: A total of 23 cases required methotrexate preoperatively and 21 cases required methotrexate postoperatively.
Usage of steroids: 15 cases required steroid preoperatively and 11 cases required steroid postoperatively.
The mean (±SD) of Knee society score was 57.3 ± 18.3 preoperatively and 97.4 ± 4.4 postoperatively. The difference in mean (± SD) Knee society score was 40.03 ± 18.45 with a p value of 0.000 which was statistically significant. The mean (± SD) of functional score was 36.3 ± 20.96 preoperatively and 85.28 ± 19.1 postoperatively. The difference in mean (± SD) functional score was 48.88 ± 24.08 with a p value of 0.000 which was statistically significant.
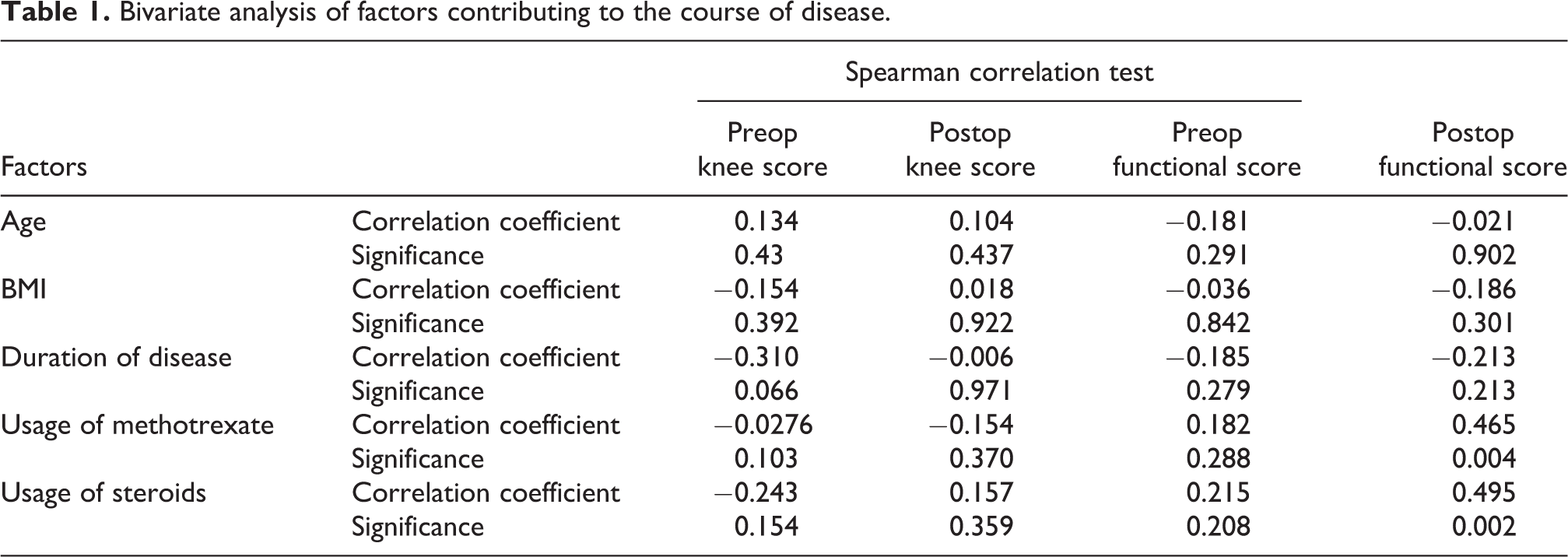
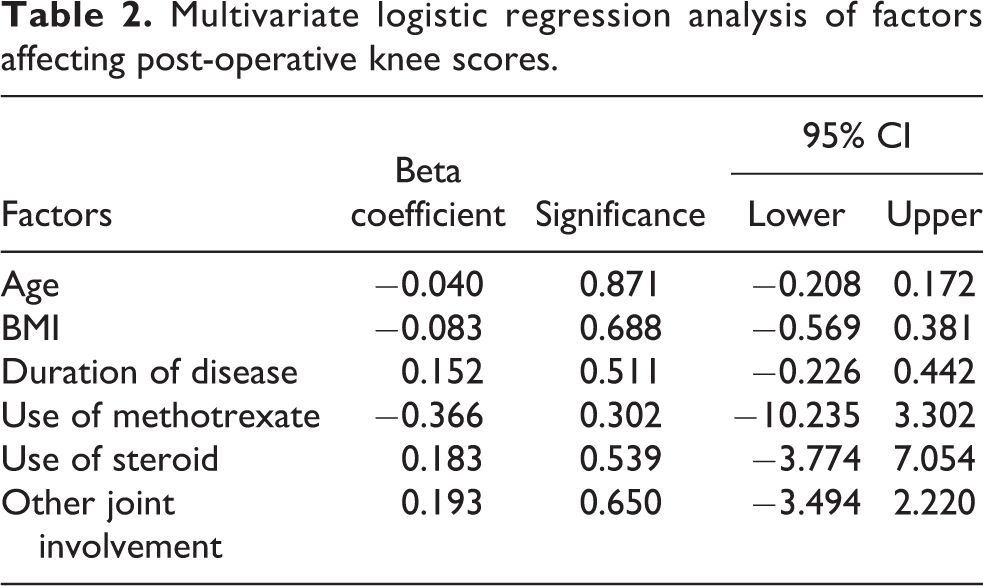
The bivariate analysis of factors contributing to the course of disease were tabulated in Table 1. Factors affecting the postoperative knee score: Factors such as age of the patients recruited, BMI, duration of disease, use of methotrexate, use of steroid and the involvement of other joints showed no effect on the postoperative knee scores by multivariate logistic regression analysis (as shown in Table 2).
Bivariate analysis of factors contributing to the course of disease.
Multivariate logistic regression analysis of factors affecting post-operative knee scores.
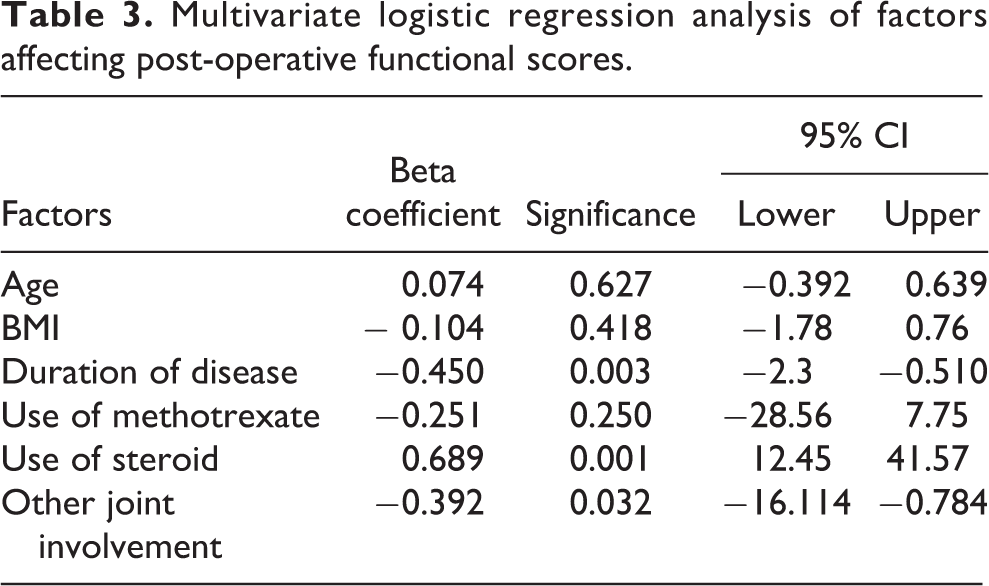
Factors affecting the postoperative functional score
Multivariate logistic regression analysis of factors affecting post-operative functional scores.
Comparison of other similar studies.

Discussion
Out of 47 TKRs performed for rheumatoid arthritis, 36 TKRs could be followed up. The probable explanations are, due to the underlying disease process, these patients are home bound, the address mentioned in the previous medical records mighty be faulty and the domicile of majority of the patients was from far off places.
The average age of the patients was 54 years in our study, which clearly depicts the fact that TKR for RA is performed at a younger age. The average of patients undergoing TKR for osteoarthritis has been quoted as 67 years 11 in one study and 75.1 years 12 in another study. The pathological process affecting the knee starts quite early in Rheumatoid arthritis progressing to more severe stages, requiring arthroplasty at an earlier age than osteoarthritis.
The average age for TKR in RA reported earlier was 43.2 years 13 and 62.8 years 10 in previous literature. The majority (n = 10) of the participants were between 51 and 60 years. There were more number of women (n = 20) than men (n = 8) who underwent TKR for RA. In RA, females are affected three times more often than males. The genetic factors (X linked) and other hormonal factors involved in the pathogenesis of the disease may explain this finding. 14 In earlier literature, among those underwent TKR for RA, 82% were females & 18% were males 10 and 80% were females & 20% were males 15 in another study. Eight out of 20 women in our study, underwent TKR in both knees as compared to only 2 males who underwent bilateral TKR. In osteoarthritis too, rates of TKR are higher for women than men. 12
Duration of RA is an indirect indicator of the severity and stage of the disease. In our study the average duration of disease prior to TKR was 8.86 years. More commonly, patients who are in stages III and IV of RA, who do not have significant improvement in symptoms with medical management (DMARDS, STEROIDS), undergo TKR for the relief of pain and improving their functional status. All the patients recruited for the study were in stage IV of the disease which is characterized by arthritis, painful restricted range of movements, soft tissue contractures and deformity. The average follow-up after the index TKR was 37 months ranging from 3 months to 93 months.
Regarding other joint involvement, around 14 patients had a symptomatic opposite knee which was not replaced yet, 9 patients had other joints involved which will have a bearing on the functional outcome of the patient.
Use of methotrexate: Though perioperative use of immunosuppressant like methotrexate has been associated with poor wound healing, in a recent study, it has not been found to increase the infection rates and it helped in better postoperative recovery with less number of flare ups. 4 In our study, 69% (n = 25 knees) were using methotrexate for the treatment of RA.
Use of steroid: In our study, 15 subjects were using steroids preoperatively and 11 were using postoperatively. Chronic steroid use has been associated with poor wound healing, poor bone quality and secondary osteonecrosis around the TKR site which can be attributed to the disease process also. 8
Knee society scores: There was a significant improvement in the American knee society scores. The average preoperative score was 57.3 points and postoperative score was 97.4 points. There was a 70% improvement in the scores after the TKR. Pain, range of motion and stability of the joint are taken into consideration for assessing the scores and TKR has been found to significantly improve the knee society scoring (p = 0.000).
Functional scores: The average preoperative functional score was 36.3 and postoperative score was 85.2, showing a 130% increase after TKR in RA. Mobility of the patient and the use of aids are taken into consideration. There was a significant improvement in the scores after TKR (p = 0.000).
Factors affecting the preop and postoperative scores
Bivariate analysis with Spearman correlation was performed to find the correlation between the age of the patient, BMI, duration of disease, use of methotrexate and steroid, and the scores. There was no statistical significance observed, on the correlation between the age, BMI, duration of the illness and the scores. However, there was significant positive correlation found between the use of methotrexate (p = 0.004) and postoperative functional scoring. There was also a significant positive correlation observed between the use of steroid (p = 0.002) and postoperative functional scores.
Using logistic regression analysis on the effect of various factors affecting the knee society (post op) and functional scores (post op) was analyzed. Only the use of steroid had a significant (p = 0.001) positive effect on the postoperative functional scores. Duration of the disease (p = 0.003) and the involvement of other joints (p = 0.03) had a significant negative effect on the postoperative functional scoring.
This can be explained by the fact that, longer the disease activity, the more severe and poly articular in nature, which has a bearing on the functional activity of the patient. RA patients have severe impairment of function, are more wheel chair or home bound, more dependent on walking aids due to the progressive inflammatory nature of the disease leading to permanent deformity and disability. There was no significant correlation noticed between age of the patient, BMI, duration of the disease, use of methotrexate, use of steroid, other joint involvement and postoperative knee society scores.
The limitations of the study are small sample size to prove the influence of various patient related factors on the pre and postoperative scores and long-term follow-up regarding the survival of the prosthesis, aseptic loosening, incidence of delayed deep seated infection and need for revision arthroplasty.
Conclusion
Total Knee Replacement has been proved as one of the most successful surgical interventions for reducing pain and enhancing physical function in inflammatory arthritis patients. However, it is crucial to understand the natural course of RA since patients with RA often have combination of medical, anesthetic and musculoskeletal problems when compared to patients with osteoarthritis. Despite such complexities often encountered in RA patients, a well-timed, well executed total knee replacement has been proven to improve overall function and quality of life of patients with disabling RA of the knee.
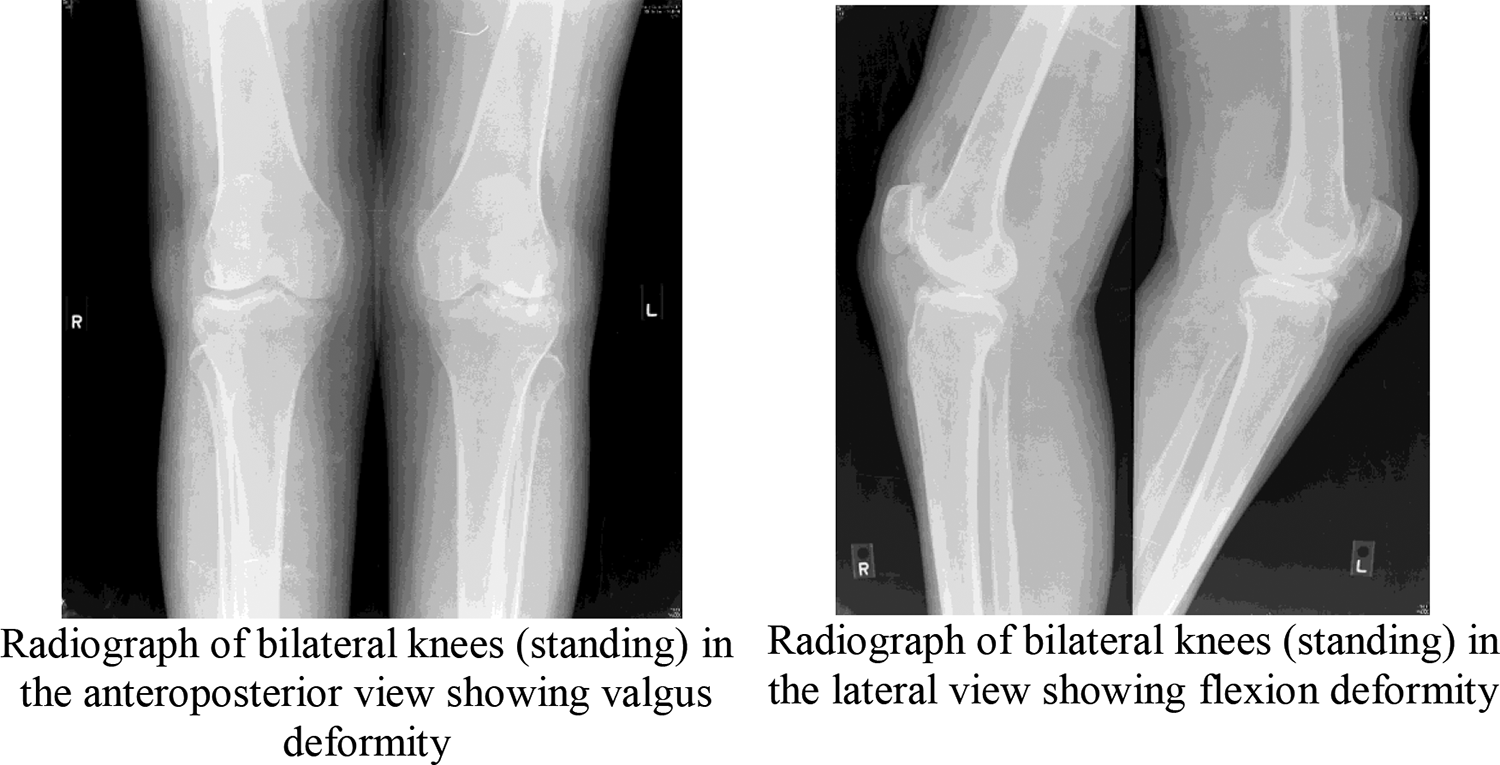
Preoperative images.
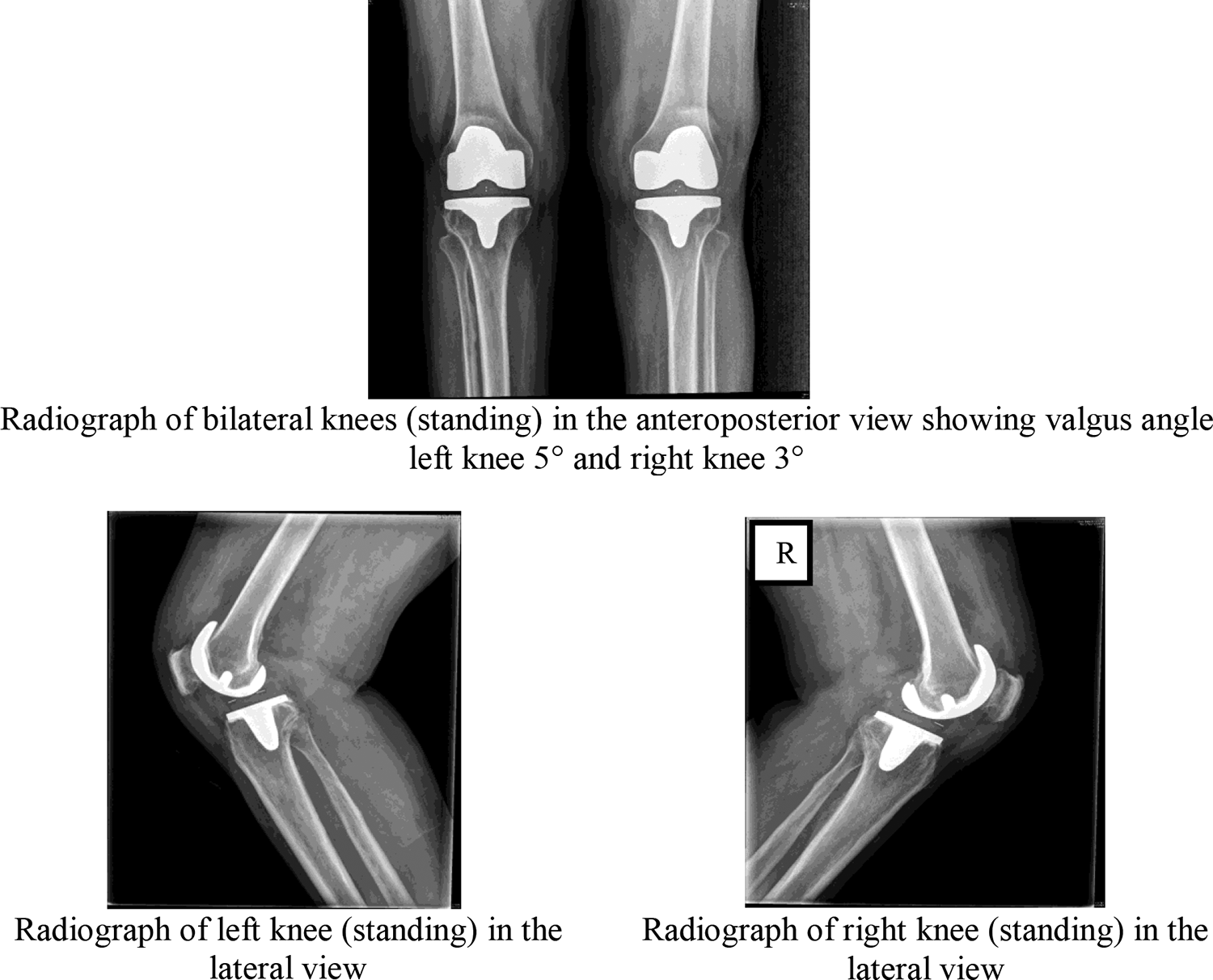
Postoperative images.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.