
Abstract
Background
Unicompartmental knee replacement (UKR) has functional and economic benefits when compared with total knee replacement, however it is technically demanding and may be associated with higher failure rates. The primary aim of this independent series study was to evaluate the survival of lateral UKRs implanted in our institution and their clinical outcomes. The secondary outcome was to compare the results of mobile and fixed-bearing prostheses.
Methods
This is a retrospective series study of 183 cemented lateral UKRs implanted in 170 patients, for advanced isolated lateral compartment arthritis, under the care of two senior surgeons. Fixed or mobile-bearing prostheses were used according to the surgeon's preference. Kaplan Meier analysis was used to evaluate prosthesis survival with the endpoint being revision for any reason. A subgroup analysis of survival was also done for each bearing type. Functional outcomes were evaluated using the Oxford knee score (OKS) at final follow-up.
Results
This series included 103 Fixed-bearing and 80 mobile-bearing prostheses. Median follow-up was 6.9 years. 9 knees required revision. The commonest reason for revision was progression of arthritis to the medial compartment. Dislocation was the commonest cause of revision in the mobile-bearing group. Survival at 10 years was 91.9% with no significant difference (p = 0.083) between bearing types (fixed-bearing 93.8% and mobile-bearing 90.6%). The OKS were comparable in both groups, the mean OKS was 44/48.
Conclusion
Good survival and functional outcomes can be achieved using cemented lateral UKRs with both bearing types. There was a trend towards superior outcomes in the fixed-bearing group.
Introduction
Isolated lateral compartment articular cartilage degeneration is reported to occur in approximately 10% of patients presenting with knee osteoarthritis (OA).1,2 The surgical treatment options for advanced isolated lateral compartment OA with full cartilage loss are usually either total knee replacement (TKR) or unicompartmental knee replacement (UKR). 2 The benefits of UKR include reduced perioperative morbidity, shorter hospital stay, and lower cost.3,4
Lateral UKR provides a significantly superior range of motion (ROM) and may improve patient-reported outcomes compared to TKR. 5 However, it is a technically demanding procedure due to the complex anatomy and function of the lateral compartment as well as its disease pattern. 6 The lateral compartment has different biomechanics than the medial side. It is more mobile in flexion than extension with more roll back and posterior translation of the femur over the tibia.7,8
Partly due to the limited numbers of lateral UKR being performed, there is limited long-term follow-up data from non-designer centres. In the UK National Joint Registry (NJR), lateral UKRs are combined with medial UKRs making outcomes assessment difficult. 9 A recent study using the Dutch arthroplasty register found no significant differences in the revision rate between lateral and medial UKR overall but an increased revision rate of mobile-bearing lateral UKR compared to fixed lateral UKR. 10 This was also concluded in a recent meta-analysis of cohort studies comparing the survivorship of fixed and mobile bearing UKRs reporting significantly higher revision rates for the lateral mobile bearing prosthesis. 11 While another meta-analysis found no considerable differences in the survival of medial and lateral UKAs. 12 Therefore, the primary aim of this independent series study is to evaluate the survival of lateral UKRs implanted in our institution and their clinical outcomes. The secondary outcome is to compare the results of both mobile and fixed bearing types.
Methods
This is a retrospective series study that has been reviewed by the Research and Development department within the trust and was deemed not to require full NHS permissions. All patients that underwent a Lateral UKR from May 2003 to December 2018 under the care of the two senior surgeons (DS) (2003–2011) and (JW) (2008–2018) were included in this series. None of the patients who received a lateral UKR during this time period were excluded from this study. Surgery was performed if standard non-operative management failed to control patients’ symptoms. The indications for surgery were bone on bone lateral compartment OA or osteonecrosis, intact ligaments, functionally preserved medial and patellofemoral articular cartilage, fixed flexion deformity <10 degrees, and knee flexion of more than 90 degrees. The patient's age and body mass index (BMI) were not considered contraindications for prosthesis implantation. Inflammatory arthritis, previous peri-articular osteotomies, or other compartment arthritis were considered contraindications to lateral UKR. Preoperative diagnostic investigations included plain radiographs; weight-bearing PA 30 degrees, lateral, and skyline views. MRI scans were used to confirm appropriate indications if needed.
Fixed or mobile-bearing prostheses were used according to the surgeon's preference. The fixed-bearing implanted between (2003–2015) was Vanguard-M prosthesis (Biomet, Warsaw, Indiana, USA) or the Oxford Fixed Lateral Partial Knee. The mobile-bearing implant used was the Oxford Domed Lateral prosthesis (ZimmerBiomet, Warsaw, Indiana, USA) implanted between (2008–2018). Both prostheses were cemented.
The surgical approach was made through a minimally-invasive lateral parapatellar arthrotomy. The sagittal tibial bone cut was made using a trans-patellar tendon approach in order to achieve accurate rotation of the tibial component. The femoral component was positioned in parallel with an intramedullary alignment rod in the coronal plane and at 90–95 degrees of flexion relative to the femoral axis in the sagittal plane. The technique aims to produce a stable knee in extension, with some laxity in flexion to mimic that of the normal knee. All patients received perioperative prophylactic antibiotics and postoperative prophylactic anticoagulation therapy. All patients received similar post-operative rehabilitation and follow-up protocols. The postoperative follow-up for clinical and radiographic evaluation was arranged at six weeks, one year, and at five years. The electronic records and radiographs of all patients were retrospectively reviewed for any reported reoperations or prosthesis-related complications.
All patients were offered a clinic appointment at their final follow-up to evaluate the outcome of their knee surgery. Patients who did not attend the final follow-up appointment had a virtual clinic via a phone call to check if revision or reoperation surgery was performed and to complete the Oxford knee questionnaires. Patients who died before completing Oxford scores were not included in the functional assessment of this study but were evaluated for implant survivorship. All patients included in the study were cross-checked with the NJR database and their GP practice was contacted to make sure revisions were not done elsewhere and that our results are accurate.
Kaplan Meier analysis was used to evaluate the overall lateral UKR prosthesis survival at 5 and 10 years and also the survival of each bearing type. The endpoint was revision for any reason. Statistical analysis was performed using SPSS software (IBM Corp. IBM SPSS Statistics for Mac, Version 23.0. Armonk, NY: IBM Corp). Revision was considered to be removal or exchange of any implant, Fixed and mobile bearings were compared for functional outcome scores and survival rates.
Patient-reported functional outcomes were evaluated using the Oxford knee questionnaires completed by patients at the final follow-up. The scores were classified into excellent (>41), good (34–41), fair 27–33), and poor (<27) as described by the Oxford group. 13 The Mann-Whitney U test was used to compare the OKS of mobile and fixed bearings with a significance level of p = <0.05.
Results
A total of 183 lateral Oxford UKRs were implanted in 170 patients within the time period. Fixed-bearing implants were performed for 103 knees in 97 patients, while 80 mobile-bearing implants were performed in 73 patients. The mean age of patients at the time of surgery was 67.8 years (range 41–87 years). Median follow-up was 6.9 years (range 1–12.7 years). Death occurred in 47 patients with 51 implanted knees (bilateral n = 4). No deaths were related to the index procedure.
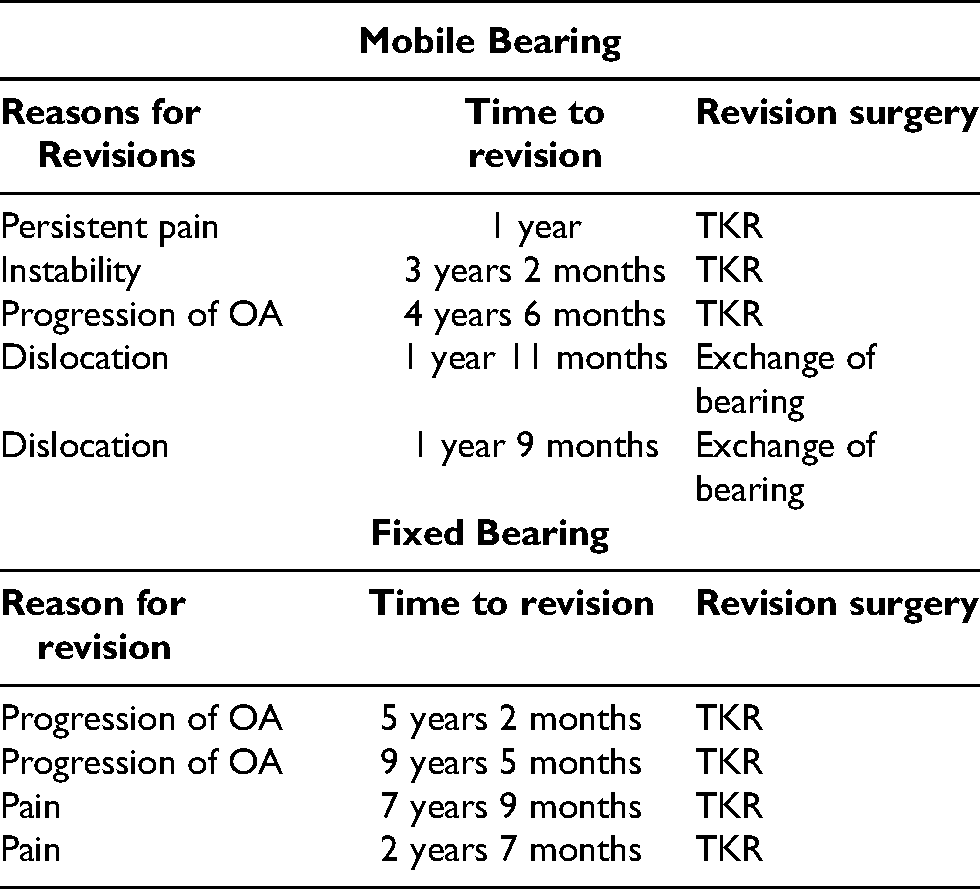
Nine patients underwent revision surgery. The most common reason for revision in all of the cohort was progression of arthritis to the medial compartment. While in the mobile-bearing group, dislocation was the commonest cause for revision by the exchange of bearing. There were 4 revisions to TKR in the fixed-bearing group and 5 revisions in the mobile-bearing group, of these two were bearing dislocations treated by implantation of a bigger bearing, with no further surgical procedures required. The reasons for revision are listed in (Table 1). The Kaplan Meier overall survival rate of the full cohort at five years was 96% (CI: 92–99%) and at ten years 91.9% (CI: 86–98%) (Figure 1).
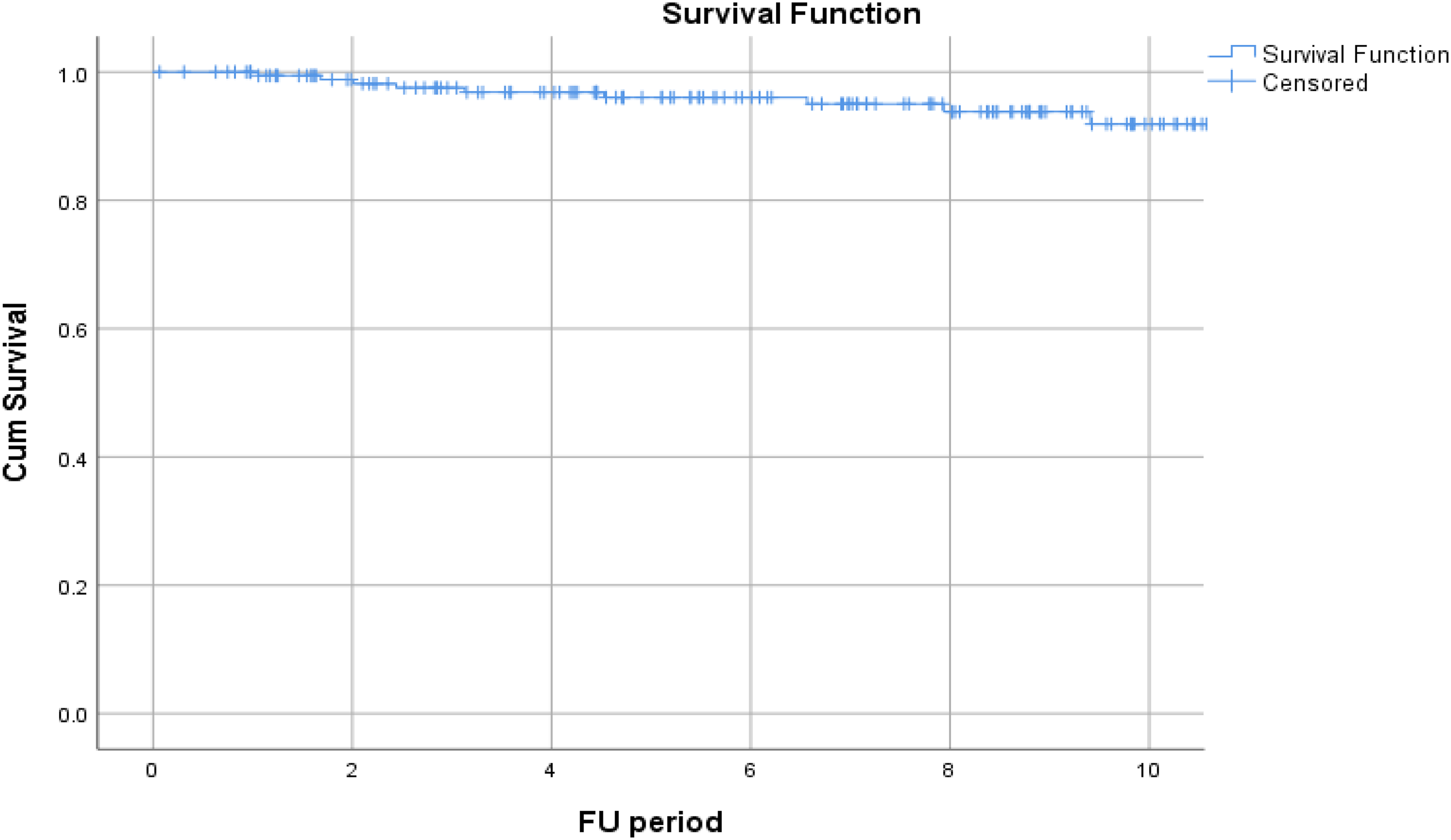
Kaplan-Meier survival analysis for all lateral UKRs (10-yr survival 91.9%).
List of revisions.
The survival rate at 5 years for fixed bearing group was 98.9% (CI:96.9–100%) and at ten years 93.8% (CI:87.7–99.9%). The survival rate at five and ten years for mobile bearing prosthesis was 90.6% (CI:%, 82.42–98.76%).There was no significant difference in outcome between the two groups at five (p = 0.06) and at ten years (p = 0.083), (Figure 2).
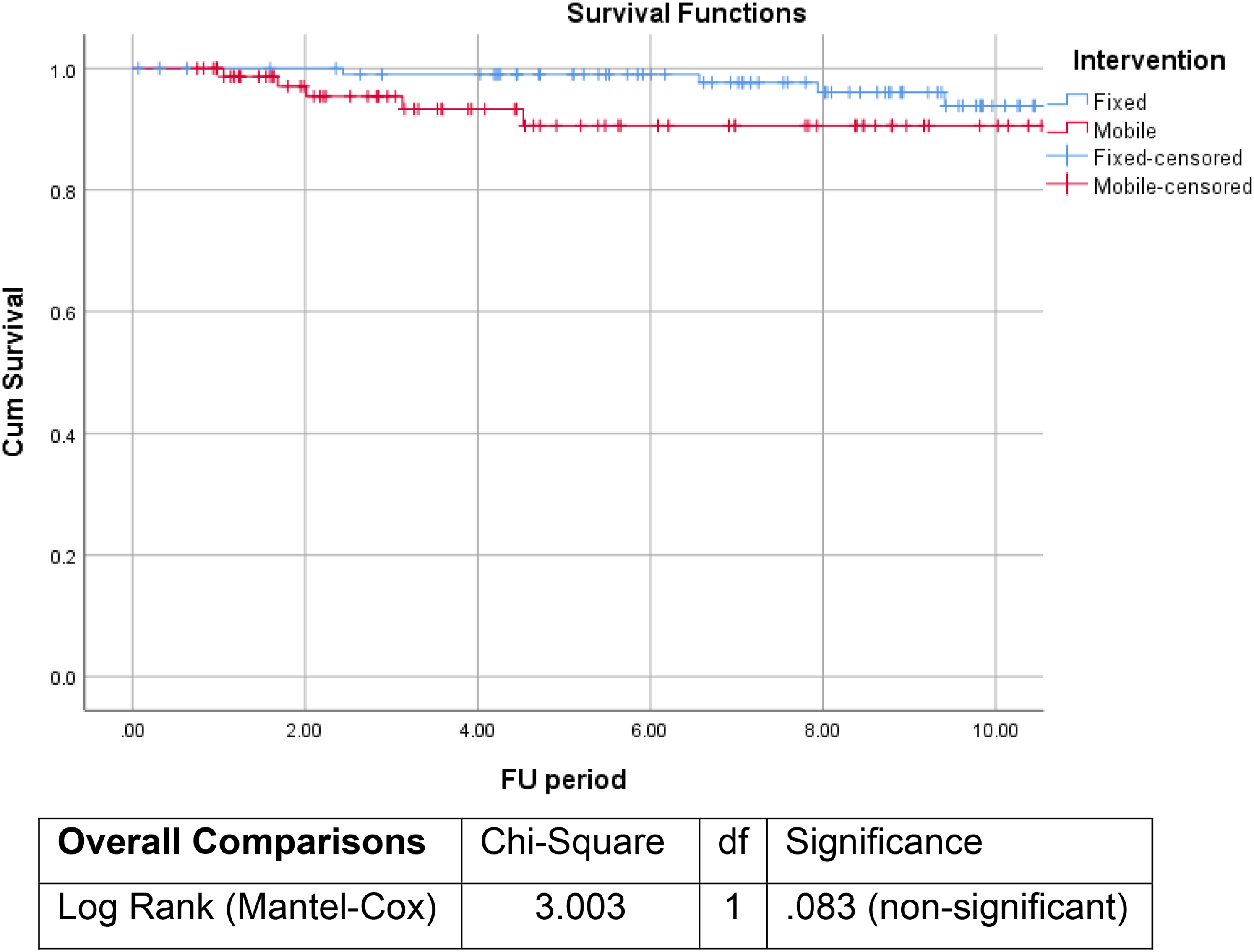
Kaplan Meier 10-year survival analysis for fixed (93.8%) and Mobile bearings (90.6%) prostheses.
One reoperation was required in the mobile-bearing group. A knee arthroscopy was performed at 8 years following index surgery. This patient had developed new onset of gradually progressive knee pain. Arthroscopy revealed scar tissue anteriorly and a medial femoral condyle ulcer. Debridement of scar tissue and chondroplasty of the ulcer were performed with a good outcome. Further surgery has not been required.
Of the full cohort, 84 patients completed OKS at the final follow-up (51 died, 9 were revised, and 39 did not complete the questionnaire). The median Oxford Knee Score for the full cohort at the final follow-up was 44/48 (range 6–48) (Figure 3). Good or Excellent scores were achieved by 85% of patients. The median OKS for patients with mobile bearing implants was 42.5 (range 6–48), while that of the fixed bearing group was 44 (range 18–48), (Figure 4). The statistical analysis using the Mann-Whitney U test to compare the OKS of mobile and fixed bearings was non-significant p-value < .05 (p = 0.14).
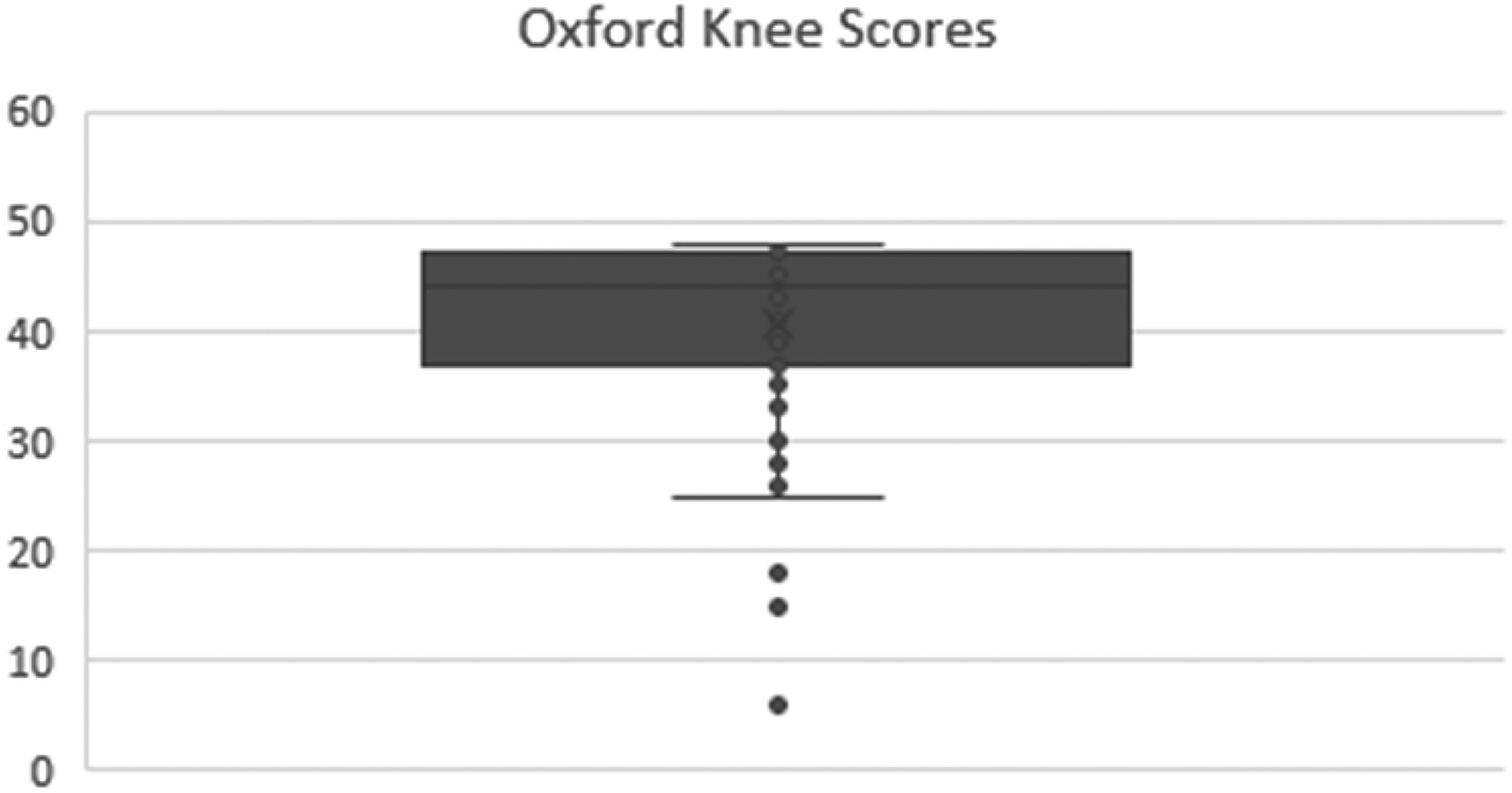
Oxford knee scores for the full cohort.
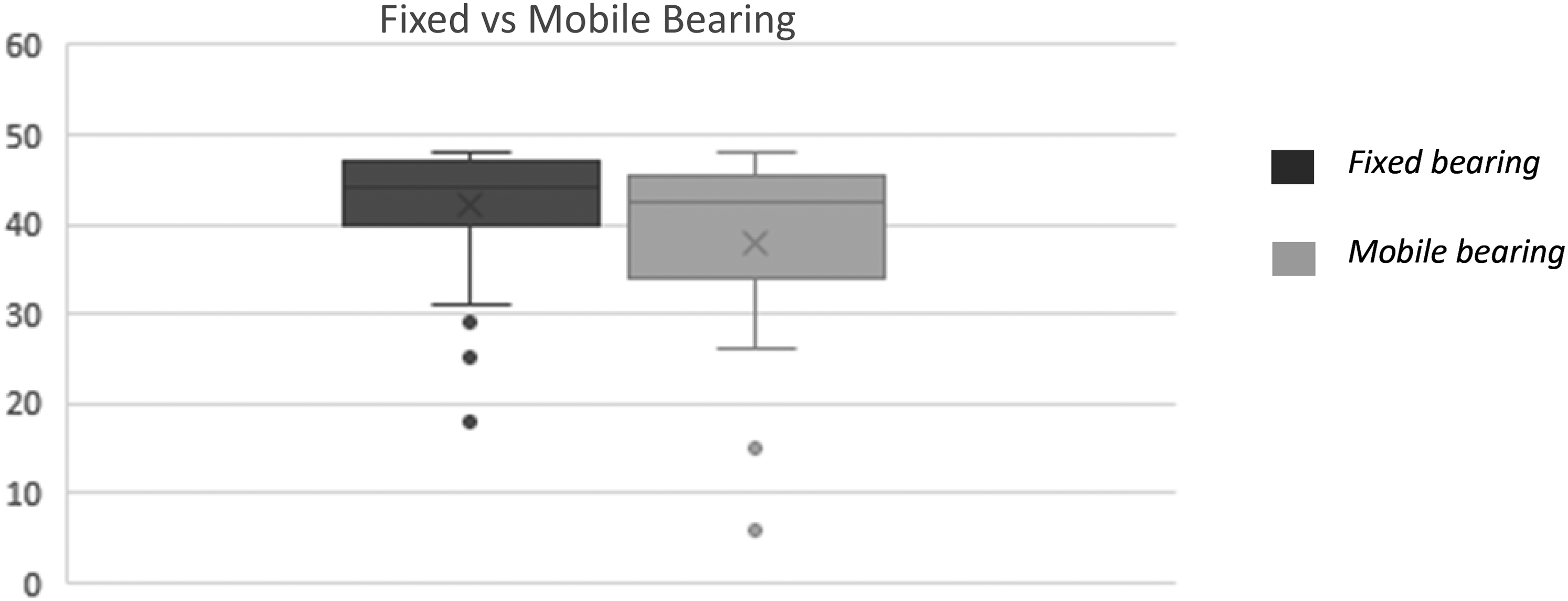
Oxford knee scores, fixed, and mobile bearings.
Discussion
The primary outcome of this study is that lateral UKR has a good survival rate out to ten years. The revision rate in this series is similar to the UK national joint registry for UKR 9 and to the reported survival for the lateral UKR in a recent meta-analysis. 12 These results show that lateral UKR is a reasonable surgical option for patients with isolated lateral compartment arthritis. The overall PROMs scores in this case series are high with nearly two-thirds of patients achieving excellent OKS (41 or above). This is comparable to a large series from the designer centre 14 as well as to the medial UKR and TKR reported in the TOPKAT study. 3
There are fixed and mobile-bearing options available for this procedure. Unacceptably high dislocation rates of 11% were seen when the mobile-bearing medial Oxford UKR (OUKR) was implanted on the lateral side of the joint to treat lateral OA.15,16 A domed lateral OUKR was introduced as well as a modified surgical technique in an attempt to reduce the dislocation rates.16,17 This seems to have been achieved as the designers reported an improved dislocation rate of 1.7% with good functional outcomes. 17 This was backed up by data reported in some independent studies.18,19 However, a large multicentre study from Germany reported higher rates of dislocation of 8.5% at five years for the mobile-bearing domed lateral OUKR and recommended the use of fixed-bearing prosthesis. 20 Furthermore, the designer recently published a large series reporting a dislocation rate of 4% with the use of the mobile bearing prosthesis, most of which occurred in the first year. 14 It therefore clearly remains an issue and although both patients that suffered a dislocation in this series underwent a relatively straightforward procedure with reimplantation of a bearing 1mm thicker, and have required no further surgery, each intervention obviously carries risk.
In a systematic review, 7 the most common reasons for failure in lateral UKR varied between joint registries and cohort studies. In cohort series studies, progression of OA was the most common cause for revision, while registry studies reported aseptic loosening to be the commonest Overall, indications for revision of lateral UKR were progression of OA (29%), aseptic loosening (23%), bearing dislocation (10%), instability (6%), infection (6%), unexplained pain (6), fractures (4%), and wear (2.7%). These results were similar to another systematic review reporting also dislocation of the polyethylene bearing as the commonest cause of early revision and the most common reason for mobile-bearing failure. 21
Overall the most common reason for revision in this series, was progression of OA to the medial compartment. While dislocation was the most common reason for early failure in the mobile-bearing group. These findings are in line with the reasons for failures for partial knee replacements across the registries and studies.7,11,14 It has been proposed that under correction of the valgus deformity in lateral UKR may prevent the risk of progression of OA to the medial compartment 22 and provides better functional outcomes. 23 However, it was found that overcorrection of the deformity during lateral UKR is more common than in medial UKR. 24 This risk of overstuffing the lateral compartment is probably due to the looser structures of the lateral compartment and the varied compartment tension in flexion and extension. It was proposed that overstuffing the lateral compartment may be a risk factor for the dislocation of the mobile bearing. 25 However, the study had low numbers of dislocations available for analysis, and more importantly, they used non-weight-bearing short AP films instead of full lower limb alignment views. In this series, we have successfully treated two bearing dislocation knees by upsizing the bearing. These two knees did not dislocate further which may mean that the primary bearing size was undersized causing the dislocation. The increase of bearing thickness for managing dislocations was also shown in a designer series 26 and other studies. 18 It appears that the bearing dislocation may be caused by under or oversizing of the mobile bearing rendering the margin for error in the mobile-bearing design lower than that of the fixed bearing. This risk for dislocation in the mobile-bearing design may also add uncertainty to mobile-bearing users and may also have a potential tendency for some surgeons to overstuff the compartment in an attempt to reduce this risk. Furthermore, overcorrecting the deformity in the lateral UKR shifts the mechanical axis medially overloading the other un-resurfaced compartment and consequently increasing the risk for progression of OA to the medial compartment. 7
It is potentially advantageous, therefore, to use a fixed-bearing prosthesis to eradicate the risk of dislocation and allow under correction of valgus the deformity more easily to achieve a reduction of the risk of OA progression to the other compartment.
One of the theoretical advantages of mobile-bearing lateral UKR proposed by the designers is the potential for reduced wear rates, by maintaining high levels of congruity and therefore a large contact surface area. 25 However, this was not yet been validated for the lateral UKR. In a recent meta-analysis of cohort studies and joint registries, none of the implanted lateral fixed bearing UKR prosthesis required revision for wear. 11 This is similar to the findings in our study. It may be that survival in the second and third decades after implantation proves this, but as yet it remains an unknown. The use of this prosthesis in younger patients could potentially be justified on that basis.
It has also been proposed that a mobile-bearing prosthesis could potentially maintain more physiological knee kinematics. 16 The design aims to allow the tibial polyethylene bearing to roll back over the posterior part of the tibial baseplate while maintaining congruity, therefore, mimicking what happens in the native knee and allowing the knee to flex almost fully and potentially improve functional outcome. Rollback of the femoral component on a fixed-bearing tibial component could potentially cause high stresses on the polyethylene and impingement leading to reduced flexion, increased wear, and poorer functional outcome. This has not been demonstrated in this series. A meta-analysis also reported no bearing breakage or impingement for the fixed bearing lateral UKR. 11
The Vanguard-M prosthesis consists of a one-piece direct compression moulded tibial component articulating with a standard Oxford Phase 3 femoral component. It was originally designed for use on the medial side of the knee, and therefore had tibial component geometry to match that compartment. A component designed for the medial side of one knee was used as the tibial prosthesis in the lateral compartment of the contralateral knee. Whilst the Vanguard-M prosthesis is no longer commercially available, we believe that the results we have shown should be applicable to the Fixed Lateral Oxford UKR as the manufacturing processes and polyethylene are identical. The shape of the tibial component has been modified such that it much more accurately matches the native tibial shape.
This series shows good outcomes for both fixed and mobile bearing implants with no significant difference in survival or functional scores. However, there was a trend towards superior results for the fixed bearing group with a slightly lower revision rate due to the risk of dislocation associated with the mobile bearing and slightly higher PROMs. None of our patients required revision surgery for wear or loosening in either group. Based on current evidence, it, therefore, seems reasonable to consider fixed-bearing designs safer for the lateral UKR. The use of the mobile bearing Domed OUKR is probably best undertaken by surgeons with a very specialist practise that includes high-volume mobile-bearing medial UKR use.
This series has also shown that good results can be achieved over a sustained period, but the operation is more technically demanding than its medial counterpart and the number of cases is considerably lower. This must be considered in the surgical decision making. It may be reasonable to offer fixed bearing lateral UKR for elderly patients with advanced lateral OA while offering a mobile bearing for the younger patients who may potentially benefit from the theoretically reduced risk of long-term wear.
This study clearly has limitations as it is retrospective with a limited number of PROMs available at final follow-up. Despite being quite a large series for this relatively rare procedure, the sample size in individual groups is limited for comparative data as reported in a systematic review. 11 However, we believe that the study is strengthened by being an independent series study with standard patient care and long-term follow-up that should apply to most hospital set-ups. A multicentre prospective randomised study may be warranted to validate these results and more importantly, to compare the results of the lateral UKR to TKR as recently the NICE guidelines has recommended that, based on equivalent outcomes and revision rates, as well as reduced risk and improved cost-effectiveness, surgeons consider the use of medial UKR over TKR when indicated for the medial compartment OA. 27 It seems reasonable to consider that this may in the future prove to be valid for lateral UKR in the treatment of Lateral OA.
Conclusion
This independent series shows that excellent survival and PROMs can be achieved using the cemented lateral UKR with both bearing types when performed by high-volume unicompartmental knee surgeons. The mobile-bearing implant demonstrates a slightly higher revision rate due to the risk of dislocation, with no significant benefits demonstrated so far. It therefore seems sensible to recommend the use of fixed-bearing implants to attain the best results, and suggest that mobile-bearing implants are used only by high-volume mobile-bearing medial unicompartmental surgeons.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest
Funding
No financial support was received. The material contained in the manuscript has not been previously published and is not being concurrently submitted elsewhere.
Author's contribution
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [Mamdouh Hefny], [Nick Smith], and [Jonathan Waite]. The first draft of the manuscript was written by [Mamdouh Hefny] and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.